
Abstract
This study examines attempted suicide in older people between 1870 and 1908 in (NSW), Australia. Statistical Registers of NSW indicate persons aged 60+ had disproportionately high rates of apprehension (10.9%) and conviction (13.0%) for attempted suicide. Newspaper reports of 110 suicide attempts in older people indicate that alcohol misuse, poor health, depression, being tired of living, financial problems, relationship difficulties, loss events and insanity were the main issues. Most were treated compassionately with medical care and support, albeit sometimes in a gaol setting. Medical casebooks of persons aged 60+ years with suicide attempts (n = 49) or suicidal ideation (n = 43) admitted to hospitals for the insane indicated that over 75% were psychotic and 50% had melancholia.
Introduction
In February 1876, Solomon Meyer, the member for Carcoar in the New South Wales (NSW) Legislative Assembly, was unsuccessful in proposing an amendment with a clause about attempted suicide – which at that time could result in imprisonment for up to two years – to the Act that abolished the coroner’s jury verdict of Felo-de-se suicide. Meyer was concerned that ‘the knowledge on the part of an intending suicide that there was a sentence of two years’ imprisonment hanging over him if he failed, would have the effect of making him commit the suicide effectually’ (Anon., 1876: 2). Instead, he proposed that a person attempting suicide should be bound over to keep the peace for six months. Meyer stated that if sent to gaol, a man ‘might become a confirmed lunatic, but if he were placed among his friends and carefully nursed he might be restored to perfect sanity’. The amendment failed as it was regarded as being beyond the scope of the Bill, but there was a brief debate during which another member, Michael Fitzpatrick, expressed the view that those who attempted suicide ‘ought to be punished to some degree’ (Anon., 1876: 3). Eventually, in Section 18 of the Criminal Law and Evidence Amendment Act of 1891 (NSW Parliament, 1891), attempted suicide was specifically covered and could be dealt with summarily by magistrates, thus avoiding long periods on remand awaiting higher courts; the maximum sentence was set at six months (NSW Parliament, 1891).
Solomon Meyer’s views probably reflected the prevailing attitudes of the time towards attempted suicide in NSW and the other Australian colonies. Greg Taylor, in his overview of how the legal system in Australia dealt with people apprehended for the crime of attempted suicide in the late nineteenth century, observed that the legal process was mainly a means of checking their welfare and ensuring they had people to care for them to prevent future suicide rather than as a process for punishment (Taylor, 2022). This approach was a reflection of contemporary views in the UK. Olive Anderson notes that suicidal behaviour in the second half of the nineteenth century was regarded as mainly occurring in the context of some form of alteration of mental function, as the result of distress from life events, particularly those associated with loss, intoxication with alcohol or drugs, physical ill-health, or outright insanity, although some people still regarded it as a sin requiring punishment. Efforts to prevent suicide attempts included social casework through police magistrates, the stipendiary and prison chaplains for those put on remand (Anderson, 1989).
Nineteenth-century research into suicide and the factors associated with it was quite far-reaching and provided clinicians and others some guidance into the assessment and management of suicidal individuals. In his Treatise on Insanity, Esquirol (1838/1845) gave examples of suicidal behaviour associated with various forms of insanity, as well as examples ‘provoked by the passions’ such as ‘a sudden and unexpected trial, love betrayed, ambition disappointed, honor compromised, the loss of fortune, by overthrowing the reason, deprive man of the power of reflection’ (pp. 256–69). Perhaps the most comprehensive nineteenth-century examination of suicide was undertaken in 1879 by the Italian Enrico Morselli, who provided a detailed statistical analysis of various sociodemographic, ethnological, geographic and psychological factors associated with suicide. Although he did not consider attempted suicide, Morselli was the first investigator to provide detailed statistical evidence that suicide rates increased with age (Morselli, 1879/1882: 215–19). Previously the relatively low numbers of older people in populations worldwide obscured the high suicide rates in their midst. In 1912, Sir George Handley Knibbs, the Commonwealth statistician, provided the first detailed evidence that Australian suicide rates in the period 1891–1910 peaked in males aged 60–65 years (Knibbs, 1912).
