
Abstract
We present a social-historical perspective on the evolution of the voice-hearing phenomenon in Western society. Based upon a systematic search from a selection of nine databases, we trace the way hearing voices has been understood throughout the ages. Originally, hearing voices was considered a gifted talent for accessing the divine, but the progressive influence of monotheistic religion gradually condemned the practice to social marginalization. Later, the medical and psychiatric professions of secular society were instrumental in attaching stigma to both voice hearers and the phenomenon itself, thereby reinforcing social exclusion. More recently, the re-integration of voice hearers into the community by health authorities in various countries appears to have provided a new, socially acceptable setting for the phenomenon.
Keywords
Introduction
Following Franck and Thibaut (2003), we shall be employing the technical term ‘auditory-verbal hallucination’ (AVH) when referring to the perception of voices in the absence of external sensory cues. This phenomenon is also independent of internal volitional cognition or what is traditionally known within psychodynamic psychology as directed thinking. Most people habitually experience AVH while dreaming during sleep; waking forms of auditory hallucination occur relatively less frequently (Larøi et al., 2012). Initially considered mystical and religious, the cultural perception of AVH has evolved throughout history to lead gradually to the present modern view, where clinical and academic research on the phenomenon and the spread of the Hearing Voices Movement (HVM) since 1987 have been indicative of a conceptual change. Since the Movement feels the phrase ‘hearing voices’ is more accurate and user-friendly than AVH, we shall use colloquial terms such as ‘voice hearing’ interchangeably with the more technical one.
The considerable impact of this new line of research on our collective and scientific conceptions of voice hearing came with the publication of a paper by Romme and Escher (1989), which showed that AVHs sometimes result from traumatic life events or accompany specific ailments such as dehydration, hearing disorders and epilepsy (Read et al., 2005; Sommer and Van der Spek, 2016). The progressive influence of these publications has been accompanied by a transformation of the psychiatric nosography that had previously considered hearing voices as an exclusively pathognomonic sign of schizophrenia (Romme and Escher, 1989). This development is highlighted by the epidemiological finding that, while voice hearing is estimated to occur in 7.3% of the general population (Kråkvik et al., 2015), only 0.7–1% of the populace has a diagnosed schizophrenic disorder (INSERM, 2020).
Faced with the discrepancy between traditional psychiatric opinion and that of the HVM, various authors have contributed to a growing body of knowledge about the origin and impact of AVHs, the remedial care offered to those experiencing them, the advantages and disadvantages of the Movement, and the possibility of diagnoses other than schizophrenia (May and Hayes, 2012). However, apart from the works of Leudar and Thomas (2000) and McCarthy-Jones (2012), and a brief review of literature by Evrard and Le Maléfan (2013), no work, at least to our knowledge, has hitherto offered a syncretic vision of the evolution of voice hearing through the ages. Current ideas relating to the phenomenon strongly suggest that we should pause to reflect on the evolution of these developments and the religious, cultural, social, political and scientific factors that have shaped an apparent paradigmatic shift.
Within this context, we systematically trawled English and French sources accessible through nine selected digital databases in an effort to identify and review pertinent scientific publications concerning the historical evolution of the voice-hearing concept. The first objective of this article has been to provide a synoptic view of the phenomenon from the perspective of its development across five broad historical eras, thus allowing the outline of the posited process to emerge; the second objective has been to offer an informed commentary on the various factors thought likely to have influenced this evolution. Combining these two approaches will hopefully allow both professionals and individuals concerned with voice hearing to gain a general and more comprehensive understanding of the phenomenon and an increased awareness of issues that led to its stigmatization.
Methodology
Using the PRISMA checklist (Page et al., 2021), we conducted a systematic search of the literature in English and French (see Figure 1) in the following nine databases: Science Direct, PsycInfo, PsychARTICLES, Cairn, Web of Science, Pubmed, Biomed, Cochrane, Taylor and Francis. Combining two lists of keywords simultaneously avoids obtaining too many non-specific results and refines the algorithm used. The following keywords were used: ‘Entente de voix/voice-hearing’; ‘entendeurs de voix/voice-hearer’; ‘psychose/psychosis’; ‘schizophrénie/schizophrenia’; ‘hallucination auditive verbale (HAV)/auditory verbal hallucination (AVH)’; ‘Réseau d’entendeurs de voix (REV)/hearing voices network (HVM)’; ‘hearing voices approach’. These keywords were combined with: ‘coping’; ‘appraisal’; ‘représentation sociale/social representation’; ‘stigmatisation/stigmatization’; ‘prise en charge/soin/care’; ‘évolution/evolution’; ‘histoire/history’; ‘siècle/century’; ‘religion/religion’; ‘médicalisation/medicalization’; ‘psychiatrie/psychiatry’; ‘moyen-âge/middle-ages’; ‘antiquité/antiquity’; ‘époque moderne/early modern period’; ‘XVIII; XIX; XX; XXI’. This systematic search performed in 2018 and repeated in September 2021 was then combined with a collection of references from the books and reports of grey literature and Google Scholar.
