
Abstract
This review focuses on the concept of care, a concept that has never been more popular as a focus of study. It undertakes a critical review, motivated by the breadth of the field and the lack of coherence and linkages across a diverse literature. The review concentrates first on organizing and reviewing the literature in terms of key focus and, second, drawing out the strengths and weaknesses of existing work and making suggestions for how future work might proceed in COVID-19 times. While the existing literature offers many insights, some quite basic things need to be reconsidered, not least definition and conceptualization. Defining care as based on the meeting of perceived welfare-related need, I develop it as comprising need, relations/actors, resources and ideas and values. Each of these dimensions has an inherent disposition towards the study of inequality and it is possible, either by looking at them individually or all together, to identify care as situated in relations of relative power and inequality. The framework allows a set of critical questions to be posed in relation to COVID-19 and the policies and resources that have been mustered in response.
Introduction
Care is the term used to refer to the labour, resources and relations involved in the provision of care and assistance for those requiring it. It is an encompassing concept; in social policy, for instance, it is commonly applied to early childhood education and care, long-term care, parental and other leaves and personal assistance for children and ill, disabled and frail adults. The concept has catalysed a large literature and has never been more popular as a focus of study. One might imagine that it can only become more important as we learn to live with COVID-19. Part of care’s appeal is that it allows us to take an integral feature of people’s lives to fashion a line of analysis that reaches deeply into society. Not only is the field vibrant but it is strongly comparative and increasingly global. As a result, the concept can claim to point to large trends in marketization, welfare state reform, transformation of private life, globalization (with up to half of the world’s female migration estimated to be associated with care in some way or another) (Peng, 2019).
That said, there are some inherent difficulties with the concept and problems in the way it has been applied. One problem is that care does not have a clear meaning or set of references – some work speaks of ‘care’, some of ‘long-term care’ and some of ‘social care’. In addition, the concept has been applied to mean profoundly different things, stretched to cover highly-abstract philosophical matters to the minute details of everyday life. As a result, it is not always clear what we are evoking when we say our research is about care, and sometimes there is no basis for a fertile conversation among perspectives. Moreover, the field has many gaps, not least between research on how provision to meet care need is institutionalized and that of articulating care as a relational practice and set of values.
In this review, I seek to make sense of the different literatures and draw out further the potential in the concept. A core question revolves around whether care can be more than a repository for a wide range of loosely-connected work. I suggest it can but that, first, we need to lay bare the span of the field and, then, undertake some key clarifications. Review is timely, especially in the context of the lethal COVID-19 virus which poses unprecedented care-related challenges. Within that context, I take this thematic review as an opportunity to reconsider the concept’s integral features and capacities as well as making suggestions for clarifying its focus for research and thinking.
The contribution is in two main parts. The first considers existing work in terms of the main sets of literature and evolving research themes. The article’s second part offers some needed clarifications and suggests elements of a research agenda going forward using the COVID-19 pandemic as a focusing lens. Given my interest in assessing the literature, I am led by the existing work which draws mainly from European and other Western countries. 1
Care as a focus of study
The academic literature on care is some 30–40 years old. In many respects, care had to be ‘discovered’, an everyday, taken-for-granted phenomenon seen through new eyes. The two main tracks to this process of ‘denaturalization’ were: work on women, family and private life; research on the medical/health system and services for frail older and ill adults and children. From these roots the field developed in four main literatures: care as labour and value orientation; care as a component of welfare state policy; care in the context of the organization and effectiveness of service provision; care as embedded in global processes. Although I will treat them separately for the purposes of review, the landscape is interstitial with considerable cross fertilization. Notably, the field as a whole is inherently cross-disciplinary, with vital inputs from social policy, gender studies, health sciences, economics and political philosophy.
