
Abstract
Citizens’ attitudes towards their national healthcare are important indicators of satisfaction and of political perspectives. In this article we summarise individual and national level patterns in healthcare evaluations across Europe. An innovative feature of our analysis is that we demonstrate that assessing healthcare evaluations in relative terms (relative to citizens’ views about the performance of national institutions in other domains), offers new insights about individual and national level variations in attitudes. Thus, we introduce an indicator of relative attitudes towards healthcare and contrast it to an absolute measure in a cross-national analysis. We use a larger dataset than previous studies of healthcare evaluations including countries from all regions of Europe and spanning eight rounds of the European Social Survey (2002–2017, N = 342,000). We find that Europeans’ healthcare evaluations are multidimensional, with different patterns sometimes operating at an absolute and a relative level. When comparing countries, for instance, several nations in Southern and Eastern Europe compare poorly to other nations in their absolute ratings of healthcare but compare favourably if assessed in relative terms. Likewise, using a relative measure, most Scandinavian countries compare less favourably to other countries, but score positively when evaluations are measured in absolute terms.
Keywords
Introduction
Research on public opinion towards institutions providing welfare services is crucial for assuring the sustainability of existing institutions in response to global and national developments. An accurate understanding of citizens’ attitudes towards public institutions allows us to assess whether existing societal arrangements are legitimate (Svallfors, 2012), and indicate whether citizens’ experiences build trust towards the institutions (Kohl and Wendt, 2004), such as healthcare systems. Citizens’ attitudes to healthcare could also impact upon other important behavioural responses – for example, compliance during the COVID-19 pandemic to vaccination and social distancing advice (see, for example, Gilson, 2003; Larson et al., 2011).
As societal arrangements differ across countries, a natural focus in social policy research has been to compare public opinion about state services between countries. Nevertheless, accurately representing variations in attitudes towards state institutions is challenging. Previous research relies largely on isolated single item measures such as Likert responses to a standard format question on an aspect of welfare – what we call ‘absolute’ measures (on government benefits and services, see for example, Andreß and Heien, 2001; Blekesaune and Quadagno, 2003; Gelissen, 2000; on healthcare evaluations, see for example, Footman et al., 2013; Schneider and Popic, 2018; Popic and Schneider, 2018; Borisova et al., 2017). Well-designed single-item questions on major surveys, such as the European Social Survey, have good criterion validity (for example, ESS, 2021a, 2021b). However, such questions in isolation are unequipped for assessing the implications of national level variations in response patterns. For example, studies have found that attitudes towards healthcare performance are more negative in Eastern than Western Europe (Popic and Schneider, 2018; Missinne et al., 2013). It remains unclear, however, whether Eastern Europeans evaluate healthcare more negatively than other national institutions, for instance in comparison to a national or regional ‘normal’ level of institutional attitudes. This matters because the implications might differ accordingly: negative attitudes across the range of institutions might imply problems of legitimacy or support for widespread policy change (for example, Kohl and Wendt, 2004); by contrast, negative attitudes applying only to healthcare systems might suggest more specific, healthcare-related challenges.
Van Oorschot and Meuleman (2012) have argued that if individuals evaluate welfare state functions (such as taxes or government involvement) differently, one underlying attitudinal indicator cannot fully capture the versatility of public support towards the welfare state. Indeed, attitudes towards national institutions are conventionally represented by their rating on some fixed, ‘absolute’ scale, but they could alternatively be understood ‘relative’ to some important contextual norm. For instance, literature about measuring poverty in these terms is well established (for example, Foster, 1998): an absolute measure of poverty evaluates circumstances against a fixed threshold defined typically by a material or economic quantity; a relative measure of poverty defines poverty contingent on the distribution of resources within the relevant society. In other areas of comparisons, researchers similarly consider comparing measures defined around fixed or absolute criteria (for example, whether or not an individual has a university-level education), or in relative or ‘positional’ terms (for example, where an individual’s educational experience places them in relation to their birth cohort norms) (for example, Harkness et al., 2003). In personal values research, rating scores of personal values are seen as relative to their ratings on all other values (Borg and Bardi, 2016).
When comparing attitudes to national institutions across countries, a plausible relative measure might standardize according to some level of national distribution – for instance, whether an individual’s expressed attitude puts them above or below their national average. This strategy, however, risks downplaying any genuine national level variations, and forces attention towards differences between people within countries. Instead, a compelling alternative relative measure utilizes surveys that include questions about several different aspects of national institutions. Thus, focusing on healthcare attitudes, we operationalize and compare a measure of healthcare evaluations which is standardized against individuals’ expressed attitudes on the performance of national institutions in other domains (discussed in the third section). The resultant measure taps into a different important dimension of healthcare views: whether individuals regard their healthcare system’s performance relatively more or less favourably compared to their attitude about other elements of institutional performance. To the best of our knowledge, such a dimension of institutional attitudes has not been explored before. However, we argue our empirical analysis shows that a measure defined in these terms reveals plausible alternative patterns of variation on inequalities in the formation of healthcare evaluations in Europe. 1
Patterns of variation in European healthcare attitudes
An understanding of variation in European healthcare attitudes is of value, first, in determining whether there is evidence of systematic associations between healthcare attitudes and measured characteristics at the individual or national level; and second, in establishing whether there are national level average differences in healthcare attitudes, either at a descriptive level or net of controls for measured characteristics.
There are reasons to expect individual or national characteristics to associate with healthcare evaluations. According to institutional theory, the institutional design of health systems shapes public support for healthcare; for instance, the extent to which care accessibility depends upon the availability of service providers or the use of referrals (Wendt et al., 2010). Many cross-national studies demonstrate strong correlations between public views of healthcare performance and specific aspects of the institutional arrangements of healthcare systems: the provision of health services (Borisova et al., 2017; Popic and Schneider, 2018; Wendt et al., 2010), and healthcare financing (Borisova et al., 2017; Popic and Schneider, 2018; Kohl and Wendt, 2004; Missinne et al., 2013). Institutional structures of different healthcare systems, such as health service supply and health expenditure, should therefore help understanding citizens’ attitudes towards healthcare between European countries.
In the European context, studies on regional attitudinal differences in citizens’ healthcare evaluations find more negative evaluations in Eastern than Western Europe (Missinne et al., 2013; Schneider and Popic, 2018; Popic and Schneider, 2018). These East–West differences have been explained by regional differences in health service delivery (Popic and Schneider, 2018), health outcomes (Missinne et al., 2013), perceptions of healthcare performance (Schneider and Popic, 2018) and economic resources, particularly in total and public health expenditure (Schneider and Popic, 2018; Popic and Schneider, 2018). Also, Mossialos (1997) observed a North–South divide in Europe in citizens’ satisfaction with healthcare systems.
