
Abstract
Growing care dependencies among the elderly due to population ageing in Europe challenge the labour-market participation of informal caregivers. While familiarized care regimes incentivize family caregiving by providing many cash-for-care-benefits, resulting in reduced labour supply, defamiliarized care regimes allocate more public spending to care infrastructure, alleviating the care responsibilities placed on family members. At the same time, care provision on the micro-level is distributed unequally across gender, age, and socioeconomic status. The question then emerges: Does the labour-market participation of informal caregivers vary between and within countries depending on the social-expenditure policy of welfare states? To answer this research question, a multilevel design was used, employing SHARE data and macro-indicators from OECD and Eurostat databases. The results reveal higher probabilities of labour-market participation for informal caregivers in general when social expenditures on formal care infrastructure are higher. However, labour-market participation was observed as being unequally distributed among the heterogeneous group of persons with and without caregiving duties. Women and individuals of lower socioeconomic status did not benefit from social expenditures in the same way as their counterparts, leading to lower levels of labour-market participation.
Keywords
Introduction
Informal care, defined as unpaid, unsecured and unrecognized care work performed by family members or other non-professional caregivers, is the main reaction to growing care dependencies in Europe and indicates to some extent the degree of intergenerational (family) solidarity (Cavallotti et al., 2017; Costa-Font et al., 2016; Szydlik, 2000). Along with personal attitudes, normative beliefs, and familial and social expectations, contextual factors and macro-level policies are distinct drivers of informal caregiving (Broese Van Groenou and De Boer, 2016). The primary burden of informal family care often falls on the care dependents’ children or partners, who are typically between the ages of 55 and 65 years and in their late-employment phase (Kaschowitz, 2021). Depending on the degree of care needed, caregiving responsibilities can compete with employment and, thus, force labour-market exits or the reduction of hours worked (Bauer and Sousa-Poza, 2015). These exits or reductions can be influenced by factors on both the individual and the societal levels, reflecting the difficult relationship between care provision and labour-market participation (LMP). Given that providing informal care is more likely among groups with a lower socioeconomic status (SES) (Quashie et al., 2022), women (Haberkern et al., 2015), and middle-aged/older persons, these groups are at greater risk of labour market-performance reduction. On the societal level, social policies and care infrastructures play consequential roles; for instance, policies addressing long-term care (LTC) policies for elderly individuals with limitations in their daily activities gain increasing relevance in an ageing society (Colombo et al., 2011). In recent years, to reduce social spending, such policies have aimed at shifting care from residential care settings to domestic care, thereby implicitly supporting family care (European Commission, 2021). This is of particular interest when assuming that welfare states that spend more on care-in-kind exhibit greater LMP among caregivers compared to welfare states with lower expenditures on care infrastructure. At the same time, countries that support more cash-for-care programmes tend to foster familial care and lower labour-market participation among caregivers (Bertogg et al., 2020; Schmid et al., 2012). Consequently, one can presume that the higher the social expenditures on care infrastructure, the higher the LMP of female, lower socioeconomic status and older informal caregivers who face the risk of reduced participation. Therefore, the present article focuses on the following questions: Does the labour-market participation of informal caregivers vary depending on the social-expenditure policies of welfare states? How does this relationship influence country-specific inequalities in caregiving between different social groups? Previous research on the link between social policies and informal caregiving has typically clustered welfare regimes on a macro level and concentrated on specific sociodemographic groups on the micro level (Dykstra, 2019; Verbakel et al., 2022). Consequently, factors such as country-specific social policy indicators, including elderly care programmes, and the individual characteristics of caregivers have largely been overlooked, preventing a nuanced understanding of the varying impact of single policy programmes across countries and how caregivers, as a heterogenous group, face specific and varying degrees of social inequalities. Thus, this study contributes to previous research by examining the relationship between welfare state provision (by selecting single policy programmes and aggregating them as social policies for formal elder care) and the LMP of informal caregivers, taking various sociodemographic characteristics into account.
Theoretical background and state of research
While ‘family members are the backbone of a society’s care supply’ (Bauer and Sousa-Poza, 2015: 115), the extent of this time-consuming care depends on the labour supply of its providers, specifically their employment status and the extent of their commitment (hours worked per week). However, the decision to participate in the labour market may depend on the extent of care provided, pointing to a mutually dependent relationship between care provision and LMP, the direction of which remains unclear (Heitmueller, 2007; Hollingsworth et al., 2021).
Labour-market participation and care provision on the individual level
On the individual level, the provision of care within the family reflects one dimension of the model of intergenerational solidarity, which generally refers to the relationship between parents and their adult children. Functional solidarity, as one dimension, is subdivided into monetary transfers, co-residence, and instrumental support, with this latter component comprising personal care, practical help in the household, and advice (Bengtson and Roberts, 1991; Szydlik, 2000). Personal care seems to be the most intense and time-consuming aspect of instrumental support, thus competing particularly with the LMP of caregivers. The decision to provide care or to participate in the labour market is driven by individual characteristics, especially gender, age, and SES. In this article, the focus lays not only on upward care (that is, care for older generations, such as parents), but also on lateral care (that is, care for the same generation, such as partners) (Bertogg et al., 2020), because informal care for a partner may be considered generational solidarity, in this sense, as intragenerational solidarity. Following Cavallotti et al. (2017), spousal caregiving is included in an overarching ‘intergenerational family solidarity model’.