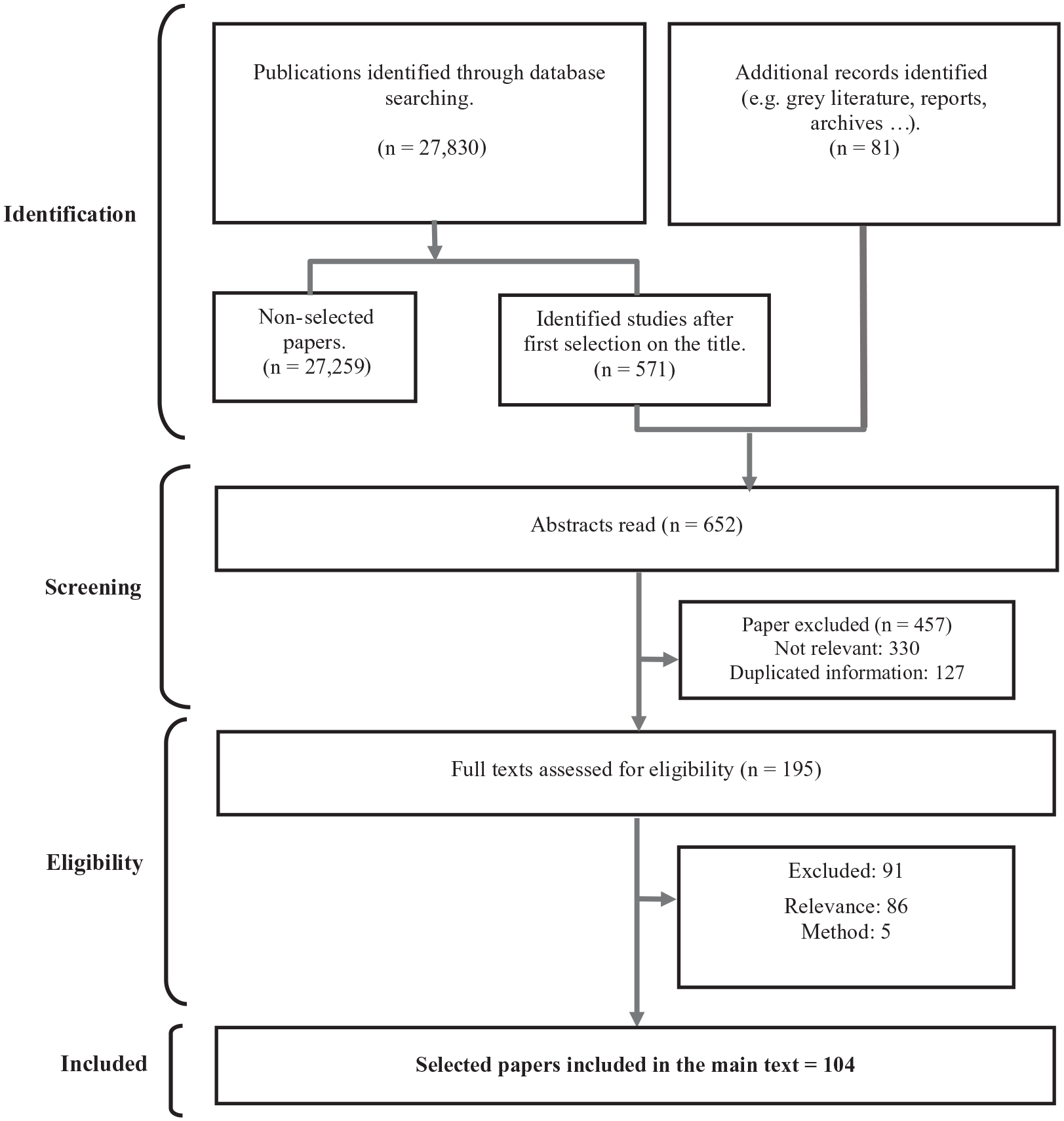
Flow diagram of the selection process on the state of play of the voice-hearing phenomenon.
The criteria for the search were based on the scope of the review and therefore included publications shedding historical light on the phenomena of hearing voices or AVH, i.e. relevant English and French scientific articles, books, book chapters, and reports. The exclusion criteria were editorial commentaries, article commentaries, conference reports and popular articles. From 27,830 database hits, a first selection of 652 writings, including 81 from grey literature, was made based on the titles of the references found. At this stage the exclusion criterion was confined to the theme of the article, which could reasonably be expected to reflect either the location of voice hearing in history or factors influencing historical changes of its conception. However, since the phenomenon in question has only recently been differentiated from the concept of madness, the authors decided to include references addressing more general notions of insanity. After eliminating 127 duplicates, 457 more articles were excluded, based on their abstracts. In total, 195 articles, including those from grey literature, were read in full, of which 91 were rejected, 86 being thematically irrelevant and 5 having methodological flaws. Consequently, 45 scientific articles and 59 from grey literature were included in our systematic narrative review of the literature.
After a thematic content analysis, the writings were placed into five distinct groups tracing evolution in the perception of voice hearing through the ages: (1) From divine inspiration to religious condemnation: the itinerary of voice hearing up to the medieval period; (2) From deviance in the eyes of religious authorities to social marginalization during the Renaissance; (3) From dispensaries to asylums: from the social marginalization of ‘mad’ individuals to the medicalization of madness at the dawn of the contemporary era; (4) Psychiatrization and stigmatization of voice hearing in the twentieth century; (5) The advent of voice hearing as a community phenomenon at the start of the twenty-first century.
The presentation of these five categories includes an account of factors that may conceivably have influenced ideological movements concerning consensual speech and notions of sanity, owing to the historical conflation of AVH and madness.
Results
From divine inspiration to religious condemnation: the itinerary of voice hearing up to the medieval period
The earliest records of the presence of voice-hearing phenomena date from the third millennium BC and, coming from Mesopotamia or ancient Egypt, they are often linked to the Sumerian religion (McCarthy-Jones, 2012: ch. 1). At that time ‘voices’ were generally considered to bear witness to a discourse between human beings and the god Marduk, who was seen as a mediator between mortals and the divine. The intermediary function of voice tuning was characteristic of many religious groups, such as the ‘howling nebiim’ (Causse, 1922), the ‘worshippers of Adonis’ (Will, 1975) and the ‘oracle of the Pythia’ such as the one at Delphi (Ménard, 1863). In this context, AVHs were seen as an ability to communicate with the divine for the purpose of discerning the will of the gods and hence human fate. We note in passing that, while some religious visions are more accurately classified as visual-auditory hallucinations, the AVH component is of particular importance since language may clearly convey instructions and meaning.