Almost all previous studies have assessed variations in healthcare evaluations using absolute measures (respondent’s subjective ranking of healthcare evaluation). However, there are good grounds for exploring similar variations in relative evaluations (the extent to which respondents regard healthcare more or less positively than they do performance of other national institutions). Any differences in patterns between absolute and relative measures might help to suggest social mechanisms associated with different dimensions of institutional support. Thus, we might see that particular social groups or nations have distinctive patterns in their profiles of absolute and relative measures, which might reveal otherwise concealed mechanisms. For instance, if a study found that immigrant respondents were more likely to combine poor absolute healthcare ratings with neutral relative ratings, their poor ratings could reflect a challenge of service delivery for immigrants across domains, including healthcare, but not necessarily specific to healthcare.
Furthermore, Roosma et al. (2013, 2014) showed that citizens’ attitudes are complex and observed four different clusters of welfare attitudes: an overall positive, overall critical, performance critical and role critical cluster. This multidimensional operationalization of citizens’ welfare attitudes might apply to institutional attitudes as well, and for instance, Wendt et al. (2010) and Missinne et al. (2013) have identified two dimensions of healthcare attitudes: preferences about the state’s role in organizing healthcare and the satisfaction with the healthcare system. These findings indicate that absolute and relative attitudes can form several combinations of healthcare evaluations and thus unveil new patterns of national variations.
Last, as well as being of empirical interest in themselves, measured characteristics at the individual or institutional level may constitute important controls when understanding national variations in healthcare evaluations. Arguably, it is more valuable to understand national differences after controlling for measurable characteristics, rather than at a ‘gross’ level of association. Trends over time in institutional attitudes may also provide an important diagnostic and thus our analysis allows us to compare attitudinal trends in Europe over 2002–2017. It might ordinarily be expected that trends over time vary in nature across countries, reflecting the dynamics of political contexts, welfare arrangements, or even compositional changes such as birth cohort churn. We take an exploratory approach to trends in absolute and relative measures of healthcare evaluation, commenting post-hoc on the emerging empirical patterns.
Data and methods
Data sources
The empirical analysis is based on individual-level data from rounds 1–8 of the European Social Survey (ESS) (see ESS, 2020), linked with country and year-level measures taken from the Global Health Observatory (GHO)’s data repository (see WHO, 2020, 2018). The ESS is a biennial repeated cross-sectional cross-national survey, of which our analysis covers 31 countries and approximately 342,000 individuals. Within our analysis, the GHO country-level indicators lead to 305 country–year observations on four different indicators between 2002 and 2017. The data is analysed with Stata software, version 16 (StataCorp, 2019), and with MLwiN (Rasbash et al., 2009), the latter implemented via the ‘runmlwin’ package (Leckie and Charlton, 2013).
While our data spans 31 countries across all European regions, not all countries provide data in each biennial survey round. Figure 1 indicates the data coverage by country and depicts descriptive trends over time in the two dependent variables in each country (as will be discussed in the section on country-level residuals in the fourth section). The country–year health system indicators collected from the GHO’s data repository are based on health-related statistics derived by GHO for the World Health Organization’s member states. Our analysis applies listwise deletion to ESS cases with missing data on any analytical variables. This reduces the dataset from 367,026 cases with data on at least some measures, to 342,236 cases with valid data on all measures. Data coverage by country, with trend lines depicting average value of dependent variables by country over time. Countries are organized into four geographical regions. Time trends are the best fitting cubic line within countries. Note: Residuals correspond to the random intercepts for models 1–4 on the ESS data as shown in Table 2.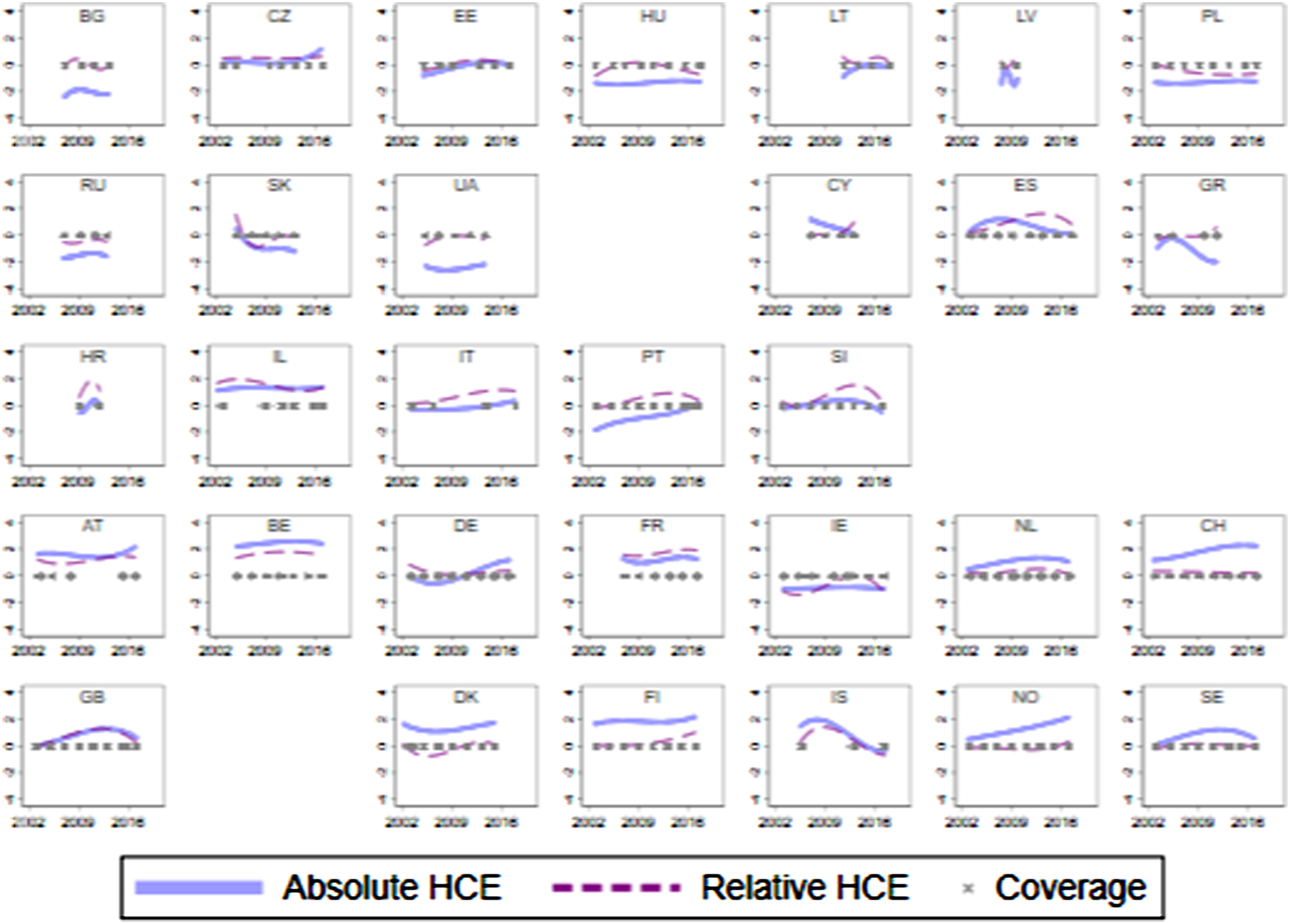
Variables
Dependent variables
For the analysis, we use two dependent variables that we call absolute and relative measures of healthcare attitudes which were treated as continuous in the analyses. The descriptive statistics for these items and for the variables used as independent and control variables in the analysis, can be found in Supplemental Table A1 (appendix). The former measures citizens’ perceptions towards their national health systems: respondents were asked to say what they think overall about the state of health services in their country nowadays on a ranked scale with 11 scale points options ranging from being extremely bad to extremely good. In our analyses, we code these scale points from −5 to 5.