In contrast to suicide, there has been limited research into attempted suicide in the late nineteenth and early twentieth centuries, particularly in older people. In England and Wales, judicial statistics provide an indication of the prevalence of attempted suicide and how it was dealt with by the judiciary. The annual number of attempted suicide crimes reported to the police increased from 914 in 1875 to 1466 in 1894, while the number of prosecutions increased from 65 (7%) in 1875 to 158 (11%) in 1894. Data from 1890–4 indicate that around 75% of prosecutions were convicted (Home Office, 1896: 41–9). In 1885–6, only seven out of 137 (5%) attempted suicides that went to trial were found insane, while of those convicted, 69% were imprisoned (usually for less than a month) with the rest fined or discharged on sureties (Home Department, 1887: 45). By the 1890s in England, recorded suicide attempts far outnumbered suicides and, in contrast to suicides which usually occurred in older men, these tended to occur in younger women. Impulsivity and drunkenness rather than insanity were common features. It was believed that in many cases death was not the intended outcome but rather it was a ‘cry for help’ or sympathy or to produce remorse (Anderson, 1989).
Details of older people who attempted suicide are limited. In a study of older admissions to lunatic asylums in Oxfordshire, Yorston and Haw (2005) found that between 1826 and 1900, of 93 patients aged 60+ years admitted to Warneford Asylum, six (7%) had presented with suicide attempts and 12 (13%) had suicidal thoughts. At Littlemore Asylum, between 1846 and 1890, of 250 admissions aged 60+ years, 53 (21%) presented with suicide attempts and a further 22 (9%) had suicidal thoughts. Males had higher rates of suicide attempts at both asylums. No other clinical details were provided about these specific patients. Similarly in NSW, as reported by Draper (2021), 24% of admissions of people aged 60+ years to Gladesville and Callan Park hospitals for the insane, between 1849 and 1905, presented with self-harm or had suicidal ideation with higher rates in females, but no details were provided of these cases.
While Taylor’s (2022) examination of attempted suicide in late nineteenth-century Australia does not include any examples of people identified as being old, it does provide a good overview of the types of factors reported in the judicial hearings and the outcomes. He notes that most were released after a ‘jolly good talking-to’ or a short time in prison for their welfare, while exceptions to this approach tended to occur after repeated attempts or ongoing suicide risk in those without family and friends, where the person was a danger to others, and if the judge had a particular aversion to the crime.
As an immigrant colony, NSW had a low proportion of older people in its population for most of the nineteenth century, and these were predominantly males. In 1861, only 3% of the population were aged 60+ years, but during the next 50 years this more than doubled to 6.2% in 1911, with the main growth occurring after 1891 (Australian Bureau of Statistics, 2006: Tables 21 and 22). Population ageing was driven by ageing immigrants, many of whom had migrated for the gold rushes of the 1850s and 1860s and had limited family support networks, few skills and no property. Due to the sex imbalance in the colony, many ageing men were unmarried and, because they had worked predominantly in labouring occupations, their health was often affected by the poor working conditions. Many were left alone in old age, having inadequate finances and chronic ill health, with their circumstances often accentuated by alcohol misuse in the masculine pub culture (Jalland, 2015: 14). During an economic downturn and prolonged drought in the early 1890s, many people lost their life savings when building societies and banks crashed in 1892–3 (Barnard, 1963: 411–12). This had an increased impact on older people, with older workers often being first to be laid off, while those who had invested in rental properties suffered from depreciation of property values and also had difficulty in getting rents from unemployed tenants (Davison, 1995: 46).
In combination with population ageing, these economic events led to a crisis in care for the aged (Jalland, 2015: 14). This was reflected in admissions of persons aged 60+ years to NSW hospitals for the insane. Between 1881 and 1905, while the total number of admissions approximately doubled, admissions of persons aged 60+ years, predominantly men, more than trebled (Draper, 2021). Similarly, O’Brien (1988: 58–9) found that admissions to Government Asylums for the Destitute and the Aged between 1890 and 1900 nearly doubled, most being immigrants with no living relatives. Both types of institutions were overcrowded, and conditions, particularly in the Asylums for the Destitute and Aged, were often poor with buildings filthy and poorly maintained (Garton, 1990: 58). In the latter, the more able-bodied inmates were expected to do all of the work as there were no paid nurses until after 1887. A governmental Board of Inquiry in 1887 acknowledged that the inmates were oppressed, neglected and cruelly treated (Jalland, 2015: 20). Even in the economic depression of the early 1890s, many impoverished older people lived by begging, were often homeless, and preferred to starve themselves to death rather than enter a ‘detested’ asylum (p. 22).