Regarding gender, women in Europe do not only provide more frequent and time-intensive care, but they also more often face the negative effects of informal caregiving on employment, in particular reductions in hours worked and withdrawal from the labour market (Kotsadam, 2011; Principi et al., 2014). According to sociological theories of gender and human capital, the underlying mechanisms may include bargaining processes within the household, which mainly transfer care responsibilities to women. Prevailing gender roles and stereotypes, anchored in conventional familial obligations, are related to norms and expectations acquired through one’s life course, shaping and determining these processes. This is reflected in the male-breadwinner model – still prevalent in many European welfare states – in which men participate in the labour market while women are in charge of the household, family, and care duties. The differential LMP of men and women can also contribute to this division of labour: through their greater material and immaterial resources and higher LMP due to normative gender-specific investments in human capital, men are more likely to continue their LMP and forgo care responsibilities. Furthermore, decisions regarding divisions of labour are often rational choices: if the value for the household is assumed to be maximized for all individuals, care is more likely to be provided. Therefore, the household or family member with a lower wage (and often, simultaneously, a lower educational level) is more likely to reduce their employment 1 (Becker, 1985; Lewis, 1992). Bargaining related to intergenerational relationships involves more individuals, family members and households. Shared norms and values, as well as reciprocity play a key role in the understanding of intergenerational family solidarity. Over their life course, individuals may receive help from family members (for example, parent’s support in childhood) or partners and seek to give something back at a later point in time or feel morally obliged to return the support. Therefore, mutual dependencies grow over the life course. Furthermore, caregiving responsibilities can arise from the negligence of other family members, who do not want to or are unable to provide care. However, regardless of the specificities, women tend to assume caregiving responsibilities, as daughters, for example, are more often the primary caregivers to their parents (Finch and Mason, 2005; Keck, 2008; Pezzin et al., 2015). Possible reasons for this are (gender) roles and identities internalized in one’s childhood and reactivated later in life (Lloyd-Sherlock et al., 2018).
In addition to gender, SES plays an essential role in care provision. A lower income increases the likelihood of leaving the labour market in the UK (Henz, 2006), and middle-aged female caregivers in Germany have lower educational levels as well as poorer allegiance to the labour market (Kelle, 2020). Meanwhile, because of unfavourable working and living conditions, coupled with unhealthy behaviours, care needs are higher in lower socioeconomic groups. Norms, beliefs, and expectations of family support are also stronger in these groups. Additionally, as access to formal care is dependent on financial resources, lower SES groups tend to use a more cost-effective informal care. Thus, the care provision can also depend on work income (Floridi et al., 2021; Quashie et al., 2022). In sum, caregiving decisions are influenced by the different needs, norms, attitudes, and financial resources of various SES groups. This is rimmed by the theoretical framework of a behavioural model of health care (Andersen and Newman, 2005), which traces the use of informal or formal help to need factors (health inequalities), predisposing factors (age and gender), and enabling factors (material and social resources). As family members are the main providers of informal care and lower SES groups primarily use it, it can be assumed that the provision of informal care is higher among these groups (Broese Van Groenou et al., 2006) and LMP is thus likely to be lower.
Positive effects of age on the probability of caregiving have been discovered (Bolin et al., 2008; Mentzakis et al., 2009). It is widely recognized that individuals within the 55–65 age group predominantly assume caregiving responsibilities, aligning with the concept of the ‘parent support ratio’, reflecting the demographic change. If the spouses and children of care dependents are the primary providers of informal care and care dependencies increase after the age of 65, especially at 80 years, it can be assumed that informal caregivers are older and probably in their late employment phase (Kaschowitz, 2021). Furthermore, according to theories of cumulative disadvantage, the detriments of socioeconomic and gender inequalities over the life course can accumulate in old age (Rosenmayr and Majce, 1978). Additionally, increasing women’s employment makes personal care by younger (female) grandchildren less likely (Lloyd-Sherlock et al., 2018). The decision to supply care is therefore more likely at more advanced ages. Based on these considerations, it is assumed that the labour-market participation (H1a) and the number of hours worked (H1b) of informal caregivers, which are dependent on SES, gender, and age, are lower (Figure 1). Hypotheses based on the theoretical assumptions and framework.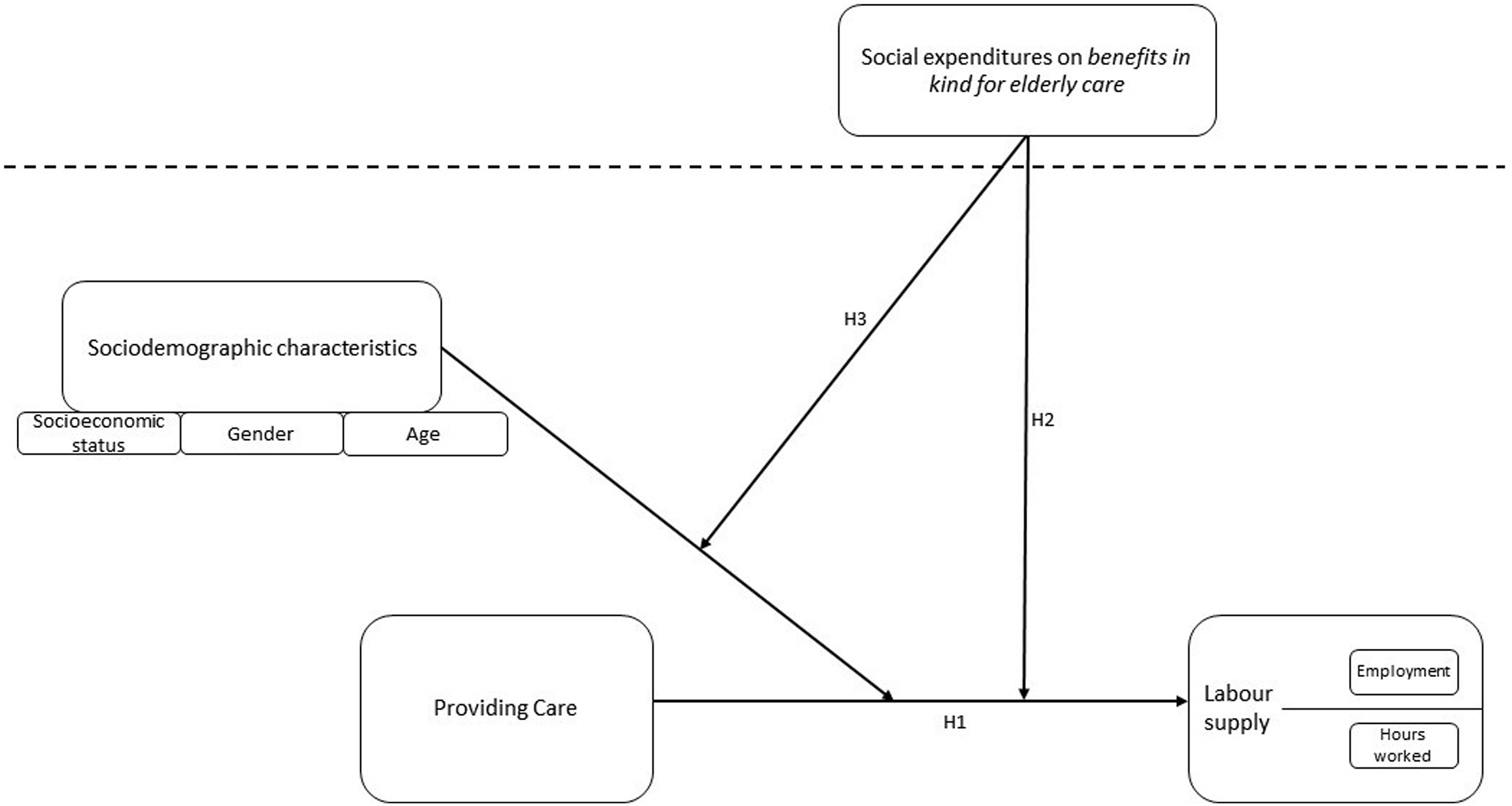
