
Abstract
This article investigates the representation and inclusion of marginalized groups in authorities’ crisis communication during the COVID-19 pandemic. Taking a Critical Discourse Analysis (CDA) approach, the study focuses on press releases and guidance documents published on official government websites in the United Kingdom and the United States in 2020–2023. In the analysis, I explore how specific groups of people are referenced by the authorities, and then zoom in on how marginalized groups in particular are discussed. The findings illustrate that the crisis communication in both countries acknowledges the disproportionate effects of the pandemic on marginalized people. However, the ways these effects are discussed may also contribute to discourses that harm marginalized communities by, for example, maintaining negative stereotypes. Overall, the authorities focus on the medical and economic impacts of the crisis on marginalized groups, with less emphasis on social phenomena, such as racism and discrimination.
Keywords
Introduction
In a world characterized by the simultaneous presence of multiple crises, ranging from the global climate crisis to more localized conflicts, crisis communication has an increasingly important role. The COVID-19 pandemic and its complex economic, political and social effects highlighted the need for effective crisis communication that is inclusive and considers different segments of the public (Walter and Glas, 2024: 230). Future crisis communication practices will be informed by lessons learned from COVID-19, which is why it is critical for academic research to zoom in on the language used by the different crisis communicators who contributed to shaping public discussions on the pandemic (e.g., Falco, 2022; Love et al., 2023). In this study, my aim is to contribute to this line of research by investigating the COVID-19 communication of authorities in the United Kingdom and the United States. More specifically, I focus on how this kind of public communication takes into consideration societal diversity and the disproportionate impacts of the crisis on marginalized people. To this end, I address the following research questions:
(1) How are marginalized groups represented in authorities’ COVID-19 communication in the UK and the U.S.?
(2) How successfully do the authorities promote the inclusion of marginalized groups through their language use?
As Wodak (2015: 368) has pointed out, it is pertinent to study how discriminatory and exclusionary discourses continue and change during societal crises. For this reason, the study takes a critical discourse analysis (CDA) approach (e.g., Fairclough et al., 2011; Van Dijk, 1993; Wodak, 2008; 2015), focusing on the representation of marginalized groups as social actors, and the kinds of actions and arguments that are connected to these actors (KhosraviNik, 2010). The data consist of public press releases and guidance documents published by government institutions in both countries on their official websites between January 2020 and May 2023.
Previous research has identified issues related to the treatment of marginalized groups during the pandemic in both the UK and the U.S. In the UK, migrant populations and refugees have been reported to have experienced inequalities in healthcare access, fear of surveillance, and mistrust in the authorities (Van Hout et al., 2024: 23–25). In the U.S. context, previous studies have highlighted President Donald Trump’s racist and stigmatizing rhetoric during the pandemic (e.g., Falco, 2022; Gollust et al., 2020), as well as the impacts of historical and structural inequalities (Gibson, 2024). The findings of the present study illustrate that while both governments report on the disproportionate effects of the pandemic, the ways in which these disparities are discussed may enforce harmful stereotypes and negative associations on marginalized communities. Moreover, the crisis communication of both countries focuses mainly on positive self-representations of the government, with less emphasis on including marginalized groups in decision-making or ascribing agency to their members.
Crisis communication and marginalized groups
During large-scale societal crises like pandemics, politicians and public health professionals must communicate effectively and engage the public (Hodson et al., 2022: 157). Since public health communication addresses highly diverse populations, gaining different audiences’ engagement becomes an important communicative goal (Love et al., 2023: 3). As such, taking societal diversity and the perspectives of different social groups into account is a crucial part of crisis communication. Previous research has showed that treating the public as a homogenous entity is unlikely to be a successful strategy (Coleman et al., 2020: 42), whereas tailored crisis communication directed at specific social sectors and groups promotes an inclusive communication environment, as well as addressing societal vulnerabilities that may result in particular groups being disproportionally affected (Tagliacozzo et al., 2021: 935). Importantly, according to principles of effective crisis communication (e.g. Wooten and James, 2008: 368) and public health leadership (e.g. Jong, 2020: 965–966), authorities also need to be empathetic in their communication and consider citizens’ emotional needs. A public health crisis is likely to cause fear and anxiety in the population, and authorities need to find ways to address the worries of specific communities while maintaining trust in their crisis management abilities.
The COVID-19 pandemic had disproportionate impacts on several minoritized and marginalized groups, including women, racial and ethnic minorities, and those with lower socio-economic status (Beazer et al., 2023: 2; Walter and Glas, 2024: 229). Previous research on crisis and public health communication has highlighted some central issues in the representation of such social groups (e.g., Gibson, 2024; Kreuter and McClure, 2004; Palu et al., 2024). In the context of COVID-19 specifically, the representation of different segments of the public in news reporting has been a prominent research interest (e.g., Beazer et al., 2023; Course et al., 2024; de Carvalho et al., 2024; Lazar et al., 2025). However, less attention has been paid to group representation on institutional communication channels, such as government websites. There are some previous studies that have looked at discourse about vulnerable or stigmatized populations as one aspect of politicians’ public health leadership during COVID-19 (e.g., Dada et al., 2021; Falco, 2022; Liu and Wan, 2024). The present study adds to this literature by critically examining how marginalized groups are represented and included through the language used by institutional crisis communicators.