The relative measure combines five different attitudinal indicators from the ESS survey that measures citizens’ evaluations on performance of society’s different institutions. We use this measure as a plausible way of indicating if respondents’ attitudes towards healthcare are relatively more positive or negative than their attitudes towards other institutions. The measure uses five survey questions in which people were asked to indicate on an 11-point Likert scale how satisfied they are with the present state of the economy in their country, the national government, the way democracy works, the state of education, and health services. To construct the relative measure, we took the respondent’s average across these five measures (each measure scaled from −5 to 5) and subtracted it from their response on the absolute attitude measure. 2 We stress that a ‘relative’ measure of this nature could in principle be constructed using a different combination of other measures and that our own choice was influenced by the coverage of attitudinal measures of institutional performance in the ESS. We believe it serves as a reliable and valid indicator of the extent to which views on healthcare are more or less positive compared to views on other institutions, because all of the component items are themselves validated instruments, and our results below suggest a level of ‘construct validity’ (that is, those scenarios where we find the relative measure differing from the absolute measure generally makes logical sense and hence the measure behaves as expected). Moreover, the items are designed to measure performance of societal systems (Thomassen, 2001; ESS, 2008). In future research, further alternative evaluations of constructing such a relative measure could be productive.
Independent variables – country-level
To analyse the relationship between citizens’ healthcare attitudes and country-level institutional arrangements of health systems, we chose two health system financing and two provision-related indicators to use in the models (see Supplemental Table A1, panel 2). We chose these four contextual factors as they represent health system characteristics commonly addressed in the literature (for example, Kohl and Wendt, 2004; Popic and Schneider, 2018; Wendt et al., 2010).
The measure of current total health expenditure (THE) captures the level of resources invested in healthcare and the financial capacity of the healthcare systems to provide care (Kohl and Wendt, 2004). THE is measured in $US per head of population by using purchasing power parity and the values were divided by 100 to scale them similarly as the other country-level variables. The indicator of private out-of-pocket payments as a percentage of THE reflects households’ healthcare related costs and financial burden (Popic and Schneider, 2018).
The provision of health services is connected to the production and delivery of health services (Kohl and Wendt, 2004), and we capture it with two health employment indicators. The number of nurses and doctors reflect the volume of health employment allocated to organizing health services (Kohl and Wendt, 2004; Wendt et al., 2010). The former is measured as the total number of nursing and midwifery personnel per 10,000 population and the latter as the total number of medical doctors per 10,000 population. All country-level independent variables are standardized to have a mean of zero and a standard deviation of one.
Independent variables – respondent-level
Our analysis also controls for individual-level measures of respondent characteristics (see Supplemental Table A1, panel 3) that are connected to citizens’ healthcare attitudes (for example, Footman et al., 2013; Schneider and Popic, 2018; Wendt et al., 2010; Missinne et al., 2013). Following previous studies, we control for age (quadratic form, to allow for a curvilinear relationship with age), gender (men having more positive evaluations than women), years of education (previous findings inconclusive), subjective income, residency area (often rural residents are more positive), subjective health, self-reported difficulties in daily activities, and six categories of employment status (often employed are the most negative). Our results largely concur with previous studies in the relationships between respondent-level characteristics and either of our measures of healthcare attitudes – for instance, we find a u-shaped relationship between age and absolute and relative healthcare attitudes: positive evaluations increase the younger or older the respondents are (see also Schneider and Popic, 2018; Borisova et al., 2017; Missinne et al., 2013). Also, we find that individuals with worse subjective health evaluate healthcare absolutely and relatively more negatively than individuals with better health (see also Popic and Schneider, 2018; Missinne et al., 2013; Wendt et al., 2010): Previous studies suggest that perceived financial strain and lower income associate with more negative healthcare evaluations (for example, Popic and Schneider, 2018; Wendt et al., 2010). We find that perceived lower subjective income relates to more negative absolute but more positive relative healthcare attitudes. We also controlled for an interaction between gender and education which reveals higher educated women being more negative towards healthcare.
Statistical analysis
We applied multilevel random effects models to summarise the influence of explanatory variables at the respondent- and country–year-level upon the attitudinal outcomes at the respondent level. The results presented below use a two-level random effects specification with individuals nested in countries. We used a random effects formulation for the cross-national data structure as this is a popular strategy for modelling cross-national survey data as it allows appropriate estimation of a combination of respondent-level and country-level explanatory variables. Our models also used fixed effects (coefficients are not expected to vary across countries) to capture the influence of time (a cubic trend for month of interview).
