
Abstract
Many countries have been working on revising their long-term care (LTC) policies to meet the increasing demand for care. Generally, little attention is paid to the potential (unintended) consequences of LTC policies for inequality among care users or informal caregivers. Saraceno previously explicitly argued that differences in care use and provision depend on the type of LTC policy, and that policies with contrasting consequences for inequality can be implemented at the same time. We call upon future research to empirically test the impact of different types of LTC policies on socio-economic inequalities in care. To stimulate and facilitate such research, our aims are to outline theoretical arguments for the differential impact of LTC policies on socio-economic inequalities in care and to create macro-level indicators for different types of supportive LTC policies in European countries over time. Our study’s research question is: Can we find and capture different dimensions of LTC policies in macro-level indicators that are comparable over countries and time? In particular, we focus on supported familialism (for example, informal caregiver support), supported defamilialization through the market (for example, in-cash benefits for care users), and defamilialization through public provision (for example, availability of beds in residential care). Besides a summary of the literature on LTC policies and how they may affect socio-economic inequalities in care, we outline our search process for macro-level LTC indicators and present descriptive information on the different types of LTC policies and their correlations. We discuss the difficulties that arise when translating theoretical insights about different types of LTC policies into high-quality measures for many countries and time points.
Keywords
Introduction
In this article, we set out our call for empirical research on the impact of different types of long-term care (LTC) policies on socio-economic inequalities in care, which is a relevant though overlooked topic in the literature on LTC policies. In order to stimulate and facilitate such empirical research, this contribution aims to provide two types of input: (a) theoretical arguments as to why different types of LTC policies may have diverse impacts on socio-economic inequality in care, and (b) a description of theoretically-based, macro-level indicators of diverse types of supportive LTC policies in European countries over time.
Our study’s background lies in the observation that governments in ageing societies are now grappling with the issue of long-term care. Projected increases in disability mean that many countries now face significant challenges in meeting the growing care needs of an ageing population (Colombo et al., 2011). An increasing demand for informal care is therefore expected. Many countries have revised their LTC policies to meet this increasing demand for care (Fernandez et al., 2016), for instance by scaling back on formal care and placing a stronger emphasis on informal care. Because of the strong focus on LTC sustainability, typically little attention is paid to the potential (unintended) consequences of LTC policies leading to inequality among care users or informal caregivers. An open question for future research is thus how key features of LTC systems (for example, cash-for-care policies or public provision of home care) may exacerbate or reduce socio-economic inequalities in care received by and given to older adults.
The answer to this question is societally relevant – as policy solutions in one domain may simultaneously have undesirable effects in another – but also scientifically relevant. It may explain mixed empirical evidence in research on socio-economic differences in informal care use or provision, for which limited evidence exists. While some research finds that, across Europe, those in lower socio-economic status (SES) groups are more likely to receive informal (Broese Van Groenou et al., 2006; Lera et al., 2021; Vlachantoni et al., 2015), formal (Rodriguez, 2014), or mixed care (Floridi et al., 2021), other studies find that those in higher-SES groups report higher use of both informal (Bakx et al., 2015; Rodriguez, 2014) and formal care (Albertini and Pavolini, 2017; Lera et al., 2021). The conflicting evidence has been partly attributed to differences in the SES indicators used, such as income versus wealth (Rodrigues et al., 2018), but other scholars argue that socio-economic inequalities in care use play out differently across different LTC systems (Albertini and Pavolini, 2017). More particularly, Saraceno (2016) argued that differences in care use and provision depend on the type of LTC policy. Certain LTC policies – even though they are designed to be supportive in one way or another – can be argued to augment socio-economic inequalities in care use and caregiving, whereas others are expected to reduce inequality (Rostgaard and Szebehely, 2012). Policies with contrasting consequences for inequality can be implemented at the same time (Saraceno, 2016). It is therefore essential to move beyond comparisons of groups (or typologies) of countries (as in for example, Albertini and Pavolini, 2017; Broese Van Groenou et al., 2006; Carrieri et al., 2017; Fischer et al., 2021; Rostgaard and Szebehely, 2012). Such an approach was used in a recent comparative analysis of welfare systems in Europe which showed that social care policies are characterized by coexisting and overlapping regimes and calling for a greater focus on specific policy areas (Bertin et al., 2021). Hence, following the theoretical contribution of Saraceno (2016), we argue that it is important to use more fine-grained distinctions of familialism and defamilialization in LTC policies in order to fully understand the impact of LTC on socio-economic inequalities in care use and informal care provision.
To encourage and facilitate future research on the impact of LTC indicators on inequalities in care use and informal care provision, we not only elaborate on the theoretical arguments underpinning the expectation of differential impacts of different types of LTC policies, but also create theoretically inspired, macro-level indicators for different types of supportive LTC policies in European countries over time. Future research could then combine these indicators with large-scale, individual-level, country-comparative datasets (for example, SHARE) to statistically test the theoretical claim that different types of LTC policies have differential impacts on socio-economic inequalities in care use and informal caregiving. Compared to already existing LTC policy collections, the macro-level database needed for this endeavour should be different in two respects. First, we need single indicators rather than typologies (as in the ANCIEN project: Kraus et al., 2010) to account for the fact that different types of support policies can be implemented simultaneously, but have contrasting effects (Saraceno and Keck, 2011). Second, we need continuous measurements rather than categorical typologies (see Saraceno, 2016) to facilitate large-scale country-comparative studies using multilevel analysis techniques. The research question in this contribution can be summarized as: Can we find and capture different dimensions of supportive LTC policies in macro-level indicators that are comparable over countries and time?
In the remainder of this contribution, we will summarize the literature on LTC policies and outline theoretical ideas on how LTC policies may affect socio-economic inequality in care; in doing so, we will stress the importance of distinguishing between different types of supportive LTC policies as they may have complementary as well as contrasting effects on socio-economic inequality. Furthermore, we will explain our search process for the macro-level LTC indicators and present descriptive information on the different types of LTC policies and their correlations. We end with a conclusion and discussion on the importance, usability and validity of the LTC indicators.
Theoretical background
Since Esping-Andersen’s (1990) seminal work identified three types of welfare states: liberal (Anglo-Saxon countries), conservative (continental Europe and Japan) and social democratic (Scandinavian countries), many scholars have argued for a more nuanced typology, particularly one that includes greater consideration of gender relations and the family in social welfare (Bambra, 2004, 2007; Leitner, 2003; Orloff, 1993). Feminist scholars have led the way in revising the typologies created by Esping-Andersen according to the extent to which welfare state arrangements facilitate women’s autonomy and economic independence from the family (Bambra, 2004, 2007). For example, Bambra (2004) created a gender-sensitive defamilialization index to capture the relationship between women, the state and the family based on measures such as the female labour participation rate, maternity leave compensation (that is the percentage of normal pay for the first 12 weeks), and the average female wage (Bambra, 2004). Using this index, for example, Bambra (2004) clustered countries into low, medium and high defamilialization groups; however, such groupings showed strong similarities with Esping-Andersen’s (1990, 1999) initial three-fold welfare state typology.