In order to address these issues, a means-tested old-age pension of £26 per annum was established in 1901 for those aged 65 years and older who had lived in NSW for at least 25 years, although it had an exclusion of ‘unsatisfactory moral character’ and required evidence of ‘sober and respectable life’ for at least five years, while Australian Aborigines, aliens and ‘Asiatics’ were totally excluded. By 1906–7, 39% of older people in NSW were on the pension. While the pension was a significant improvement, it still left many older people struggling (pp. 26–31).
Thus, during the late nineteenth and early twentieth centuries, older people in NSW faced many challenges, and it is little wonder that some attempted suicide and others died by suicide. The aims of this investigation are, for the period 1870–1908: (i) to determine the number of apprehensions (arrests) and judicial outcomes for attempted suicide in NSW with a focus on those aged 60+ years; (ii) to examine newspaper reports of arrests for attempted suicide in older people to determine factors identified as contributing to the act and the reported outcomes of judicial hearings; and (iii) to examine admissions of people aged 60+ years to NSW hospitals for the insane, who had attempted suicide or expressed suicidal ideation, and to describe their symptoms, behaviours and mental disorders, and the treatment outcomes.
Method
Information about suicides and attempted suicides was extracted from the annual NSW Statistical Registers which are retained at the NSW State Archives, although the collection is incomplete for the period 1870–1908; the registers for the following years are available: 1870–1, 1873–4, 1879–83, 1887–90, 1892–3, 1895–6, 1898–1904, and 1906–8. Attempted suicides were reported as crimes, although the style of reporting varied over time and usually not by age. Between 1879 and 1890, however, the number of apprehensions aged over 60 years were reported, and between 1906 and 1908 the number of convictions aged over 60 years were reported. Between 1889 and 1906 the gaol sentences of those convicted of attempted suicide were reported.
Newspaper reports of ‘attempted suicide’ in people aged 60+ years or described as ‘elderly’, ‘aged’ or ‘old’, but without a stated age, were examined in a search undertaken on the Trove search engine of newspapers compiled by the National Library of Australia. The search was limited to the period 1870–1908 for suicide attempts in NSW. In this era, newspaper reports were usually published at the time of the arrest, where information focused on details of the attempt and associated medical issues, and after the magistrates hearing where extra information might be provided along with details of the outcome. At both time points the identity of the individual was published, and frequently the age as well as a variable amount of information about living arrangements, marital status and the circumstances pertaining to the suicide attempt. Reports from multiple newspapers were obtained where available to maximise the information. A sample size of approximately 100 suicide attempts was targeted.
The medical casebooks of patients aged 60+ years admitted to Gladesville and Callan Park Hospitals for the Insane in the period 1870–1906 were examined in 2019–22 at the NSW State Archives. All admissions in this period were involuntary. The medical casebooks are very large bound books that include up to 300 patients per book, including demographic details and the admission diagnosis at the top. The admissions were added chronologically in each casebook, and each patient was given an ID number. Data were extracted from casebooks which were randomly selected from each decade: eight out of 20 casebooks were from the 1870s; nine out of 25 casebooks were from the 1880s; nine out of 32 casebooks were from the 1890s; and six out of 14 casebooks were from 1900–6.
Admissions aged 60+ years that had either evidence of a suicide attempt or suicide ideation including threats were selected. Data extracted included socio-demographic details, reason(s) for admission, identified stressors, recorded diagnosis, symptoms and behaviours, mental state examination, outcomes of the admission (discharge, transfer, death and length of stay) and any incidents of care such as episodes of self-harm. Verbatim transcripts of the admission notes were made, as well as medical certificates accompanying the admission and pertinent continuation notes. A sample size of approximately 50 individuals with suicide attempts was targeted.