Care as labour and relational orientation
The first – for some the cradle – is scholarship focused on the labour and relationships involved in maintaining family life and connectedness in kinship. Much of this was feminist or gender inspired. It trained the spotlight on women’s work in responding to the needs of others and maintaining the household. There were many micro-level studies of the tasks involved in domestic carework (like tending, dressing, feeding, nurturing). The aim was to reveal the reality of providing care and give recognition both to the activities and those who undertake them (Graham, 1983; Waerness,1984). With the focus on the labour and type of engagement involved, I see caring rather than care as the conceptual terrain here. Over time, the field was expanded to take in a wider range of actors and settings (formal carers, migrant carers, male carers and care outside the home). Macro-level theorization mirrored the interest in micro-level engagement. The domestic division of labour and social reproduction were concepts developed to place care in the context of economic and other forms of power. Unpaid care labour was analysed as part of ‘the family under capitalism’ (Dalla Costa and James, 1975; Duffy, 2005). Scholars made important arguments about the specificity of the domestic economy and its contribution to capitalism, locating the treatment of care under economic and social policies as drawing lines of gender, class and other forms of inequality.
In a more positive framing, the study of emotional investment and complexity (‘love’ but also ambivalence) moved scholarly thought beyond the tasks and functions served. Now we see care in a much broader light, located within but also beyond the home and elaborated as a vital way of relating to others and to our world. Care is imbued with moral purpose. It is a universal entity, a way of being in the world. Its reach infinite, it applies to the universe and environment as much as to the persons we live with or alongside. The work of Fisher and Tronto (1990) is classic here in defining caring as a generic species activity involving four registers: caring about; caring for; care-giving; care-receiving. Emphasizing relationships and dispositions, care-giving is developed as an ethical orientation and practice, requiring attentiveness to need, willingness to respond to it, direct action (care-giving) and reaction to the care process (and hence to the person receiving care) (Graham, 1983; Tronto, 1993).
To summarize, this literature opens our eyes to the presence and significance of care labour and the process of caring as involving emotional investments and ethical orientations. The activities and dispositions are elaborated, especially from the perspective of the carer, and care provision is shown to be part of a much larger set of relations in capitalist systems. There are real tensions and contestations in this literature, though, especially about the place of care in the feminist project and whether it should be valued and rewarded as a distinct set of engagements or treated as equivalent to paid work (Sainsbury, 2013).
Care, social policy and the (welfare) state
A second strand of work explores how the welfare state engages with care and in doing so adjudicates on what is considered deserving of public support. The rights and entitlements granted to mothers (and increasingly fathers) and/or carers of disabled, ill or frail adults are especially interesting in this context, as are the claims of those who require care. Whether studying care for children or adults, this work excels at uncovering the different modalities of provision. We now know these to include a range of employment leaves, working time flexibility, taxation reliefs, vouchers for purchasing services, care-related credits for pension and other benefits, as well as a host of service-based responses (Daly, 2002; Ranci and Pavolini, 2013; Saraceno and Keck, 2010). One important contribution has been to differentiate types of care – home care as against institutional care, formal as against informal care – and how the welfare state shifts the boundaries between them (Leira and Saraceno, 2002).
In a challenge to existing theorizations, it is now accepted that a breadwinner model – grounded in the ideology of woman as carer and family as private – widely underpinned the classic welfare benefits (Lewis, 1992). Moreover, the extension of rights around care has been shown as an important arc of both the reform of welfare states over time and associated politics. Weighty concepts like citizenship have been re-envisioned, in terms of unpaid work as a (potential) source of rights, for example, and challenges posed to the liberal notion of citizens as independent and autonomous individuals (Hernes, 1987; Knijn and Kremer, 1997; Sainsbury, 2013). Inequalities and hierarchies in regard to the needs or exigencies that are recognized and supported have been shown to be baked into a tiered and divided welfare state.
It is insightful to briefly consider the line of development of this most prolific field of study. In a first notable trend, scholarship has become increasingly comparative, examining care as integral to welfare state variation. This way of thinking has facilitated configurational approaches, through identifying care regimes, for example, and bringing the care literature into closer conversation with the welfare state regime scholarship (for example, Bettio and Plantenga 2004; Saraceno and Keck, 2010). The concept of the care diamond was developed to theorize the broad settings and politics of care which span state, family, market and civil society (Razavi, 2007). Secondly, a focus on institutions – in the sense of the architecture of benefits and services – has come to overshadow some of the original interests in politics and inequalities. There is a strong impetus in contemporary work towards categorization and what might be called ‘micro’ studies – increasingly detailed analysis of single policies. Outcomes are widely studied in terms of concepts that tend to be used descriptively rather than theoretically – for example familialization/defamilialization, work/life balance.