Labour-market participation and care provision in welfare-state context
LTC policies, targeting the formal (that is, inpatient facilities, such as nursing homes or day-care centres) and informal support (that is, legal obligations to support family members or cash benefits for informal caregivers or receivers) of care dependents vary across Europe and are highly contingent upon the welfare states in which they exist. For instance, the Scandinavian welfare states have a high provision of benefits in kind, while the Mediterranean model has means-tested benefits with relatively low levels. The continental model provides comprehensive benefits as it shows a mixture of cash benefits and benefits in kind. A relatively low level of benefits is provided in the Anglo-Saxon model (Colombo et al., 2011; European Commission, 2021). As seen here, policies moderate the interplay between state, market and family regarding care arrangements and express the level of (de)familization, a concept for which there is a broad literature 2 (see Lohmann and Zagel, 2016 for an overview). In particular, it refers to the degree of (in)dependence of individuals on the state and the market, but also on their family concerning gender or intergenerational relations. 3 If there is a comprehensive state-organized or market-based formal care infrastructure that people with care needs or responsibilities can use, necessities of informal care provision and, in this sense, family care may decrease, while the need for state and market may increase 4 (Lister, 1994; McLaughlin and Glendinning, 1994). Both defamilization and familization can occur at the same time, such as a state that offers both care infrastructure and care allowances (Kalmijn and Saraceno, 2008; Leitner, 2003; Saraceno, 2016; Saraceno and Keck, 2010; Zagel and Lohmann, 2020). Previous research has shown that welfare states providing only or primarily cash benefits compel family members to provide care and limit LMP (familization), whereas welfare states with greater support for public spending on care infrastructure reduce family care provision (defamilization) (Bertogg et al., 2020; Broese Van Groenou and De Boer, 2016; Schmid et al., 2012).
Thus, social expenditures can stimulate, enable and determine the extent to which individuals can access formal care and the (in)dependence of family members from/on care responsibilities and of work. 5 Through the provision of (cost-effective) formal care infrastructure, the general need for informal care can decrease, and financial barriers can be lowered. For persons in their late employment phase or with other care responsibilities (for example, childcare), time barriers can be lowered, and the mutual dependence between caregivers and care receivers can decrease (Saraceno, 2016; Verbakel, 2018). Thus, the welfare state affects individuals’ potential for caregiving, LMP and their level of intergenerational family solidarity. If there is no need for informal family care because the state provides sufficient formal care infrastructure, only the normative decision of informal care by family members, based on expected norms and inhabited values, can compete with LMP. Previous studies have clearly shown differences across national contexts. For instance, the probability of employment among daughters who provide care to their parents is reduced in ‘family care countries’, but not in ‘formal care countries’ (Heger, 2014). The lowest employment rates are found in the Mediterranean and the transition model, which are marked by culturally and institutionally anchored family–care responsibilities (Principi et al., 2014). Care provision for a co-residing adult reduces the employment probability more in Southern than in Northern Europe (Ciani, 2012), and caregiving daughters have a lower probability of employment in Southern European countries (Crespo and Mira, 2014). These variations could be a result of differential LTC policies and the types of support across Europe: support and help are more frequent and demanding in Southern Europe and less often as well as more sporadic in Northern Europe (Brandt et al., 2009). Nevertheless, there tends to be a reduction in LMP across Europe when children provide informal care to a dependent parent (Kolodziej et al., 2018), as well as fewer hours worked for female informal caregivers (Heger and Korfhage, 2020). Furthermore, cash-for-care expenses increase the probability of labour-market exits by persons who provide upward or lateral care (Bertogg et al., 2020). These studies, however, demonstrate that the welfare-state context makes a difference in the relationship between care and LMP. Thus, two hypotheses can be derived: The higher the social expenditures on benefits in kind for elderly care, the higher the labour-market participation (H2a) and the number of hours worked per week (H2b) of informal caregivers (Figure 1).