Sometimes a suggested approach is to analyse the ESS using random effects for both countries and interview rounds (for example, Schmidt-Catran and Fairbrother, 2016). We explored alternative hierarchical specifications including (i) a two-level model for individuals in country–year combinations; (ii) a three-level cross-classified model for individuals nested both in years and countries, and (iii) a four-level model with individuals nested in years, countries, and country–year combinations. Models for (iii) could not converge, and models using (i) and (ii) did not lead to any consequential differences in parameter estimates of interest. Accordingly, our two-level models used random intercepts to allow for significant variation in the attitudinal responses from country-to-country net of controls. Many of our models also considered a random slope parameter with other explanatory variables, to allow for the possibility that the relevant measure is associated with the outcomes differently to country-to-country net of other controls. Model results presented do not apply sampling design or population weights. Sensitivity analysis applying weights for the ESS sampling design showed no important differences in model results except that the significance of the country-level explanatory variables was diminished in the models using weights. ESS data may also be weighted by a country’s population size, but this is less common in analyses such as ours which control for respondent- and country-level variables and use country-level random effects. Moreover, sensitivity analyses using population weights suggest their impact would be limited, albeit they showed generally smaller national level patterns of difference. This might reflect that population weights in this context could inappropriately dampen the empirical patterns of difference between countries.
In preparatory analysis we considered several model specifications with different formulations of explanatory variables such as their functional form and possible interactions between them. The models we considered the most helpful for illustrating associations with healthcare evaluations, from which we present results, include null models with country-level random intercepts (models 1 and 2, for absolute and relative healthcare outcomes respectively, which provide insight on the gross level of national differences across countries); a ‘full’ model including main effects for all explanatory variables, random intercepts for countries and a random slopes terms for variations in the influence of income from country to country (models 3 and 4, for absolute and relative healthcare outcomes); and four permutations of intermediate models with the same specifications as models three and four except that we fit only one of the four country-level health system indicators (models 3a–d and 4a–d, presented in recognition of the risks of collinearity when fitting all four country-level measures in the full model). Two additional models discussed below (5 and 6) allow random slopes permitting the effect of time trends in attitudes to differ from country to country.
Results
Models with respondent- and country–year-level explanatory variables
Multilevel regression models predicting standardized measures of absolute and relative healthcare attitudes (models 1–4).
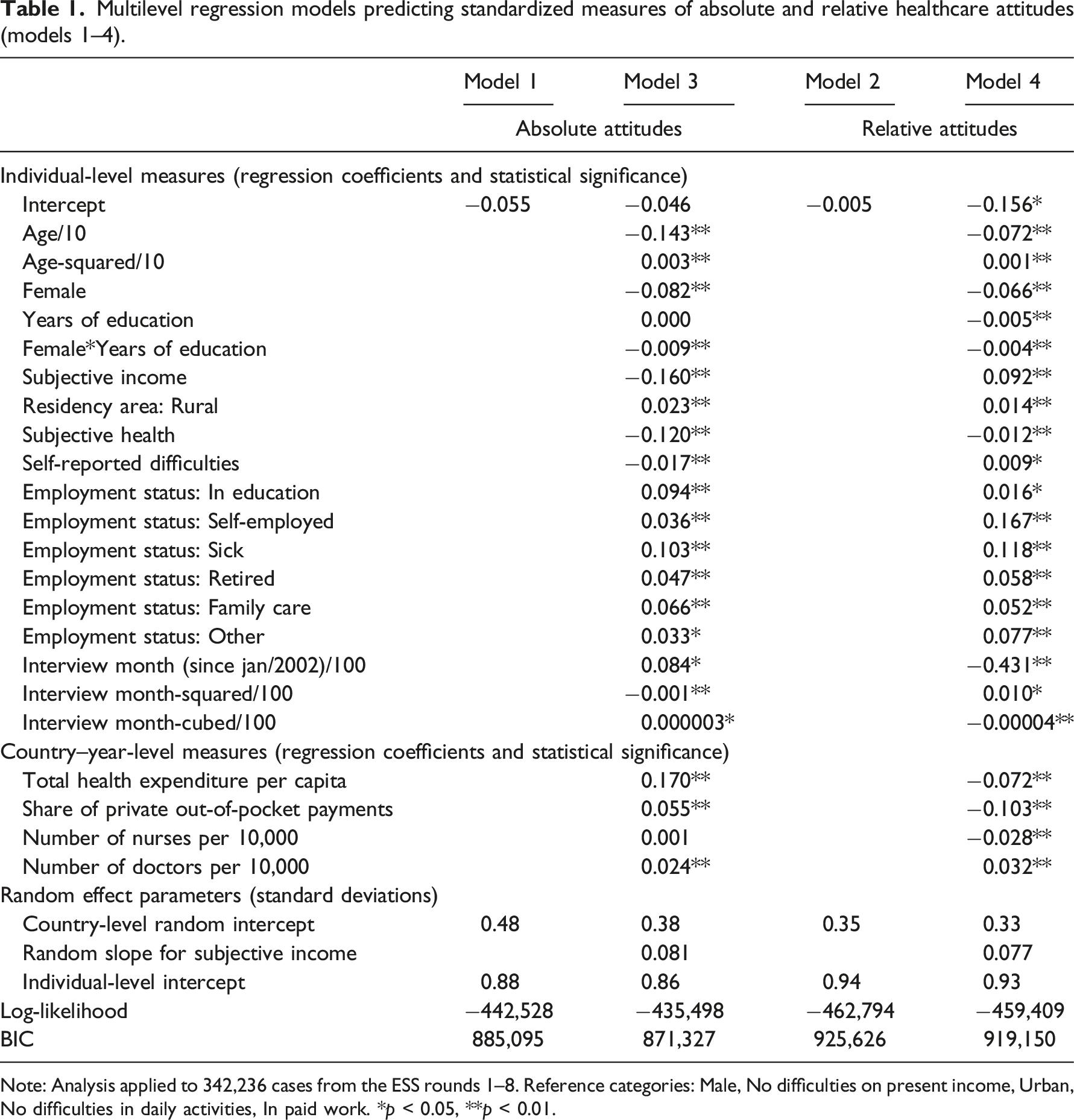
Note: Analysis applied to 342,236 cases from the ESS rounds 1–8. Reference categories: Male, No difficulties on present income, Urban, No difficulties in daily activities, In paid work. *p < 0.05, **p < 0.01.
Associations between country–year level variables and absolute and relative attitudes measures across different model specifications.