Various factors related to socio-economic status, cultural and political background, and the ability to absorb crisis messaging all have their effect on individuals’ trust in authorities and their willingness to comply with rules and restrictions during a public health crisis (Love et al., 2023: 3; Coleman et al., 2020). The communicative and linguistic choices made by institutional crisis communicators may also, unintentionally or intentionally, contribute to discriminatory discourse (Falco, 2022: 155). For example, in Falco’s (2022: 155) study on the communicative strategies of the WHO, Donald Trump, and Boris Johnson during COVID-19, an important finding was that authorities “tend to exacerbate [. . .] forms of social and cultural stigma, hate and discrimination”. When authorities communicate in a way that either ignores the systemic discrimination and stigma faced by specific groups, or directly contributes to maintaining discriminatory practices, trust in authorities’ crisis management abilities suffers, particularly within demographics affected by such discrimination.
According to Love et al. (2023: 3), there is a need for research that investigates public health communication by drawing upon “systematic and rigorous analysis on individual linguistic patterns”, as such studies can provide concrete applications of language use for crisis communicators. Similarly, I argue that the CDA approach utilized in this article can be valuable in providing public health authorities and crisis communicators insights into addressing societal diversity and the disproportionate impacts of crises.
CDA as an approach to representation and inclusion
CDA is an interdisciplinary research approach that views discourse as a form of social practice; the ways we use language are shaped by existing social structures and institutions of power, but at the same time, our language use also contributes to shaping, maintaining, or disrupting these structures (Fairclough et al., 2011: 357). Importantly, CDA aims to make visible those structures that contribute to oppression in society, positing itself on the side of the oppressed groups and viewing dominant groups critically (Fairclough et al., 2011: 358). In the present study, my approach to CDA investigates discourses on marginalized groups from the “outside” – that is, I focus on how marginalized groups are being talked about in a crisis context by those in power, and the ways in which this language use contributes to positive self-representation of the nation in crisis, politicians, and government authorities, while simultaneously potentially “othering,” erasing or misrepresenting those with marginalized identities (Wodak, 2008: 55). These linguistic constructions of exclusion (or inclusion) can be expressed explicitly or implicitly, and their use can be intentional or unintentional (Falco, 2022), which is why a close, qualitative analysis facilitated by CDA is a suitable approach to studying them.
My analysis of group representation in authorities’ COVID-19 communication is informed by KhosraviNik’s (2010) approach to conducting CDA, which focuses on the analysis of social actors, social actions and argumentation in texts, as well as connecting these intra-textual elements to broader discourse topics and socio-political contexts. The level of social actors focuses on what social actors are referenced in the texts, and how these actors are portrayed through processes of perspectivization. By perspectivization, KhosraviNik (2010: 63) refers to the range of possible linguistic strategies that are available to text producers, and the strategic choices involved in deciding on particular representations. For example, a range of people can be chosen to be represented as a collective entity through aggregation, and pronouns can be strategically used to highlight us/them categorizations (KhosraviNik, 2010: 64). Social actors may also be labelled in various positive or negative ways through the use of predicational strategies that attribute evaluations on the actors (Wodak, 2008: 63).
On the second level of KhosraviNik’s (2010: 64–65) model, the focus of CDA is on social actions. This means that the analyst pays attention to the actions that are attributed to social actors in the texts, and how actions and actors are connected in the broader discursive context. For example, certain actions connected to specific actors can be exaggerated or played down to further the ideological goals of the text producers (KhosraviNik, 2010: 64–65). As Van Dijk (1993: 23) points out, racist discourse typically attributes characteristic actions to people based on their belonging to racial and ethnic minorities, and these actions are viewed as inherent to the racial or ethnic identity of the group that is represented. The role of actions attributed to the social actors is also relevant when considering questions of agency – that is, whether marginalized people are represented as having agency to perform actions and to exercise control over their situation (Irmer et al., 2024: 202).
Finally, KhosraviNik’s (2010: 65–66) third level focuses on argumentation. Argumentation strategies are used to justify or legitimate discourses of inclusion and exclusion (Wodak 2008: 63). On this level, the analysis centers on the kind of arguments made in the texts, and the ways these arguments are strategically constructed (or omitted). For example, arguments can be made overtly or covertly, and they may strategically utilize features such as allusions and metaphors (KhosraviNik, 2010: 65–66), or intensification and mitigation (Wodak, 2008: 63).
Data and method
The data for the study come from a larger corpus (ca. 2.9 million words) that was collected for a project on public communication during historically significant pandemics in the UK and the U.S. The corpus consists of press releases and publicly available guidance documents related to COVID-19, published between January 2020 and May 2023, and collected in 2023. The timeframe for the corpus is based on the World Health Organization’s categorization of COVID-19 as a Public Health Emergency of International Concern (PHEIC). The UK dataset was collected from the Gov.uk-website, and it consists of two sub-corpora: releases from the “News and communication” section under the heading of “Rules and restrictions during COVID-19,” and releases from the “Guidance and regulation” section under the heading of “COVID-19.” The U.S. data come from three different sources: the Department of State (DoS) COVID-19 releases, the Centers for Disease Control and Prevention (CDC) COVID-19 releases, and the White House COVID-19 releases from both the Trump Administration (2020) and the Biden Administration (2021–2023).