Taken as a whole, this work reveals how we can read key aspects of the history and orientation of welfare states through the lens of care. The configurational approach emphasizes the connections between the organization of care (public vis-à-vis private, women alone or with the help of men and/or supportive services) and (often gendered) norms and values about the appropriate response to need from the collective institutions of family, market, state and community. Over time, work on care and the welfare state has become narrower in the sense of focusing on the details of institutions or single policies, somewhat downgrading the focus on power, politics and economics that drove earlier work.
System functioning; Appropriate care-related interventions
The third literature is related to the second in its interest in care as a domain of need and exigency but its focus is on the service responses, in terms of functional, organizational and financial/funding particularities. This literature is very diverse – in its focus but also disciplinary orientation – and is the most difficult to bring together under a single rubric.
‘Delivery’ and ‘meeting need’ are keywords in this literature, deriving from a focus on the system of provision as squeezed between external pressures (such as population ageing and the growing prevalence of dementia-related conditions) and available resources (OECD, 2004). Viewing provision in terms of a welfare mix (rather than care diamond for example), the service infrastructure is scrutinized for efficiency and effectiveness in meeting need (Sirovátka and Greve, 2017). Differentiating the field from healthcare is an important contribution, in particular by highlighting the history of personal social services to support families and communities with their ageing members (Sainsbury, 1977; Anttonen and Sipilä, 1996). Community care and deinstitutionalization of long-term care also draw the interest of scholars here. This literature is less oriented to theory-building as compared with the other two and it problematizes gender inequality considerably less so. What animates it especially are matters of resource use and the extent to which the aims and orientations of provision are realized and measurable in outcomes for systems and their users. New public management ideas find a receptive place in some of this literature, applied to review innovations such as personal budgets, reablement and the application of robotic and other technologies. The field is especially marked by an interest in measurement, for example the use and development of schema for assessing levels of need and potential outcomes like ASCOT (Adult Social Care Outcomes Toolkit). 2
When it looks at more macro considerations, this literature is especially interested in governance, tracing care provision to the relationship between the state and local municipalities (Anttonen and Sipilä, 1996; Martinelli et al., 2017). There is also a growing body of work on vertical and horizontal responsibilities, associated with, for example, decentralization and other processes that have led to the reshuffling of responsibilities and funding between bureaucratic levels and entities (Martinelli et al., 2017). Care markets and marketization of care are also important empirical lines of enquiry.
Taken in broad strokes, this literature explores care as a human need and exigency which calls forth a variety of organizational and governance-related responses, especially in health and human services. These are seen to merit investigation especially for their functionality and outcomes, in scholarship marked by quite a specialist set of interests.
Care and global systems/processes
The fourth literature is also concerned with socio-spatial dimensions, but it locates care in the geopolitics of global systems. Its driving interests are to make linkages between the conditions under which care is carried out in different parts of the world and to see how an increasingly unstable care regime in the Global North is leading to new inequalities and relations of care worldwide (Yeates, 2012). Both feminist and critical development perspectives are leading disciplines. This literature picks up on and develops some of the core themes in earlier feminist work on care as reproductive labour and as associated with power and inequality and marries them with critical theorizations of globalization and colonialism. It increasingly uses frameworks that connect micro, meso and macro levels (known as ‘multi-scalar’ approaches) (Michel and Peng, 2017; Williams, 2018). There has been much study of the voices and experiences of the migrant care worker and the different relations that she has to manage, including her own family’s care needs (Baldassar and Merla, 2013; Parreñas, 2001). Among the trends identified more broadly are, first, an internationalization of care labour and a growing global care labour market (prior to COVID-19 anyway) that strongly influences migration patterns (Michel and Peng, 2017; Yeates, 2012). A second trend is of growing inequalities and the role of increased outsourcing of care work by families and public authorities in reproducing gender, class and racial inequalities (echoing formations of a class of domestic servants which featured prominently in earlier work) (Aulenbacher et al., 2018).
