
Abstract
European countries have developed a range of long-term care (LTC) policy responses to support the increasing share of older people. However, little is known about the effectiveness of LTC services and benefits, particularly their impact on older peoples’ quality of life (QoL). This paper investigates the role of personal, care service and environmental characteristics on the effects of home care services on QoL across England, Finland and Austria. We used data from surveys conducted in England, Finland and Austria. In total, 811 older adults were included in the analysis. OLS regression including main effects and country-specific interactions was used to explore variation in gains in long-term care service-related quality-of-life (LTC-QoL). Explanatory variables were derived from the production of welfare framework and comprised home care service user socio-demographics, needs indicators, social support and environmental variables and characteristics of home care service provision. In all three countries, LTC-QoL gains increased with needs, indicating that home care services perform well, with additional gains declining the higher the needs. Also, better process quality contributed to LTC-QoL improvements in all three countries. In addition, the availability of informal care, social contact, financial household situation and living alone, were associated with changes in LTC-QoL only in one or two of the countries. Home care services increased service users’ QoL in all three European countries. The increase in QoL, however, varied across the countries. The results also provide insights into the benefits and limits of home care service provision and areas for future improvements.
Introduction
In many Nordic and Western European countries, home care service provision is an essential pillar of long-term care (LTC) policies, enabling frail older adults to age in place. Home care services support community-dwelling older adults in coping with (instrumental) activities of daily living ((I)ADLs) and may also include nursing care. To respond to people’s preferences (European Commission, 2007) and to balance public funding constraints, home care services have been given political priority over residential care in many countries (Spasova et al., 2018). Major changes in home care also relate to the (quasi-)marketization of services, client or customer orientation and support for informal carers (Bode et al., 2012). While drivers and aims of reforms appear to be similar, LTC policies still differ substantially across Europe (Spasova et al., 2018), reflecting different welfare structures, values and traditions that account for the diverse qualities and characteristics of LTC systems.
Comparative studies in the field of LTC provide substantial evidence on differences in European LTC policy designs (e.g. Da Roit et al., 2007; Österle, 2012), developments (e.g. Pavolini and Ranci, 2008; Ranci and Pavolini, 2015), market structures (e.g. Harrington et al., 2017) and macro-level LTC indicators (e.g. OECD, 2017; Pickard et al., 2007). In line with and building on this type of research, there has been increased interest in combining insights at the macro level with micro-level indicators of care outcomes to better understand how LTC policy subsequently influences the lives of care service users.
Recent developments in measurement tools have enabled researchers and policymakers to gain insights into the impact of LTC service provision, particularly on quality of life (QoL) (e.g. Degenholtz et al., 2014; Netten et al., 2012a). So far, the effectiveness of home care services on older people’s QoL has only been studied for single countries, for example for England (Forder et al., 2017; Netten et al., 2012b), the Netherlands (van Leeuwen et al., 2015) and the United States (Degenholtz et al., 2014). Information on LTC outcomes and potential explanatory factors across countries is lacking, limiting the potential to investigate their comparative impact and identify areas for improving practice and the allocation of scarce resources.
This article is the first to investigate factors influencing the impact of home care services on service users’ QoL across three European countries – England, Finland and Austria – using the Adult Social Care Outcomes Toolkit (ASCOT) for measuring QoL outcomes of LTC service provision. In line with the ‘production of welfare framework’ (Knapp, 1984), we expect different personal, care service and environmental characteristics to affect changes in LTC service-related QoL (LTC-QoL). Since the three countries have different LTC systems, with England’s safety net approach, Austria’s strong family orientation complemented by a universal LTC allowance, and Finland’s stronger public responsibility for LTC support, we expected the impact of these characteristics to differ between the three countries. Thus, the analysis also gives insight into what groups of home care service users across the three countries benefit relatively more or less from home care service provision.
Characteristics of home care service provision in Austria, England and Finland
The starting point for many international comparisons of LTC systems is the concept of care regimes, which implies that countries cluster into a small number of types of care systems, with similar internal logics that can be described along a set of dimensions. Efforts to identify ‘ideal’ LTC regime types have, however, resulted in different groupings of the same countries depending on the choice of dimensions used for the characterization (Longo et al., 2015; Schulmann and Leichsenring, 2014). Additionally, countries within categories diverge greatly (Schulmann and Leichsenring, 2014). Indeed, one classification using organizational depth and financial generosity for the typology of LTC systems (Kraus et al., 2010) assigned the countries of interest in this article, Austria, England and Finland, to the same ‘informal care oriented, high private financing’ cluster. There are, however, significant differences in the LTC systems of these three countries across several dimensions that would be expected to influence the way home care is delivered and the effectiveness of home care provision. We draw on these differences to explore the impact of the LTC system and policies on the lives of older people.
For the purpose of this article, we describe selected characteristics of LTC regimes that may influence home care service provision and outcomes either directly or indirectly, such as the boundaries between long-term care and healthcare (Billings and Leichsenring, 2006), eligibility criteria defining target group(s), funding arrangements and budget constraints that may affect service provision overall as well as specific groups of service users (Colombo et al., 2011; Wanless et al., 2006), the role of informal care and skill levels and qualifications of care workers that may affect their ability to meet the needs of care users (Stone and Harahan, 2010). We also report these differences in Table 4 in the Supplemental Appendix.
In Austria, healthcare and LTC services are provided by separate institutions, with healthcare being organized and co-funded by the social health insurance system and LTC services being organized at the local level and funded mostly via taxes and private co-payments (Trukeschitz et al., 2013), supported by a nationwide universal LTC cash benefit. A national means-tested cash benefit aims to enable 24-hour care in private households. Informal care, however, still plays a major role. In terms of care worker education, a nationwide system of educational standards was set up in 2005; education programmes range from 400 hours for home helpers to 3 years for care workers with diplomas (Österle and Bauer, 2011).