Although the monotheistic religions have strenuously endeavoured to exclude many aspects of pagan belief through the artifices of assimilation and condemnation, they have nevertheless all proposed interpretations of AVH phenomena that are similar to those of polytheistic religions (Ménard, 1863). For example, the stories of Jesus, St Paul and Moses common to the Jewish, Christian and Muslim religions all mention a connection with the divine through the hearing of voices (Murray, Cunningham and Price, 2012). The accounts of Abraham’s life, for instance, are peppered with episodes of visual and auditory hallucinations, such as his ordeal and moral dilemma of being commanded by God to sacrifice his beloved son (Genesis 22:1–24).
Throughout antiquity, AVHs were fully integrated into the mystical and religious elaborations of the populace, thereby giving meaning to the phenomena and embedding them within the social fabric. In the West, the position of AVHs remained constant until the Middle Ages, although even in antiquity there had been thinkers who attributed them to a disease of the individual soul and therefore espoused a form of medical interpretation (Quétel, 2012: 21–48).
These early ideas on what today are called AVHs evolved in parallel with theories on the concept of the voice in general, which played a major role in the philosophical and medical reflections of the time. Antiquity was notably the cradle of acoustic and phonetic conceptions of the voice (Bouton-Touboulic, 2021). Epicurus described it as the only sound produced consciously and voluntarily, to which Aristotle added that it was linked to the subject’s psychic reality and its representations. Philosophers of the time also associated the voice with physical phenomena and, in particular, the breath, thereby becoming a real equivalent of thought and life (Maury, 1845). As for auditory hallucinations, they were more generally associated with death in religious narratives, as Maury (1845) reminds us in his evocation of angelic voices accompanying the souls of the righteous as they rise to heaven. In ancient myths, they may even be the actual cause of death, as in numerous examples describing the experiences of sailors in contact with mermaids.
Despite the early philosophical and medical writings of these thinkers, the societies in which they lived failed to retain and transmit these ideas, and so they were rarely mentioned before the Renaissance, owing to the prevalence of religious thought. Today it is difficult to obtain precise information about the general state of knowledge in the medieval period (Laharie, 1993), and so it is hardly surprising that we have few if any references to voice hearing from that time. However, it does seem inherently unlikely that the phenomenon was absent from the mystical, social and medical domains. Fossier (2004) contends that the lack of data is all the more pronounced because madness and voice hearing were considered a private matter at that time and so were not commented on in public. Given the extensive timeline, this view is naturally open to question as it is based on the unwarranted assumption that all published sources of the time have survived until now. It also fails to consider the possibility of unpublished accounts, non-scientific writings, oral histories, and relevant experiences going unrecorded because those who had them did not or could not write.
Despite these shortcomings in the historical record, evidence of a contrary trend can nevertheless be observed in the late Middle Ages, for the period was characterized by an increasing influence of Christian doctrine which produced numerous iconographies and a rich literature on madness (Fritz, 2015). The importance of religious belief led to the protection of various societal elements and, along with them, the phenomenon of AVH. Henceforth recognized as a matter for the religious and pontifical authorities, voice hearers considered as deviant were progressively labelled as heretics and hunted down by the Church as it sought to combat the deviance it had criminalized (Powell and Saunders, 2021: 15–44). Suspects were examined for signs of the Devil (Daneau, 1564) and often sentenced to death or life imprisonment, as was the case with Thomas of Apulia (Ternon, 2016). In happier circumstances, voice hearers could benefit from the pharmacopoeia of the monks which aimed to ‘purify’ those living under the ‘influence of the Devil’ (Coudeyrette, 2019).
In spite of this condemnation and social ostracism by Christianity in the West, certain aspects of AVH were nevertheless glorified and politicized. For example, the 13-year-old Joan of Arc heard the voices of St Michael, St Catherine and St Margaret, who all exerted total control over her as she set herself the goal of ‘driving the English out of France’ in order to enable the coronation of the Dauphin, Charles VII (Brémaud, 2008). After verifying her virginity, which was held to place her beyond reach of the Devil, the Church considered the voices prophetic in nature and used them to raise armies and promote social acceptance of the war and in particular to legitimize the hostilities of 1429–30.
Once considered an individual phenomenon of public utility, AVH gradually became a private matter whose nature was now confused with the intrinsic qualities of the experiencer. This ideological shift can be viewed as contributing to the social marginalization of consensual speech and resulting in the stigmatization and discrimination of voice hearers.
Given these developments, and the scarcity of primary sources, we should naturally be cautious of adopting a Foucauldian-style view in which voice hearers are inevitably perceived in a positive and often religiously significant light by their contemporaries. Rather, we must assume a perennial and polarized conflict between the forms of stigmatization to which voice hearers are prone and their integration into the social order. Both perspectives were already present in antiquity, and changes in the balance of power are clearly visible in later periods.
From deviance in the eyes of religious authorities to social marginalization during the Renaissance
During the Renaissance, society was shaped by profound societal and philosophical changes combined with major scientific discoveries concerning access to, and the dissemination of, information. The position traditionally occupied by religious dogma gradually lost ground to a more modern movement towards the ideology of social action (Gourvil, 2010). Gradually, societal mores achieved what Lebrun (1993: 90) described as a ‘transfer of God’s share to Man’s share’. As knowledge advanced in Western society, certain monarchies, such as the regime of Louis XIV in France, encouraged the emergence of the scientific-like professions of apothecaries, barbers and doctors (Hoffman, 2007). By furthering proto-scientific theories from antiquity, the updated medical knowledge and methods of the Renaissance led to the beginnings of a power struggle between science and religion, culminating in the advent of psychiatry in the eighteenth century.
For De Luca (2008), thinkers of the Renaissance tended to confuse AVH with epileptic and melancholic seizures, while ecclesiastical scholars continued to understand voice hearing as the work of the Devil or of God. The coexistence and confrontation of scientific and religious thought were all the more visible among the philosophers and artists of the Enlightenment. Descartes (1596–1650), for example, formulated and disseminated his ‘cogito ergo sum’ maxim following a series of three dreams which he interpreted as confirming his mission to introduce a new philosophical method to the world. For this philosopher, inspirational dreams were of divine origin, but scientists subsequently working with Descartes’ material variously rationalized them in terms of auditory hallucinations emerging from the unconscious mind, the results of post-traumatic syndrome, tumours of the right ethmoidal sinus, or even ‘exploding head syndrome’ (Otaiku, 2018; Withers, 2008).