Frequency distributions were analysed using the chi-squared test. Ethics committee approval was obtained from the University of New South Wales Human Research Ethics Committee (#190705) and approval was obtained from the NSW Ministry of Health to use the medical casebooks in de-identified form.
Results
NSW Statistical Registers
The annual number of apprehensions and convictions for attempted suicide across the age range increased over the study period, with convictions increasing at a greater rate than apprehensions, particularly after 1890 when the number of people whose charges were dismissed, withdrawn or were acquitted declined (see Table 1). Using NSW Census statistics (Australian Bureau of Statistics, 2006), population-based rates of conviction increased from around one per 38,750 persons in 1871 to a peak at around one per 17,300 persons in 1892, before declining to around one per 23,350 in 1901.
Mean number and percentage of annual apprehensions, commitments, discharges, convictions, acquittals and gaol sentences for attempted suicide in NSW, 1870–1908.
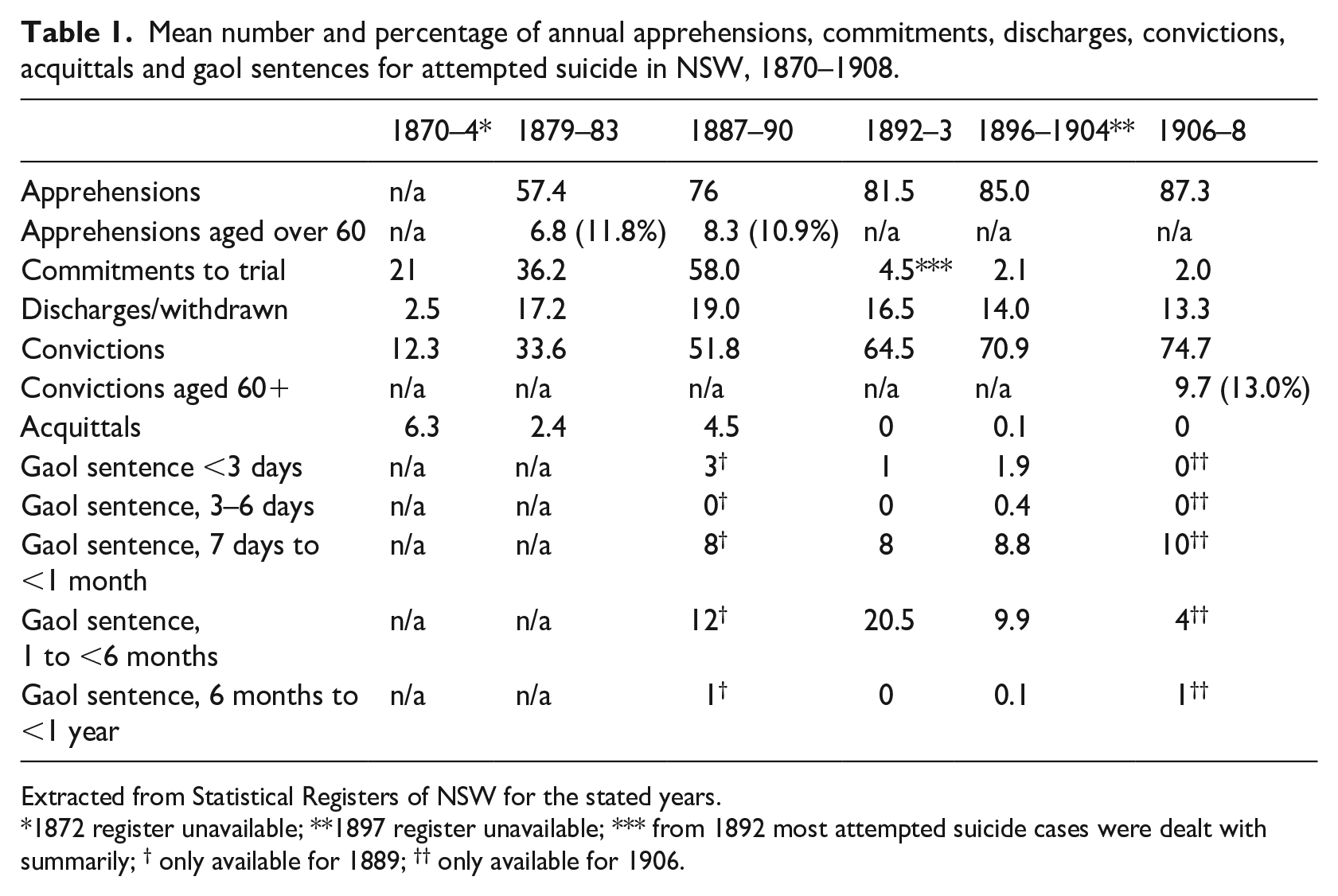
Extracted from Statistical Registers of NSW for the stated years.