Its conceptual lynchpins include global care chains (Hochschild, 2000; Yeates, 2012), care circles and transnational social inequality (Lutz, 2018). All of these emphasize care as globally mobile – think of the movement of care workers and companies around the world. One of the main messages from this work is a need to broaden the paradigm – conceiving of care as part of a gender, care and migration regime. This, in turn, requires a recognition that practices and conditions in parts of the world which appear remote from each other are closely connected and interdependent (Michel and Peng, 2017; Williams, 2018). We are especially forced to rethink the nation state as the unit of analysis, although it continues to be important to pay attention to national contexts and policies (Sainsbury, 2013). This literature is frequently intersectional in its thinking. It is especially predisposed to integrate race and ethnicity along with gender and social class into the story of care and to enquire how policies on race, ethnicity and migration interact with care practices and care policy.
This literature, taken as a whole, returns to themes of inequality and oppression, broadening the sphere of analysis, connecting different scales and locations of care and pinpointing how care-giving (and often care-receiving) crosses borders and can be a conduit of inequality. A weakness in earlier work – underemphasizing the national policy context – is being addressed, especially by multi-scalar approaches and a more complex conceptualization of national policies as intersecting regimes (economic, health, social, migration).
How do we assess and take forward these insights?
Taking stock and looking forward
This section first suggests some necessary clarifications and then highlights possibilities for research going forward, with COVID-19 in the foreground.
Strengths and weaknesses of the concept and the literature
One striking feature of the care literature taken as a whole is that it places care at the centre of analysis rather than at the margins (Peng, 2019). This lends the concept a systemic focus. Although the respective literatures conceive of the underlying ‘system’ differently (caring dyad, family and kinship system, social service system, welfare state, gender order, global and national capitalism), they share a preference for configurational thinking. A second cohering interest is in organizational factors – how individuals, families, communities, companies, states and/or economies organize for and resource care. The seeds of this interest were present in some of the original scholarship as far back as 40 years ago, and the field has gone on to reveal complex and changing intersections between the welfare state, family, economy and community.
It is important not to overstate the strengths or commonalities, however. One main criticism of the care literature (and of care as a concept) is about the relative ‘silencing’ of the voice of the person needing care, especially adults. This is a critique levelled by some disability activists and researchers, and is especially directed at earlier work (Morris, 1991; Shakespeare, 2013). It is not just that the person receiving care was secondary – they were often rendered as dependent and objectified. This was manifest in a tendency to view them mainly in terms of their needs rather than their full personhood and agency; the terms ‘care-recipient’ and ‘care-receiving’ conveying a passive register. As a counter to this position, the notion of care as located in relations of interdependency has developed (Barnes, 2012). I see another potential weakness in some of the scholarship as well – the tendency for the study of the rules and conditions attaching to benefits and services to be an end in itself, the underlying objective being to classify rather than explain. This, as mentioned, tends to sideline the critical roots of the concept of care and its capacity to interrogate policy’s role in perpetuating inequalities, asymmetrical control over resources and other relations of power.
Hence, to progress care as a field some fundamental issues need to be addressed.
Key clarifications: Conceptualization and constituent elements
As will be obvious, care – which is used as both noun and verb – has many meanings, even in everyday conversation. It is not just the polysemy that is challenging though – it is the complexity. Specification is therefore crucial. It is notable that many definitions remain at a general level, especially those drawing from a care ethics perspective. For Held (1996) care is a cluster of values and practices; Tronto (1993: 103) views care as ‘a species activity that includes everything that we do to maintain, continue and repair our “world” so that we can live in it as well as possible’. Obviously, care is boundaryless in this framing. In contrast, those researching the field of policy and provision are more inclined to ground their conceptualization in the practice of care: for Kremer (2007: 28) care is the provision of daily socio-psychological, emotional and physical attention to people; for Daly and Lewis (2000: 285) care encompasses ‘the activities and relations involved in meeting the physical and emotional requirements of dependent adults and children, and the normative economic and social frameworks within which these are assigned and carried out’.