For Voltaire (1694–1778), who denied the religious character of auditory hallucinations altogether, miracles like this simply did not exist and such phenomena were partly fabrications of the Church, which he sought to demonstrate through his analysis of Joan of Arc’s trial in Rouen (Voltaire, 1752). Since many religious AVHs possessed a marked musical component (James, 1906: lectures 16–17), enlightenment scholars sought rationalistic explanations for ‘musical hallucinations’, thereby replacing mysticism with scientific theory, as in the example of the posited existence of a musical memory (Roger, 1803: 160–73). Artistic hallucinations present among Enlightenment artists gave rise to reflections on the link between perception, creativity and hallucinatory activity (Ferrières-Perstureau, 2007).
While science-philosophy gradually appropriated the AVH phenomenon, the Renaissance’s mystical interpretations continued to offer a field of expression to those who experienced them (Colleyn, 2013). This ‘intermingling’ of religious and scientific thinking demonstrates how ‘the privileged relationship between illness and the sacred is a consequence of the relationship between illness and society’ (Hoffman, 2007: 75). This engendered the formation of two poles claiming to support the voice hearer: on the one hand religion, facing criticism for its dogmatic attitude, progressively softened its position; on the other hand, the scientific and philosophical speculation associated with the emergence of medical philosophy considered the hearing of voices as a disease of the soul. The Renaissance was therefore the historical period that established the dual appropriation of AVH phenomena by religion and the emerging sphere of philosophy.
In the face of this dual claim, and under the influence of the humanist current known for its social vocation, the task in the seventeenth century was to find a place for those individuals blessed or afflicted with voice hearing. Affirming madness to be a matter for social support rather than demonology, Renaissance physicians and humanist theologians such as John Wier [Johann Weyer] (1515–88) and Juan Luis Vives (1492–1540) contributed to the creation of a current of thought aiming to provide assistance to the insane and therefore, by implication, to voice hearers. Building on earlier writings like the La nef des fous (Brandt, 1494) and Éloge de la folie (Érasme, 1511), which gave people described as sick and deluded the integrity of a personal place within society, the responsibility for supporting voice hearers became organized around a shared monopoly between religion and society.
Considered as social deviants since the Middle Ages and no longer benefiting from their identity as mediums for the divine, many voice hearers were classed with madmen, beggars, debauched women and other stigmatized groups (Quétel, 2012: 49–88). No longer accepted at the heart of their communities, they became victims of social ostracism by being placed in dispensaries. Theories explaining AVH in terms of cerebral dysfunction, which had become established in the West since the Renaissance, were then discarded and would give way to a combination of psychic marginality and moral deviance (Touboul, 2016).
From dispensaries to asylums: from the social marginalization of ‘mad’ individuals to the medicalization of madness at the dawn of the contemporary era
At the start of the modern era, the first institutions dedicated to the confinement of individuals classified as socially deviant grew significantly in number. So those voice hearers who were not protected by their social status or religious power, and despite their peculiarity eliciting no public comment or hindering their social integration, were corralled into dispensaries. Both the real and symbolic exclusion of individuals considered to be marginal was eventually perceived as a form of renunciation of social power in the face of deviance (Foucault, 1961: 56–91; Roscioni, 2011). In this way, the emergence of a form of medicalization of deviant and marginal behaviour was achieved through a transfer of responsibility from the social authorities to the medical domain. Consequently, dispensaries, which had been characterized primarily in social terms, took on features relating to the medicalization of madness and became asylums, echoing the medical conceptions that had been construed by institutional wardens from their contact with the incarcerated.
More precisely, by making it possible to gather a concentration and diversity of mental disorders under one roof, the policies of the time facilitated the emergence of the first ‘psychiatric’ nosographies to be inspired by the classification system of Linnaeus (1707–78) (Grenouilloux, 2010). Classified in this way, the voice-hearing phenomenon was not recognized in its own right because it was considered to be a secondary symptom of madness resulting from an episode of mania, delirium or dementia (Pinel, 1798: 123–8). Subsequently, at the start of the nineteenth century the combination of emerging nosographies of mental illness and regular contact with individuals suffering from AVH led to the first theories on hallucinatory phenomena. As early as 1814, the work of Esquirol (1772–1840) emphasized the psychic origin of delirium by distinguishing between hallucination and illusion (Esquirol, 1814). He subsequently proposed the first medical definition of hallucinatory phenomena (Esquirol, 1838: 80–100) by describing them as ‘the intimate conviction of a sensation actually perceived, while no external object capable of exciting this sensation is within the reach of one’s senses’.
The emergence of new definitions and classifications of madness, combined with the use of moral treatments, facilitated the spread of the medicalization of madness during the nineteenth century. In France, this tug-of-war ended in 1838 with the introduction of a law on the insane (Foucault, 1961: 483–530), which considerably reduced the role of religious authorities in the decision-making and care-giving in regard to madness. This was achieved by granting the medical field decision-making powers and a local presence in the départements or counties, hence establishing the beginnings of a regional organization of psychiatric services (Clesse et al., 2018). Driven by the hygienist movement and the emergence of Public Health (Cavé, 2016: sections 1 and 2), similar legislation spread through the rest of Europe as the nineteenth century drew to a close, thereby socially validating the notion of the medicalization of madness and shifting the conception of AVH towards notions of disease (Foucault, 1961: 316–60).
In the metaphorical and metonymic confusion with notions of madness, voice hearers lost their residual social and religious position attributed to them by the mores of the time. Nevertheless, it was true – depending on the individual, cultural or religious interpretation of the persons in question – that hearing voices could still be perceived as a mystical phenomenon. Henceforth perceived as a public health problem subject to the prophylactic paradigms currently in vogue (Kråkvik et al., 2015), the hearing of voices was considered as an expression of mental illness from the second half of the nineteenth century onwards. In this context, AVH became an object of medical research, the components of which were explored by a group of alienist physicians who are today considered to be the precursors of psychiatry in Europe (Brémaud, 2016).