In England, responsibilities for LTC are split between the National Health Service (NHS), responsible for nursing care and local authorities, responsible for social care. There has traditionally been a clear separation between healthcare (which is free at the point of delivery) and publicly-funded social care which is means tested (Lewis, 2001). Access to social care services funded by local authority revenues (and, to a much lesser extent, central government funds) is restricted to lower-income people with eligibility determined through a means-test. People can receive social care services in kind or in cash via direct payments. Care provision and arrangement is carried out by local authorities, following nationally-set, needs-based eligibility criteria. The English LTC system also relies heavily on unpaid care (Pickard, 2015). The LTC system is not ‘carer-blind’ as the availability of informal care is taken into account when social care packages are devised (Comas-Herrera et al., 2010; Forder and Fernandez, 2011). Care service jobs have been traditionally classed as manual work in England, with little formal entry qualifications and short induction programmes as well as low wages (Simonazzi, 2009).
The Finnish LTC system is characterized by strong integration between social welfare and healthcare services, with a focus on providing comprehensive care (Leichsenring, 2004). LTC is steered by legislation and a national quality framework issued by the Ministry of Social Affairs and Health in 2017. Municipalities are responsible for needs assessment and the provision of care and services (Kangas and Kalliomaa-Puha, 2018; OECD and European Commission, 2013). In general, care packages are standardized, leaving little room for adjustments by care workers (Kangas and Kalliomaa-Puha, 2018). Funding is split between municipalities, service users and the state government, which contributes by non-earmarked subsidies to the municipalities (Colombo et al., 2011). Informal carers can sign a contract with their municipalities to get access to a better benefit package comprising financial support and services (Kröger and Leinonen, 2012). Training for care personnel is strictly regulated and care workers usually have a two- or three-year degree in health or social care, with longer programmes for certain types of professions (Kröger and Leinonen, 2012).
Framework for the analysis and hypotheses
Our model is based on the ‘production of welfare (POW) framework’ (Knapp, 1984) that puts emphasis on the combination of input factors to create intermediate outputs (e.g. hours of care provided) and final outcomes (e.g. changes in LTC-QoL). Both resource (related to the care services) and non-resource (such as service user and environment characteristics) factors are considered as inputs in the production process and affect LTC service outcomes, with limited influence of care providers on non-resource factors (Malley and Fernández, 2010; Trukeschitz, 2014).
Building on this POW approach, we expected (1) personal characteristics of the home care service users, for example, needs levels, (2) their environmental and social support characteristics and (3) care service characteristics to influence LTC outcomes. As home care is provided within a broader country-specific LTC policy context, we also investigate country-specific effects, which occur if the relationship between these resource and non-resource characteristics and LTC-related changes in QoL (final outcome) is different in at least one of the countries included in the analysis (Figure 1).
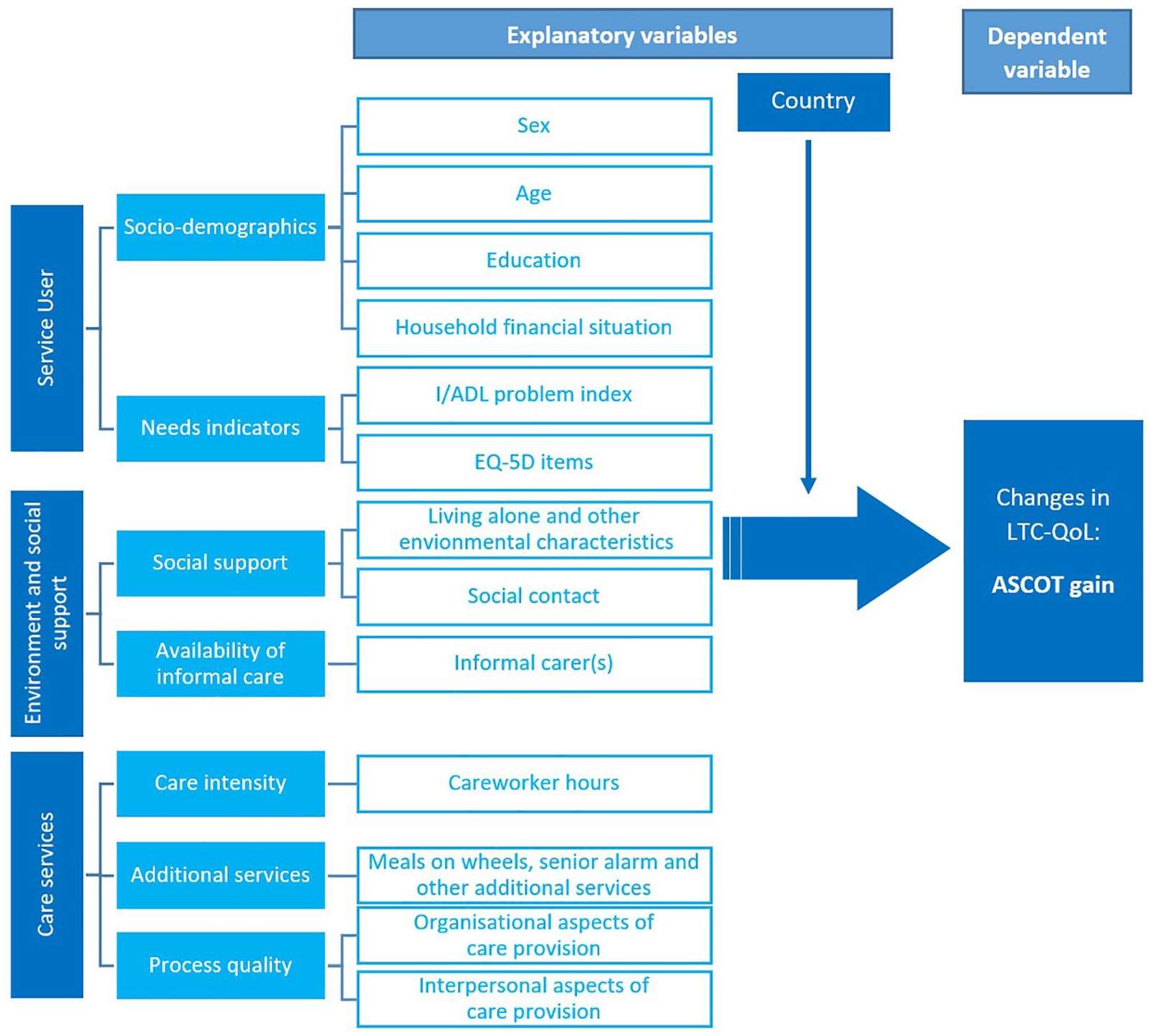
Model overview and variable groups.