Having a grounded definition is very important for the purpose of policy analysis. Scholars need to know what the foundations of care are and what precipitates public recognition of care need (de São José, 2016). I suggest that perceived need – and especially welfare-related need – should be thought of as at the core of a policy-oriented conceptualization of care. I am guided here by an observation by Leira and Saraceno (2002: 62) that only caring in relation to a need is an issue for social policy intervention (unlike broader conceptions of care). Scholarship tells us that need may be defined narrowly or broadly (Dean, 2010), depending on whether the focus is on what is essential to survive and/or flourish (Doyal and Gough, 1991). I am not prescribing either usage, but I do want to underline a number of points of clarification. First, we have to recognize an association between need and vulnerability. Those experiencing need may have physical vulnerability or emotional/psychological vulnerability and they may also be in an economically and socially weak position. This indicates that any framework must comprehend relations of hierarchy and relative powerlessness. Second, I am suggesting that need be seen as a phenomenon that is both interpreted and deeply political (Fraser, 1989). My conceptualization also brings in a sense of need as perceived exigency, a felt compunction to act which means that giving and receiving of care cannot be conceived of independently of each other.
Care I define, then, as a vital sphere of human engagement and welfare-related activity focused on practices oriented to meeting perceived need.
This, as it stands, is mere description. To advance a more dynamic understanding we can draw on the insights of existing scholarship about component elements and defining features of care and the significance of the conditions in which care is situated (Barnes, 2012; Leira and Saraceno, 2002; Rummery and Fine, 2012). I suggest that there are four key component elements, which I organize as a configuration (see Figure 1). These are: need, relations and actors, resources and ideas/values. I theorize care, then, as situated at the intersection of need, relations/actors, resources and values.
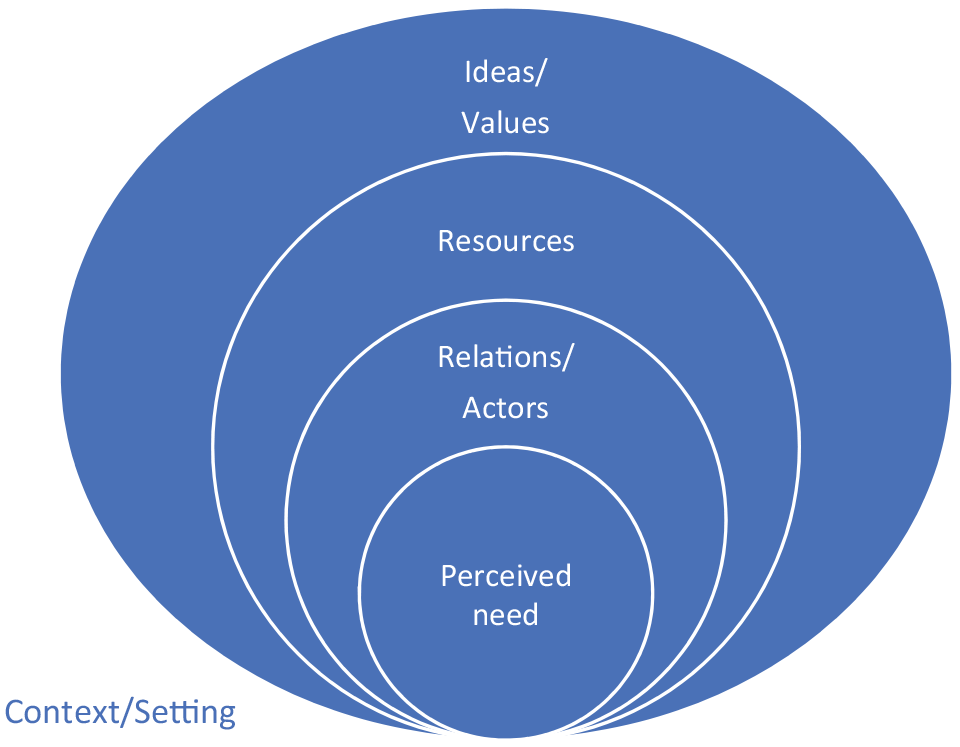
Care as configuration.