Initially, one line of research aimed to separate the concept of hallucination from the notion of illusion: Esquirol (1838: 159–201) considered the cerebral and psychical character of AVH to be different from false sensations, sense illusions or erroneous perceptions. This view developed with Moreau (1845:170–345) drawing a distinction between hallucination and reverie, and Baillarger (1846: 369) proposing a model differentiating between ‘complete’ psychosensory hallucinations produced by ‘the double action of the imagination and the sense organs’ and psychical hallucinations resulting from ‘the involuntary exercise of the memory and the imagination’. Falret took up the notion of conviction, which had also been developed by Esquirol, with special emphasis on its role in the hallucinatory process. The perception of AVHs, particularly in the psychiatric field, still depends on the degree of conviction the experiencer adopts towards them.
Conclusions from this work were further enriched by a new field researching the links between thought and language, which considered the way voice hearers talk about their own thoughts and attribute them to ego-dystonic causes (Baillarger, 1846: 369; Moreau, 1845: 346–9). In particular, the work of Séglas (1892) established the beginnings of a nosology of language associated with the phenomenon of AVH, thus influencing the work in the twentieth century that associated psychological pathology and language (Moreau, 1845). A third phase of development by Ball (1880–83: 59–131) established the connection between hallucination and madness by considering the former to be a symptom of the latter, the severity of which was defined in terms of nosography (Brémaud, 2016).
These sensory, intellectual and linguistic strands of research into AVH were three primary lines of development that profoundly influenced the future psychological and psychiatric sciences of the twentieth and twenty-first centuries (Patouillard, 2007). Each of these three lines of research helped, in its own way, to form specific theoretical approaches to twentieth-century psychology and psychiatry: the sensory strand influenced the development of neuropsychology; the intellectual influenced the development of cognitive psychology and psychiatry; and the linguistic provided a knowledge base that facilitated the development of psychoanalysis (Grollier, 2011).
The epistemological difficulties encountered by researchers at that time, especially when defining madness and its parameters, opened up a gap for some scientists to reintroduce a spiritual conception of voice hearing. In particular, hallucinations compatible with reason gave rise to debate because they appeared in healthy subjects and therefore did not correspond to Esquirol’s definition of hallucination. For Brierre de Boismont, explaining intellectual and moral actions in terms of pathology was tantamount to suggesting that the most sublime opinions, particularly religious ones, were advocated by madmen (Maury, 1845). This was untenable for him and for many thinkers of his generation, and his mystical interpretation in the case of Joan of Arc rekindled debates between alienists that were often influenced by their own religious affinities.
During the rise of psychical research at the turn of the twentieth century, AVH progressively became an object of interdisciplinary research at the frontier of science in the form of telepathic and veridical hallucinations, thus allowing a discourse between natural science and social science that led to speculations on the hidden potentialities of the mind (Le Maléfan, 2008a). The emerging Spiritualist movement of the mid-nineteenth century interpreted AVHs in terms of clairaudience and the transmission of messages from ‘the beyond’, thereby restoring their divine function and contributing to further discussion on such matters (Le Maléfan, 2008b).
Psychiatrization and stigmatization of voice hearing in the twentieth century
The twentieth century saw the emergence of various theoretical schools influenced by lines of research developed in the nineteenth. These reinforced the notion that hearing voices was a pathological sign, and proposed therapeutic treatments which aimed at curbing the negative impact of AVH on the adaption of individuals to the reality of their external environments. As early as 1894 the psychoanalytical movement under Freud linked hallucinatory phenomena to psychic conflict and thereby led to the concept of regression and the emergence of a subjective pleasure principle (Freud, 1894/1973).
As shown by Baud (2003), these Freudian psychological mechanisms inspired certain doctors of the Swiss school to abandon the term ‘dementia praecox’, with its connotation of a premature degeneration of the brain, in favour of the term ‘schizophrenia’, which Bleuler had introduced as early as 1908, and this conceptual splitting of the mind reinforced the idea that voice hearing was symptomatic of a specific mental pathology. No longer hidden behind the more general notion of hallucination, auditory hallucinations became a component of schizophrenic symptomatology, representing a division (Die Spaltung) or dissociation of subjective consciousness. Henceforth, the paradigm of mental illness that had been dominant since 1856 gradually gave way to the structural paradigm resulting from the new Bleulerian conceptions (Grenouilloux, 2010).
The earlier categorizing of hallucinations gave way in time to a notion of AVH centred on the subjective experience and structural identity of the personality. It is in this context that Séglas (1892), employing the conceptions of Freud and Bleuler, led to the emergence of the structuralist psychoanalytical paradigm with its strong emphasis on language, as represented by the work of Clérambault (1872–1934), Lagache (1903–72), Lacan (1901–81) and Ey (1900–77) (see Brémaud, 2016). AVH phenomena were thus embraced and integrated into the concept of mental automatism (De Clérambault, 1987), which itself was to inspire Lacan (1980) to define these automatisms as elements within the broader field of the psychoses. Hypothesizing that unconscious processes were at play in the production of hallucinatory mechanisms, Lacan broke with the organo-dynamic psychiatric conceptions of Henri Ey, by insisting on the concepts of unconscious projection (Lagache, 1934: 1–129), forclusion (Lacan, 1956, 1994), and metonymy borrowed from Jakobson (1963: ch. 2).
In parallel with these psychoanalytical developments, the recognition of voice hearing by the psychiatric profession as a suppressible symptom led to the development of various treatments that were thought to be therapeutic, such as insulin injections, electroconvulsive shock therapy and lobotomies, all of which reinforced the stigmatization of madness and the fear and horror associated with AVH. In this context, it was not a matter of listening to the voices and working with their content, but of reducing and countering them.