Home care service user characteristics
According to Netten et al. (2010), service users with the highest needs have the greatest potential to benefit from adequate service provision. Thus, if home care services perform well in all three LTC regimes, we expect a positive relationship between needs and LTC-QoL gains, irrespective of the country. In line with the economic concept of diminishing marginal utility, however, we anticipate a lower increase in LTC-QoL the higher the needs and, ultimately, at a certain needs level, no further improvements of service users’ LTC-QoL (H1a). This would indicate that home care services can reach their limits for meeting frail persons’ needs. The qualification level of home care workers differs across the three countries, with England, compared to Austria and Finland, investing comparatively little in the qualification of care workers and the building of multidisciplinary teams. Therefore, we expect lower gains in LTC-QoL for home care service users with challenging needs (such as depression/anxiety) in England (H1b).
If home care services meet the needs of all socio-demographic groups similarly, then changes in service users’ QoL will not depend on age, sex, educational background (H2) or financial situation (H3) after controlling for other factors.
Environment and social support characteristics
During the last decades, single-person households have become more widespread among people aged 65 and older, with Finland having the highest proportion of older people living alone among the three countries (EUROSTAT, 2015; Reher and Requena, 2018). We thus expect the Finnish system to have adapted to this demographic pattern and better account for the needs of single-person households and generate higher LTC-QoL gains (H4a). A country’s LTC regime may also influence the relationship between LTC-QoL of service users and both forms of social support, namely frequency of social contact (H4b) and availability of informal care (H4c).
LTC service characteristics
As home care services are produced and consumed at the same time (Baldock, 1997), processes of service provision become important for outcomes. We thus assumed a positive relationship between users’ process quality ratings and LTC-QoL outcomes, particularly if the process indicators relate to the domains captured by ASCOT for service users (H5). In addition, LTC regimes providing care packages (a combination of services tailored to the service users’ needs), such as England and Finland, are assumed to achieve a higher impact of LTC-QoL than in Austria. Therefore, we expected additional services to have a positive effect on LTC-QoL in England and Finland, but not for Austria (H6). Finally, we assumed that care intensity also positively affects LTC-QoL outcomes, but with diminishing marginal utility (H7).
Methods
Data
We used data from purposively-designed surveys conducted in Austria, England and Finland. English data were collected as part of the IIASC project (Forder et al., 2016) in 2013/14, Finnish and Austrian data as part of the EXCELC project (Linnosmaa et al., 2020; Trukeschitz et al., 2018) in 2016/17. Data collection in Austria and Finland followed the English protocol with adaptations to institutional characteristics.
In England, 22 (out of 150) local authorities (LA) participated in the study. Each LA was asked to identify a random sample of service users in receipt of community-based social care from the LA’s records. LAs mailed an invitation to participate in the survey to sample members aged 55 and older. Service users, who consented to take part in the research by returning a form in a freepost envelope, were then interviewed face-to-face using a structured questionnaire approach to gather data (Forder et al., 2016). In Finland, an invitation to participate in the study was sent to the 21 largest municipalities or health and social care regions, in order to ensure sufficiently large regional subsamples, 12 of which gave written consent to participate in the study. The final sample consists of regular home care service users (aged 55 or older) residing in the participating municipalities or health and social care regions (Linnosmaa et al., 2020). In Austria, there are no national or standardized regional records of home care service users. Thus, two main recruitment strategies were applied (Trukeschitz et al., 2018). Home care service users were recruited in cooperation with the Austrian Federal Ministry of Labour, Social Affairs and Consumer Protection by drawing on a national sample from the Austrian Home Visit and Counselling Programme (HVCP), a programme aimed at assessing the care situation of community-dwelling LTC allowance recipients (Trukeschitz, 2010). In addition, care organizations or local authorities sent out invitation letters to home care service users in all nine Austrian regions.
For the purpose of this comparative paper, we restricted the analyses to home care service users aged 65 and older receiving regular support from care workers (including nurses). We performed Little’s MCAR test (Little, 1988) on the reduced sample to determine whether missing values were systematic and could not reject the null hypothesis that the data was missing completely at random.
Model and measures
We performed an OLS regression for explaining variation in LTC-QoL gains across and within countries. Both bootstrapped and regular standard errors were used, but the results showed little difference. The analysis was carried out in Stata 15.
To capture main effects and country-specific effects, we modelled an individual’s i LTC-QoL change y using equation (1):
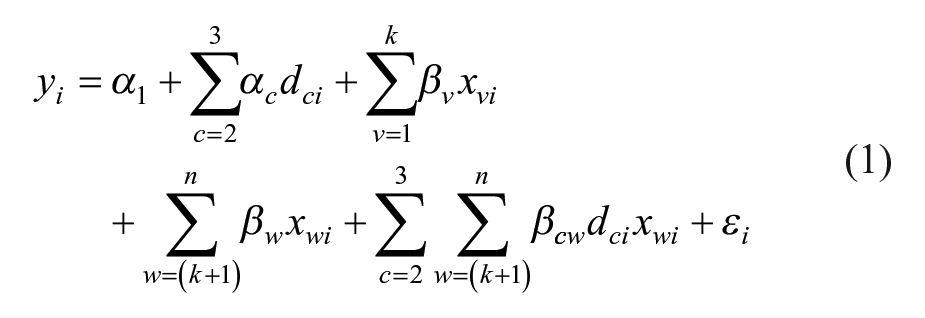
With
Dependent variable: LTC service-induced changes in QoL
There is a range of measures available to assess the QoL of older people receiving LTC. An empirical comparison of three tools suggested OPQoL-Brief, the EQ-5D-3L and ASCOT to be suitable for measuring QoL outcomes in community-dwelling older people (Kaambwa et al., 2015). ASCOT, however, is the only one of these measures for assessing LTC service-induced changes in QoL in observational studies (Malley et al., 2019b).