Bambra’s work focused on one of the two key interpretations of defamilialization: one that is more women focused (Bambra, 2004, 2007), while the other is more care focused (Leitner, 2003). In an influential article, Leitner (2003) classified welfare states according to whether policies are familialistic (encourage either childcare or elder care), or de-familializing (assume paid work by individuals of working age and care outside the family through intervention by the state). Building on earlier work by Leitner (2003) and others, Saraceno (2016) further developed the familialism concept by arguing that a distinction between familialism and defamilialization is not completely satisfactory because the kinds of LTC policies that fit within each of these views may have different consequences for the behaviour of care users and caregivers, as well as for the gender and socio-economic inequalities that may arrive from these LTC policies. She distinguished five conceptual policy types. Familialism by default refers to a policy context in which the state does not offer publicly provided arrangements to take over or support family care, assuming the family will care for those who need help. Prescribed familialism refers to a situation with laws obliging family to care or to pay for care needed by their family members. It is therefore an active way to promote (prescribe) family care. Supported familialism occurs when policies are aimed at supporting family caregivers. As with the previous two types of familialism, the basic assumption is that the family, and not the state, is the main provider of care. However, supported familialism policies acknowledge that care provision often ends up on the shoulders of women, which conflicts with policy aims encouraging greater female labour market participation and gender equality. Supported familialism aims to facilitate the combination of care and work. Defamilialization reflects the belief that the state should be the principle responsible actor in care provision, so that care users can autonomously decide how to meet their care needs without being dependent on family members. There are two ways to arrange defamilialization. Supported defamilialization through the market implies that care users receive in-cash benefits to buy their own care services on the market. Defamilialization through public provision implies that policies directly provide public care that is available to those in need of care.
Out of these five policy types distinguished by Saraceno (2016), the latter three can be described as supportive policies, meaning that the state actively supports families, either by providing in-kind or in-cash LTC services or by facilitating or helping them to provide care. In this contribution, we focus on the three supportive LTC policy types (that is, supported familialism, supported defamilialization through the market and defamilialization through public provision). We argue that supportive LTC policy types are especially interesting to study because – due to their supportive nature – one could intuitively think that they have positive outcomes for families. However, that may not be the case for the unintended consequences of some of those supportive policy types. We would like to stress two important distinctions we see between these three supportive LTC policy types, which may have theoretical consequences for the effects of LTC policies on the SES gradient in care use and provision. First, supported familialism is targeted to informal caregivers, whereas both types of defamilialization are targeted to care users. Of course, policies that benefit care users may indirectly also affect caregivers and vice versa (indirect effects). For instance, if care users receive generous public care, efforts of their informal caregivers may be relieved; or if informal caregivers are well supported, they may be better able to continue providing care and doing so at a high-quality level, which benefits the care user too. The trickle-down effects are not perfect, however. Mechanisms driving the use of informal care are in part different from those that drive the provision of formal care (for example, Geerts and Van Den Bosch, 2012; Broese Van Groenou and De Boer, 2016). Therefore, distinguishing the target group of a certain LTC policy helps us to understand who is likely to be affected the most by the support policy. Second, the two types of defamilialization differ from each other by the channels through which they operate: via monetary support that can be exchanged for care on the market (in-cash) versus via direct public care provided, organized and paid for by the state (in-kind). We acknowledge that our distinctions based on the receiver (caregiver or care user) and form (in-cash or in-kind) is to some extent simplistic. Especially regarding the role of monetary support, more refined interpretations can be found in the literature. Saraceno and Keck (2011), for instance, argue that the link between monetary support to care users and policy type depends on the specific requirements that come with the monetary allowances. They argue that if care users are obliged to use the monetary transfer to buy services in a state-regulated market, it may in practice be an alternative form of defamilialization through public provision rather than supported defamilialization through the market, at least to the extent that liberal market options are not available. If monetary allowances come without any requirement on how to spend it, they argue that it is sometimes not even a matter of defamilialization, but a form of supported familialism. This would be the case if care users use the money to compensate their informal caregiver or – in the case of spousal care – to integrate the allowance in the family budget. However, as cash benefits aim to enhance the autonomy of the care user, we primarily interpret monetary support to care users as a form of defamilialization.
The main theoretical proposition we want to elaborate on in this contribution to stimulate future research is that different types of supportive LTC policies may affect socio-economic inequalities in care use and informal caregiving in opposite directions. Let us suppose that, on average, it is individuals in lower-SES groups who are more likely to use and provide informal care. If there is a strong level of supported familialism, which is targeted to caregivers to facilitate their caregiving role, ‘typical’ caregivers will be most responsive to these policies and thus start to provide more care. As a result, socio-economic inequalities in informal caregiving are likely to increase with more generous supported familialism policies. The greater responsiveness to supported familialism policies among lower-SES informal caregivers indirectly affects the use of informal care among their family members. Consequently, socio-economic inequalities in informal care use are also likely to increase with higher levels of supported familialism. In contexts with an emphasis on supported defamilialization through the market, that is in contexts where people are expected to buy care on the market, individuals in lower-SES groups may be disadvantaged (despite cash-for-care allowances) compared to individuals in higher-SES groups because of information asymmetry or lack of negotiating power, both needed to find one’s way in a liberal care market. This is for instance the case in Italy where individuals with higher educational attainment and in receipt of a care allowance are more likely to employ migrant care workers in comparison to their less educated counterparts (Barbabella et al., 2016). Moreover, in-cash benefits provided through public LTC may not be sufficient to buy care of the same amount or quality as that available to higher-SES individuals given their greater purchasing power. As a result, compared to higher-SES groups, lower-SES groups may become more dependent on informal care, directly increasing its use and indirectly its provision. Hence, socio-economic inequalities in care use and informal caregiving are likely to increase with more generous supported defamilialization through the market policies. In contrast, with LTC policies focusing on defamilialization through public provision, that is if publicly financed and regulated services are largely available, all SES groups will be more likely to rely on these services to meet care demands and to combine different care sources according to specific needs. In addition, the groups that were overrepresented among the informal caregivers are no longer obliged to provide care. Therefore, socio-economic inequalities in care use and informal caregiving are likely to decrease with more generous defamilialization through public provision policies.
Methods
We set out to find and capture different dimensions of LTC policies in macro-level indicators that are comparable over countries and time. As our ultimate goal is to fuel future empirical macro–micro studies that assess the impact of several types of supportive LTC policies on socio-economic inequalities in care use and informal caregiving, certain conditions must be met. First, the indicators must be quantifiable, meaning that we went beyond (single country or small-scale comparative) descriptions of the policy context (Saraceno, 2016). Second, the indicators needed to be theoretically distinguishable, so that they can be analysed simultaneously. As such, we expanded on earlier work that collected a range of policy indicators capturing different dimensions of care systems in several European countries and regions (Brugiavini et al., 2017; Glaser et al., 2013; Schmid et al., 2012; for regional indicators see Wagner and Brandt, 2018; Deindl and Brandt, 2019). Third, the indicators should be available for many countries (or regions) and years to warrant enough variation at higher levels of analysis to allow for statistical multilevel analyses. We strived to cover the countries and years that match the data collected in SHARE (Survey of Health, Ageing and Retirement in Europe, www.share-project.org) (Börsch-Supan et al., 2013), which provides country-comparative, individual-level panel data on care use and provision, among other things.