Wodak (2015: 369–370) has pointed out that studying discrimination and marginalization necessitates an in-depth, qualitative approach to the analysis. As such, I decided to focus on a sample that would be possible to analyze qualitatively. To this end, 180 texts (30 from each sub-corpus) were extracted. The procedure for data selection was randomized; I did not limit the selection to certain types of releases, or releases that referenced specific groups. This approach was chosen as I did not want to limit the analysis to any pre-determined group categorizations that could have caused me to miss other types of representations. It should also be noted that the sub-corpora are not balanced nor directly comparable, as some of them contain more data from specific years than others – for instance, the DoS sub-corpus features very few releases from 2020, whereas the UK News and Communication sub-corpus contains more releases from the early stages of the pandemic. Overall, the amount of data available tapers off towards 2023, as communicating about COVID-19 becomes a less urgent matter. Because of the imbalances between sub-corpora, my goal is not to provide diachronic comparisons – rather, I focus on a close, critical investigation of the discourses constructed around marginalized groups that arise in different contexts across the sub-corpora. The distribution of texts investigated from each sub-corpus per year is presented in Figure 1 below.
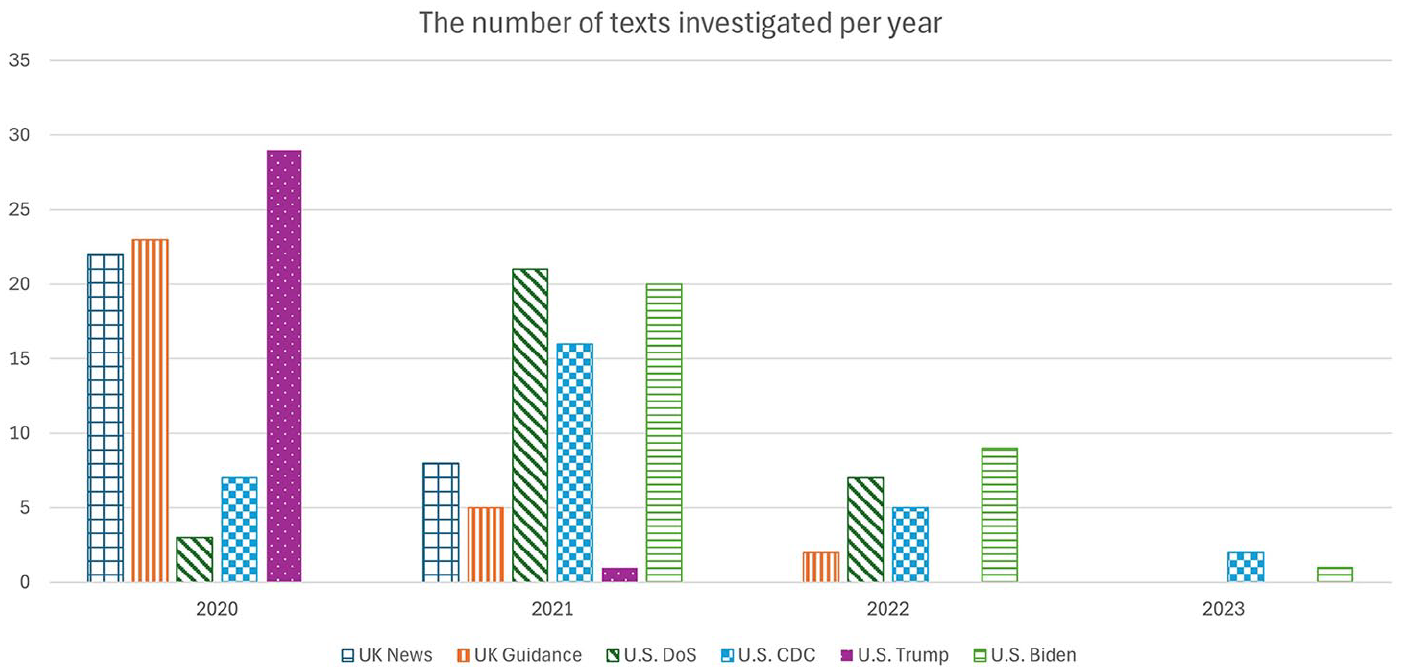
The number of texts investigated from each sub-corpus per year.
The analysis proceeded as follows. I first examined all 180 texts to identify terms used to describe different groups and segments of the population. In the context of KhosraviNik’s (2010: 65) framework, this stage establishes which social actors are present in the texts. Next, I grouped the terms into thematic categories and compiled them into country-specific lists to identify potential differences between the UK and the U.S. 1 Finally, I looked more closely at the discursive and linguistic context in which different terms occurred to map the broader discourses relating to marginalized groups. In other words, I focused on how the social actors were referenced in the texts, as well as investigating what kind of actions and arguments were associated with these actors (KhosraviNik, 2010: 65–66). The qualitative data analysis software Atlas.ti was used for coding the data.
Results
In this chapter, I present the results of the analysis, first providing an exploratory insight into some of the terms used when referring to different (marginalized) groups and segments of the public in the sub-corpora (section “References to groups”), and then moving on to the discursive representation of these groups (section “Discursive representation and inclusion”).