LTC service-induced changes in QoL (short: LTC-QoL changes) were measured using ASCOT-INT4 (Netten et al., 2012a), which can be used for directly assessing the impact of LTC services on service users’ QoL by calculating the difference between two LTC-QoL states. ASCOT is available in different languages, including English (original instrument), Finnish and German (Trukeschitz et al., 2020).The ‘current’ LTC-QoL scores indicate a person’s overall LTC-QoL in the current situation (that is, with the LTC services they are receiving) and ‘expected’ scores indicate their overall LTC-QoL in the absence of these services. The ASCOT service user measure includes eight domains (control over daily life, personal care, food and drink, accommodation, personal safety, social participation, occupation and dignity). As there is no question capturing dignity in the absence of services (expected state without services), we have excluded this domain for the purpose of this article.
The dependent variable (LTC-QoL changes) is the difference between the current and expected ASCOT scores of values from seven domains excluding the dignity domain:

The current and expected ASCOT scores (


Both
Explanatory variables
Service user characteristics comprised socio-demographic variables and needs indicators. Sociodemographic variables captured sex, age groups, education and self-assessed household financial situation. Physiological needs were accounted for using an (I)ADL problem index with 12 (I)ADLs, with values ranging from 0 to 12, with 12 indicating the highest possible need (i.e. the person cannot do any (I)ADLs). The psychological aspect of needs intensity was measured by the EQ-5D-3L-item for anxiety/depression (The EuroQol Group, 1990).
Environment and social support contained variables on the social environment, comprising the living situation of the home care service users (living alone or not), help from informal carers (yes or no) as well as service users’ intensity of social contact. The data contained four variables on social contact, asking how often a person (1) speaks to relatives or friends on the phone, (2) texts or emails relatives, (3) speaks to neighbours and (4) meets up with relatives or friends. These were combined to form a binary social contact variable indicating whether a person had stated to have some form of social contact on most days or not.
LTC service characteristics comprise the intensity and process quality of home care and the availability of an emergency call system (senior alarm). To reflect formal care intensity, we used care worker hours provided by any type of home care worker in the week prior to the interview. Two measures of home care process quality (PQ) were used. Information about changes in home care service provision (PQ: changes) reflected whether the service user was kept informed about day-to-day changes in the care they receive. A second process variable (PQ: do things you want) indicated whether the care workers generally do the things that the home care service user wants done.
Results
Sample description
The sample comprised 811 home care service users (177 in England, 264 in Finland and 370 in Austria). Table 1 describes the variables included in the analysis. Average LTC-QoL changes differed across the countries, with the highest mean change in England (0.37 index points) and the lowest in Austria (0.19 index points) (Table 1). The average LTC-QoL change overall was 0.25 index points. Assuming that changes in LTC-QoL are generally positive (net gains), this is equivalent to an improvement by 25% points for a possible range of gains from 0 to 1. Depending on where the individual stands at the initial QoL-range, this may be an improvement from a very bad (close to 0 index points) state to a state with limited basic QoL (0.25 index points) or an increase resulting in high or very high QoL for individuals starting at a higher initial LTC-QoL.
Sample description.
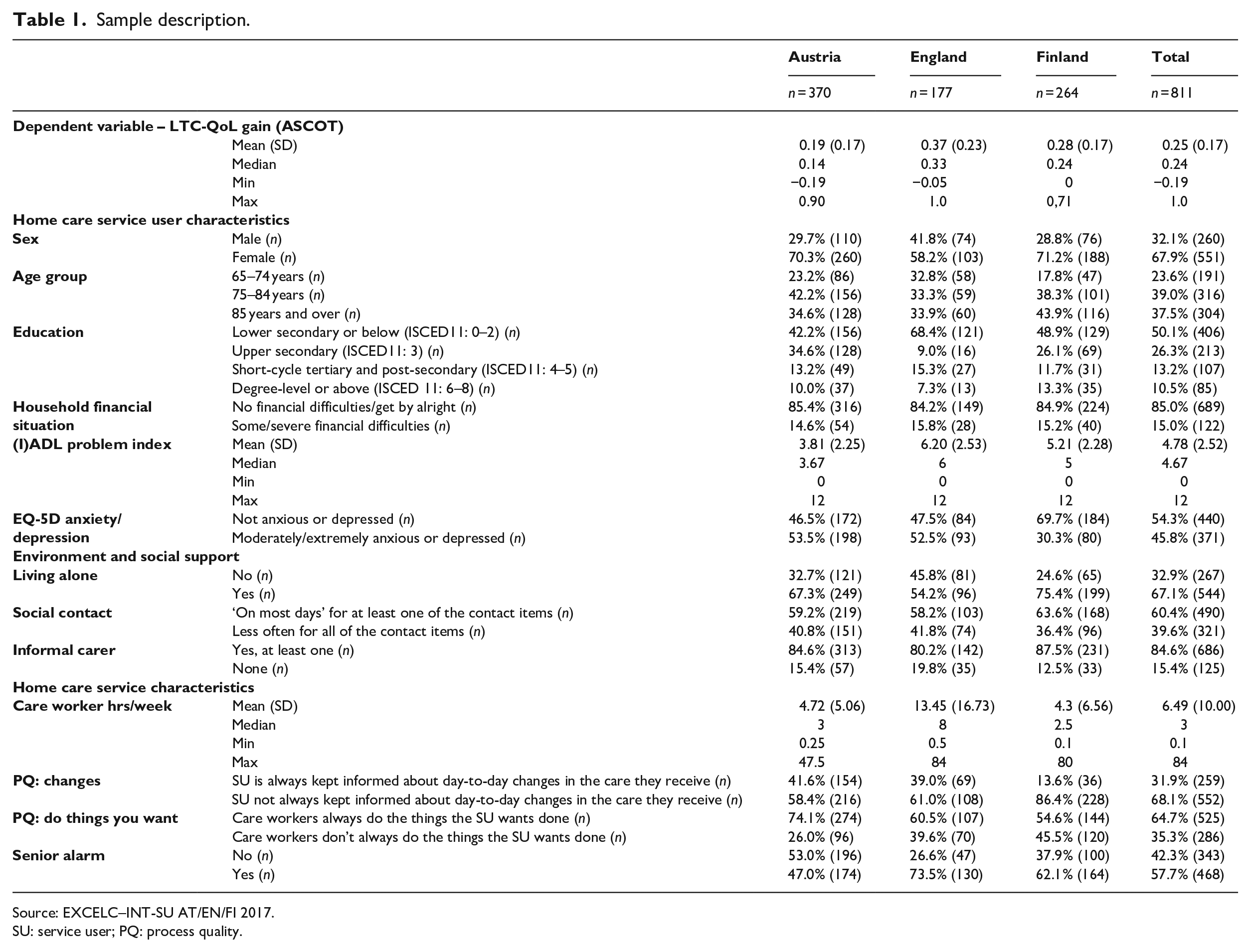
Source: EXCELC–INT-SU AT/EN/FI 2017.