Summary overview of supportive LTC policy types with their distinctive features.
Second, we performed an extensive and systematic search in a variety of existing databases and datasets, including Multilinks Intergenerational Policy Indicators, Eurostat, OECD, Mutual Information Systems on Social Protection (MISSOC), European Quality of Life Survey, European Social Values Survey, and relevant publications on LTC policies in multiple countries (Courtin et al., 2014). Our search was not limited to information on LTC, but also included key features of the population, economy, pension and health insurance and cultural attitudes as well. We set out to cover information for 27 OECD countries: Austria, Belgium, Bulgaria, Czech Republic, Denmark, Estonia, Finland, France, Germany, Greece, Hungary, Ireland, Italy, Latvia, Lithuania, Luxembourg, Netherlands, Poland, Portugal, Romania, Slovakia, Slovenia, Spain, Sweden, Switzerland, UK and Japan. We searched within the time range from 2004 to 2018, although data from 1993 were also included for given indicators as many sources began data measurement in this year.
In the third step, we created composite measures for each of the three LTC policy types by selecting indicators from the broad macro-level database. We strongly followed a theory-based approach. Thus, for an indicator to be selected, it was crucial that the indicator unambiguously referred to a particular type of LTC support policy, which disregarded several available indicators. Furthermore, we balanced our selection of indicators based on their measurement validity, the ability to quantify the information, and their availability in as many countries and years as possible to match individual-level SHARE data. We created the following indices for each of the three LTC policy indicators.
Second, cash benefits to caregivers was a dichotomous measure indicating whether public cash-for-care payments existed that were paid to the caregiver. It therefore represented financial support directly paid to the caregiver. The measure was available for 27 countries in the years 2004 and 2009. This and the following two indicators were based on the Multilinks Intergenerational Policy database.
Third, in addition to the previous indicator, the cash benefits to caregivers’ index differentiated eligibility criteria or restrictions in use as well as levels of monetary allowances. The index was based on whether or not a country had policies that pay in-cash benefits to informal caregivers (1 = yes, 0 = no), whether formal regulations such as contracts or verification of costs must be met in order to receive these benefits (1 = no, 0 = yes), and the minimum and maximum amount of money that was paid to the informal caregivers. The minimum and maximum amount were corrected for price level indices (for actual individual consumption of the corresponding year with EU28 set to 100). Subsequently, the minimum and maximum amounts were separately categorized as low (2/3 of the median allowance of all countries with allowances or lower), medium (between 2/3 and 1 1/3 of the median allowance), and high (1 1/3 of the median or higher). The final score on the amounts of the monetary allowance was based on the highest score of the minimum and maximum amount (2 = high, 1 = medium, 0 = low). The index was the sum score of the three elements and ranged from 0 through to 4 with 0 referring to countries without cash benefits and four referring to countries with the most generous forms of cash benefits. The measure was available for 20 countries in 2004 and 21 countries in 2009 and was once again based on the Multilinks Intergenerational Policy database.
The second indicator reflected the relative number of formal LTC workers. Formal long-term care workers provide care to long-term care recipients at home or in long-term care institutions (other than hospitals). Nurses as well as personal care workers who are not qualified or certified as nurses were considered. The measure was available for 7–14 countries in many years between 2003 and 2018 and was based on data from the OECD. As with the indicator for LTC beds above, it is assumed that it captures those working in largely publicly subsidized facilities and services.
Results: LTC indicators
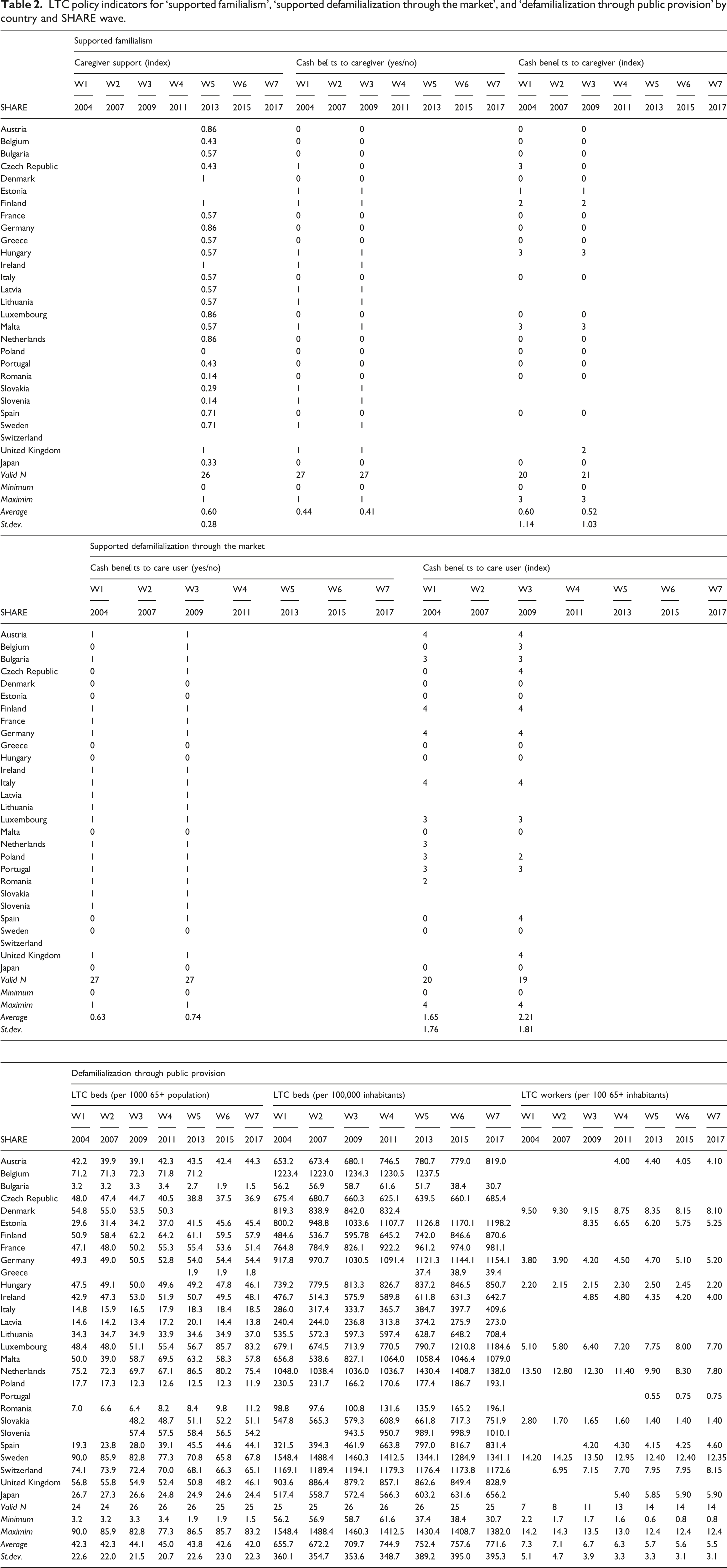
LTC policy indicators for ‘supported familialism’, ‘supported defamilialization through the market’, and ‘defamilialization through public provision’ by country and SHARE wave.