Labour-market participation and care provision: Cross-level influences
Considering cross-level interactions regarding gender, daughters are more often caregivers to their needy parents than sons, even when both have the same resources, and are, therefore, at higher risk of labour-market exit. Although gender inequalities remain pervasive in rather defamiliarized countries, they are more pronounced when there are fewer offers of professional care and more cash benefits for elderly care (Haberkern et al., 2015). Here, mechanisms on the individual and societal levels interact and reinforce each other. As discussed in the second section, due to gender-specific responsibilities within the family, care and labour supply are differently distributed between women and men, whereby these mechanisms can be strengthened or mitigated by social policies, for example, formal care services.
Moreover, the provision and use of informal care is more common among lower SES groups and ‘appears to behave in different ways in different societies’ (Broese Van Groenou et al., 2006: 748). For instance, welfare states with a higher proportion of long-term care beds facilitate access to formal homecare for lower SES groups (Floridi et al., 2021), and higher service provision for care and social-protection expenditures improve access to formal care (Albertini and Pavolini, 2017; Quashie et al., 2022). In the second section it was discussed that, under the influence of specific need factors, material resources and strong norms of family support among SES groups, the likelihood of personal care on the individual level is higher. Cost-effective offers and those with low access barriers allow welfare states to reduce the probability of personal care for these groups. Nonetheless, studies addressing the link between social policies and employment among different socioeconomic caregiving groups are absent.
Furthermore, the main responsibility for care falls on the spouses and adult children of the care receivers (aged 55–65 years), who face employment risks in their late employment phase. In the UK, there is a growing probability of care provision, especially for female caregivers and in particular in cases of parent care at more advanced ages (Henz, 2023). The underlying mechanisms on the individual level may be reciprocity and norms within the family as well as the greater availability of time for care (for example, no time barriers related to childcare) and cumulative disadvantages over the life course. Studies, focusing on the link between social policies and employment in age-related caregiving are, so far, lacking.
While defamilized welfare states seem not to dissolve gender inequalities completely, they lower inequalities between different socioeconomic groups: when financial access barriers are removed via higher social expenditures on elderly-care infrastructure, lower-income groups tend to switch from informal to formal care. Here, material resources on the individual level seem to play a more prominent role than norms and attitudes towards formal-care use, though gender-specific roles, norms, and expectations do not disappear entirely. Therefore, two main cross-level hypotheses can be derived: The higher the social expenditures on benefits in kind for elderly care, the higher the labour-market participation (H3a) and the number of hours worked (H3b) of female, middle-aged and lower socioeconomic status caregivers (Figure 1).
Methodological approach and data
To analyse how European Welfare states’ social expenditures on elderly-care policies affect the LMP (employment status and the number of hours worked) of people who care for elderly partners or parents across sociodemographic characteristics, a multilevel analysis was used, enabling an exploration of the link between two (or more) levels (Snijders and Bosker, 2012). On the micro level, six waves (1, 2, 4, 5, 6, and 7) of the Survey of Health, Ageing, and Retirement in Europe (SHARE) (Börsch-Supan, 2021; Börsch-Supan et al., 2013; SHARE, 2022) and macro-level indicators from OECD and Eurostat databases were used for the analysis 6 (Eurostat, 2022; OECD, 2019, 2022). After restricting the sample to respondents aged 50–68 years and considering missing values, the merging of the data yielded 58,383 observations, six observation time points (2004–2017), and 16 countries. Cross-sectional data were employed since using the panel structure would exclude more countries and individuals. Only the newest observation for a respondent was considered, so 2017 had the most observations (20,243), and 2011 had the fewest (1830). Observations within the countries ranged from 1033 in Portugal to 5436 in Belgium. This use of cross-section data introduced potential limitations to the study: While it was possible to demonstrate the LMP of informal caregivers in different welfare state contexts, this alone was insufficient to make a causal statement regarding whether informal caregiving leads to changes in LMP. Because care activities in the late employment phase were of central concern, caregiving for partners and parents was aggregated, focusing on the relationship between the social expenditures of welfare states and the LMP of informal caregivers. LMP was investigated through the individual employment status, labelled as 0 for ‘not employed’ and 1 for ‘(self-)employed’, and the total number of hours worked per week, ranging from 0.3 to 70 h. Because personal care for parents or partners is time-consuming and can thus affect caregivers’ LMP, it served as the main independent variable of the analysis and reflects the care provision. Personal care within the same or in another household was summarized and labelled as 0 for ‘Not having provided care to partner or parents’ and 1 for ‘Having provided care for partner or parents’. 7 Moreover, through cross-level interactions, the joint effect of social policies, care provision, and individual factors on LMP was measured. Therefore, this study investigated the relationship between LMP and instrumental support (in the form of personal care) as one dimension of functional solidarity 8 within the concept of intergenerational family solidarity, moderated by social policies and individual characteristics. The hypotheses were tested through linear probability models (employment status) and linear models (working hours). Results are presented through scatterplots for the predicted values of the dependent variables, for which non-caregiving serves as the reference group of caregiving to reveal the gap between those two groups. It was assumed that social expenditures have a positive effect on that gap, so its narrowing was expected when the benefits in kind were high. Since advice and practical help in the household, in addition to personal care, correspond to instrumental support and, thus, may have an impact on the link between caregiving and LMP, they were taken into consideration as further dichotomous independent variables. Additional independent variables were household income (z-standardized) and educational level (ISCED-97), which represent SES, gender, age (z-standardized), frequency of help, subjective health, marital status, household size, and country (Börsch-Supan, 2021). The primary macro indicator was social expenditures on benefits in kind for elderly care (as a share of GDP in the national currency) according to the OECD Social Expenditure Database. Therefore, in this study, each single policy programme for elder care was considered separately for each country and, to the extent that it was found to support formal elder care, expenditures on these programmes were considered and aggregated at the country level (Table A4 in the appendix). This approach was intended to ensure that only policies which explicitly supporting formal care were included in the analysis. Further macro indicators were taken from the OECD labour force statistics, OECD Demography and population data, the OECD health and life expectancy data, and OECD health long-term care data, as well as Eurostat data on economy and finances, including GDP, female labour-force participation rate, further life expectancy rate and the proportion of persons aged 65 years or older, which served as control variables (Eurostat, 2022; OECD, 2019, 2022). Country-years were used as a grouping variable to address the small-N problem 9 and increase the number of groups considered. This number ranged from 41 observations in Greece in 2004 to 3033 in Poland in 2017.