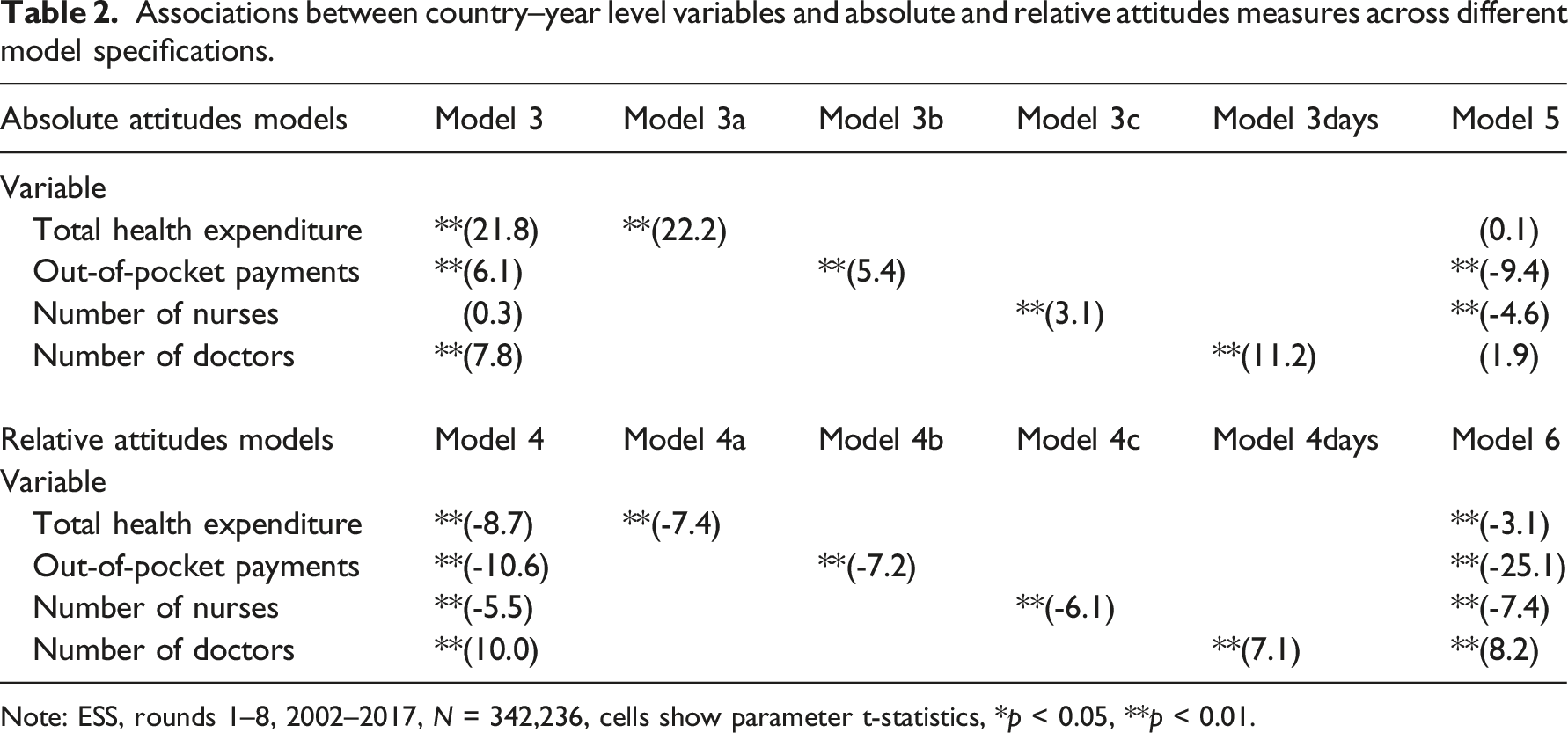
Note: ESS, rounds 1–8, 2002–2017, N = 342,236, cells show parameter t-statistics, *p < 0.05, **p < 0.01.
The absolute attitude models suggest that higher THE increases positive healthcare evaluations, however the opposite relationship applies to the relative attitude measure. Likewise, higher share of out-of-pocket payments increases positive evaluations in the absolute attitude models but decreases them in the relative attitude models. In the absolute attitude full model, the number of nurses is not significant, but in model 3c it is. These results suggest that a higher number of nurses is associated with less positive healthcare evaluations when those attitudes are assessed relative to attitudes about the performance of other national institutions. The parameter estimates of macro-level variables can be sensitive to small variations in empirical patterns at the macro-level (the moderate empirical correlations between three of the four measures could exacerbate this sensitivity – the average correlation between number of nurses, total and out-of-pocket expenditure is about 0.4, although there is only a weak correlation between these indicators and the number of doctors). Models 3a–3d and 4a–4d assess the consistency of these results in models not controlling for the other macro-level variables, and Table 2 suggests the parameters are robust to control for other macro-level characteristics.
Table 2, however, suggests other grounds for caution in describing these country–year-level parameter effects. In models 5 and 6, other model controls remain the same, but an additional random slope is allowed for the time trend, that is, allowing for the cubic effect of months to work differently across countries. As expected, adding this term improves the model fit but it also has a knock-on effect on the estimated parameters for the country–year-level explanatory variables, which change dramatically in their nature for the absolute attitudes measure (model 5 compared to model 3), while they follow the same pattern, but change in magnitude, for the relative attitudes measure (model 6 compared to model 4). Reflecting on these results, we believe the parameters in models 3 and 4 are more appropriate than those in models 5 and 6, since in the latter it might be unrealistic to disentangle the country–time trend from the country–year-level indicators. However, we recognise that alternative interpretations could favour the macro-level parameters from models 5 and 6.