SU: service user; PQ: process quality.
Figure 2 shows the distribution of the dependent variable (LTC-QoL change). Only very few home care service users were affected negatively by the care service they got (e.g. through decreasing perceived control over daily life). Average LTC-QoL changes were clearly positive (Table 1, Figure 2).
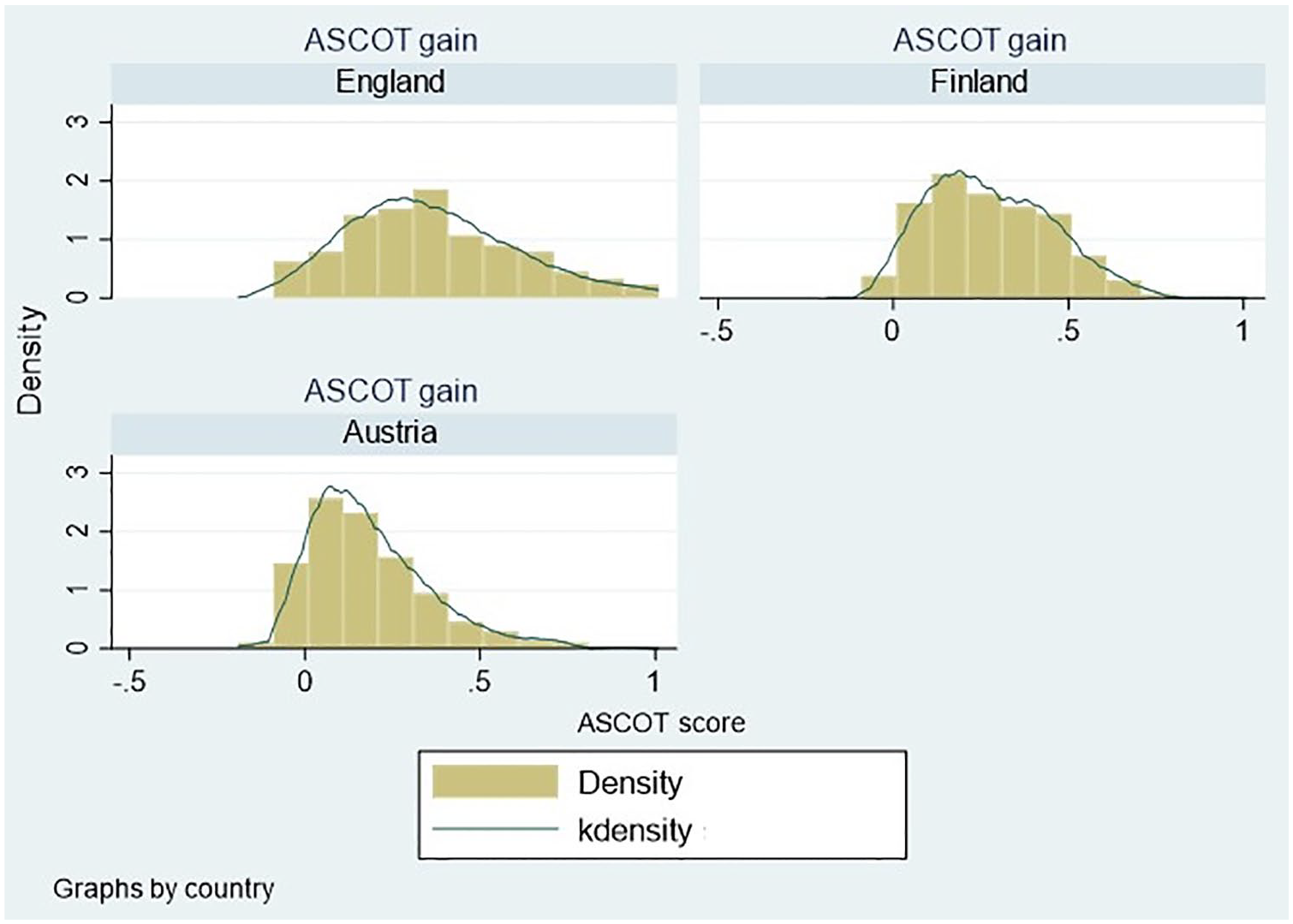
Distribution of LTC-QoL gains (ASCOT), dependent variable.
Regression analysis results
Table 2 shows the regression results including interaction and quadratic terms. As the inclusion of higher-order terms affects lower-order coefficients (Brambor et al., 2006), we report marginal effects of variables used in interaction and quadratic terms in Table 3.
Regression results.