Distribution of LTC indicators over countries and time
Supported familialism appeared to be relatively high in Scandinavian countries as well as in some Northern and Western European countries (UK, Ireland, the Netherlands, Germany, Luxembourg, Austria) as far as (mostly non-monetary) caregiver support was concerned (Figure 1). Monetary benefits to caregivers were more common in Eastern European countries, next to Scandinavian countries (Figure 2); they hardly changed between 2004 and 2009. Supported familialism: caregiver support index by country, 2013. Supported familialism: cash benefits for caregiver by country (yes/no), 2009. Note: Countries without data are in grey.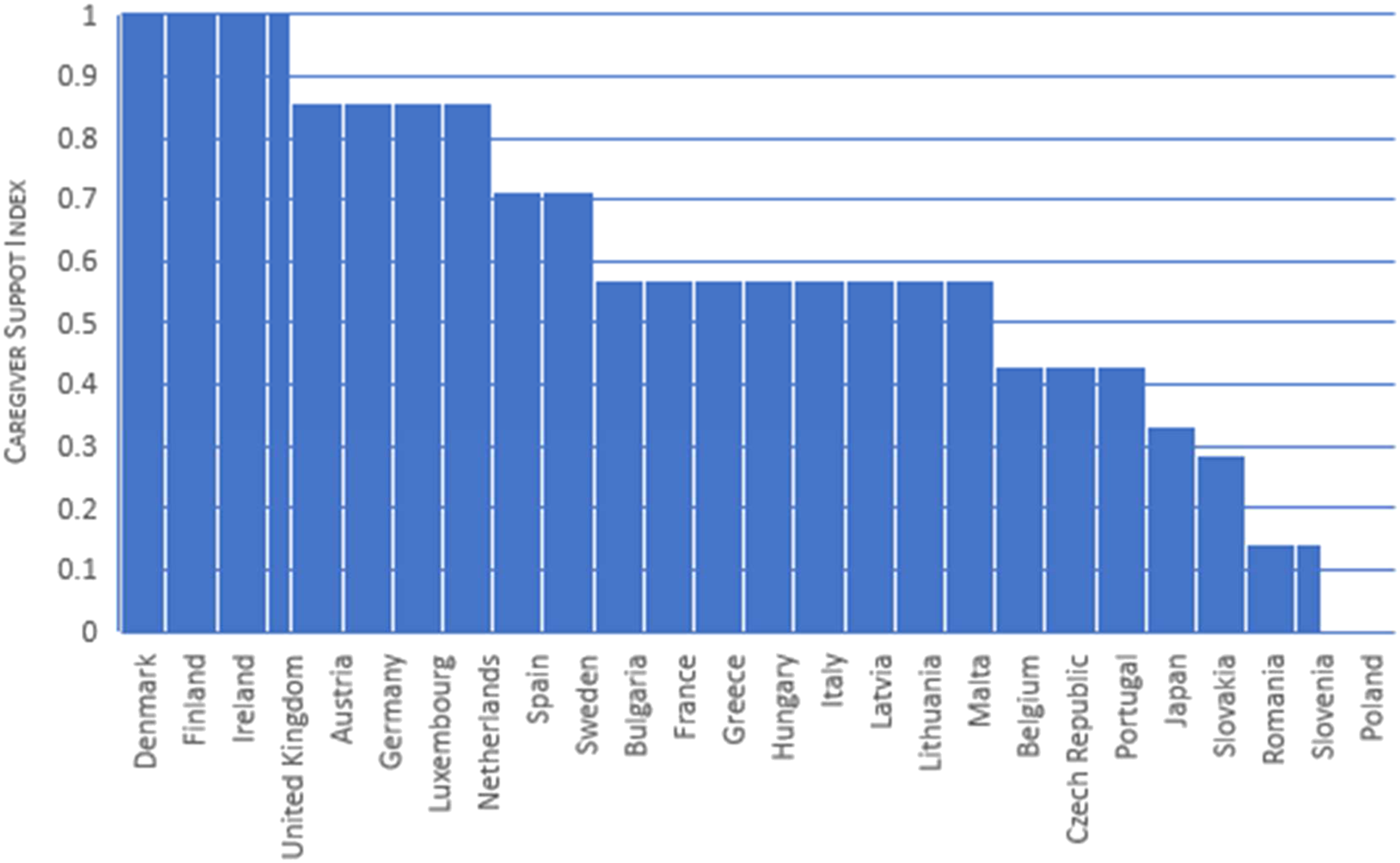
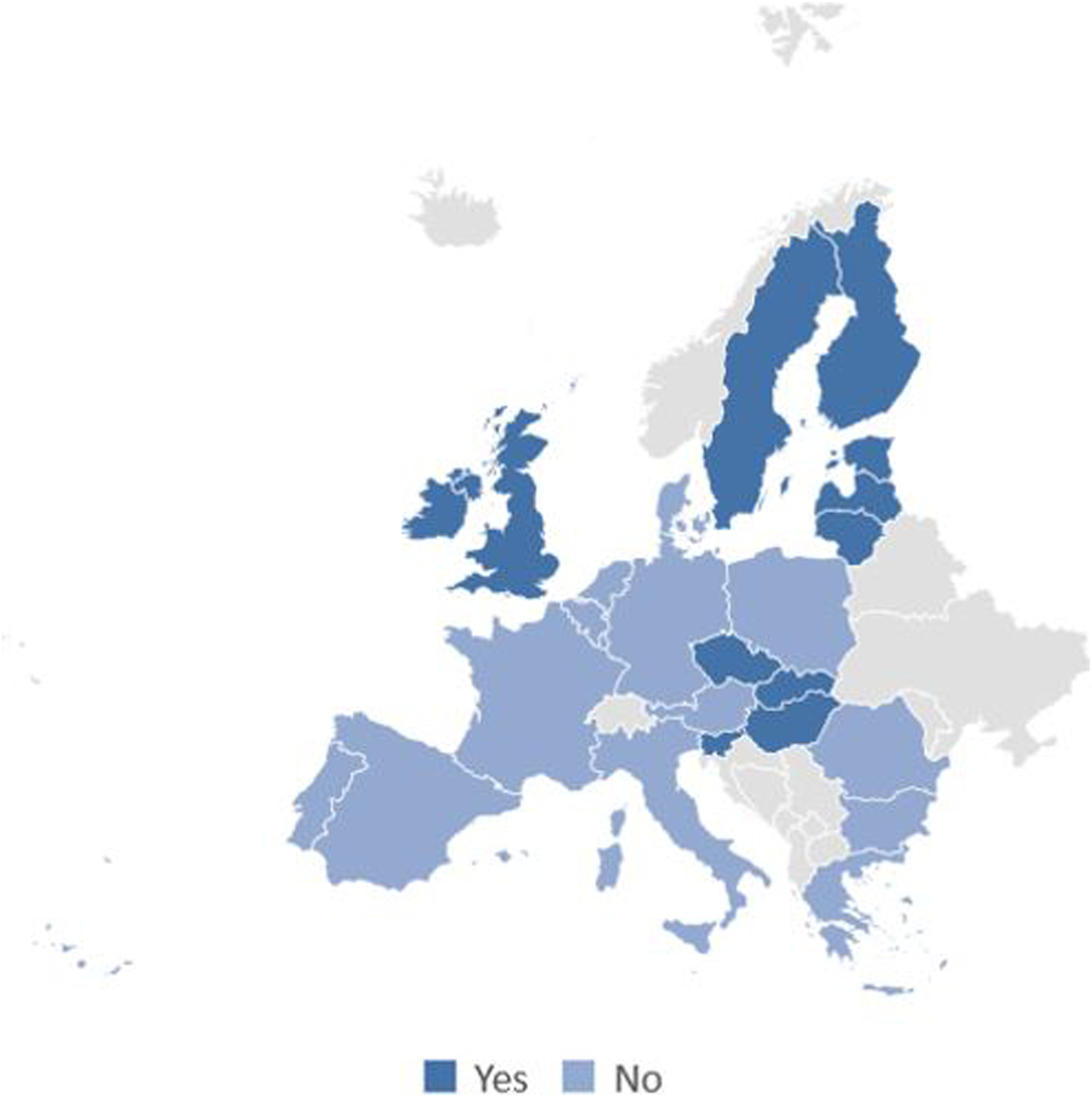