‘Relations’ signify care as a set of relational practices connecting all those involved in providing and/or receiving care. Focusing on relations moves the dial away from both individualized conceptions of care and dichotomous thinking to emphasize processes. It also avoids the passive register. In addition, adding actors in gives recognition to the breadth of agency and how the relations of care involve agency on the part of different actors. ‘Resources’ is conceived broadly to include material and immaterial resources, for example, labour, money, time, moral and emotional investment. Thinking in terms of resources makes us enquire about such matters as whether care is paid or not, the services and other forms of organization that exist but also the emotional roots. The third vector – ‘ideas and values’ – plumbs the ideational and moral framing of care and directs enquiry to such factors as prevailing philosophies and ideal(s) of care and perceptions of the valuing of ‘claims’ around care.
Of course, there is also a wider context that needs to be taken account of especially in terms of outcomes. Even a cursory review of the literature makes it obvious that there is great diversity in the settings within which care need is situated and that the context or setting is therefore transversal to all of the component elements.
Each of these dimensions has an inherent disposition towards the study of inequality and it is possible, either by looking at them individually or all together, to identify care as situated in relations of relative power and inequality. The framework allows a set of critical questions to be posed in relation to COVID-19.
Research going forward
Facing forward at this juncture, it is hard to see a future without transformation wrought by COVID-19. Care is at the pandemic’s epicentre – the global virus involves, if nothing else, an avalanche of care need. This is true in a health sense given associated mortality, illness and compromised physical and mental wellbeing. But it is also the case that the pandemic has transformed the need for the kind of care thinking and enquiry that is the focus of this article. In short, the pandemic has greatly increased the call on unpaid care, the demands on existing arrangements and the need to connect care to wider processes. I want to take the remaining space to indicate some of the insights from considering COVID-19 through the framework developed above. These insights, I suggest, are double-sided, in that care helps us better to understand the pandemic but, equally, COVID-19 both changes the environment and sharpens and refocuses the study of care in key ways. Of course, how we conceptualize the pandemic is crucial. In what follows I think of it not as a short-term shock that will soon pass but as a more long-term phenomenon that challenges the ways in which we live and the demands on social policy and public health and other areas of regulation.
One of the first lines of investigation might focus on the interpretation of need, questioning what is recognized as a valid care need, what is prioritized and what justification is offered. It is too early to draw definitive conclusions, but it does seem universally clear that COVID-19 – understood as both the virus and the response to it – has been interpreted primarily in health terms. A three-fold funnelling of resources has followed: on people who have the virus or are vulnerable to it; on hospitals as settings of care; and on resourcing medical personnel and research. This has been to the relative detriment of non-healthcare needs, locations of care apart from hospitals, and those non-medical personnel for whom the term ‘carers’ was coined. The high infection and mortality rates in nursing and care homes across quite different care regime countries (for example, Belgium, Canada, Italy, Spain and the UK) make clear that there has been a relative downgrading of needs that are typically located within the care system. Children very quickly came to be defined by medical science as non-vulnerable with the result that an entire age group had little visibility or currency during the first 3 months of the pandemic which saw widespread shut-down of childcare and education services. Moreover, if children were seen to have need this was interpreted in educational terms, namely, the channelling of teaching and education resources to families to the almost complete neglect of care resources. In a swift reversal of the public/private care dynamic under social investment perspectives, children’s care was effectively reprivatized to the family. We can see similar processes at work for other populations: service withdrawal and social distancing may well further informalize provision for adults needing care at home. As we move out of the crisis phases and start to live with COVID-19 as an everyday phenomenon, it will be important to observe how the interpretative map changes and what happens when need recognition is more contested. This will be especially important as attempts to control and limit the resources going to care intensify.