Results
Descriptive findings
The descriptive findings are presented in Figure 2. The means of LMP for caregivers and non-caregivers across countries are applicated through bar charts on the top and, on the bottom, differences in employment rates between caregivers and non-caregivers in the individual countries are shown in a scatter plot. At a first glance, the results indicate that Denmark had by far the highest LMP among those who provide care to their partner or parents and those who do not, although the outcome was lower among caregivers. However, Denmark displayed relatively low hours worked compared to other countries, which were lower for caregivers than for non-caregivers. Employment status varied between countries more than hours worked. In Denmark, for example, more than twice as many (60%) were employed than in Slovenia (28%) when care is provided. Furthermore, while the differences between caregivers and non-caregivers were relatively high in Greece and Spain (higher employment rate of non-caregivers), they were almost non-existent in the Netherlands. Additionally, the proportion of employed caregivers was lower in Estonia, but they hardly differed from non-caregivers in terms of hours worked per week. The situation was reversed in Poland: caregivers worked fewer hours but had higher employment rates than non-caregivers. In some countries, caregiving seems to affect employment itself (that is, no time to work at all), while in others, it influences the extent of employment more strongly (that is, time to work but reduced volume of hours). Top: Employment rates (left) and of working hours (right) over country if respondents provide care or not; Bottom: Differences of employment rates between caregivers and non-caregivers by benefits in kind and employment (left) as well as working hours per week (right).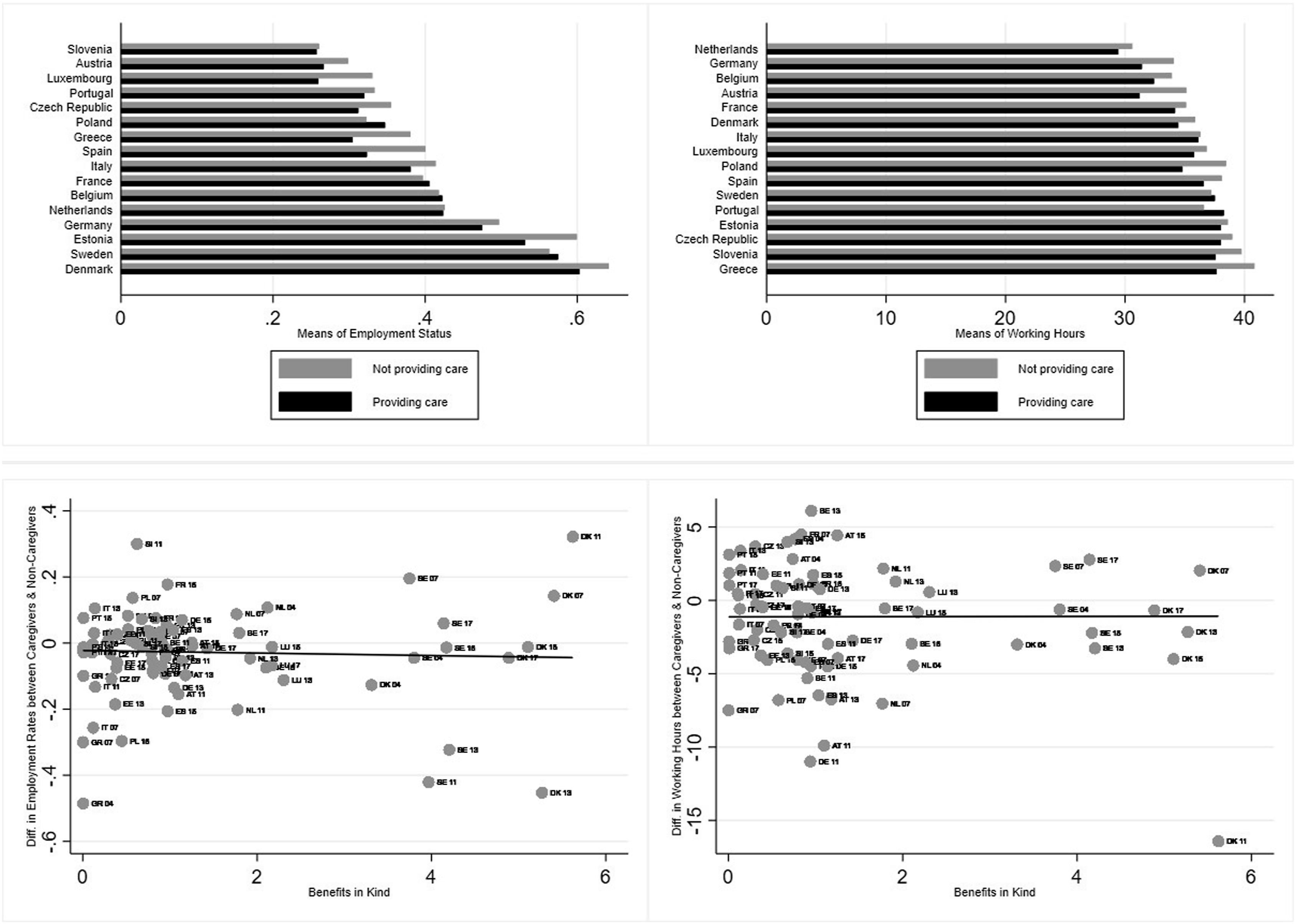
The group means of caregivers and non-caregivers by benefits in kind and employment status/hours worked did not reveal many differences between caregivers and non-caregivers. 10 Regarding employment status, differences seem to increase with higher benefits in kind but decrease for hours worked at the same time. However, it should be noted that Sweden and Denmark offered the highest benefits in kind, whereas Greece and Italy exhibited low expenditures and Luxembourg and the Netherlands medium expenditures. How they are connected to employment status and hours worked could not be inferred and, thus required multi-level regression models.