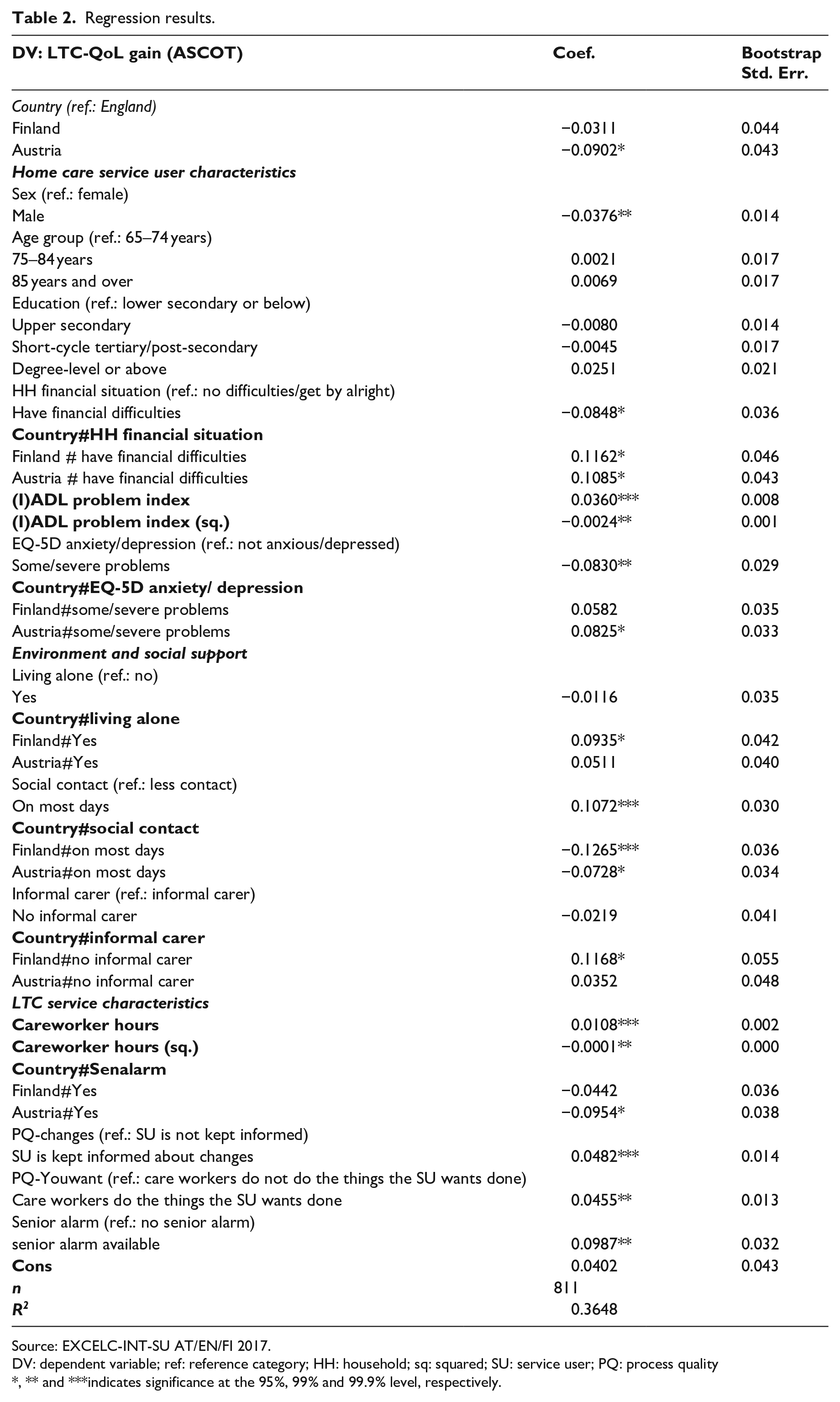
Source: EXCELC-INT-SU AT/EN/FI 2017.
DV: dependent variable; ref: reference category; HH: household; sq: squared; SU: service user; PQ: process quality
, ** and ***indicates significance at the 95%, 99% and 99.9% level, respectively.
Average marginal effects for variables used in country-interactions (Austria, England and Finland) and marginal effects at specific values for variables used in quadratic terms.
Regression results and 4 Average margina.
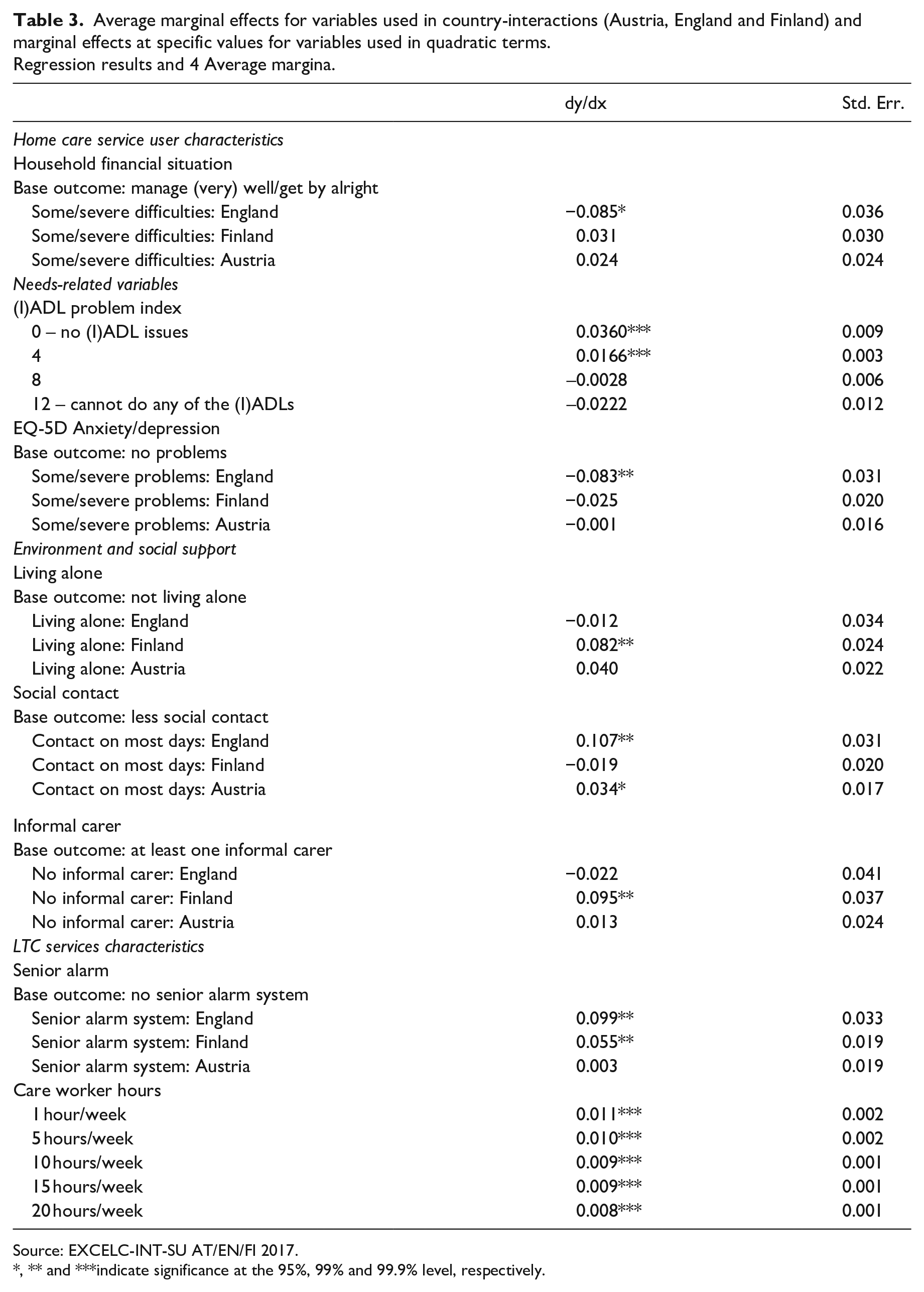
Source: EXCELC-INT-SU AT/EN/FI 2017.
