
Abstract
Although the European Health Insurance Card (EHIC) was meant to bring Europeans together, this study shows that it is amplifying social inequalities across regions and classes. First, we evaluate the effects of east–west EHIC mobility, and of Eastern Europeans’ participation in it, on the practice of EU social citizenship rights to access cross-border care along spatial (east–west) and social class divides. We then assess the impact of these mobilities on healthcare resources in Western and Eastern Europe. Our findings show that the EHIC reinforces rather than reduces the spatially and socially uneven access to social citizenship rights to cross-border care. Moreover, EHIC patient outflows from Eastern to Western Europe result in a much higher relative financial burden for the budgets of Eastern European states than outflows from Western to Eastern Europe do for Western European countries. As a result, east–west EHIC mobility is reproducing rather than reversing healthcare inequalities between the two regions. Hence, the EHIC does not fulfil its promise of European social integration – not, however, because it creates a burden on Western European welfare states as often argued in Eurosceptic tabloids, but because it increases social inequalities both inside and between richer and poorer EU member states.
Keywords
Introduction
At the time of its introduction in 2004, the European Health Insurance Card (EHIC) was hailed as more than a tool to access unplanned care while travelling in another EU state. The EU also promoted it as ‘another piece of Europe in your pocket’ (European Commission, 2004) and thus a symbol of a European citizenry united across borders. Since the eastern enlargements, however, the promise of European social integration through the EHIC has been increasingly challenged. East–west differences in economic development and welfare systems have translated into ‘significant differences in the substantive social rights of EU migrant citizens’ (Bruzelius et al., 2017: 1239). Nonetheless, during the financial crisis the rise in east–west migration led to allegations in Western European (WE) countries that Eastern European (EE) migrants’ healthcare practices were a drain on WE healthcare resources (ICF GHK, 2013; Mikl-Leitner et al., 2013). These allegations concerned mostly EE migrants’ use of health services in the host country (Ehata and Seeleib-Kaiser, 2017). The ‘rhetoric of suspicion’ (Gabarro, 2017: 31), however, has been extended to EE migrants’ use of EHICs in their countries of origin. In the run-up to the Brexit referendum, for example, several newspapers featured stories of EE migrants obtaining the EHIC in the UK to access services in their home countries at the expense of the NHS.
In this article, we address the promise of EHIC as a tool of European social integration in the context of the growing politicization of the card. Social integration is the process through which people are brought together in a common social space (Threlfall, 2003), although this process does not necessarily mean that ‘the relationships so described are harmonious’ (Scott and Marshall, 2009: 752). Social integration has historically involved various mechanisms. According to supporters of the mid-twentieth century class compromise, social integration requires re-distributional measures to secure the integration into a polity and society of excluded social groups, such as the working class (Marshall, 1950) – or, for that matter, migrants. The emerging European healthcare union, however, does not include much cost-sharing despite it being a federal system (Vollaard et al., 2016). This is because EU social citizenship rights were primarily granted to secure the mobility of people in the Single Market rather than serve as tools for citizens’ equal participation in the EU polity (Threlfall, 2003). The resulting ‘market citizenship’ (Bartle, 2006) echoes a ‘bourgeois conception of the citizen as the passive consumer’ of individual liberties and benefits (Heller, 1971 [1928]; see Dyzenhaus, 1996: 1131). This conception is nonetheless problematic, as shown by the divisive debates about the effects of cross-border care in an enlarged EU marked by low levels of social equality. In this article, we therefore address two questions on EHIC uptake and use in the uneven healthcare union: (1) To what extent does EHIC mobility, and EE migrants’ participation in it, translate into substantive differences in EU social rights across regions and classes? and (2) What are the distributional effects of EHIC mobility on WE and EE healthcare services?
Concretely, we first situate the EHIC in the EU’s market-based understanding of European social integration and citizenship, the resulting EU cross-border care law, and the spatially and socially uneven European healthcare space. Subsequently, we present our methodology and the data on EHIC mobility used in this article. In the empirical sections, we first evaluate the distribution of EHIC uptake and use across regions and classes by placing it in the broader context of intra-EU mobility. Then, we assess EE migrants’ use of the EHIC in two situations, as they may possess a card issued by their EE country of origin; or one issued by their WE host country. Finally, we evaluate the distributional effects of EHIC use on WE and EE healthcare resources.
Our findings show that EHIC uptake and use are unevenly distributed between Western and Eastern Europe, as well as among social classes. In this context, EE citizens’ participation in EHIC mobility reflects the constraints of the EU migration system in terms of access to labour markets, residency and public services in home and host countries (Favell, 2008), rather than simply the free choices of European consumer-citizens. Moreover, east–west EHIC patient outflows result in a much higher relative burden for EE states than west–east outflows do for WE countries. As a result, east–west EHIC mobility contributes to reproducing rather than reversing spatial and social inequalities in access to healthcare and in healthcare resources across the EU. We conclude that the current operation of the EHIC fails to bring Europeans together – not, however, because it creates a burden on WE welfare states, but rather because it amplifies social divides within and between Western and Eastern Europe.
The EHIC and EU market citizenship
The EHIC is a prime example of an EU social policy designed to bring Europeans together through the development of market citizenship, that is, the enhancement of free movement rights stemming from the Single Market (Bartle, 2006).