Country-level residuals
Multilevel regression models assess robustly whether outcome patterns diverge from the European average for specific countries at either the gross descriptive level, or net of controls for other measures. In Figure 2 we communicate the country-level ‘empirical bayes’ residuals for the random intercepts within models 1 to 4. Broadly speaking the residuals can be interpreted as conservative estimates of the extent to which a particular country deviates from the average in its healthcare evaluations on the given measure, net of all other variables controlled for in the model (a positive residual in Figure 2 implies a more positive evaluation). Models one and two are null models whose residuals reflect country-level averages. Models 3 and 4 feature numerous other controls, including the country–year-level healthcare characteristics, thus highlighting other unexplained differences between countries. Random effects residuals at the country level using null and full models with absolute and relative healthcare evaluations. Note: As Figure 2.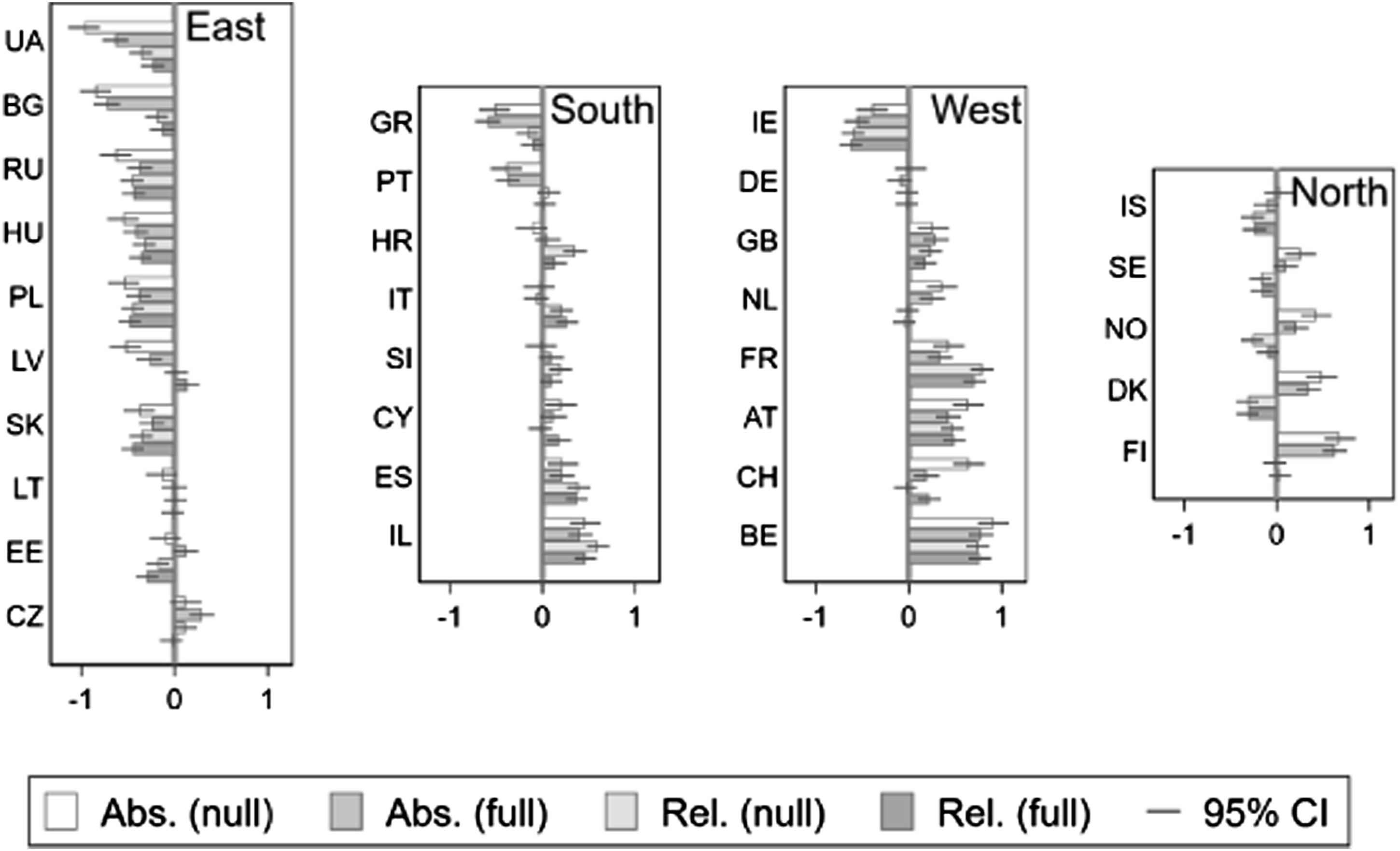
Figure 2 reveals several interesting features of national level variations in healthcare evaluations, including obvious tendencies towards regional variations, and differing patterns of absolute and relative attitudes. As the models used arithmetically standardised dependent variables, we can note that national differences are more pronounced when analysing differences in the absolute than in the relative measure (as the magnitude of the residuals tends to represent a larger fraction of the standard deviation of the dependent variable). The larger magnitudes among the absolute measure generally make regional and national patterns of difference easier to spot – however, as discussed above, the absolute measure might be inadequate for understanding national differences in institutional attitudes, suggesting in turn that the empirical literatures using absolute measures might potentially have exaggerated the scale of national differences.
Perhaps the most obvious feature of Figure 2 is the pattern of regional differences. The Eastern European countries consistently provide more negative evaluations according to both absolute and relative measures. Countries in the South, West and North generally have more positive attitudes albeit not without variations. Divergence between absolute and relative attitudes is pronounced in the Northern European countries but is less substantial in the other regions.
Figure 2 enables comparisons between the relative rankings of different countries by either measure. Some countries occupy positions that might deviate from health expenditure expectations. For example, Germany’s health spending is high, but the model residuals do not rank Germany as positively as we might expect given that resource. By contrast, in Israel health spending is relatively low, and we might have expected more negative healthcare evaluations compared to our results.
The most interesting change in national ranking relates to the different properties of the absolute and relative measures. Between countries, the ranking of relative measure seems more heterogeneous (see also Figure 1) and less strongly linked to regions. Especially, in the Nordic countries Iceland, Denmark, Sweden and Norway, people are relatively more negative towards healthcare than other institutions. In France, Belgium, Israel, Austria, Spain, the UK, and Switzerland, people are relatively more positive towards healthcare.
Within countries, we see a reduction in the magnitude of the residual term in the full model by comparison to the null model (adding controls for other measures diminishes any country-level disparity). A reduction typically arises due to adding the country-level variables. However, some countries diverge from that pattern: the residuals for these countries do not decline in magnitude, and may even increase, when moving to the corresponding full model. This suggests that healthcare evaluations within these countries are not associated with country-level healthcare characteristics as they are on average across Europe.