, ** and ***indicate significance at the 95%, 99% and 99.9% level, respectively.
In terms of characteristics of home care service users, we found a significant relationship between the outcome and sex of the service users for all three countries. On average, LTC-QoL improvement was 0.04 index points lower in men than in women (this is equal to a reduction by 15% of the mean LTC-QoL gain for men) (Table 2). No significant relationship was present for age or education. We found differences between the three countries regarding the financial situation of the household (Table 3). The coefficients listed in Table 3 are country-specific marginal effects indicating the change in predicted LTC-QoL when moving from the base outcome to another category within a country. Home care service users who reported having some or severe financial difficulties had significantly lower LTC-QoL gains in England only. We thus reject H2 and H3 that home care services in the three countries meet the needs of socio-demographic and socio-economic groups in a similar way.
Needs-related variables
As expected, there was an inverse U-shaped relationship between LTC-QoL changes and the (I)ADL problem index (Table 2). For all countries, a significant but diminishing positive effect could be found up until an index value of 7, after which coefficients became non-significant (Table 3). As such, the data support H1a, which predicted a positive, but declining marginal utility of home care services with increasing needs.
There was also a significant negative relationship between the EQ5D-item anxiety/depression and LTC-QoL changes in England, where home care service users affected by anxiety/depression had lower gains in LTC-QoL (Table 3). The difference was 0.08 index points, which is equivalent to 22% of the average LTC-QoL gain in England (0.37 index points). This supports H1b that home care service users with challenging needs (such as depression/anxiety) benefit less from home care provision in England, a country investing comparatively little in the qualification of home care service workers.
Environment and social support
Home care service users living alone had greater LTC-QoL gains than those living with someone else in Finland only (Table 3). We thus found support for H4a that the Finnish system better accounts for the needs of home care service users living alone. Service users who had social contact on most days experienced higher effects of home care service provision on QoL in England and Austria (H4b). Those who had no informal carers reported significantly higher LTC-QoL gains in Finland compared to those who had at least one informal carer (H4c) (Table 3).
LTC service characteristics
As expected, LTC-QoL gains increased with home care service intensity, but marginal effects diminished with higher service intensity (Tables 2 and 3), with no differences between the countries. This supports H7 predicting positive, but declining marginal LTC-QoL gains for increasing numbers of care hours.
Home care service users who were being kept informed about changes in their care provision had significantly higher LTC-QoL gains on average (Table 2). The difference was 0.05 index points, the equivalent of 19% of the average LTC-QoL gain (0.25 index points). Home care service users also experienced higher LTC-QoL gains when care workers always or usually did the things which the service users wanted done. This supported H5 that better process quality contributes to LTC-QoL improvements.
Finally, the availability of a senior alarm system was associated with higher LTC-QoL gains in England and Finland, but not in Austria (Table 3). We thus found some weak evidence (restricted to senior alarms only) for H6 that additional care services contribute to improvements in LTC-QoL in countries where services are usually provided as parts of integrated care packages instead of individually.
Discussion
This analysis aimed to explore general and country-specific relationships between service-user characteristics and the QoL-impact of home care services in three European countries. By using unique micro data, we were able to compare outcomes of home care services by assessing home care service-induced changes in QoL for England, Finland and Austria. We found that home care services improved people’s LTC-QoL in all three countries, but their impact differed across groups of service users. Some factors influenced LTC-QoL outcomes in similar ways, irrespective of the country, such as process quality, care dependency, gender and care intensity. We also found country-specific differences in how service users’ QoL is affected by home care services, for example in terms of financial situation, specific needs and living situation.
In all three countries, LTC-QoL gains were positively associated with service user needs, showing that home care services could cope with the challenges of care dependency, but additional LTC-QoL gains declined with higher needs. These results are consistent with findings from previous studies reporting positive relationships between service intensity and outcomes with diminishing marginal benefits for England (Forder and Caiels, 2011; Forder et al., 2014, 2017). Thus, home care services support vulnerable people living at home but may face limits in compensating very high needs. In the same vein, we found that the home care hours provided positively affected outcomes, but additional gains decreased with higher care hours – as the capacity to benefit decreases, additional care hours help to maintain QoL or only slightly increase it. Again, this may indicate limits of home care service provision.