Since the creation of the European Economic Community, various pieces of EU law have sought to remove barriers to labour mobility resulting from restrictions to access social security, including health services, while abroad. This led to the development of European social rights for mobile EU citizens being largely left to the courts and laws intended to support the making of the Single Market (Leibfried and Pierson, 2000). The 1957 Treaty of Rome already included provisions regarding access to, and export of, social security across borders to support workers’ freedom of movement (Martinsen and Vollaard, 2014: 681). Successive European regulations refined the criteria for the cross-border portability of social security rights for various categories of persons, that is, workers, pensioners, students and tourists. The regulations covered access to host countries’ health services for persons who (a) changed their country of residence, (b) travelled temporarily to another state and accessed unplanned care that was ‘immediately necessary’ or (c) were referred to health services in another state and accessed planned care pre-authorized by the authorities in the state of residence (Fillon, 2009: 214).
After its creation by the Maastricht Treaty in 1992, EU citizenship led to further extensions of the right to access cross-border public services and benefits (Kostakopoulou, 2007; Recchi, 2009). Following several EU court rulings, subsequent EU laws further enhanced EU citizenship rights of access to cross-border health services (Martinsen and Vollaard, 2014), that is, the 2004 citizens’ rights Directive; the Regulations on the coordination of social security of the 2010s (hereinafter the Regulations); and the 2011 Directive on patients’ rights to cross-border care (hereinafter the cross-border care Directive). The Regulations harmonized the criteria to access unplanned cross-border care and extended it to ‘medically’ rather than solely ‘immediately necessary’ cross-border care, and to ‘all persons insured in a member state’ rather than solely workers and other special categories (Fillon, 2009: 214). They also introduced the EHIC to facilitate access to unplanned care for migrant workers, businesspeople, tourists, students, job seekers and pensioners during a temporary stay in another member state (Vollaard, 2006: 218). The card proves insurance status, a precondition for accessing unplanned and medically necessary care in another member state. Issued free of charge and available to all residents covered by a member state’s healthcare scheme, the card simplifies paperwork for patients.
At its birth in 2004, the then Commission president, Romano Prodi, hailed the EHIC as ‘another piece of Europe in your pocket’ (European Commission, 2004), and subsequently the EHIC was portrayed as a means to bring Europeans together (Maas, 2008). The EHIC thus epitomizes the EU’s market citizenship (Bartle, 2006), inasmuch as it enhances freedom of movement under the Single Market and promotes the figure of the consumer-citizen free in his/her choices to travel and access care abroad.
The drive towards market citizenship in healthcare did not stop with the EHIC. The cross-border care Directive added individual patients’ right to choose health services among both private and public providers across the EU to the existing Regulations-based citizens’ right to access publicly covered healthcare abroad (Peeters, 2011). It also more clearly defined states’ discretion in imposing pre-authorization or in refusing authorization for cross-border care, in a bid to further enhance patients’ choices.
EHIC use is thus part of an increasingly intricate mosaic of possible pathways to cross-border care, which EU citizens are invited to navigate by making informed choices (European Commission, 2015). In so doing, they are encouraged to see their rights of access to cross-border care in consumer-citizen terms, as individual choices between various routes. In this mosaic, the EHIC is by far still the most significant pathway. 1
Cross-border care and Europe’s social divisions across regions and classes
Recourse to cross-border care requires specific knowledge of rights and administrative procedures, and money to pay for travelling and staying abroad (Baeten, 2011; Hervey and McHale, 2015). In the EU, these material and symbolic resources are unevenly distributed across space and social classes. Indeed, accession to the EU did not lead to social convergence between the East and the West (Beacháin et al., 2012; Bohle and Greskovits, 2012; Filauro and Parolin, 2019). Instead, the incorporation of east–west divisions alongside existing north–south ones contributed to shaping the EU as an unevenly developed social space (Hardy, 2014; Rae, 2011). In turn, the still significant wage gap between Western and Eastern Europe led to the latter becoming the main reservoir of labour for Western Europe (Favell, 2008; Meardi, 2013; Stan and Erne, 2014), mostly in low-waged, low-skilled sectors (European Commission, 2019). This uneven development is also reflected in the significant east–west gap in average healthcare expenditure per capita (Busse et al., 2011), which in 2016 was €3218 in Western Europe compared to €1285 in Eastern Europe (Eurostat, 2018, [demo_pjan]; WHO, 2018, our calculations). Moreover, in the same year, only 1.9% of the working-age population in Western Europe reported unmet healthcare needs for reasons of their being too expensive or too far away, or waiting lists, but more than twice (4.7%) did so in Eastern Europe (Eurostat, 2018, [hlth_silc_08]; [demo_pjan], our calculations).
Spatial east–west divisions in the EU are criss-crossed by transnational class divisions, leading to complex landscapes of differentiation inside EU member states as well as among EE migrants. Divisions between higher and lower classes are generally more acute in Eastern than in Western Europe (Hugrée et al., 2017). Compared to WE countries, EE countries display a steeper class gradient in accessing healthcare (Moscelli et al., 2018), as illustrated, for example, by higher rates of unmet medical care needs among lower socio-economic groups in these countries (Eurostat, 2018, [hlth_silc_08]). More worryingly, EE countries are confronted with a wider disenfranchisement of notable sections of their populations (e.g., the unemployed and those working in the informal economy or in subsistence farming) not covered by social health insurance (Stan and Toma, 2019; Waters et al., 2008). Likewise, EE migrants are differentiated along class lines between a relatively thin stratum of higher-skilled, higher-paid workers and a large majority of workers in lower-skilled, lower-waged jobs. Therefore, the higher barriers to accessing health services which EE migrants encounter in their host (WE) countries as compared to their EE countries of origin (Ehata and Seeleib-Kaiser, 2017; Glinos et al., 2010; Migge and Gilmartin, 2011) apply differently to these two categories of EE mobile citizens.