References to groups
My first analytical step was exploring what kind of terms were used when referring to groups of people in the authorities’ texts. This gave me a better idea of who exactly were included and represented in the crisis communication. The list in Appendix 1 illustrates the range of terms from the UK-based sub-corpora, whereas Appendix 2 illustrates the terms from the U.S.-based sub-corpora. 2
Both sets of corpora feature terms that can be classified into ten categories: (1) Age, (2) Crime and victims of crimes, (3) Disabilities, medical conditions and the need for care/support, (4) Ethnic and racial groups, (5) Family and relationships, (6) Gender and sexuality, (7) Nationality and localized identities, (8) Religion, (9) Socio-economic status, and (10) Vulnerability to COVID-19. Additionally, both the UK and the U.S. data feature some terms that do not fit any of these broader categories, such as references to specific roles and occupations (“students” [UK], “humanitarian aid workers” [U.S.]), representatives of political parties (“Democrats” [U.S], “Republicans”[U.S.]), and people with different language abilities (“non-English speakers” [UK]), as well as references to vaguely defined groups (“folks” [U.S.], “people with specific characteristics” [UK]) or very broad descriptions of groups (“all marginalized and underrepresented populations” [U.S.], “the public” [U.S.]). These terms were grouped into their own category: 11) Other.
Unsurprisingly, the categories of Age, Disabilities, medical conditions and the need for care/support, and Vulnerability to COVID-19, are among the most prominent ones in both countries. In the UK data, these categories also feature some of the most frequently referenced terms, such as “older adults”, which was the most commonly occurring expression referring to a group of people in the UK sub-corpora with 218 occurrences. The abundance of medicalized terminology is explained by the nature of the data – since one of the central communicative goals of the government releases is informing citizens about COVID-19, its spread, symptoms and potential risk factors, it makes sense for them to highlight medical vulnerabilities and categorize citizens based on such factors. Similarly, specific age groups can be instructed to act in different ways; as the virus is more likely to cause a severe illness in older demographics, these groups were prioritized when vaccines first became available. Because of this reason, both datasets contain both very specific (“males aged 65 to 74 and females aged 65 to 84” [UK]) as well as more general (“the elderly” [U.S.]) references to people belonging to certain age groups.
References to groups affected by disabilities and medical conditions tend to emphasize person-first language (“people with intellectual and developmental disabilities” [U.S], “those with long-term conditions like diabetes” [UK]) in both countries. However, the data also contain other types of formations (“the disabled” [U.S.], “autistic people” [UK]). Person-first language is typically favored in health communication, because it is seen to emphasize the individual instead of focusing on their disabilities or medical conditions (Best et al., 2022). Despite its prevalence in health communication, the use of person-first language is a somewhat contested practice; those with lived experience may prefer identity-first language, as they may feel that person-first language presents disability as a negative trait (Best et al., 2022). Such contrasting perspectives may present one explanation for the range of different descriptors appearing in the corpora.
Even though the terms that are present in the two sets of corpora can be classified under the same ten main categories, there are also some differences in the range of terms included under each category. These differences start to emerge when looking more closely at the categories of Age and Vulnerability to COVID-19. In the U.S. data, there are several terms in these categories that feature the first-person plural pronoun “our” as a pre-modifier (“our most vulnerable citizens” [U.S.], “our youngest kids” [U.S.]). While a similar construction also appears in the UK data (“the most vulnerable in our families and communities”, [UK]), modifying a group with “our” appears a more consistent practice in the U.S. sub-corpora, where it features also in the categories of Ethnic and racial groups (“our African American and Hispanic communities” [U.S.], Family and relationships (“our families”, [U.S.]), and Nationality and localized identities (“our fellow Americans” [U.S.]).
Similarly, the word “American” appears in multiple categories as well (“American men and women”, “American people who are out of work”, “Americans who suffer long-term side effects from COVID” [U.S.]). Overall, the U.S. data features a broader range of terms related to nationality, which may function as both in-group (“our own people” [U.S.]) and out-group (“noncitizens” [U.S.]) identity markers. In fact, “Americans” are the most frequently referenced group in the U.S. data with 227 occurrences. Based on the prevalence of such terminology in group description, it appears that the U.S. data relies more heavily on a discourse of a shared, national identity (Bucholtz and Hall, 2005: 604). By addressing citizens as members of a nation, the authorities can evoke ideas of shared responsibility in complying with the rules and restrictions in place during the crisis. 3
Distinctive qualities of the UK data include a broader range of terms in the Crime and victims of crime category, as well as the presence of the UK-specific umbrella term for non-white individuals, “BAME” (Black, Asian and Minority Ethnic) in the Ethnic and racial groups category. The terms included in the Crime and victims of crime category illustrate the UK authorities’ concern about the increase in particular criminal activities, especially domestic violence, during the “lockdown” periods. The acronym “BAME” was previously used in government communication in the UK to refer to non-white ethnicities; however, as of 2021, its use is no longer recommended, as it can be viewed to present the experiences of diverse groups as similar, thus erasing some of the more specific forms of discrimination and oppression faced by different groups (Gov.uk, 2024). As the analysis in the following section demonstrates, the discursive practice of grouping different marginalized groups together was common in the data, also in contexts where the term “BAME” did not occur. Finally, some terms present in the UK data reflect the genres of texts included in the Guidance and Regulation corpus. This corpus features reports on scientific research, and guidance documents directed at specific groups (e.g., healthcare professionals or carers), in addition to more general information distributed to the public. As a result, more formal and academic registers are present (e.g., “women of childbearing potential” [UK], “adults with multimorbidity” [UK]).