In the 1950s the appearance of new chemical therapies such as tranquillizers, neuroleptics, antidepressants and hypnotics led to a general pharmacological approach in psychiatry that inevitably aimed to achieve the remission of what were construed to be psychotic symptoms. Soon after the introduction of psychotropic drugs, the idea that psychological pathologies derived from chemical imbalances in the brain swiftly gained ground within the scientific community, resulting in the publication of numerous studies on the physiological causes of voice hearing and attempts to reduce its incidence (Rapin et al., 2016). The introduction of chlorpromazine in 1954, in combination with other psychotropics such as Haloperidol and Valium, effectively abolished AVHs or the patients’ responses to them (Missa, 2008).
In some cases, psychopharmacology has made it possible to establish a dialogue with those who were otherwise untreatable, by reducing the incidence or severity of the AVHs that were causing suffering. Furthermore, it is important to emphasize that psychotropic treatments have made it possible to set up outpatient follow-up strategies, allowing individuals previously held in institutions to regain their autonomy. However, these advantages are counterbalanced by a loss of feeling and self-expression in the patient, which has become colloquially and aptly known as a chemical strait-jacket. This bio-psychiatric shift, accompanied by the emergence of behavioural therapies also aiming to abolish abnormal symptoms, has been particularly widespread in English-speaking countries.
In this context, a psychoanalytical approach that attributed meaning to symptoms according to the life history of the patient progressively lost ground to a psychiatric approach, where the curative aim was to control AVHs and thereby bring about a remission of the psychosis of which they were thought to be symptomatic.
The advent of voice hearing as a community phenomenon at the start of the twenty-first century
The 1960s saw the introduction of new theoretical models showing the need to consider the socio-environmental aspects and personal aspirations of the individual, which led to a transformation of the psychiatric field. Firstly, dissemination of a bio-psychosocial model proposed by Engel (1977) recalled the importance of psychological and societal influences in the genesis of psychiatric disorders. Then, having been foreshadowed by the Alma-Alta declaration (World Health Organization [WHO], 1978), the dissemination of the Ottawa Charter (WHO, 1986) counterbalanced the authority of the biomedical model by introducing the idea of promoting mental health. The concept consisted of granting individuals more control over their own psychological well-being by giving them greater means of improving it. In particular, these proposals advocated: the development of new mental health policies; the creation of an environment favourable to the mental health of the individual; the acquisition of personal skills; and the strengthening of community action (Clesse et al., 2018). Anchoring these initiatives to concomitant notions of empowerment and recovery created a context that has been conducive to Western psychiatry’s orientation towards a more community-based approach to mental healthcare.
It was within this context that psychiatrists such as Marius Romme (b. 1934) began re-evaluating voice-hearing phenomena, and in this regard his meeting with Patsy Hage, one of his patients whose AVHs were resistant to drug treatment, had proved decisive. After reading the book by Julian Jaynes (1976), Patsy reframed her voice hearing in the light of a different relationship to consciousness (Evrard and Le Maléfan, 2013). In his book, Jaynes suggested that, at an earlier stage of our evolutionary history, internally generated voices were interpreted as external commands coming from the gods and that this framing of perceptions and beliefs had some similarity with the schizophrenic experience of hallucinations and delusions.
Jayne’s theory was based on the neurological concept of there being a functional asymmetry between the left and right cerebral hemispheres, the former being associated predominantly with language and reasoning and consequently predisposing researchers to connect it with the mediation, if not the generation, of the conscious mind; on the other hand, the latter hemisphere was assumed to be the neurological substrate of the unconscious. Nevertheless, by reinterpreting ancient perceptions of voice hearing in the light of modern neurological research, Jaynes reintroduced the hypothesis of a mystical, spiritual origin for the phenomenon. As a result of this perspective, Patsy was able to establish a more peaceful relationship with her voices, and Romme thereby became aware of the important influence of an individual’s beliefs about the origin and causes of their AVHs. Since then, Romme has demonstrated how the introduction of complementary interpretations, including religious, medical, mystical, psychodynamic and parapsychological factors, has enabled subjects to enter more easily into a dialectical relationship with their voices, supported by a more personal and individual construction of meaning (Romme and Escher, 1993).
In a second phase of their research, Romme and Escher took an interest in the place held by AVH within the general population, and particularly in the number of individuals living with their voices in a monosymptomatic and adaptive manner (Evrard and Le Maléfan, 2013). To this end, Romme participated in a television programme in 1987 which appealed for voice hearers to contact them; they received 450 testimonies, 150 of which came from individuals who had adapted specifically to common social situations. To ascertain the nature of the strategies used for dealing with AVHs, Romme and Escher sent a questionnaire to these 150 individuals and conducted a series of in-depth interviews with 20 of them. Although partly biased by the willingness of participants to testify, the publication of the study (Romme and Escher, 1989) and the book that followed (Romme and Escher, 1993) had a major impact by proposing an approach that differed radically from the conventional biomedical model aimed at the suppression or erasure of AVH. Indeed, their work rested on a community-based approach to voice hearing which promoted research on AVH using a range of aetiologies and interpretations; they stressed the importance of exchanging information on the phenomena, and focused on the coping strategies that allowed voice hearers to live peaceably with their condition.
It is quite surprising that, of the seven cases selected by Romme and Escher (1993: 59–87) in illustration of the way some hearers manage to adjust to their voices without resorting to the mental health services, all had adopted a paranormal or spiritual interpretation of their experiences. As this kind of explanation became more common, it was less justifiably dismissed as being inevitably delusional. From their 1987 survey, Romme and Escher (1993: 98) found a predominance of paranormal interpretations over biomedical ones such as neurochemical imbalance or perceptual and cognitive failure.
According to Myrtle Heery (1989), the significant presence of paranormal and spiritual interpretations derives from the fact that they constitute an intermediate zone between the classical pathological perspective and the traditional religious one. This intermediate position provides enough flexibility for everyone to find something to seize upon in their attempt to find suitable meaning in their unusual experiences (Evrard, 2014); it also allows the individual to combine elements from several models without having to follow fixed dogmas or accept limiting conventional perspectives. Neither saints nor psychotics would seem to be the watchwords for Heery. This is reminiscent of the key role played by the paranormal in Western culture, where an affiliation of the demonological and preternatural provides an intermediate conception leaning towards the typically Western cleavage between science and religion (Kripal, 2022).