Our perspective hence brings into the picture the constraints that an uneven access to resources poses to mobile EU citizens’ access to cross-border care and EHIC mobility. Thus, we problematize the alleged choices that EU citizens, and in particular EE migrants, may deploy when obtaining and using the EHIC.
Data and methods
We rely on three types of data to support our argument: (1) quantitative data on intra-EU mobility; (2) qualitative data on the transnational healthcare practices of EE migrants; and (3) quantitative data on EHIC uptake and EHIC patient and payment flows between WE and EE states. In our study, EE refers to the 11 states that joined the EU in 2004, 2007 and 2013 (excluding Malta and Cyprus), whereas WE refers to the 15 ‘old’ EU member states.
Two Eurostat datasets allow us to assess work and non-work intra-EU mobility. These are: data on the participation of the EU population aged 15 years or over in outbound trips of one night or over for personal purposes (Eurostat, 2018 [tour_dem_totot]) – for non-work intra-EU mobility; and data on the number of employed working-age persons in the EU by country of citizenship (Eurostat, 2018 [lfsa_egan]) – for work mobility. These data allow us to assess intra-EU mobility patterns across social classes, regions and purposes of travel.
In order to assess EHIC uptake across the EU, we use data from the EU-wide 2016 Commission survey (Pacolet and De Wispelaere, 2017) on ‘EHICs in circulation’ (p. 11). 2 In order to assess EE migrants’ participation in cross-border care and EHIC mobility more specifically, we draw on studies led by peers and ourselves on EE migrants’ transnational healthcare practices. This allows us to assess their participation in EHIC mobility as part of migrants’ overall cross-border patient mobility and then to investigate the spatial and social class distribution of these various mobilities.
In order to assess EHIC patient and transfer payment flows between Western and Eastern Europe, we compiled, aggregated and analysed Pacolet and De Wispelaere’s (2017) data on EHIC use. Despite some missing values in the Commission dataset, we were able to track most country-to-country flow dyads, as the corresponding data are always recorded twice, namely, in the data reported by sending countries broken down by countries of destination (pp. 43, 44) and in the data reported by countries of destination broken down by sending countries (pp. 45, 46). We then aggregated country-to-country flows at regional EE and WE levels. Even if there are delays between the use of the card and the processing of the corresponding reimbursement forms and payments, the Commission’s EHIC survey provides good proxies for patient and payment flows in a given year. In order to make meaningful comparisons, we also weighted patient outflows by the population of the sending region and transfer payment outflows by total healthcare expenditure in the sending region. This allowed us to evaluate the relative size of EHIC mobility and its financial impact on WE and EE healthcare budgets.
The uneven social and spatial landscapes of EHIC possession and use
In order to acquire and then use an EHIC, EU citizens have, first, to be publicly insured in their country of residence as well as master specific knowledge of rights and administrative procedures (conditions of obtaining the card), and, second, to be able to travel abroad and to afford that travel (conditions of using the card). Given the uneven socio-spatial distribution of these resources among the EU’s population, it is not surprising that EHIC possession and use are also highly uneven.
Thus, EHIC possession is selective in the EU (39% of the population), but it is more so in Eastern than in Western Europe. In 2016, 45% of the population in Western Europe had the card, compared to just 18% in Eastern Europe (Eurostat, 2018 [demo_pjan]; Pacolet and De Wispelaere, 2017: 11, our calculations). This difference reflects both the steeper class gradient in access to insurance and healthcare and the more cumbersome administrative practices and higher barriers to accessing reimbursed cross-border care in EE compared with WE states (Vasev and Vrangbæk, 2014).
Engagement in the cross-border travel needed to make use of EHICs is likewise space and class selective. In 2016, most intra-EU mobility was for personal (non-work) purposes (138 m EU citizens), rather than work migration (only 8.4 m) (Eurostat, 2018 [tour_dem_totot]; [lfsa_egan], our calculations; see Supplemental Figure A in the online annex). Both work and non-work intra-EU mobility were directed mostly to WE countries (European Commission, 2019; UNWTO, 2018). Non-work mobility originated mainly in WE countries (88% of the EU’s non-work travellers), whereas work mobility originated as much in Western as in Eastern Europe (respectively, 47% and 53% of intra-EU labour migrants).
In 2016, Western Europeans were twice as likely as Eastern Europeans to engage in non-work mobility (respectively, 35% and 19% of the population over 15 years old) (Eurostat, 2018 [tour_dem_totot]; [demo_pjan], our calculations). This reflects the fact that access to holidays abroad displays a steeper class gradient in Eastern as compared to Western Europe (Hugrée et al., 2017). Whereas in 2014 73% of the upper classes in Romania and 97% of their counterparts in Luxembourg, Sweden, or Finland could afford at least 1 week of holidays in another European country, the corresponding figures for the EU’s popular classes differ to a much higher degree across Europe, namely, 89% in Sweden and 28% in Romania (p.173).