Differences in LTC-QoL changes by financial household situation, as found in England, may point to within-country variation. More disadvantaged areas have been affected the most by budget cuts and rationing, creating or reinforcing substantial local variation within the country (Pickard et al., 2007; Tinson et al., 2018). If persons with financial difficulties tend to live predominantly in poorer areas, the statistical relationship may reflect these regional disparities in the provision of care. Since charges for publicly-funded home care are only levied on those with the means to pay, structural disadvantage seems a more likely explanation than an alternative that this finding reflects differences in the level of care provided to the most financially disadvantaged households.
Environment and social support variables were found to have differing relationships with LTC-QoL changes in the three countries. Persons living alone and persons without any informal carers benefited more in Finland. The relatively larger proportion of single older people in Finland (EUROSTAT, 2015; Reher and Requena, 2018), also reflected in our sample, may have shaped the LTC system to be more aware of and equipped to meet their specific needs. Furthermore, Finnish LTC policy takes measures to actively integrate family carers into the publicly organized care system and create formal support for informal carers (Kröger and Leinonen, 2012), which may in turn benefit service users as well.
In England, mental health issues were related to lower LTC-QoL gains, but this was not the case for Finland and Austria. It may be that the disjointed way LTC is provided in England is particularly problematic for people with mental health issues. Home care workers for older people may not be trained to deal with these issues specifically, as mental health issues are not the focus of typical care work with older people in England. Furthermore, as care worker training is usually not that extensive in England (Table 4 in the Supplemental Appendix), staff may not be equipped to deal with these issues. English LTC policymakers may thus want to invest in developing the skills and competencies of care workers, perhaps through mandatory qualifications or training to enable them to provide better tailored support to people with mental health problems. Strategies may include training care workers to identify mental health conditions and signpost service users to mental health provision, developing specialist care workers trained in supporting people with mental health conditions, or involving care workers in multi-disciplinary teams that include experts in supporting people with mental health conditions (Social Care Institute for Excellence, 2018).
The strong relationship between process quality variables and home care service-induced QoL outcomes in all three countries stresses the importance of the care process, which has a clear impact on home care service users’ QoL. The importance of process quality for QoL outcomes have been investigated for England (Malley et al., 2019a), showing that perceptions of a positive care experience were strongly associated with better LTC-QoL outcomes. In our comparative three-country analysis, two aspects of process quality that relate to having control over what care workers do were particularly important – service users’ LTC-QoL improvements are higher when they are kept informed and involved in how services are provided. This stresses the importance of emancipatory aspects of home care service provision.
Last, but not least, the results point to the need for more research on the typology of LTC systems. Some of the care regime literature suggests that two or all three countries are similar enough to be assigned to the same group. The results of this study show that there are differences in how the systems seem to produce outcomes for certain groups of home care service users and for service users in different countries. The results should therefore be a cause for reflection on the dimensions (e.g. care worker qualifications) that are relevant for building typologies of LTC systems, if the aim of comparative research is to identify elements of LTC systems that are likely to produce greater well-being. This work can therefore be instructive for the body of literature that seeks to develop LTC system typologies.
The study has some limitations. Data collection on the living situations of people using LTC services across different LTC systems comes with challenges. Although we followed the English data collection protocol, institutional differences made it difficult for the Austrian and Finnish data collection to adhere to it in all its details. Such deviations may result in differences in the study samples, although we aimed to collect samples that are representative of home care users within the respective nations. The English data are, however, wanting in that respect as the sample is younger and more male than the publicly-funded home care population. Since we are interested here in relationships between variables and control in the models for age and gender, the representativeness of the sample should not be a very significant limiting factor, but care should be taken in drawing conclusions about differences between the characteristics of home care populations. In addition, publicly accessible data to compare the three countries using LTC-related macro-indicators, such as number of service users in a particular age group, are not complete, requiring national, European and international efforts to improve the database.
The lack of regional indicators in the dataset made it impossible to study regional variation. It can, however, be inferred from some of the country-specific effects, which might be related to within-country regional differences. Understanding regional variation when comparing LTC systems can be especially important in countries with substantial regional variation in care organization and supply, as is particularly the case for Austria and, to a lesser extent, for England and Finland, and is thus recommended for future research.
This study is the first to investigate the impact of home care services on service users’ QoL across three European countries using individual-level data and to discuss the factors influencing QoL at the level of the service users, their environment and social support and home care services. Home care services improved service users’ QoL in all three countries, which supports the relevance and usefulness of such services for care-dependent older people. In addition, this study has demonstrated the value of conducting comparative research into home care QoL-outcomes using individual-level data; we have shown through the inclusion of both overall and country-specific effects how LTC services can either have similar or varying effects on people’s lives in countries with different LTC policies. This statistical evidence provides insight into the benefits and limits of home care service provision in different countries. The comparative results can be used to help national policymakers and care providers to evaluate their LTC systems and practices and identify areas where investment or new approaches may have the potential to deliver benefits and improve older people’s QoL.
Supplemental Material
sj-pdf-1-esp-10.1177_0958928720974189 – Supplemental material for Investigating factors influencing quality-of-life effects of home care services in Austria, England and Finland: A comparative analysis
Supplemental material, sj-pdf-1-esp-10.1177_0958928720974189 for Investigating factors influencing quality-of-life effects of home care services in Austria, England and Finland: A comparative analysis by Birgit Trukeschitz, Assma Hajji, Judith Kieninger, Juliette Malley, Ismo Linnosmaa and Julien Forder in Journal of European Social Policy
Footnotes
Acknowledgements
We would like to thank all those who participated in the research by sharing their experience about home care services or enabling data collection.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by the NORFACE Welfare State Futures programme under grant number 462-14-160. In addition, the Austrian contribution to this project was co-funded by the Austrian Science Fund (FWF, project number I 2252-G16) and the Vienna Social Fund (FSW). The Finnish contribution to this project was co-funded by the Finnish Institute for Health and Welfare (THL). The views expressed are not necessarily those of the funders.
The OPEN ACCESS publication of this article was jointly funded by WU Vienna University of Economics and Business and its Research Institute for Economics of Aging.
Informed consent
All study participants provided informed consent
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.