Results of the multi-level analysis
Random slope multilevel linear regressions of personal care on labour market participation (employment status 0–1) as well as on working hours per week (0.3–70) and sociodemographic characteristics, benefits in kind and (cross-level) interactions with micro variables (M1|M2|M6|M7), macro indicators (M3|M4|M8|M9) and both (M5|M10).
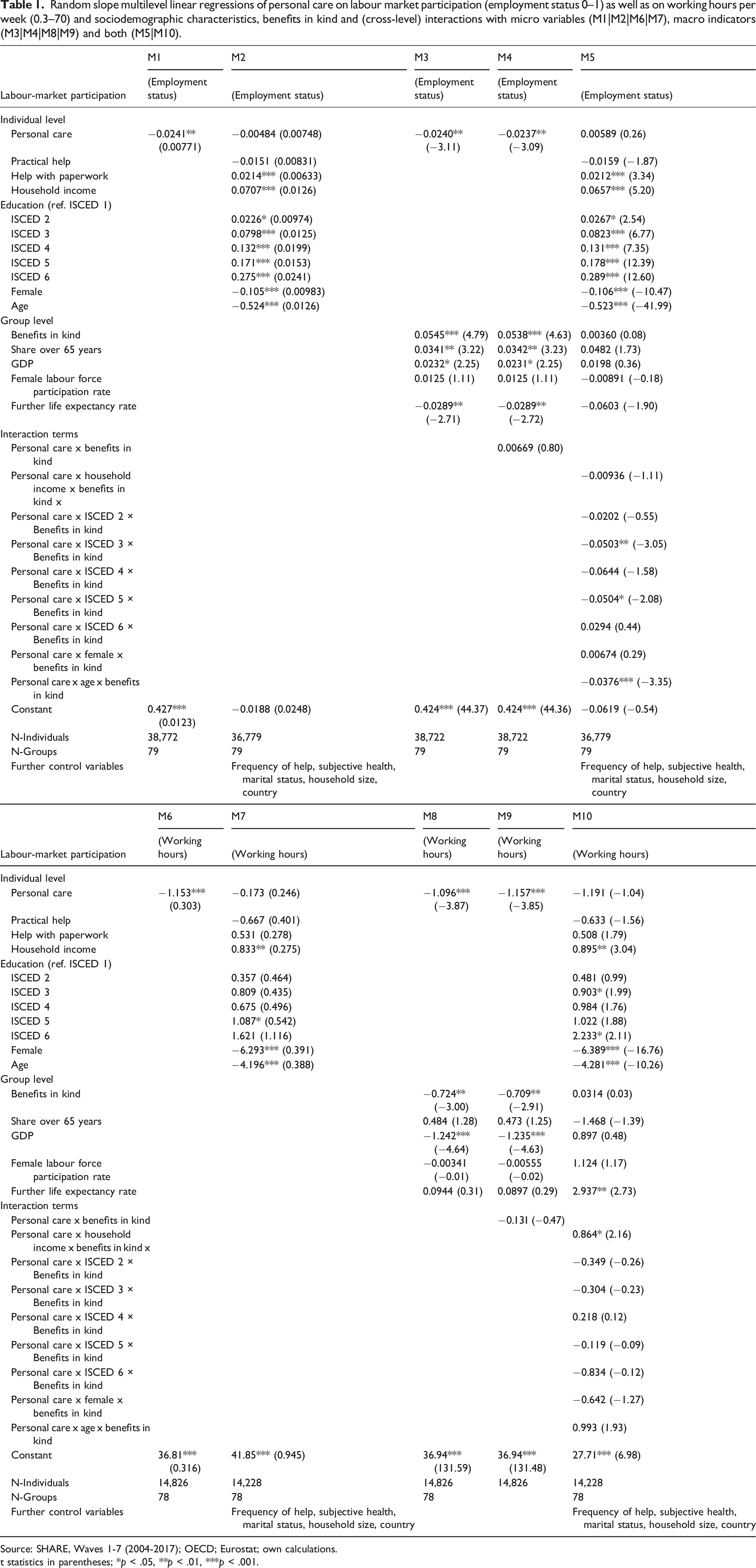
Source: SHARE, Waves 1-7 (2004-2017); OECD; Eurostat; own calculations.
t statistics in parentheses; *p < .05, **p < .01, ***p < .001.
Models M5 and M10 include all micro variables and macro indicators considered, as well as cross-level interactions. For a better illustration and interpretation, the marginal effects for the predicted probabilities at specific values (benefits in kind −1|0|1) were plotted (Figure 3), and the results are described below. The standardized values of benefits in kind are shown on the x-axis; 1 indicates one standard deviation upward from the mean, −1 is one standard deviation downward from the mean, and 0 is the exact mean for caregivers (grey line) and non-caregivers (black line). The y-axis reflects the linear prediction of employment probabilities (left) and hours worked (right). The predictions are made at specific values of benefits in kind for different groups of income (standardized values ‒1|0|1), educational level (ISCED 1−6), gender (male|female), and age (standardized value −1|0|1). Notably, caregivers and non-caregivers did not differ considerably in their LMP, and any differences were nonsignificant across all characteristics considered.