In contrast, in 2016, Eastern Europeans were five times as likely as Western Europeans to engage in work mobility (respectively, 5% and 1% of the working-age population in each region) (Eurostat, 2018 [lfsa_egan]; [demo_pjan], our calculations). Whereas many EE migrant workers are overqualified for their occupations in Western Europe (Leschke and Weiss, 2020), it also remains that EE work-related movers have on average lower levels of education than WE ones (European Commission, 2019: 86). Thus, popular classes in Eastern Europe engage more in work as opposed to non-work mobility.
Given the much bigger size of non-work as compared to work mobility across the EU, and the wider participation of Western Europeans across all social classes in leisure travel, it is no surprise that most EHIC users come from Western Europe. Indeed, in 2016, absolute outflows of EHIC patients from WE countries largely dwarfed those from EE countries (1.5 m as compared to 0.3 m, see Supplemental Figure B in the online annex). Interestingly, EE possessors of the card were more prone to use it than their WE counterparts (17 EHIC patients per 1000 EHIC possessors in EE countries but only 8 in WE countries) (Pacolet and De Wispelaere, 2017: 11, 43, 45, our calculations). This does not change the fact that EHIC use is overall more limited in EE, as proportionately fewer citizens possess the card (18% of the population, vs 45% in WE countries) or engage in intra-EU mobility (24% of the population, vs 36% in WE countries) (Eurostat, 2018 [lfsa_egan]; [tour_dem_totot]; [demo_pjan], our calculations).
The lower EHIC uptake among EE as compared to WE citizens reflects the bigger size of popular classes and the greater social inequalities in Eastern Europe, as well as higher institutional barriers that EE citizens must overcome to get the card. Thus, the card participates in the ‘categorization and sorting of individuals within Europe into those granted entitlements and those not granted them, perpetuating and even creating social disparities between different categories of people’ (Maas, 2008: 268).
EE migrants and EHIC mobility: Uneven landscapes of choice and constraints
Where do EE migrants situate themselves in this uneven landscape of EHIC possession and use across spatial and class divisions? Available data on EHIC use do not indicate patients’ mobility status. We therefore evaluate EE migrants’ place in EHIC flows based on an assessment of their transnational mobility patterns.
EE migrants are prime characters in the EU’s new patterns of temporary mobility (Favell, 2008) and thus move between a variety of statuses. An EE secondary school student, for example, may visit her relatives working in a WE country (as a tourist), decide to stay on for the summer and work in the hospitality sector (thus becoming a migrant worker), and then return home to continue her studies (student). Later, she may respond to weak employment prospects in her country of origin and leave again for the same destination country to visit her relatives (tourist) but also search for a job (job seeker). Throughout her migration trajectory, she is first linked to her home country through her passport (home country resident) and entitlement to its health insurance (home country insured person). However, on finding employment in the host country (migrant worker), she may thereafter stay long enough to fulfil ordinary residency requirements (host country resident) and be covered by its public healthcare scheme instead of that of her country of origin (host country insured person).
EE migrants may thus avail themselves of the EHIC in two situations. One is when they keep their residence and insurance status in their country of origin to obtain the EHIC and eventually use the card during their temporary stay in another member state. The second is when migrants change their residence to the host country, obtain healthcare coverage and an EHIC from the latter, and then use the card to access care while temporarily travelling to another EU country (including their country of origin).
In looking at the two situations (EE migrants having, respectively, EE and WE cards), we note that EE migrant workers often diverge from images of EU consumer-citizens or migrants who have real choices in relation to travel, work, healthcare insurance, or cross-border care. Rather, studies on EE migration have shown that migrants’ decisions are embedded in larger social constraints. These include the need to support themselves and their families, and consultations with other family members (Potot, 2008) in response to poor employment prospects and working and welfare conditions in their country of origin (Meeus, 2013). Once in the host country, EE migrants’ decisions as to when, where and what type of jobs and health services to access are constrained by the structure of employment and welfare in the home and, even more importantly, in the host country (Ehata and Seeleib-Kaiser, 2017; Faist, 2017).
In the following two sub-sections, we discuss migrants’ cross-border care strategies in the two situations outlined above. We also assess these strategies considering migrants’ social class and thus look at migrants’ uptake of social citizenship rights to cross-border care from a distributional perspective.
EE migrants with EE EHICs
We first consider the case of EE migrants who maintain their affiliation to the public healthcare scheme in their country of origin. Often, far from taking this decision freely, they do so because their entitlement to healthcare coverage in the host country is restricted by habitual residency requirements (Bruzelius et al., 2015) – and this applies particularly to the large contingent of temporary EE migrants engaged in short stints of work abroad. Nonetheless, even after fulfilling the habitual residency requirement, EE migrants may lack knowledge of rights and health services in the host country (Ehata and Seeleib-Kaiser, 2017; Scheibelhofer and Holzinger, 2018) and thus continue to avail themselves of coverage in their home country as a backstop. Finally, some of those in the younger working age bracket deem that they do not need healthcare at all and thus end up being covered neither in their home nor in their host country.