With respect to supported defamilialization through the market, we found that cash benefits to care users were implemented in 75% of the OECD countries on which we had data and were thus more common than cash benefits to caregivers (Figure 3). Countries in which supported defamilialization through the market was best developed (indicated by highest index score) were scattered around Europe, with examples in the north (Finland), south (Italy, Spain), east (Czech Republic), and west (Austria, Germany, UK) (Table 2). Hardly any change was observed between 2004 and 2009. Supported defamilialization through the market: cash benefits for care users (yes/no) by country, 2009. Note: Countries without data are in grey.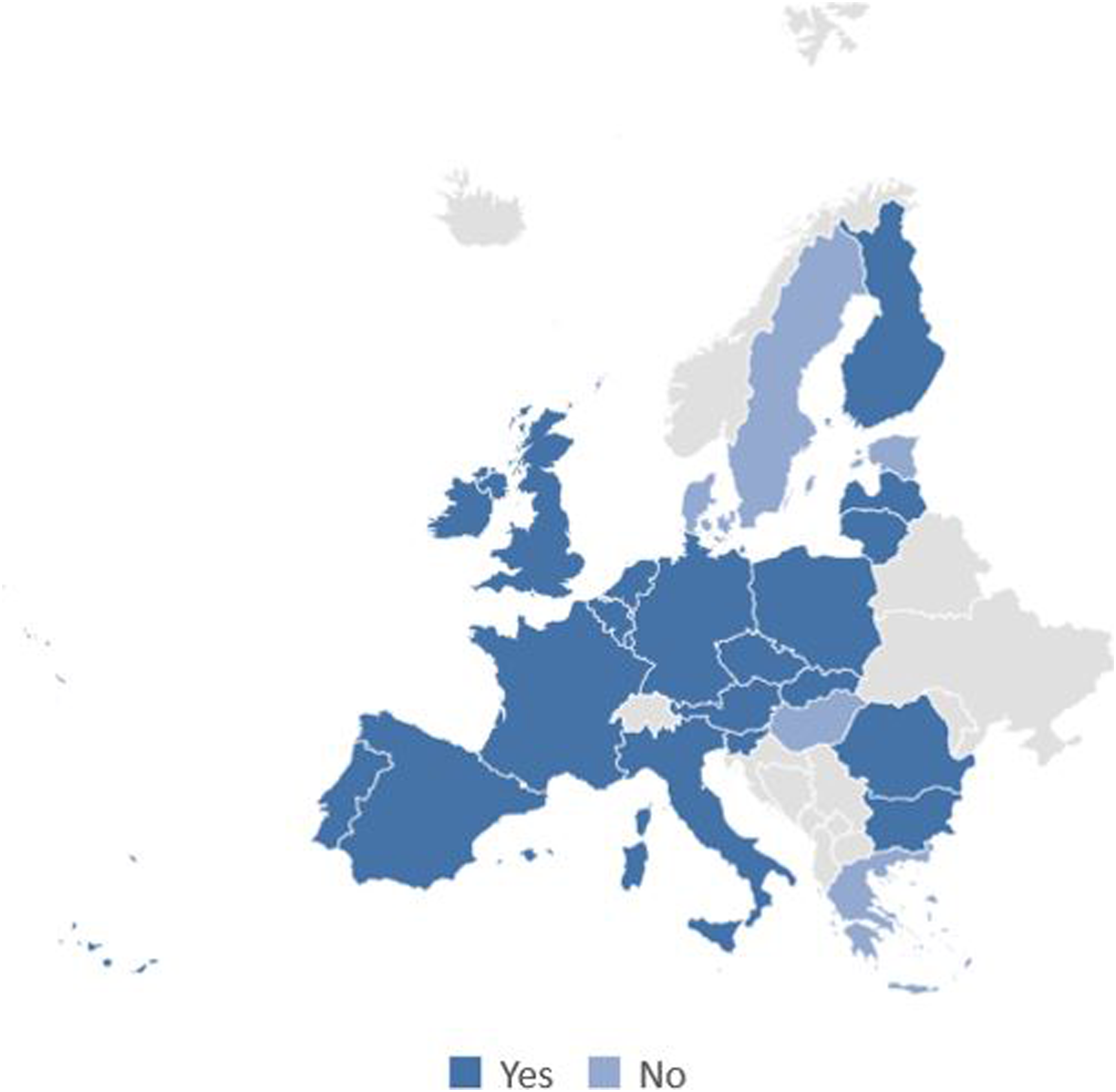
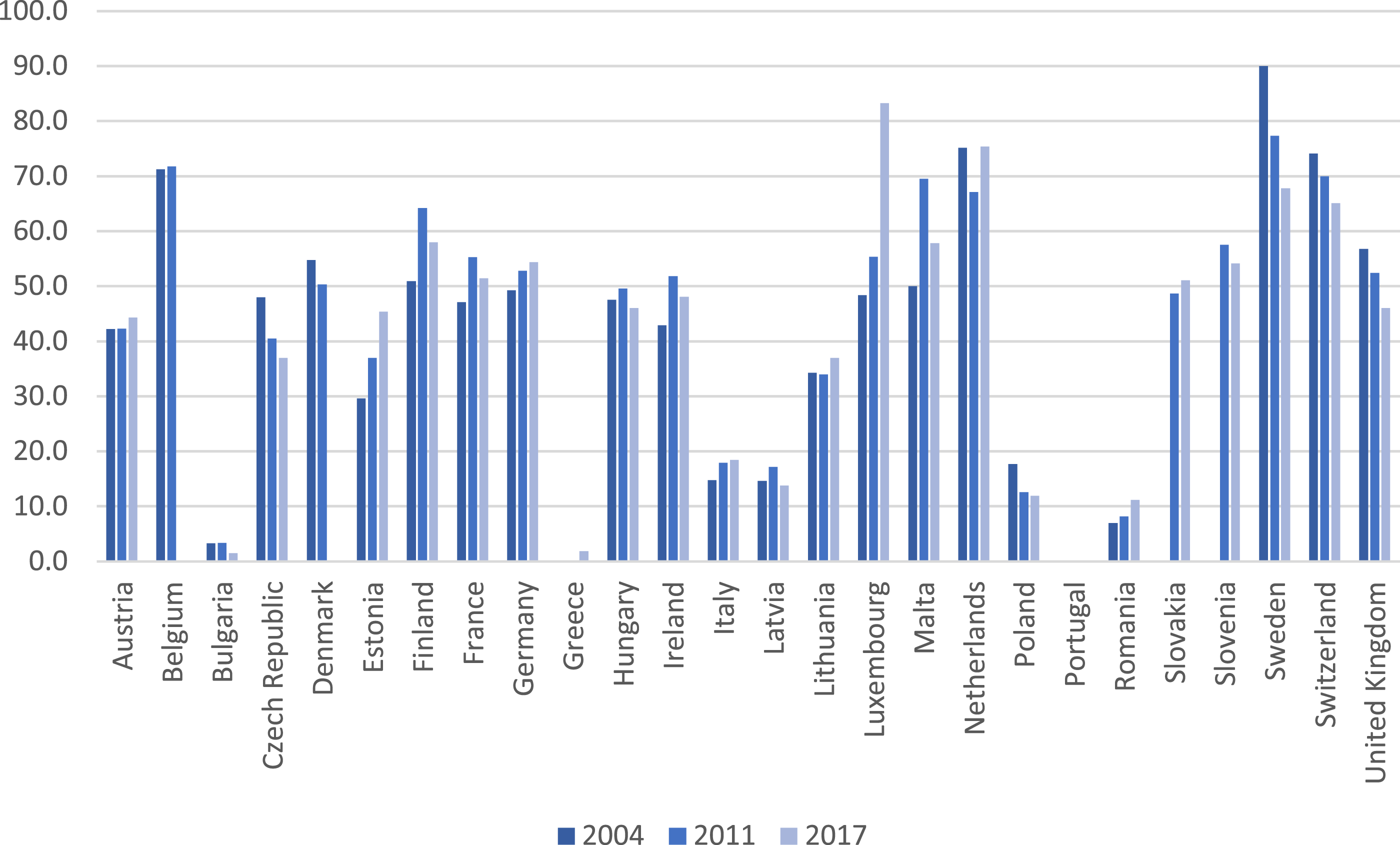
Switzerland, Sweden, the Netherlands and Luxembourg had high levels of defamilialization through public provision, whereas levels were generally low in