Discursive representation and inclusion
In this section, I discuss the findings on the representation and inclusion of marginalized groups in authorities’ communication. The findings are presented according to four broader themes that emerged in the analysis: (1) Marginalized people as included and protected by the government, (2) Marginalized people as targets for actions and restrictions, (3) Marginalized people as grouped together, and (4) Marginalized people as “others.”
Marginalized people as included and protected by the government
Much of the communication by authorities in both the UK and the U.S. represented marginalized groups as particularly vulnerable to the effects of COVID-19 and highlighted the importance of protecting these groups through the efforts of the government and other citizens. In these contexts, marginalized groups were typically given little agency as social actors, and the focus was instead on the actions attributed to the authorities themselves: Example 1: The Government is committed to addressing the longer-term implications of COVID-19 for communities that have been disproportionately impacted, some of which were already disadvantaged before the pandemic. The Government is drawing on the knowledge and expertise of medical professionals and the best available evidence to develop and test new approaches to control the spread of the virus in order to protect affected individuals, communities and the NHS. (UK/Guidance and regulation during COVID-19, February 2021)
In Example 1, which comes from a document titled “Spring 2021 COVID response,” the UK authorities acknowledge that the pandemic has affected certain minorities disproportionately. The active party here is the government – they are engaging in actions like committing, protecting, controlling and developing. The positive self-representation of the authorities is further legitimated with science-based arguments (“knowledge and expertise of medical professionals,” “best available evidence”). Here, marginalized communities are mainly depicted as passive recipients of government actions (Course et al., 2024: 8). However, there were also examples in the data where more agency was attributed to the marginalized groups: Example 2: The issue of ensuring that women play a role not only, as you rightly say, in the decision-making, but that we are also keeping a clear and focused eye on the acute impact of the pandemic and all of the shadow pandemics – economic, health, education and otherwise – have on them. I would never say that we’re all the way there, Pearl. You’ve known me long enough to know that we’ve always got a lot of work to do. But I think we saw great evidence today of the power of leadership by women. (U.S./Department of State, November 2021)
The excerpt in Example 2 comes from the U.S. data. It is a reply by Gayle Smith, Coordinator for Global COVID-19 Response and Health Security, to a question posed by a journalist about women’s role in global health leadership during a press briefing. Despite not being a minority in terms of population numbers, Beazer et al. (2023) argue that women can be considered a minoritized group “due to their lack of power, access to power, and public prominence.” In the response in Example 2, Smith affirms the journalist’s stance on the importance of diversity in the global COVID-19 response (“as you rightly say”) and acknowledges that this is an area for improvement on the stage of international politics (“we’ve always got a lot of work to do”). However, the focus remains on the role of the government and their actions – they are “keeping a clear and focused eye” on how the pandemic affects women. Interestingly, even though she refers to the government as a collective “we,” Smith also takes a personal approach to her response by addressing the journalist by her first name and referring to their interpersonal relationship (“you’ve known me long enough”), which contribute to a trustworthy impression of herself as an authority. Overall, Smith’s response does ascribe agency to the marginalized group discussed – although it is worth noting that concrete details on the kind of “work” the U.S. government is doing to empower women are not provided. More prominently, however, the response contributes to a positive self-representation of the authorities.
Inclusion and equality in times of crises were thus used as political tools by the authorities – and successes in these areas were posited as evidence of good crisis management skills, as in the following example from U.S. President Joe Biden’s speech: Example 3: And the U.S. government has successfully put equity at the heart of a nationwide public health response. Hispanic, Black, and Asian adults are now vaccinated at the same rates as White adults. This is the result of an all-of-society effort that got America to where it is today: employers who offered paid time off for their employees; child care providers who offered drop-in services for caregivers to get vaccinated; public transit authorities and ride-sharing companies that provided free rides to vaccination sites; churches, civic organizations, barbershops, and beauty salons, who opened their doors to be trusted spaces for vaccinations; and the families who made vaccination a family affair. (U.S./ Biden Administration, March 2022)
Example 3 references the issue of vaccine hesitancy amongst racial and ethnic minorities. Although the wariness that members of marginalized groups experienced towards the rapidly developed vaccines stems from a long, complex history of medical inequality and mistreatment (Gibson, 2024: 263), the excerpt from Biden’s speech constructs it as a temporary obstacle that his administration has been able to solve. Biden frames lower vaccination rates among minorities as an issue of access and lists a range of actors from different levels of society who have engaged in mitigating actions – a strategy of bringing people together and creating social cohesion (Walter and Glas, 2024: 232). Notably, people belonging to racial and ethnic minorities are contrasted with white people, who are implied to have behaved in a desirable way (by getting vaccinated) from the start. Minority communities, again, are portrayed here as having less agency – for them to be able to act in a way the government expects, protective actions provided by an “all-of-society effort” have been necessary.