The degree of freedom of choice versus constraint involved in EE migrants’ decisions on healthcare coverage also depends on their social positions and the ways in which they deploy their social, symbolic and economic resources (Bourdieu, 1986) in both their home and their host countries. Thus, lower-skilled EE migrants have fewer chances of finding in their home countries jobs that adequately provide for their subsistence (Stan and Erne, 2014) and are therefore subject to greater constraints than their higher-skilled, higher-waged co-nationals in considering the prospect of working abroad. Similarly, as we have seen, the high selectivity of EHIC possession in EE countries (where less than 1/5 of EE citizens have the card) points to its steeper class gradient, with higher-class, better educated citizens being more likely to obtain the card than lower-class, less educated ones.
Even when they do possess an EE EHIC, EE migrants’ use of the card is far from resulting from their free choice. As mentioned above, unplanned care accessed through the EHIC has been extended beyond the strictly immediately necessary care of the first Regulations to include various degrees of emergency. This opens the possibility for the EHIC to cover care that is certainly medically necessary, but that could be, to a certain degree, postponed. However, the large contingent of EE migrants engaged in jobs with low wages and low employment protection are not only more exposed to work hazards (Ronda Pérez et al., 2012), but also, in the case of illness, more often face the imperative need to rapidly resume work – and of making potentially life-changing decisions about accessing or postponing care.
Thus, when still attached to their home country’s healthcare resources (including the EHIC), the engagement in cross-border care of EE migrants from lower social classes is an expression of the constraints of their mobility and employment status rather than a reflection of their free choice between health services in their home and their host countries. In addition, the low EHIC uptake in Eastern Europe suggests that the ‘choice’ that most EE citizens (including mobile ones) face is often one between sticking to their home country’s public health services or not availing themselves of any healthcare coverage at all.
EE migrants with WE EHICs
Given its dependence on knowledge of specific rights, administrative procedures and complex healthcare systems (needed to obtain the statuses of ‘resident’ and ‘insured’ required by the card), EE migrants’ uptake of the EHIC in their host countries is likewise class dependent. Longer-staying EE migrants may manage to fulfil habitual residency requirements and thereafter obtain entitlement to public healthcare in their host country. However, they also encounter important barriers to accessing health services (Ehata and Seeleib-Kaiser, 2017; Scheibelhofer and Holzinger, 2018), most importantly in terms of knowledge of language, rights, administrative procedures and health system configurations. True, Western Europe displays higher levels of EHIC possession than Eastern Europe. Yet, given that medium and low education levels prevail among both EE movers and stayers, the acquisition of the EHIC is more class selective among EE migrants than among the native population of their WE host country.
EE migrants possessing a WE card therefore also bifurcate in their use of it, depending on their socio-economic status and integration in the host country. A fringe of higher-skilled, higher-paid EE migrants who are better integrated in host countries may mimic native residents in using the card when travelling abroad (mostly as tourists) as an addition to (rather than a substitute for) these countries’ health services (Vollaard, 2006).
In contrast, most EE migrants, that is, those in lower-skilled, lower-paid jobs, display both dissatisfaction with health services in the host country and familiarity with health systems in their home country, two main drivers of recourse to cross-border care (Vollaard, 2006). This recourse is informed both by their preference for healthcare in their country of origin (choice) and by the barriers to care that they encounter in their host country (constraints).
More importantly, west–east EHIC patient flows (less than 0.5 m, see Supplemental Figure B in the online annex) are relatively modest in comparison to the total number of EE migrants residing in Western Europe (more than 4.4 m, see European Commission, 2019). This indicates that, even if EE migrants were a significant contingent in patient flows from WE countries (Horsfall, 2019), their use of the EHIC to access cross-border care is marginal to their overall transnational healthcare practices. As several studies have documented (Ehata and Seeleib-Kaiser, 2017; Migge and Gilmartin, 2011; Osipovic, 2013; Sime, 2014; Stan, 2015; Węgrzynowska, 2016), EE migrants, and most particularly those in lower-skilled, lower-waged jobs, respond to barriers to accessing healthcare in their host country in a variety of ways. These include consultations in medical practices established by EE physicians in the host country; informal advice and care from family members, friends and acquaintances; and accessing health services in their countries of origin. Both EE medical practices in host countries and health services accessed by migrants in home countries are mostly situated in the private sector – and thus are not included among services covered by the public health schemes in either location. The casual ‘return medical journeys’ in which EE migrants engage during their frequent visits back home amount therefore to a much larger overall patient mobility, of which mobility fuelled by EU cross-border care legislation, let alone the EHIC, is only a small fraction.
Many lower-skilled, lower-waged EE migrants thus choose to use some of their savings to avail themselves of care in their country of origin, for which they pay privately. Insofar as they do so, they fail to enact not only social rights to healthcare in their host country, but also EU citizenship rights to cross-border care, and enter the realm of healthcare consumerism. 3 This is a part-constrained, part-chosen consumerism, whereby EE migrants’ visits back home become an occasion for them to both fulfil their own and their families’ healthcare needs (constraints) and make visible their social mobility by availing themselves of the ‘choice’ of private healthcare (Węgrzynowska, 2016). Rather than being iconic European consumer-citizens, many lower-skilled, lower-waged EE migrants have instead both chosen and been pushed to avail themselves of the rising private health services that over the last decades have mushroomed across the EU (André and Hermann, 2009), including in Eastern Europe (Stan and Toma, 2019).