Eastern and Southern European countries (Figure 4). There was no common trend in public provision between 2004 and 2017 (Figure 5): some countries had witnessed a (strong) increase, whereas others had witnessed a (strong) decrease. Defamilialization through public provision: LTC beds per 1000 65+ population by country, 2016–2017. Defamilialization through public provision: trends in LTC beds per 1000 65+ population by country, 2004–2017.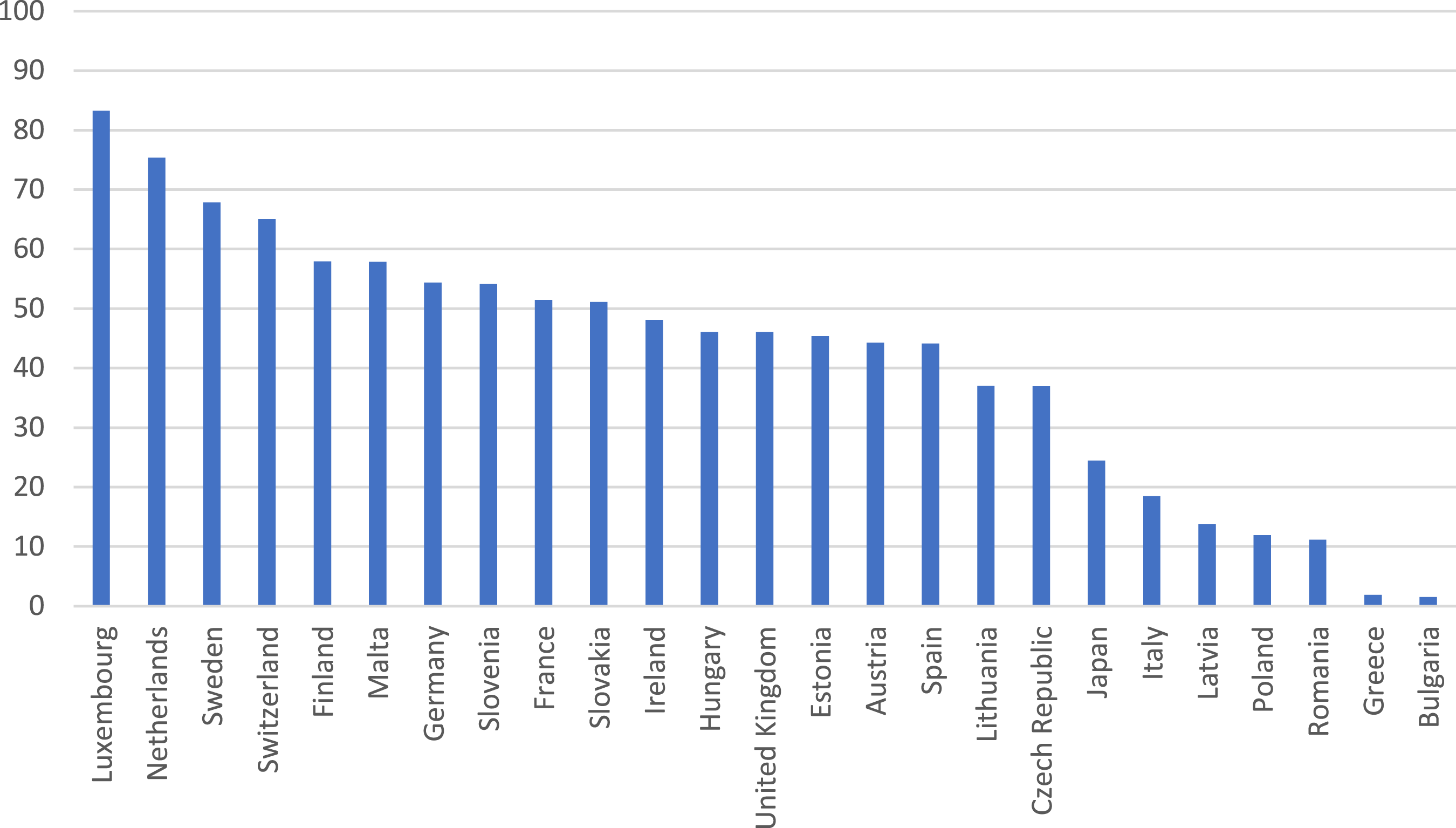
Association between types of LTC policies
As argued before, the three different types of LTC policies can be implemented in a country at the same time, while they are expected to have contradicting effects on socio-economic inequalities in care use and provision. In this section, we describe to what extent indicators of the different types of LTC policies were associated.