In terms of the relational and agentic components of care, my framework would suggest critically reviewing how COVID-19 measures have affected care provision in nursing homes, crèches and domestic settings especially in terms of whether the nature and relations of care receipt and provision have changed, including the working conditions of staff and informal carers and the nature of the relations between the carer and the care recipient. With much care shifted to the domestic sphere, the boundary lines between paid and unpaid care on the one hand and different locations of care on the other hand may well have been changed. The interpersonal and social contract around care may be different also – for example, we should enquire if the pandemic has led to a rise of mutual support and how care was/is situated in a context of where we are exhorted to increase the amount and significance of non-monetary, community-based interactions and exchanges. There is considerable evidence that the old gender division of care labour manifested quite early in lockdown with women far more likely than men to undertake caring activities, especially those occasioned by the closure or cutback of services (UN Women, 2020). Judging on what has transpired, the typecasting of care as women’s work seems to be a fundamental societal underpinning, the equilibrium point; we will have to wait longer to see if this remains the case and whether the ‘care settlement’ struck in the last decades between women, families and the state (and the related ‘bargains’ within couples and between families and migrant workers) has been undone. Other critical questions relevant to the relational and agentic components of care include: To what extent were the voices of those with care need heard during the pandemic? Have the policies instituted to manage the pandemic heightened relations of dependence or independence? In pandemic conditions and beyond, to what extent are paid care workers expected to show loyalty or even ‘love’ to those to whom they provide care?
Turning to resources, core questions enquire about what resources are called forth and/or cut back in the response to COVID-19 and how the division of resources between public and private support systems is reworked. We know that responding to illness and controlling the spread of the virus has been prioritized and that the broader welfare state support architecture put in place for COVID-19 has prioritized income support and generally downgraded social services (Eurofound, 2020). The implications of this for the resourcing of care must be examined in close detail, especially for whether it worsens gender, class and ethnic background inequalities. The period prior to COVID-19, which was one of significant austerity in Europe and elsewhere, saw a number of contradictory trends in long-term care especially, including: greater marketization and use of migrant workers while shifting some care back to the domestic setting; increased care-related rights in some welfare states but selectively so; greater instability in funding local and national provision (Ranci and Pavolini, 2015; Spasova et al., 2018). So how will the pandemic affect these and other trends and tensions? It seems thus far that families have absorbed the costs of the adjustment and the home is reaffirmed as the premier site of caring. In this regard, the concept of ‘depletion’ could be useful, developed by Rai et al. (2014) to articulate and draw out the costs of non-recognition and lack of support for social reproduction. Depletion is for these authors a tipping point when resource outflows exceed resource inflows over a threshold of sustainability, making for a harmful situation for those engaged in this work (whether individuals, households or communities). This concept could spearhead very interesting and multi-level analyses of the resource conditions under which care (provision and need) is rendered sustainable or unsustainable in COVID-19 times.
Turning to the fourth dimension, we can enquire about the care-related values and valuations that are being revealed by the pandemic. We know from existing scholarship that prevailing philosophies of both state and society play a very significant role in influencing how policy deals with care (Kremer, 2007; Saraceno and Keck, 2010). Known variations in this regard sensitize us to the necessity for comparative analyses. A core matter is the ethical and cultural resonance of the policy response to the pandemic. In some countries the needs of those in nursing and care homes have been reinterpreted to refer only to basic services (for example, in the UK COVID-19 emergency legislation was used to significantly ease the obligations of English local authorities to meet need for care in their communities (Daly, 2020)). There is little sense, as of yet, that the pandemic elevated the valuation of the type of care that this article is talking about, although we need to keep posing this question as policy develops. When we have better access to research sites, we might enquire about how different restrictions have balanced rights, entitlements and norms in a way that is ethically proportional.
The concept of care also prompts a broader set of questions. COVID-19 is an opportunity for us to review the meaning of human wellbeing and pose questions as to whether the virus is caused by a lack of attention to care as a valued engagement with our world (in the understanding developed by care ethicists). This kind of thinking touches upon fundamental debates around wellbeing, social inequality and economic growth; climate change; the future of work and the interconnections between production and social reproduction.
Footnotes
Acknowledgements
I would like to acknowledge the helpful comments of Rossella Ciccia and Ertugrul Polat on earlier versions of this article. The feedback of the journal’s reviewers is also gratefully acknowledged.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.