15
The amount of social expenditures did not seem to influence the gap between caregivers and non-caregivers regarding their LMP; therefore, generous welfare states generally seemed to be related with higher LMP of caregivers and non-caregivers. The probability of employment was higher among all income groups when benefits in kind were higher, although the increase and initial levels were highest for high-income groups and lowest for low-income groups. For all educational levels except for ISCED 4, there was a significant constant increase in employment probabilities when social expenditures on informal elderly care were higher. Although this increase was stronger for caregivers than non-caregivers within low-education (ISCED 1) and high-education (ISCED 6) groups, these differences were nonsignificant. This is also true of gender differences between those who did and did not provide care. While gender differences were observable, employment probabilities increased significantly with higher benefits in kind for both genders. The increase was stronger for women, although the gender gap was not closing but merely narrowing. Regarding age, there were hardly any effects – a slight increase for low age and (nonsignificant) mean age and not notable decrease for high age – and almost no (or only nonsignificant) differences between caregivers and non-caregivers. Interaction effects of personal care, household income/education level/gender/age and benefits in kind on employment status (left) and on working hours (right).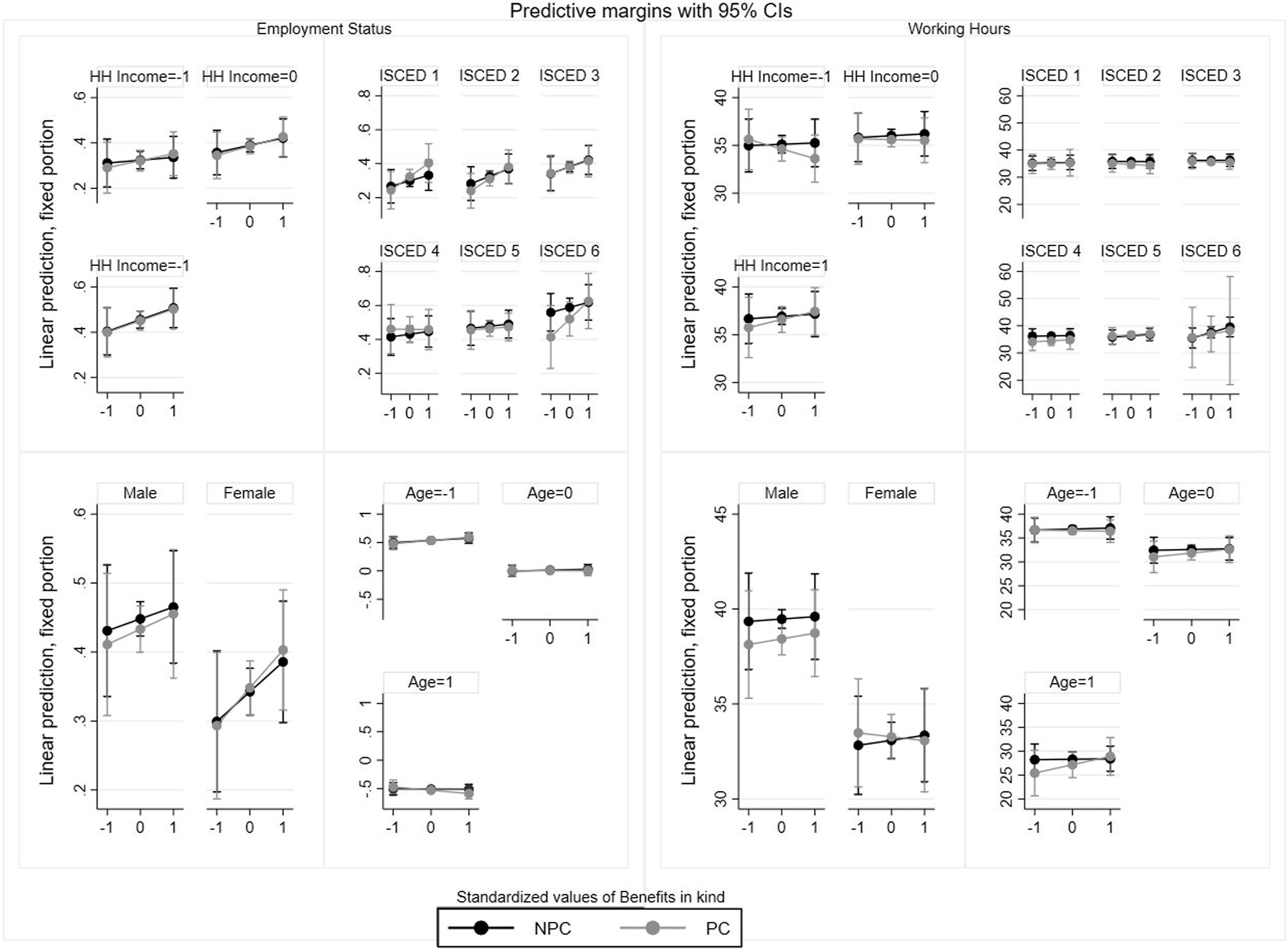
Hours worked decreased significantly for low-income caregivers when benefits were higher. The mean-income group indicated a slight increase, and the high-income group a somewhat greater increase (both significant). Regarding educational level, a strong increase was observable only for the highly educated (ISCED 6). For the levels ISCED 2 and 3, there was a slight decrease, whereas there seemed to be no variation for ISCED 1, 4, and 5. Female caregivers’ hours worked decreased with higher benefits in kind, whereas those of male care- and non-caregivers as well as female non-caregivers rose. There were no noteworthy effects of age, only a minor increase in hours worked for all age groups except for older non-caregivers. For all observations, the differences between caregivers and non-caregivers were nonsignificant. Moreover, the results indicate different directions than the descriptions.
Discussion
Although at first glance, LMP decreased when individuals provided care to partners or parents, further analysis demonstrated that SES, gender, and age have much stronger predicting power for LMP than care duties. Thus, hypotheses H1a and H1b, which assumed the opposite, are rejected. Caregivers were primarily female, older, and of lower SES. An accumulation of these indicators may be reflected in the results. Nevertheless, women exhibited lower LMP due to bargaining processes based on gender stereotypes, norms, and expectations in society.