First, supported familialism was higher in countries without (0.63) than with (0.59) supported defamilialization through the market, though a T-test confirmed that this seemingly negative association was non-significant (t = 0.26, df = 24, p = 0.80). Second, a clearly positive association existed between supported familialism and defamilialization through public provision (see Figure 6): countries that scored high on caregiver support tended to score high on the number of LTC beds as well (r = 0.43, p = 0.04). This result underscores the importance of separating the two types of LTC policies as they were argued to have opposite effects on socio-economic inequalities in care use and provision. Third, a negative, but non-significant, association existed between defamilialization through public provision and through the market (40 vs 51 LTC beds per 1000 population in 2009–2010 in countries with and without cash benefits to care users in 2009 respectively; t = 1.07, df = 23, p = 0.30). Association between supported familialism (caregiver support index, 2012) and defamilialization through public provision (LTC beds per 1000 65+ population, 2012–2013).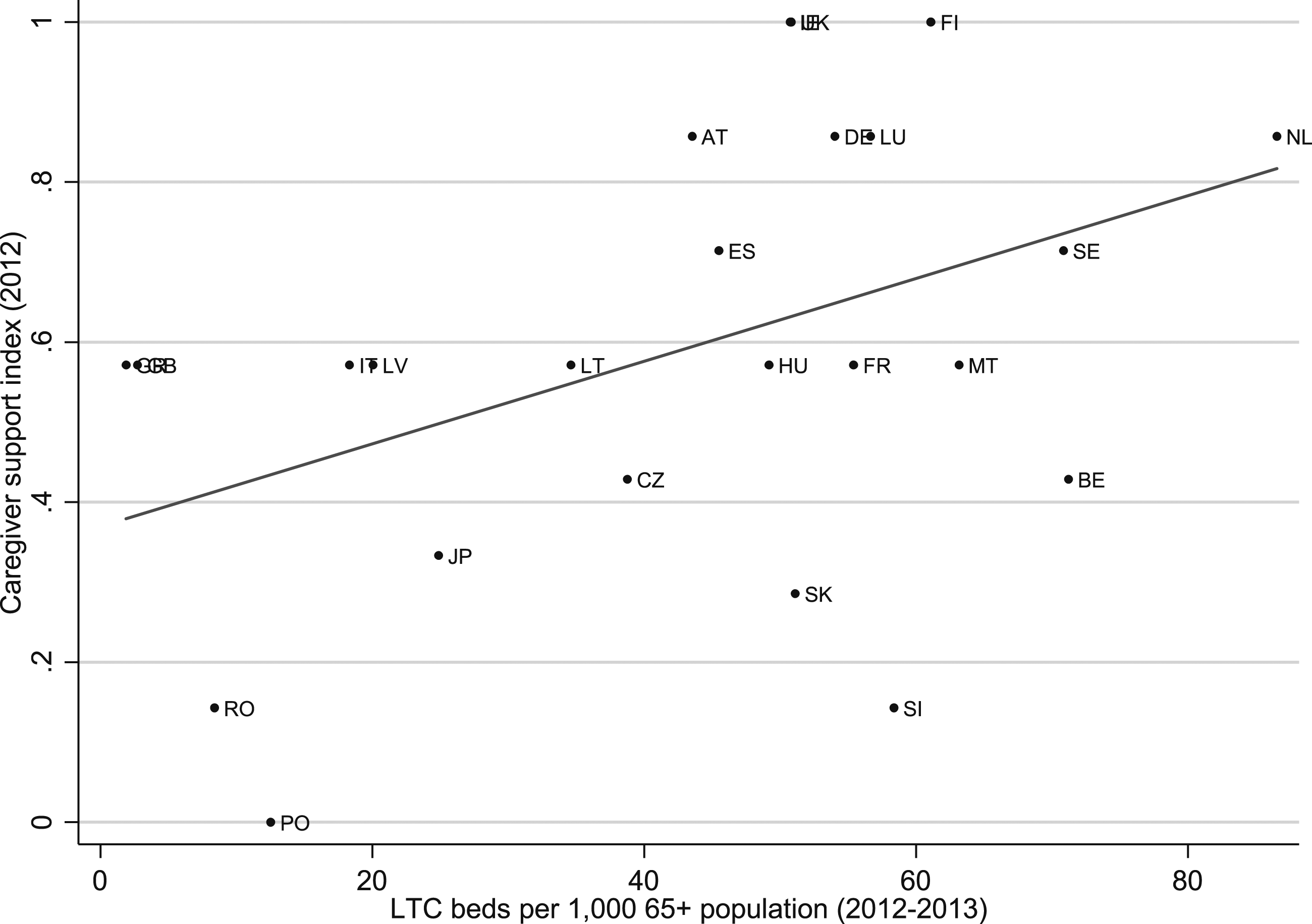
Discussion
Our study’s aims were to outline theoretical arguments on the differential impact of different types of LTC policies on socio-economic inequalities in care and to build a theory-based database with macro-level indicators of specific LTC policies. In doing so, we want to stimulate and facilitate future empirical research on whether and how specific LTC policies influence socio-economic inequalities in care. We searched for country and time-comparative indicators to capture Saraceno’s (2016) dimensions of supported familialism (policies directed at informal caregivers facilitating family care), supported defamilialization through the market (income transfers to care users to help buy services), and defamilialization though public provision (public care services directed at care users). Our work provided a theoretical overview of the literature on LTC policies and emphasized that different supportive LTC policies, which may be implemented simultaneously, may have a different impact on the SES gradient in care use and provision. We reported on the construction of the LTC indicator database and summarized the descriptive results from it. The LTC indicators based on our extensive and systematic quest are provided in this article (see Table 2) and can be used in future research.