Distributional effects of uneven EHIC patient and payment flows across Europe
Given the uneven landscape of EHIC possession and use across the EU, including among EE migrants, what are their distributional effects on healthcare resources across Europe? The overall size of EHIC patient and payment flows is still small in comparison to domestic healthcare. 4 Nonetheless, in border regions (Vollaard, 2004) or countries with limited financial resources, like EE states, the impact of EHIC flows may be much more significant.
EHIC patient and transfer payment outflows are uneven between Western and Eastern Europe (see Supplemental Figures B and C in the online annex). As stated, absolute outflows of patients and payments from Western Europe are considerably higher than those from Eastern Europe. The same applies to patient and payment outflows from Western to Eastern Europe as compared to those in the opposite direction (respectively, 0.5 m patients and €160 m, vs 0.2 m patients and €68 m).
Certainly, EHIC patient and payment outflows also reflect considerable differences in population size and total health expenditure between the two regions. Figures 1 and 2 show that, relative to the situation in the sending region, patient outflows from Eastern Europe are still significantly lower than those from Western Europe (respectively, 3002 vs 3782 EHIC patients per 1 m population, or a 20% difference). In contrast, relative payment outflows from EE countries are significantly higher than outflows from WE countries (respectively, €647 vs €503 per €1 m total health expenditure).
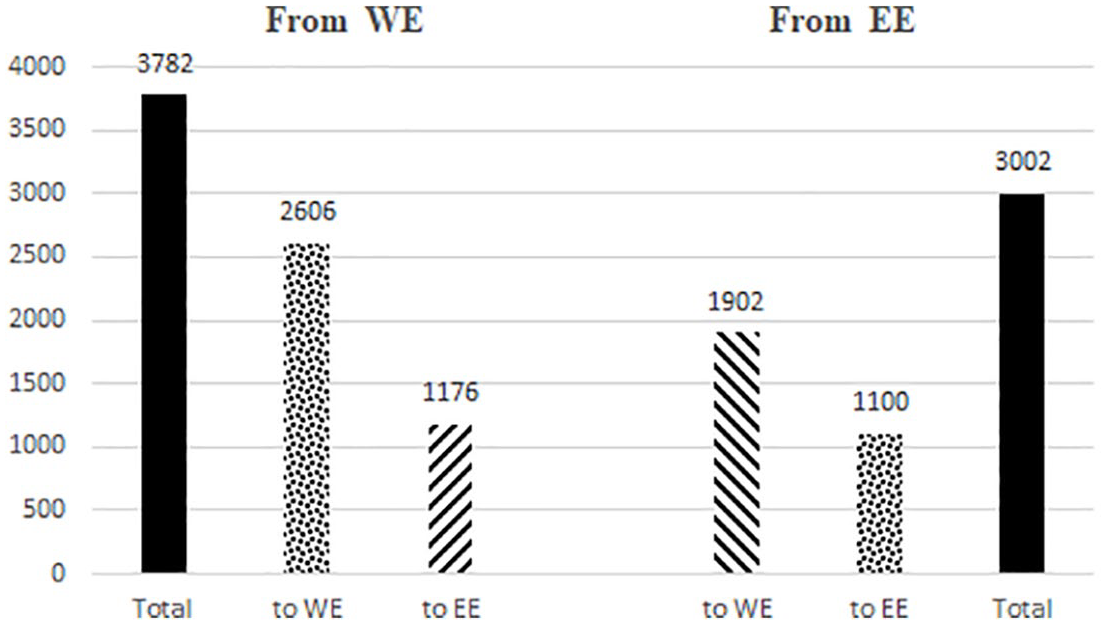
Outflows of EHIC patients, weighted per 1 m population in sending region, 2016.
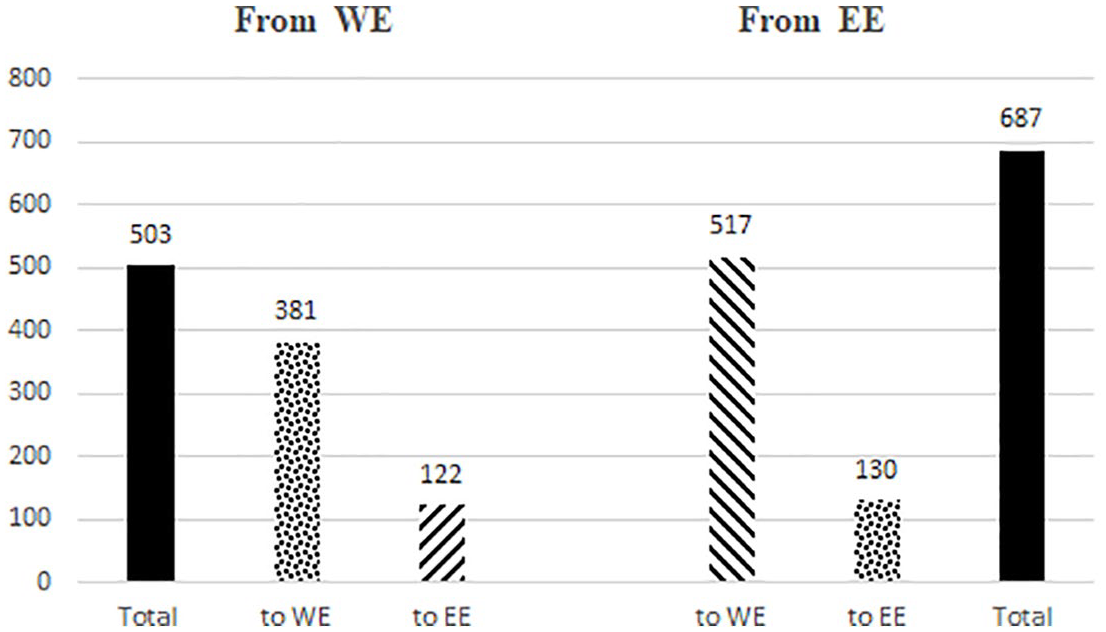
Outflows of EHIC payments, weighted per €1 m total health expenditure in sending region, 2016.