As the results further suggest, the higher social expenditures on benefits in kind for elderly care, the higher the LMP among caregivers. Therefore, hypothesis H2a is supported. On the contrary, the findings indicate that (non-)caregivers work fewer hours when benefits in kind are high; thus, hypothesis H2b cannot be confirmed. The results may point to the welfare states’ failure to lower financial and time barriers for individuals as well as the mutual dependencies between caregivers and care receivers as discussed in the second section. Alternatively, formal care services may remain expensive and, thus, less frequented, or information about access could be lacking. One key finding is that there are only a few weak differences between caregivers and non-caregivers. Welfare-state spending seems to play a key role for both groups as their employment probabilities rise and working hours decrease. This suggests that, in general, fulltime employment is not necessary in more generous welfare states, but individuals who are more likely to work are enabled to do so, even to a lower extent (such as through broader childcare infrastructure, stronger social security and so on).
The main hypotheses, namely, that the higher social expenditures on benefits in kind for elderly care, the higher the LMP (H3a) and hours worked (H3b) for female and middle-aged caregivers and those with lower SES, are supported, leading to two main conclusions: First, there are substantial differences between welfare states. While more generous ones (in terms of social expenditures on elderly care) enable higher LMP among nearly all groups of (non-)caregivers, those that spend less show opposite results. Connecting these findings to the discussed literature, a defamilizing function in the form of higher LMP and degrees of independence from care and family can be assumed. Nevertheless, considering the cross-level interactions, the distinct differences first occur at the individual level. Second, within welfare states, differences were observed within the groups of (non-)caregivers, indicating persistent social and gender inequalities. LMP among caregiving individuals was indeed higher in more generous welfare states (for example, Denmark and Sweden), but especially female and lower socioeconomic (non-)caregivers did not benefit in the same way. The defamilizing function by welfare states appeared to be uneven for all (non-)caregivers, and their LMP was thus unequally distributed. For some groups, welfare state spending even acted as a familizing force as female and low-income caregivers reduced their hours worked when social expenditures were high (although the differences to non-caregivers were nonsignificant). Therefore, the direction of welfare-state spending is unclear, and gender and social inequalities are not eliminated but persist. Different working time models with high flexibilities in more generous welfare states, such as the Nordic countries (Chung and Tijdens 2013), could affect these outcomes, which could only be assumed in this study but not tested. This could be reflected in the outcomes of Denmark (Table A3 in the appendix), where the benefits in kind are high but working hours are low compared to the other countries. Further research should test whether there is a link between high social expenditures and the shape of working-time models in European countries and if that link could affect the LMP of (non)caregivers. On the individual level (can also be interpreted for the results of hypotheses H1a and H1b) prevailing norms regarding reciprocity, gender stereotypes, and roles, which are generally stronger in lower SES groups, as well as gender-specific investments in human capital, can lead to different employment histories and tendencies, thus resulting in gender and socioeconomic inequalities in terms of LMP. For caregivers, access to professional care could also be expensive and, therefore, unaffordable for low-income groups. Highly educated individuals may have better access to information about professional care because of greater degrees of human capital. Age appeared to have little effect, and retirement may play a greater role than welfare-state spending, although this is dependent on the social-security systems of welfare states. But, in general, older individuals may be more likely to retire, even before becoming a caregiver. If they retired because of caregiving, which cannot be said because longitudinal data is missing, it may be an expression of cumulative disadvantages over one’s life course, due to an accumulation of gender and socioeconomic detriments in older age as discussed in the second section. 16 As there were no significant differences between caregivers and non-caregivers, it is not possible to demonstrate the impact of social policies on the reduction or increase of intra-class differences within caregivers. Further, due to the restricted number of cases on the micro and macro levels, a panel analysis was not possible. 17 Thus, the relationship between LMP and care provision cannot be assumed to be causal, even if this study controlled for female LMP (typically fewer hours worked). Additionally, due to missing information on hours of care provision, care supply could not be illustrated in an encompassing manner. Furthermore, some macro indicators, such as long-term care beds in institutions and the overall share of care receivers, could not be integrated into the analysis because of missing data for some countries. Despite these limitations, this study shows that through social policies, especially social expenditures on elderly care, welfare states can moderate the balance between care and labour supply by strengthening, stabilizing, or mitigating the (in)dependence of family members from/on care responsibilities and work. In employment-centred societies, where employment constitutes the basis for social security in retirement, it is important to prevent periods of non-employment, labour-market exits, and reductions in hours worked. Because those inequalities are shown in the results for non-caregivers as well, social policies should address them by implementing or extending programmes that aim to increase LMP rates among women and lower SES groups. One possible approach could be to implement working-life time accounts for a better compatibility of times with care responsibilities and working times as well as to prevent that women and lower SES groups are mainly responsible for informal care work. Moreover, it is essential to not only increase the social expenditures of welfare states but also expand formal care infrastructure. In ageing societies, care will become a basic need for numerous older people and should be treated as such. Everyone’s care needs must be met conscientiously without affecting individuals’ LMP, regardless of gender, age, and socioeconomic status. That is to say, social inequalities must be dissolved.
Supplemental Material
Supplemental Material - Defamilization? Not for everyone. Unequal labour-market participation among informal caregivers in Europe
Supplemental Material for Defamilization? Not for everyone. Unequal labour-market participation among informal caregivers in Europe by Miriam Laschinski in Journal of European Social Policy.
Footnotes
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: the research leading to these results received Funding From the Landesforschungsförderung Hamburg (Behörde für Wissenschaft, Forschung, Gleichstellung und Bezirke) (LFF-FV64 “Sorgetransformationen. Forschungsverbun).
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.