A key rationale for our effort in constructing separate measures for supported familialism, supported defamilialization through the market and defamilialization through public provision was that these different types of policy instruments can be implemented in a country simultaneously, while we expect partly opposite effects from them on socio-economic inequalities in care use and provision. Hence, we argued that countries cannot simply be considered as one particular type of LTC regime, and that distinct measures for the different types of policy instruments are needed. Our descriptive results supported our claim. Our findings showed no significant association between supported familialism (that is, caregiver support index) and supported defamilialization through the market (that is, cash-for-care payments to care users) or between supported defamilialization through the market and through public provision; however, we did find a significant positive correlation between supported familialism and defamilialization through public provision (that is, long-term care beds). Hence, empirically, the two types of LTC policies were positively correlated, but theoretically, we argued that supported familialism is likely to increase socio-economic inequalities in care, whereas defamilialization through public provision is likely to decrease them. Overall, there was no clear pattern of association between LTC policies emerging among countries. For instance, in some countries we identified policies capturing dimensions of both supported familialism and defamilialization (for example, Netherlands and Spain) whereas in others we found only policies suggesting supported defamilialization through the market (for example, cash-for-care policies in Romania). In sum, our conclusion is in line with Saraceno (2016) who argues that a richer set of indicators is needed to better classify LTC policies in order assess their different individual outcomes, given that they affect family care responsibilities differently.
One central feature of the LTC policy database we desired was the availability of comparable indicators for many countries and many time points to facilitate statistical testing of the impact of LTC policies in large-scale empirical studies. For these types of analysis, sufficient variation in LTC policies across contexts is required. We encountered several limitations in this respect when constructing the database. First, existing international databases collect few comparative and systematic indicators on LTC policies. For example, while the MISSOC dataset provides detailed information on LTC policies for 27 EU countries between 2004 and 2019, the information does not allow for systematic comparisons of specific policies across countries. The lack of more comprehensive and comparable measures in this area is most likely due to difficulties in capturing the complexity of LTC systems. Relatedly, the detailed information collected on specific long-term care policies, for instance in the MISSOC database, is largely qualitative and descriptive, making it difficult to quantify. It is also likely to be because much of this data is compiled at the local government level from administrative records rather than at the national level (Carers UK, 2018). Moreover, data that is held by private or voluntary sector organizations such as care agencies may be difficult to access. Thus, even though we examined several international databases (for example, OECD and so on), we found information on key LTC policies to be sparse, and comparability a significant issue. A second limitation referred to the scarce availability of information at different time points. Not only were the most recent data for some of our indicators relatively old (cash benefits to caregivers and care users, for instance); our indicators for supported familialism and supported defamilialization through the market were available for only two time points. This largely reduced variance in the measure and hampers analyses that aim to relate changes in LTC policies to changes in (socio-economic inequality) in care use and care provision. Besides variation over time, geographical variation was relatively limited too. Especially, regional data was lacking, except for LTC beds.
We encourage future endeavours to reckon with these limitations of comparability and variation over time and place. For example, large-scale international comparable surveys are increasingly collecting comparable, aggregated contextual data, which can then be linked to individual level micro-data. Adding more nuanced data on long-term care would be a valuable addition to this endeavour. Brugiavini and colleagues (2017) have already begun to collect contextual information on legislation-based eligibility rules for access to cash-benefits or in-kind services for home care for disabled older people across selected European countries. Eligibility thresholds typically involve an assessment of care needs (for care users), care provided (for informal caregivers), living arrangements, employment status and are often means tested (Hoyer and Reich, 2016). Emerging work on this issue shows considerable variation across European countries (and over time) in the nature of the benefit and in who is entitled to receive it, which depends on a country’s definition of need. This information can then be linked to the harmonized micro-level data on older populations around the world creating an individual-level binary index for each respondent capturing their eligibility for home care (Carrino et al., 2018). We anticipate that our theoretical outline will inspire (future) data projects, such as that associated with the Gateway to Global Aging Data (https://g2aging.org/), to construct theory-based indicators of LTC policies.
In constructing the distinct measures for the three types of policy instruments, we identified distinctive theoretical features of the three types of LTC policies. These refer to whom the policy instrument is directed (supported familialism directly benefits informal caregivers; defamilialization directly benefits care users) and via which channels care users are supported (through the market or through public provision). We think these distinctive features are helpful to derive theory-based LTC indicators. However, we also experienced difficulties in applying them as there was a notable lack of information in the international databases to capture more nuanced aspects of LTC policies. We specifically encountered validity problems with respect to the availability of LTC beds. Although we assume that LTC beds are a sign of defamilialization through public provision, LTC beds may, in some countries more than others, be privately provided. Lack of detail in the availability of information hindered us from distinguishing between private and publicly funded long-term care beds. This implied that we may not have been as successful as we wished to separate the two types of defamilialization. Even if available information was detailed enough, difficulties in relating specific LTC policies to one of the three types of LTC policy on theoretical grounds emerged in other instances as well. Following the distinctive theoretical features of Saraceno’s types of LTC policies, cash benefits to care users (for example, Pflegegeld in Germany) would be classified as supported defamilialization through the market. This makes sense if such benefits may be used to employ private caregivers, for example, migrants from abroad. However, what if these cash benefits are largely transferred to informal caregivers? The LTC instrument then implicitly becomes an example of supported familialism. For example, this may be the case in Germany as most frail older people use their cash benefit to compensate family members (Eichler and Pfau-Effinger, 2009). Another grey area emerges when benefits paid to care users (here classified as supported defamilialization through the market) may only be used to buy services in a regulated market (for example, in France, Spain and Portugal). Such policies – here classified as supported defamilialization through the market – may come closer to defamilialization through public provision as the state, though not directly providing services, explicitly finances and mandates their costs. In such cases it is not clear to which type of LTC policies it would relate. In sum, our interpretation of Saraceno’s theoretical model on different supportive LTC policies – just like any theoretical model – cannot fully capture the complexity of LTC policies in the real world. We welcome further debate on the theoretical distinctions between LTC policy types and how they translate to concrete, quantifiable indicators.
Nevertheless, we stand by our argument that it is a relevant approach to distinguish between different types of LTC policies along the familialism/defamilialization continuum as their consequences for inequalities in care may differ. This is important because LTC regimes are often categorized by policy instruments reflecting different degrees and patterns of familialism and defamilialization. The recognition of varying and specific forms of familialism and defamilialization in countries’ LTC policies is critical if we are to address a key strategic objective of the WHO’s Global Strategy for healthy ageing: the development of sustainable and equitable systems of LTC (https://www.who.int/publications/i/item/global-strategy-and-action-plan-on-ageing-and-health).
In closing, we hope that our theoretical discussion of LTC policies and the LTC indicator database will fuel empirical research on the impact of different types of LTC policies on socio-economic inequalities in care use and care provision. In addition, we call for more systematic and comparable information on LTC policies among time and place in the future.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by an Open Research Area grant from the Netherlands Organisation for Scientific Research (NWO) (grant number ORA 464.18.106), the Economic and Social Research Council (ESRC) (grant numbers ES/S01523X/1), and the German Research Foundation (DFG) (grant number BR 3868/4-1) within the Open Research Area for the Social Sciences (ORA) for the project ‘In-CARE: How are varying care systems associated with inequalities in care and wellbeing in later life?’ (![]() ).
).