More importantly, in relative terms, EHIC payment outflows from Western to Eastern Europe (€122 per €1 m total health expenditure) are much smaller not only than east–west outflows (€517), but also than outflows internal to Western Europe (€381). Otherwise said, WE countries’ EHIC payments go more to other WE countries than to EE countries.
All in all, our analysis of EHIC payment flows contradicts the idea that EHIC mobility between Western and Eastern Europe constitutes a drain for Western Europe. Rather, it is Eastern Europe that faces the highest relative drain of money resulting from EHIC mobility between the two regions.
The east–west imbalance in the relative financial burden of EHIC mobility results from the combination of imbalances between the two regions in patient flows (as seen in Supplemental Figure B in the online annex) and in average healthcare costs. Average prices claimed per patient in EHIC flows to Western Europe were 1.5 times higher than average prices claimed in flows to Eastern Europe (respectively, €451 and €300 per patient) (Pacolet and De Wispelaere, 2017: 43–46, our calculations). Likewise, our calculations based on Lorenzoni and Koechlin (2017) indicate that, in 2016, average prices for healthcare were more than twice as high in the 13 selected WE countries as in the seven selected EE countries. And yet, these price differentials do not make the corresponding east–west EHIC payment imbalances unproblematic. They only confirm that Western and Eastern Europe are differently positioned in an uneven European healthcare space, most notably in terms of use of costly medical technology and more highly paid medical practitioners.
EE migrants’ participation in EHIC mobility has similar uneven distributional effects on Western and Eastern Europe. If EE migrants use EE cards to access services in WE countries (and are thus part of east–west EHIC flows), their cost constitutes a drain on EE countries’ healthcare resources, as the latter have to cover WE care costs, which are on average higher than those provided domestically. In turn, if EE migrants use WE cards to avail themselves of cross-border care in their home countries, this constitutes a saving rather than a drain on WE healthcare resources, as the latter have to cover costs for health services in EE countries, which are on average lower than those in WE countries. Moreover, EE migrants’ use of privately paid healthcare in their home countries constitute an additional saving for WE countries.
Overall, EE migrants’ participation in EHIC mobility leads to savings for WE host countries but to losses for their EE countries of origin. Insofar as this participation results in outflows of cross-border care payments from already meagre healthcare resources in EE countries, it contributes to reproducing and even enhancing the structural inequalities between WE and EE healthcare services.
Even so, WE Eurosceptics have repeatedly targeted west–east EHIC transfer payments for EE migrants residing in their country, rather than the much more sizeable payments to other WE countries for their native citizens, to justify their claims about the alleged misuse of WE healthcare resources by mobile EE citizens. These fears thus ultimately reflect not so much the importance of actual EHIC payment outflows, as the issue of EE migrants’ citizenship status and entitlement to public healthcare resources in their host countries. Indeed, they spring from the assumption that, as foreigners, EE migrants do not make their due contribution to their host societies and therefore lack legitimacy in their claims to these countries’ healthcare resources. Rather than drawing on the criterion of residency enshrined in EU citizenship (Kostakopoulou, 2007), this view of citizenship draws on narrowly defined employment, ethnic and even racial (Fox et al., 2012) criteria, which exclude non-nationals and those in precarious employment – that is, a group which is including many EE migrants.
This narrow view of citizenship pits foreign and native sections of the lower classes against each other, while legitimizing the transnational class inequalities in which intra-EU and EHIC mobility are embedded. These inequalities configure cross-border patient mobility across Europe as a socially divided field. At the upper end of the cross-European class gradient, a select group of citizens from both Western and Eastern Europe engages in intra-EU mobility, mostly for non-work purposes, having also managed to appropriate the EHIC and the publicly covered cross-border care to which it gives access. Lower down the class gradient, lower-waged EE migrant workers respond to barriers to accessing their host countries’ public health services by returning to their countries of origin to avail themselves of private healthcare. Still further down, disenfranchized EU citizens (mostly, but not exclusively, located in Eastern Europe) find themselves excluded from entitlement to public health services in their country of residence, and the mobility and cross-border care assets that come with it, and either tap into their networks for informal care or abstain from care in the first place (Stan and Toma, 2019).
Conclusion
The EHIC pathway to unplanned cross-border care has not attracted much attention from EU healthcare experts, as most of them see its operation as unproblematic. Instead, they have studied planned cross-border care (Carrera and Lund, 2010) or the role of medical tourism in the making of an EU healthcare market (Mainil et al., 2017). In contrast, scholars of European social citizenship have cited the card as a tool to foster European citizenship, increase the visibility of Social Europe, and bring Europeans together (Bauböck, 2019; Maas, 2008).