1872 register unavailable; **1897 register unavailable; *** from 1892 most attempted suicide cases were dealt with summarily; † only available for 1889; †† only available for 1906.
There were more male than female apprehensions throughout the period, although the proportion declined from 79% between 1879 and 1883 to 63% between 1906 and 1908. While females accounted for only 22% of apprehensions between 1879 and 1890, 35% of discharges were female. After 1890, the proportion of females who were discharged declined, so that by 1906–8 they only represented 27.5% of discharges, although they accounted for 37% of apprehensions.
Between 1879 and 1890, apprehensions in persons aged over 60 years totalled 67 (10.9%) for the nine years where data was available. This is more than double the proportion of people aged 60+ years (4.3%) in the NSW population in 1881 and 1891 (Australian Bureau of Statistics, 2006: Table 21). Convictions for attempted suicide in persons aged 60+ years were reported between 1906 and 1908; all were males. The proportion of convictions by those aged 60+ years (13%) was more than double the proportion of persons aged 60+ years in the population (5.6% in 1901, 6.2% in 1911) (Australian Bureau of Statistics, 2006: Table 22).
While no information was available about sentences in older people who were convicted, for the period 1892–1906 a third of all convictions were gaoled. Convicted males (n = 540) were significantly more likely to receive gaol sentences (n = 214, 39.6%) than were convicted females (n = 225), of whom 41 (18.2%) were gaoled (χ2 = 32.75, df = 1, p < 0.0001). While a higher proportion of male gaol sentences were for one month or over (n = 117, 54.7%) longer than female gaol sentences (n = 19, 46.3%), this difference was not statistically significant.
Newspaper reports
Newspapers reported 81 individuals aged 60+ years who had attempted suicide between 1870 and 1908; two made multiple attempts, with one male making five attempts using the same method over a five-year period and another male making two attempts with the same method within four months. A further 29 individuals were described as ‘elderly’, ‘aged’ or ‘old’ without a specific age; of these, one male made two attempts with different methods. The most common method of self-harm was a cut throat (n = 71, 64.5%), while overall 90 (81.8%) involved cutting some part of the body (see Table 2).