In a third phase, Romme and Escher endeavoured to encourage the participatory and community aspect of voice hearing by creating an organization to coordinate and support the Hearing Voices Movement by enlisting voice hearers, their relatives and friends, and mental health professionals including therapists, social workers, nurses, psychiatrists and psychologists. INTERVOICE (The International Network for Training, Education and Research into Hearing Voices) was announced at the first congress on voice hearing in Maastricht in 1997. At this major scientific event, the 20 voice-hearers who had been interviewees were invited to give lectures on their experiential knowledge of AVH and their personal coping strategies. This innovative approach already represented ‘the displacement of knowledge from a psychiatry considered closed to popular knowledge, in a process of emancipation and self-management of mental health’ (Evrard and Le Maléfan, 2013: 625). This experiential-based emancipation is illustrated by the Hearing Voices Groups (HVGs) set up in 1988 (Gardien, Héas and Laval, 2019), which were organized within a system of community-based peer support. These groups aimed to assist those concerned with the AVH phenomenon by pooling experiential knowledge and thus helping voice hearers to help themselves.
Since this initiative, HVGs have enjoyed the benefit of exchanging experiences and strategies within an environment that is not subjected to the negative social perceptions usually associated with AVH within psychiatric settings (May and Hayes, 2012; Molinié, 2018). It should be noted that choosing the name ‘voice hearers’ was intended in itself to reduce negative attitudes by placing the notion of the individual at the very heart of the HVM (Romme and Escher, 1996: 137–51). The name echoes the many lexical changes within the field of mental health that have aimed to provide a context for the patients by characterizing them as active participants in their treatment in order to reduce the metaphorical and metonymic confusion between a subject and his or her psychological problem (Clesse et al., 2018; Morrison, Frame and Larkin, 2010). Although tentative at the start of the 1990s, the establishment of HVGs accelerated during the decade in the UK and later in Canada and the Netherlands (May and Hayes, 2012).
The research dynamic around voice hearing is thought to have allowed INTERVOICE to benefit from scientific support that has consequently modified the previous negative attitudes within certain institutional circles that were resistant to the notions of collaboration and full participation (Corstens et al., 2014).
From the 2000s onwards, the spread and acceptance of community-based support within the domain of mental health, along with the decompartmentalization of psychiatry and an opening up to the social field, facilitated the setting up of HVGs throughout Western society (Longden, Read, and Dillon, 2018; May and Hayes, 2012). Local initiatives to create such groups were then considered as a participatory alternative that strengthened the substratum of citizens hearing voices. Similarly, the psychiatric field, influenced by the idea of psychosocial rehabilitation, seems to have forged useful links with HVGs (May and Hayes, 2012) and recognized their social relevance and secondary therapeutic benefits (Sapey and Bullimore, 2013; Styron, Utter and Davidson, 2017). The development of patient-centred listening appears to circumvent some of the stigma and marginalization associated with mental illness (Bacchi et al., 2023). However, ‘the effects of hearing voices groups on participants’ voice hearing are still poorly studied’ (Molinié, 2018: 118).
Driven by this general community-based dynamic, the voice hearing – which had previously been considered an object of study and then later of activism – has, since 2019, become a research field in its own right (Iudici, Quarato and Neri, 2019). Thus, the questioning of diagnostic categories related to AVH (Woods, 2013) has led to research bringing a more detailed understanding of the similarities and differences between the phenomenon and the condition of psychosis (Baumeister et al., 2017; Braun, Evrard and Génot, 2020; Moskowitz, Mosquera and Longden, 2017; Sommer and Van der Spek, 2016). Similarly, further study has shown how the phenomenon may be preferentially associated with psychosocial characteristics (Longden, 2017), personal variables such as self-esteem and self-consciousness (Fannon et al., 2009; Naudin et al., 2000), shame (Woods, 2017), and the disruption of the relationship between an individual’s outward speech and their inner thoughts (Brar, 2018). Finally, original studies have highlighted the role and place of gender in AVH (McCarthy-Jones et al., 2015).
Although research on AVH appears to be growing, the efficacy of HVGs awaits scientific validation and the recommendation of health authorities. On the other hand, the growing number of HVGs in many Western countries suggests the HVM and the INTERVOICE institution supporting it are becoming recognized by associations and local authorities.
Discussion
Our systematic survey of the literature has enabled us to retrace the historic path of voice hearing. Perceived in antiquity as a mystical phenomenon with a recognized social position and utility, the phenomenon gradually lost its usefulness during the medieval period, largely owing to a variety of religious dogmas that represented it as a deviant practice. In the Renaissance, under the influence of the humanist movement, such dogmatic perceptions were accompanied by the creation of socially regulated dispensaries wherein those who heard voices were confined, along with others the Church considered as being marginal members of the community. During this process, voice hearers lost the social position they had enjoyed for centuries. In contemporary times, the individual social exclusion and attendant loss of democratic political power resulting from these dynamic processes allowed the emerging medical powers to impose their authority within the dispensary; this favoured the generation of new approaches to the nosography of voice hearing incorporating a medical definition of hallucinations. The incipient medicalization of madness and voice hearing in turn facilitated the integration of medical authority into the managerial structures of the dispensaries which subsequently became known as asylums. This whole process was accompanied by the development of psychoanalysis and later by the development of twentieth-century psychological and psychiatric science, which jointly aimed to suppress AVHs because they were deemed by the biomedical model to be an unacceptable symptom of mental illness. Finally, from the end of the 1980s onwards, the founding of the Hearing Voices Movement made it possible to envisage a new ideal in which voice hearers were helped to achieve cohabitation with their voices.