Marginalized people as targets for actions and restrictions
Even though marginalized groups were, for the most part, portrayed as passive recipients of others’ protection, there were also examples that focused on marginalized or vulnerable individuals’ own responsibility in complying with rules and recommendations. Sometimes marginalized groups were even directly addressed with particular messaging. For example, releases from both countries referenced the lower vaccination rates amongst certain ethnic minority groups. As we saw in Example 3, this was constructed as an important issue that the authorities – or “we” – needed to address. In Example 4, from the UK, unvaccinated minority groups are directly addressed by the Home Secretary, Priti Patel, in a transcript of a speech: Example 4: And I want to take this moment and opportunity to counter some of the disinformation about the vaccine – especially any messages targeted towards those from an ethnic minority background. This vaccine is safe for us all. It will protect you and your family. It is our best chance of beating this virus. So I urge everyone across our wonderfully diverse country to get the vaccine when their turn comes to keep us all safe. (UK/News and communication on COVID-19, January 2021)
The excerpt in Example 4 presents the argument that ethnic minority groups are more likely to be exposed to vaccine disinformation but fails to acknowledge the complex, socio-historical factors that may have led to such minorities being less trusting of authorities as a source of information (Beazer et al., 2023). In terms of language use, the speaker’s relationship to the group addressed switches between out-group and in-group representations. Ethnic minority groups are, on the one hand, constructed as an out-group who need specific instruction – “those from an ethnic minority background” are urged to “get the vaccine when their turn comes” – but, on the other hand, they are also included in the more broadly defined “we” through statements that highlight the safety of the vaccines “for us all” and name getting vaccinated as “our best chance of beating the virus”. In this way, Patel simultaneously targets the message to specific groups and invokes citizens’ collective responsibility to “keep us all safe”. She also mitigates her potentially face-threatening action of “urging” ethnic minority groups to comply with government guidance by attributing positive features to the groups by referencing “our wonderfully diverse country”.
The U.S. data also featured several releases that addressed the specific effects the crisis had for racial and ethnic minorities. Although some of these releases acknowledged the socio-historical context of such groups being disproportionally affected, there were also discursive choices in the crisis communication that could lead to “othering” of ethnic minorities (Van Dijk 1993: 23; Wodak, 2008: 56). Example 5 comes from a press briefing between Vice President Mike Pence and the governor of Arizona, Doug Ducey, regarding the COVID-19 situation in Arizona. In the excerpt, one of participants of the briefing, White House Coronavirus Response Coordinator, Dr Deborah Birx, discusses meeting with local community members and healthcare leaders in Arizona: Example 5: So in that meeting for community members from the Hispanic community, from the African American community, and today I got to meet with the tribal nation leaders – understanding that messages are not a standalone; that they have to translate into the very fabric of our communities so that people understand what their risks are, so that people can get tested, and so that people understand the importance of wearing a mask. [. . .] I want to thank the African American leader I met yesterday from the community who set up an African American task force to really make sure that messages from the Governor and the health team were being translated at the level of the people who needed to hear it. (U.S./Trump Administration, July 2020)
Even though Birx emphasizes the importance of targeting tailored messaging to certain ethnic minority groups, the arguments she makes also have more covert, problematic messaging. As Birx represents the U.S. government, she likely wishes to avoid acknowledging the lack of trust in authorities among ethnic minorities. Similar to Biden focusing on access in Example 3, Birx presents health inequality as caused by a lack of understanding – the authorities need to collaborate with community insiders in order to “translate” their messaging so that it is understood “at the level of the people”. Whether it is intentional or not, Birx’s speech portrays minorities negatively as “people who do not understand” the authorities’ crisis communication. Thus, a message meant to highlight the actions of the government positively – they are including and engaging minority communities – ends up potentially contributing to harmful stereotypes and stigma.
Marginalized people as grouped together
Particularly in the UK data, aggregation (KhosraviNik 2010: 64) was used often when referring to marginalized groups, meaning that a variety of different groups of people were “lumped together” in the texts. This kind of discursive choice carries the assumption that the experiences of the groups’ members are comparable; as Wodak (2008: 70–71) points out, mentioning specific social actors together “in the same breath” discursively constructs them as belonging together or as “the same”. Example 6 comes from the UK government’s release concerning the country’s COVID-19 recovery strategy, where several groups viewed as disproportionally affected by the crisis are mentioned: Example 6: Evidence shows the varying impacts on different groups or people with specific characteristics, including, but not limited, to BAME individuals, single parents, disabled individuals, victims of domestic abuse and low income groups, many of whom have been disproportionately affected. We have taken action to mitigate the impact on these groups, for example, tailoring communications to different groups, facilitating testing for high contact professions, enabling single adult households to form support bubbles, providing funding for charities working with vulnerable people, such as the victims of domestic abuse, and assisting disabled people to access employment opportunities via the Access to Work scheme.” (UK/Guidance and regulation during COVID-19, July 2020)
In Example 6, the UK authorities list a broad range of marginalized groups facing “varying impacts” of the pandemic, followed by the different actions they have taken to mitigate these impacts. Grouping various types of differently impacted people together in this way allows the authorities to also present their mitigating actions in the form of a list, which rhetorically highlights the broad variety of steps that have been taken, making them appear comprehensive. Presenting evidence of awareness and inclusion in this manner is efficient and impactful from the authorities’ perspective – however, grouping the actions together can also make it unclear how exactly specific groups are being helped (i.e., which actions benefit which groups). Some of the actions listed are also less concrete than others; for individuals struggling due to increased racism or structural oppression during the pandemic, the benefits of charity work and targeted crisis communication may not feel immediate enough. Again, the communication appears to function more as impression management for the authorities (Goffman, 1959) – evidence of what they are “doing right” – rather than providing helpful information for citizens.