After the EU eastern enlargements and the austerity cuts adopted after the 2008 crisis, however, EHIC mobility became an increasingly divisive issue. First, EHIC mobility involves more people and higher cross-border payments compared with the EU’s planned cross-border care pathways. Second, the EHIC connects public healthcare systems, whereas medical tourism is a private affair. The greater visibility of EE migrants and the public service dimension of EHIC mobility thus offered WE Eurosceptic movements a lever that they could use to politicize it. The more a policy is politicized, however, the more attention must be given to its material effects (Bruzelius et al., 2017). Therefore, we assessed: (1) the extent to which EHIC mobility, and EE migrants’ participation in it, translates into substantive differences in EU social rights across regions and classes and (2) the distributional effects of EHIC mobility on WE and EE healthcare services.
On the first question, our analysis shows that EU citizens’ participation in EHIC mobility is differentiated along spatial and class lines. EE migrants’ participation in EHIC mobility is a function of the constraints of the EU’s migration system and class divisions among EE migrants. Therefore, EHIC mobility in the uneven European healthcare space translates into substantive differences in social EU citizenship rights. This, however, does not simply reflect mobile EE migrants’ low uptake of health services in destination countries and their preference for services in their countries of origin (Ehata and Seeleib-Kaiser, 2017). Instead, their uneven participation in EHIC mobility is permeated by both inequalities between natives and migrants and (transnational) class inequalities among (more or less mobile) WE and EE citizens (Amelina, 2017; Heidelmaier and Blauberger, 2017; Lafleur and Mescoli, 2018). Our study thus shows that the EHIC’s operation amplifies rather than reduces healthcare inequalities between people in different regions and social classes.
On the second question, our analysis shows that EE citizens’ use of rights to unplanned cross-border care constitutes a gain rather than a drain for WE health systems. The fears of WE Eurosceptics are thus unjustified. On the contrary, the existing EHIC disbursement mechanisms result in a higher relative financial burden for EE healthcare systems. The more EE migrants participate in EHIC mobility, the more WE health services profit from the corresponding transfer payments. Whereas EHIC disbursement mechanisms formally treat all national healthcare systems equally, the substantive differences in EE and WE healthcare costs have created an EU healthcare union that distributes the costs of EHIC mobility at the expense of EE healthcare systems. The EHIC is therefore hardly a tool of social integration, as it serves to reinforce both spatial divides between national healthcare systems and social divides between social classes. If, however, the EHIC is really meant to become a tool of EU citizenship and social integration, it should reduce rather than amplify these divides.
Our findings therefore make an important contribution to current debates about the future direction of the EU’s healthcare union (Vollaard et al., 2016) and solidarity in the EU (Bauböck, 2019). The article shows that the feeble cost-sharing in Europe’s federal healthcare system has important distributional implications for social citizenship in the EU. These implications were pithily captured by the president of the Romanian health insurance fund (CNAS): ‘In the last eight years we have settled healthcare bills of over half a billion euros abroad, while we have issued invoices for only five million euros. [. . .] Imagine what we could have done if this money had remained in the country!’ (Statul român a decontat o sumă uriașă pentru tratamente în străinătate, Gândul, 4 Oct. 2018, our translation). Perhaps a pathway to more sustainable EHIC mobility would consist in using EU funds to cover the difference in healthcare costs between richer and poorer member states, as already trialled in a pilot project on planned cross-border care in the Czech-Austrian borderland (Böhm and Kurowska-Pysz, 2019).
Our study is also politically relevant given ongoing concerns about the social rights of EE migrants in Western Europe and the politicization of cross-border care in both Western and Eastern Europe. The Covid emergency made the reliance of the WE economy on seasonal EE workers much more evident, notably in agriculture, food processing and elder care. The emergency also led to a legislative proposal for an ‘EU4health’ programme with a budget of €9.4 billion, as the Commission recognized that ‘there are a number of further challenges in the areas of health security and health systems impeding their overall functioning . . . in particular: inequalities in health status among population groups, countries and regions and access to affordable, preventive and curative health care of good quality’ (European Commission, 2020: 1). It remains to be seen whether European social and political actors will seize the opportunity provided by this proposal and press for it to be used to address the inequalities in cross-border care highlighted by our study.
Supplemental Material
sj-pdf-1-esp-10.1177_0958928720974188 – Supplemental material for Bringing EU citizens together or pulling them apart? The European Health Insurance Card, east–west mobility and the failed promise of European social integration
Supplemental material, sj-pdf-1-esp-10.1177_0958928720974188 for Bringing EU citizens together or pulling them apart? The European Health Insurance Card, east–west mobility and the failed promise of European social integration by Sabina Stan, Roland Erne and Susan Gannon in Journal of European Social Policy
Footnotes
Acknowledgements
We thank the three anonymous reviewers of the Journal of European Social Policy, as well as Janine Leschke, Martin Seeleib-Kaiser and Catherine O’Dea for their very helpful comments and suggestions on earlier versions of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project has received funding from the European Research Council (ERC) under the European Union’s Horizon 2020 research and innovation programme, grant agreement No 725240 (Erne, 2018) and from the School of Business, University College Dublin.
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.