At present, research on the AVH phenomena suggests only a minority of individuals are able to achieve the ideal, so the initiative has so far had only a mild impact on mental health. Hearing Voices Groups which were set up in English-speaking countries during the 1990s have spread to the rest of Europe in the following decades. The primary objective of this process has been to nuance the prevailing medical discourse in Western society by insisting on the importance of individual empowerment for the voice hearer and the authentication of their experiences and knowledge. It has also tended to provide a social place for the AVH phenomenon and to articulate a feeling of social utility for those who experience it, within a setting of helpful peers and facilitators. Although participants in HVGs have themselves said the experience has helped them to rejoin society, so far the scientific research has not provided significant validation of this nor of any change in the social perception of voice hearing.
Various factors have profoundly influenced the social-historical evolution of the AVH phenomenon and contributed to an awareness of the way in which the perception of voice hearing across the ages has evolved according to the social position it has been allocated. An initial restriction within the social sphere was apparent towards the end of antiquity and became more pronounced during the Middle Ages when the great monotheistic religions dogmatically condemned voices as the work of the Devil. The ensuing debates between belief and reason and between religion and science questioned the validity of ascetic practice and mystical phenomenology, and the consequent displacement of beliefs and the modification of their content called into question the nature of the unseen, which until then had been explained in terms of the existence of supernatural entities (Schmitt, 1995). This process seems likely to have reinforced the condemnation of voice hearers, since they were now no longer able to be understood and accepted in the former manner, and this conjectured loss of a social place for voice hearing would have been completed with the institutionalization of individual hearers in modern times.
The loss of a social place for voice hearing has led to the disappearance of its social utility, especially its traditional function of mediating with the divine; since antiquity this progressively declined in importance owing to tendencies which first characterized the phenomenon as deviant, then as a social disorder, and finally as an expression of pathology. By ceasing to be an integral part of Western culture, the hearing of voices has moved from a public and visible sphere to a private one. From a global perspective, invisible forces in general and the role of individuals in maintaining a divinatory function for voice hearing have been subjected to this process of exclusion in the West (Réal et al., 2014). The restriction of certain categories of experience to the strictly private domain under the pretext of a social or religious taboo is characteristic of numerous instances of social stigmatization leading to marginalization and discrimination (Perrot and Collin, 1988). Recently, however, modifications made to major international classifications in terms of diagnostic criteria suggest that mediumship, along with other exceptional psychological experiences, are tending to be depathologized (Braun et al., 2020).
The diffusion of HVGs through the social spaces allotted to them in Western society may at least allow individuals experiencing AVHs to regain a social position based on the notion of community. By activating various levers inherent in the re-establishment of a social place for voice hearers, the Hearing Voices Movement and INTERVOICE hope to promote the re-appropriation of a useful role and visible public presence for voice-hearing individuals. This is another reminder of the importance of social factors in the domain of mental health and of the need for genuine cooperation between the various political, medical and social authorities in the effort to improve the care and support for those requiring mental health services (WHO, 2013–20). Similarly, it shows once again how the integration of marginalized individuals into society leads to empowerment by allowing them to feel socially useful and making it easier for them to become active participants in the course of their own lives (May and Hayes, 2012).
Finally, it is important to note that, in spite of its anti-psychiatric dogmatism (Braun et al., 2020), the HVM has generated a great deal of the psychiatric and psychological thinking on the AVH phenomena. Indeed, the birth of the movement has reintroduced voice hearing as a distinct object of research, for previously it had been indefinitely classified under the more general notion of hallucination or delusion, but it is now an object of study in its own right and recognized for its transdiagnostical nature (INSERM, 2020). Despite the existence of antagonistic opinion, it is likely that the movement will bring a better understanding of AVH in the psychiatric field: firstly, by forcing the clinical and scientific fields to modify their views, the personal and societal repercussions of which have long been neglected; and secondly, by encouraging the creation of community spaces that make mental disorders visible, reconsidering their place and usefulness within society, and initiating a policy of reconciling individuals to their disorders. However, the movement’s perceived political activism may possibly have been a hindrance to the dissemination of the recent scientific data on voice hearing, as research results do not necessarily support the ideal claimed by those extolling the movement (Bacchi et al., 2023).
Strengths and weaknesses
A particular strength of the approach used in this paper has been to include most of the literature on the history of hearing voices in one narrative systematic review. One of its advantages has been the bilingualism of the selected references, although of course a multi-linguistic selection going beyond English and French would be even better. This bilingualism has a limited significance since our study is focused on a limited number of countries.
Other advantages have been the large number of keywords and databases, and the inclusion of grey literature known to be a relevant medium of dissemination. Finally, an effort of contextualization has been undertaken to highlight the various factors that have potentially influenced the evolution of hearing voices through the ages.
However, this work is not without significant limitations. The methodological content of the reviewed literature, with its limited number of articles specifically focusing on the history of voice hearing, must certainly be considered as one of them; another is the existing confusion between voice hearing and the more general notion of delusion or hallucination, which has probably led to the exclusion of relevant articles not mentioning the notion of hearing voices as a specific concept.
Naturally, an extensive timeline necessarily allows for only brief sketches of each period and in insufficient detail. Applying a systematic review to the historical literature, the study might be considered a historical research paper examining secondary sources in the history of psychiatry with a critical lens, while giving attention to historiography.
Conclusion
A history of voice hearing highlights the importance of the sociocultural factors at play, contributing to the public perception and official position of the phenomenon. We envisage this article as a meeting place for those interested in the history of psychiatry, taking voice hearing as a common thread. What emerges, even across the medicalization of hearing voices, is that there were exceptions granted to individuals with social, religious or political power. By dealing with the phenomenon within the community and creating groups of empowered voice hearers, it may eventually become possible to allow voice hearers to find a place for themselves within society.
Instead of the taboo and the automatic fear of ‘going crazy’ that usually accompany such experiences (Schetsche, 2013), a form of alternative socialization may emerge that allows those who hear voices to occupy a more rewarding place within our Western societies, rather like the shamans, seers and mystics in other cultures and of former times.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.