Figure 3 highlights the relationship between the residual magnitudes of the outlying countries (the vertical axis values are offset to assist display). Countries above the line of equality have larger residuals in null than full models, which is the common expectation (see also Figure 2). However, for countries below the line of equality, the magnitude of the residual estimate in the full model is just as, or more positive or negative than in the null model. For the absolute measure for instance, Ireland and Czechia have the largest non-standard change in their residuals. In Ireland, absolute attitude residuals are more negative net of controls, that is, compared to what they would be if predicted by country-level indicators – this may suggest worse evaluations even despite relatively more favourable institutional arrangements. In Czechia, attitudes are more positive net of controls, which might suggest better evaluations than would be warranted by healthcare characteristics alone. Magnitudes of random effects residuals at the country level, comparing null and full model results for the corresponding healthcare evaluation measure.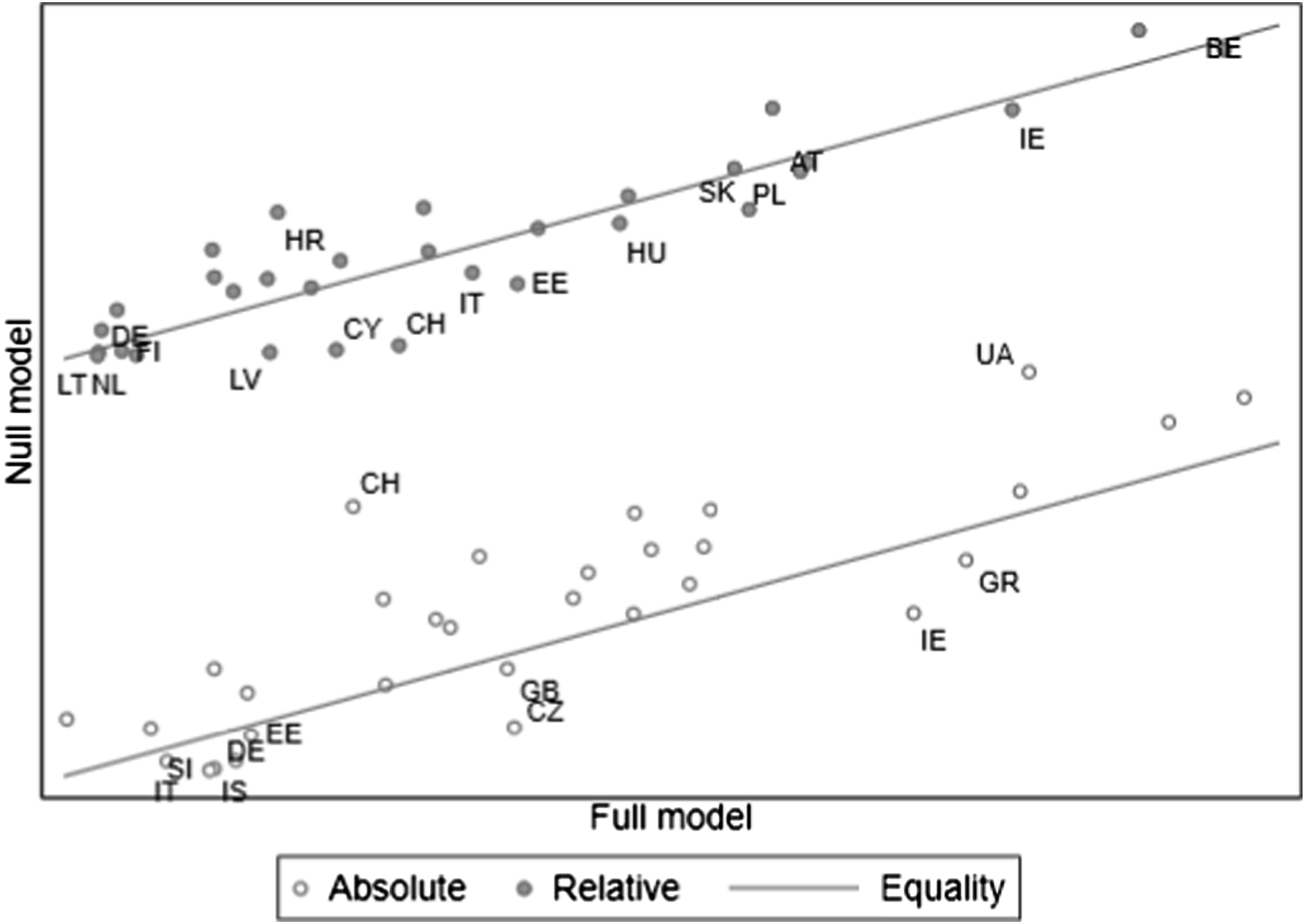
Our findings indicate five categories of Europeans’ healthcare attitudes which mimic an organizational typology used by Roosma et al. (2013, 2014) to classify countries according to patterns in welfare evaluations. Austria, Belgium, France, Israel, Spain, the UK, and Switzerland are the group of ‘overall positive’ countries in which healthcare attitudes are absolutely and relatively more positive than European average healthcare attitudes. However, in Bulgaria, Hungary, Ireland, Poland, Slovakia, Russia and Ukraine, citizens attitudes towards healthcare are ‘overall negative’ – more negative than average in both absolute and relative terms.
The third group are ‘relatively critical’ on healthcare referring to more positive absolute than relative healthcare attitudes. This may reflect disproportionately poor healthcare evaluations, but also generally quite positive attitudes towards societies’ institutions when citizens do not evaluate healthcare any differently. Only in Denmark are healthcare attitudes absolutely more positive and relatively more negative than average. In Czechia, Finland, Norway, and the Netherlands, healthcare attitudes are absolutely more positive but relatively average. In Sweden, Iceland, and Estonia, the absolute healthcare attitudes are European average but relatively more negative.
The fourth country group we call ‘absolutely critical’ in which relative healthcare attitudes are more positive than absolute attitudes meaning that citizens evaluate healthcare more positively than other institutions. In Italy, Croatia, Cyprus, and Slovenia, healthcare attitudes are absolutely average but relatively more positive whereas in Latvia, Greece, and Portugal, the absolute healthcare attitudes are more negative but relatively average. In addition, we recognize a fifth attitudinal group, overall average including Germany and Lithuania, in which both absolute and relative healthcare attitudes are average in the European context.
Conclusion and discussion
Based on earlier research, we expected to find differences in citizens’ healthcare evaluations in Europe (see Footman et al., 2013; Missinne et al., 2013; Mossialos, 1997; Schneider and Popic, 2018; Popic and Schneider, 2018). Our findings indicate that Western and Northern Europeans are absolutely more positive towards healthcare than Eastern Europeans whereas Western and Southern Europeans are often relatively more positive than Northern and Eastern Europeans, however, with regional differences being less clear cut. Mostly, Eastern Europeans are more negative, and Western Europeans more positive, across both dimensions, and Northern Europeans are absolutely more positive, but relatively more negative, towards their national healthcare. Southern Europeans’ views of their national health systems differ between countries in absolute terms, but in general their relative evaluations are more positive. Exceptions exist, such as Ireland whose citizens evaluate healthcare more negatively in either term. Our findings however seem consistent with those of Roosma et al. (2013, 2014) on the multidimensionality of welfare attitudes: we found a variety of circumstances across countries according to the two dimensions of absolute and relative attitudes. One possible interpretation of the different profiles between absolute and relative measures is that the relative measure diminishes the impact of the cultural or attitudinal climate of a country or region on healthcare evaluations. Consequently, the different properties of the two measures might suggest that cultural climate shapes Europeans’ evaluations of healthcare performance.