Example 7 is another instance of grouping several, differently and intersectionally impacted groups together in the UK data, and it comes from a government release concerning changes to the two-meter social distancing guidance: Example 7: The social, economic, and health impacts of changing the 2m guidance are not evenly distributed. People employed in closed sectors are more likely to be young, not have a degree, and to work in low-skilled occupations. COVID-19 death rates are higher among older people, people in Black and Asian ethnic groups, and for men. It will continue to be important to advise medically vulnerable people to avoid closed spaces, crowded places and close-contact settings. (UK/Guidance and regulation during COVID-19, June 2020)
In this release, the government is reporting on new guidelines for social distancing, which allow for people to only keep a one-meter distance from each other under certain conditions. Throughout the release, scientific research on social distancing is referenced and used as a justification for revising the guidelines. However, in the excerpt in Example 7, an acknowledgement is made that the new guidance may not be applicable to certain vulnerable groups. Again, the release lists multiple groups that have different and intersecting risks: people of lower socio-economic status (described here with negative connotations, as working in “low-skilled occupations”), people belonging to certain demographics in terms of age, ethnicity and gender, and people considered “medically vulnerable.” The release does not provide any concrete details on how people belonging to one or more of these groups are considered in the guidance – instead, it states in general terms that these people should “be advised to avoid” situations where there is a heightened risk for infection. The responsibility of keeping oneself safe then falls to the marginalized individuals, even though it is mentioned in the guidance itself that this may not be possible in industries where workers are more likely to belong to vulnerable minorities. Thus, despite mentioning some marginalized groups as “exempt” from the revised restrictions, the guidance ultimately fails to consider people who occupy the intersections of multiple marginalized positions.
Marginalized people as “others”
While the releases from both countries featured examples of more covert exclusion or “othering” of, for example, racial and ethnic minorities (see section “Marginalized people as targets for actions and restrictions”), explicitly excluding the countries’ own citizens was rare. However, in the U.S. data, there was evidence of the authorities viewing specific non-U.S. groups as “others.” Overall, such discourses were realized through patterns of positive self-representation and negative other-representation (Van Dijk, 1993; Wodak, 2015). For instance, the role of the U.S. in the global fight against the pandemic was represented positively by emphasizing features like humanitarianism (providing vaccines to other countries “no strings attached”) and high morals (descriptions of Americans as “committed,” “generous,” or “united”). The common practice of modifying group descriptors with “our” and “American,” observed in the section “References to groups”, also adds to this positive self-representation of the U.S. as united, and its authorities as inclusive and caring. Foreign governments and citizens of other countries, however, were depicted more negatively by, for example, emphasizing their struggles in managing the crisis. As a part of this “us vs. them” polarization, people from other countries were labelled as a threat to the public health and the security of the nation. For example, in a CDC release about temporary changes to migration policy (U.S./CDC, August 2021), “certain noncitizens” were said to “[create] a serious danger” of spreading COVID-19. This type of discourse is in line with previous research, which has identified a rise in nationalism and anti-migrant attitudes as one of the broader, political consequences of the pandemic on a global scale (Walter and Glas, 2024: 230).
The exclusionary discourse in the U.S. data was most apparent in discussions pertaining to China and Chinese people. The outbreak of COVID-19 in Wuhan increased tensions between the U.S. and China, and lead to a surge in Sinophobia and racism towards Asian ethnicity groups (Kania, 2023; Walter and Glas, 2024: 230). As discussed in earlier studies (e.g., Falco, 2022; Kania, 2023: 335), the U.S. President Donald Trump contributed to these discriminatory discourses by, for example, referring to COVID-19 as the “Chinese virus”. In the present study as well, there are several instances of portraying China (and the Chinese) as an outgroup in the Trump Administration sub-corpus. Example 8 comes from a transcript of a press conference where Trump answers the question “Do you have an expectation of what the death toll is going to look like by the summer”: Example 8: You know what? I don’t want to think about it, even. I know that we’re doing everything we can. We’re doing a good job. We acted very early. We acted extremely early in keeping China out of our country and banning people from China coming in, other than our citizens, which we obviously had to take. And they were quarantined or watched carefully. They were tested. They were watched very carefully. (U.S./Trump Administration, May 2020)
In the excerpt in Example 8, Trump constructs both positive self-representations and negative other-representations. In terms of self-representation, he describes the actions of the U.S. government (“we”) with repeated positive evaluations (“good,” “extremely”), emphasizing that they are not at fault for the death toll. China and “people from China” are positioned as the out-group – the guilty party bringing in the virus despite “our” preventative actions. Interestingly, Trump’s response appears to also position U.S. citizens who were in China at the time of the outbreak in the out-group – as a “they” that “we had to take [in]” and carefully monitor. Thus, there is a negative association with not only China and the Chinese people, but also people with any connection to China.
Discussion and conclusion
While the COVID-19 pandemic is largely considered to be over in 2025, the need for crisis communication that addresses societal diversity and actively promotes equality is particularly apparent now, as societal polarization increases, along with the rise in political conservatism and far-right ideologies in many Western societies (e.g., Bridges et al., 2023). Against this background, critical studies of the language used by authorities during times of crisis are vital. The results of these studies can provide useful insights for authorities and public health professionals.
The findings of the present study illustrate that a broad variety of groups of people are referenced and addressed in the UK and U.S. authorities’ crisis communication, and particular challenges that affected these groups during the crisis are identified. However, potentially harmful representations also emerge. First, authorities’ crisis communication tends to focus on prioritizing the actions of the government, giving little voice, agency or concrete resources to the marginalized groups. While focusing on the role of the government as a “protector” of marginalized groups is not an inherently negative way of representing such groups, systematically assigning a role of passive recipient to marginalized individuals may still contribute to negative stereotypes (Course et al., 2024: 8). Moreover, there is a risk that marginalized groups are discursively reduced to a tool for authorities’ impression management and political campaigning through positive self-representation (Goffman, 1959; Wodak, 2008). This may lead to public health communication that “reports on disparate outcomes without addressing disparate harm in policy discussions” (Gibson, 2024: 257).
Second, while tailoring messages to specific recipients during a crisis may be helpful (Tagliacozzo et al., 2021), the ways authorities address minorities are not necessarily nuanced enough. My analysis illustrates that authorities often fail to consider the complexity of power dynamics between the government and historically marginalized groups. For example, lack of opportunity and education are seen as the primary reasons for marginalized people’s vaccine hesitancy, instead of a lack of trust in the authorities (Gibson, 2024: 261). Crisis communication that ignores the historical and systemic forms of oppression that have led to minorities’ distrust in authorities and medical providers is unlikely to be successful in the long run. Instead, public health communicators may want to focus more of their efforts into building trust.
Third, there is a tendency to discursively group various marginalized groups together, which can be harmful, as the circumstances experienced by these groups are not always similar, and many are intersectionally impacted. Homogenizing differently impacted segments of the public into one, broad group may lead to a “one-size-fits-all” approach that overlooks specific structural barriers that marginalized people face when seeking healthcare and can cause these people to avoid medical care altogether (Van Hout et al., 2024: 25). Finally, although there was little explicit “othering” of marginalized groups in the data, more implicit links were made between, for example, foreigners and immigrants and threats to “our” public health and security. Such exclusionary discourse, whether explicit or implicit, is likely to exacerbate distrust towards the authorities among minority communities. Discursive patterns of exclusion or negative stereotyping in official government communication may also have broader harmful effects on public discourse, as these texts are often used as source material by the media (Dada et al., 2021: 9–10). Notably, while previous studies have broadly acknowledged exclusionary and discriminatory language use in Donald Trump’s communication during COVID-19 (Dada et al. 2021; Falco, 2022; Gollust et al., 2020), the present study found examples of more implicit discursive marginalization across all sub-corpora that were investigated.
Overall, the UK and the U.S. data feature similar discursive patterns when it comes to the representation and inclusion of marginalized groups. The crisis communication in both countries acknowledges the disproportionate effects of the pandemic on marginalized people – however, while such effects are frequently discussed in a medical or economic context, through various representations of “high-riskness”, less attention is paid to social issues like racism or other forms of systemic oppression. For example, the way the pandemic amplified racist attitudes towards East Asian people was not discussed in any of the releases investigated in the present study. In terms of differences between the two countries, the broader range of references to nationality and localized identity groups suggests that national identity has a more central role in group representation in the U.S. However, as the present study had more U.S. based data, this conclusion should be considered tentative. Future studies should expand on the present study by focusing on more quantitative comparisons between authorities in different countries, using larger corpora and integrating data from non-English speaking countries. In addition, to better evaluate the success of authorities’ crisis communication, future studies need to investigate citizens’ reactions to the inclusion and representation of marginalized groups in government communication. To this end, I am currently working with social media data featuring citizens’ responses to authorities’ communication.
Supplemental Material
sj-docx-1-das-10.1177_09579265251353793 – Supplemental material for “The impacts are not evenly distributed”: Representation and inclusion of marginalized groups in authorities’ COVID-19 communication
Supplemental material, sj-docx-1-das-10.1177_09579265251353793 for “The impacts are not evenly distributed”: Representation and inclusion of marginalized groups in authorities’ COVID-19 communication by Hanna Limatius in Discourse & Society
Footnotes
Ethical Considerations
Not applicable, as the data consist of public government websites.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was conducted as part of the project Languaging Crises: Diachronic Perspectives on Public Communication during Three Pandemics (LanCris), funded by the Research Council of Finland (decision number 356219).
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated during and/or analyzed during the current study are not publicly available at present, as the data are related to a research project that is still on-going.
Supplemental material
Supplemental material for this article is available online.
Notes
Author biography
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.