Previous studies reveal similar findings on country differences in absolute healthcare evaluations; Eastern Europeans are less satisfied compared to Western Europeans (Missinne et al., 2013; Schneider and Popic, 2018; Popic and Schneider, 2018). The East–West differences have been connected to distinct financial resources (Schneider and Popic, 2018; Popic and Schneider, 2018), health service supply (Popic and Schneider, 2018); outcomes (Missinne et al., 2013) and performance perceptions of health systems (Schneider and Popic, 2018). Our findings partly support the argument that health system structures explain attitudinal differences in healthcare evaluations between European countries.
Using a relative measure of healthcare evaluations demonstrates new patterns, however. As noticed, positive or negative absolute and relative healthcare evaluations sometimes concur at the national level, but the two patterns also diverge. Institutional structures of health systems are important in explaining absolute and relative healthcare attitudes but connect to the attitudes differently. For the health system characteristics, only the greater number of doctors indicated both more positive absolute and relative healthcare attitudes which earlier studies support (Borisova et al., 2017; Popic and Schneider, 2018; Wendt et al., 2010). Both the number of doctors and nurses relate to the general availability of healthcare providers, though our findings suggest that greater number of nurses connects to relatively more negative attitudes. The relationship between healthcare evaluations and health professionals other than doctors is less studied and thus we were interested in how the number of nurses relates to citizens’ attitudes as it has been associated with improved access to health services and patient satisfaction (Maier et al., 2017).
Also, we found that higher THE increases positive absolute healthcare attitudes, which supports earlier findings (Popic and Schneider, 2018; Kohl and Wendt, 2004; Mossialos, 1997). However, higher THE is linked to more negative relative attitudes. Moreover, previous findings suggest that greater out-of-pocket expenditure is connected to more negative healthcare evaluations (Borisova et al., 2017; Popic and Schneider, 2018), but our results indicate that it is associated with more negative relative and more positive absolute attitudes. These complex relationships with financing indicators may reflect several different mechanisms in shaping evaluations. Expenditure in any form might improve access or quality, thus increasing absolute evaluations, but also reflect an awareness of a greater burden of healthcare costs (see Popic and Schneider, 2018; Wendt et al., 2010), therefore reducing relative evaluations.
The cultural climates in European countries and regions might also explain the relationships between health system characteristics and the two attitudinal measures. The importance of THE and number of nurses in explaining relative attitudes might be smaller than expected because in countries with high THE and number of nurses, the cultural climate of a general confidence in societal institutions improves absolute but not relative evaluations. The same logic can be applied to out-of-pocket expenditure, if high public expenditure implies low private health spending (for example, OECD, 2019). The health system financing resources in Eastern and Southern European countries are inferior to the Northern and Western European systems which may also reflect a wider cultural climate. We already know that high-risk population groups are less satisfied with the welfare state performance in Southern and Eastern Europe (Blomberg et al., 2012). Furthermore, Southern and Eastern Europeans evaluate their welfare systems as less effective (Van Oorschot and Gugushvili, 2019), likewise Eastern Europeans evaluate their health systems as less effective (Schneider and Popic, 2018) than Western and Northern Europeans.
Furthermore, welfare characteristics might clarify the regional differences in Europeans’ healthcare evaluations. When analysing welfare attitudes in four European regions, Roosma and Van Oorschot (2017) noted that Northern and Western Europeans are more positive while Southern and especially Eastern Europeans are more negative towards the welfare state performance which they associate with different socio-economic circumstances. Also, van Oorschot and Meuleman (2012) find that Eastern and Southern Europeans show low satisfaction with welfare state performance. Generally, former communist countries of East-Central Europe differ from the Western countries in their welfare characteristics and outcomes (Fenger, 2007). Furthermore, the Northern European countries hold high institutional trust, whereas in Ireland and Eastern European countries institutional trust is low (Ervasti et al., 2019). Also, Footman et al. (2013) found that trust in political institutions increased healthcare satisfaction. These findings support our results of the impact of regional and country related cultural and attitudinal climate on evaluating societal institutions. Further research could explore the relationship between healthcare evaluations and institutional trust and other cultural climate related factors.
One enduring concern in cross-national attitudinal research is that response variations may just represent the cultural and attitudinal climate of different countries. In our application, citizens might put more value in their societal institutions in the ‘overall positive’ countries, whereas might be more sceptical in ‘overall negative’ countries. Still, this does not automatically mean that healthcare or other institutions function better or worse. However, for our results, any explanation of national differences based on cultural variations fits much better to the patterns in absolute attitudes than in relative attitudes (because the pattern of differences between countries in the absolute measure seems to align to differences that we might expect in terms of a general cultural or attitudinal climate, whereas the pattern of differences using the relative measure is less predictable). Our analysis is unable to provide an authoritative evaluation (which would benefit from explicit measures of ‘attitudinal climate’), but our initial results raise the possibility that a relative measure provides a better opportunity to capture ‘genuine’ variations in healthcare evaluations that diminish any impact of cultural or attitudinal climate than an analysis using the more traditional absolute attitudinal measure.
In summary, the comparison of absolute and relative attitudinal patterns presents interesting insights on formation of healthcare attitudes. It seems that in ‘absolutely critical’ countries, citizens evaluate other national institutions more negatively than healthcare – further research might investigate whether the health system characteristics in these countries make citizens view healthcare more positively. Equally, further research on the ‘relatively critical’ countries might offer new understanding about healthcare evaluations in those countries – mainly Nordic – where healthcare evaluations are relatively more negative than evaluations of other institutions. To conclude, our results show that together with the health system structures, healthcare evaluations are shaped by the cultural climate of how citizens’ regard the performance of national institutions of their own countries. Like welfare attitudes, healthcare evaluations are more than absolute for-or-againstattitudes (see Roosma et al., 2014) and therefore, the measure of relative healthcare attitudes helps to understand the regional and country specific differences in healthcare attitudes.
Supplemental Material
Supplemental Material - Attitudes toward healthcare performance in Europe, 2002–2017: How absolute and relative measures can reveal different patterns
Supplemental Material for Attitudes toward healthcare performance in Europe, 2002–2017: How absolute and relative measures can reveal different patterns by Iris Moolla and Paul Lambert in Journal of European Social Policy
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.