Newspaper reports of attempted suicide in older people in NSW, 1870–1908.
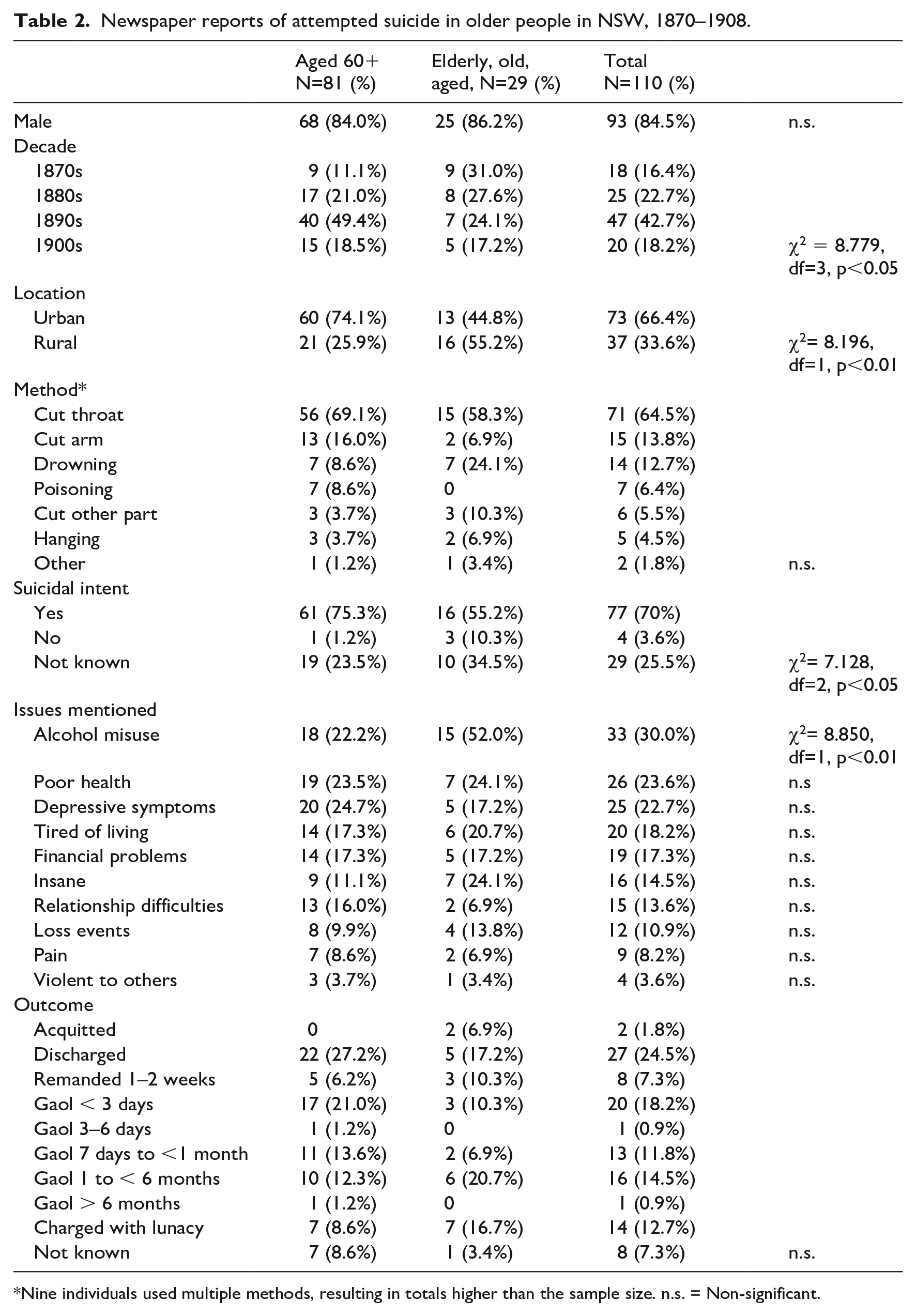
Nine individuals used multiple methods, resulting in totals higher than the sample size. n.s. = Non-significant.
In individuals with a recorded age, males (mean age 69.5 years) were older than females (66.6 years), with the oldest person being a 90-year-old male residing in an asylum for the destitute and aged. Marital status was infrequently mentioned (36/110), with most of these being married which largely featured in the reports as the spouse discovering the victim. Living arrangements were mentioned more frequently (72/110) and notably 12 were residents of asylums for the destitute and the aged, nine were homeless, and nine lived in a boarding house.
Table 2 summarises reported features of the suicide attempts, the methods used, and the outcomes of the legal proceedings (in those with multiple attempts, only the index attempt is considered). While there are broad similarities between those aged 60 and over and those described as being ‘elderly’, ‘aged’ or ‘old’, those with a specific age were significantly more likely to reside in an urban area and the suicide attempt was significantly more likely to occur in the 1890s or 1900s. Those with a known age had significantly clearer evidence of suicidal intent.
Alcohol misuse was the most commonly identified issue, particularly in those without a known age. Some were described as having a long history of alcohol dependence, while others were intoxicated in the context of a life event such as financial loss, bereavement or physical ill health, or were drinking heavily while feeling depressed. Many had been drinking heavily before the attempt, with the effects sometimes described as being in a state of ‘delirium tremens’; for example, one old man who had been drinking heavily at an isolated rural property imagined that he heard men outside plotting against his life and consequently cut his throat with a knife he found on a nearby table (Anon., 1891). Heavy drinking could be associated with health and accommodation issues; for example, in 1903 a 70-year-old homeless old-age pensioner had been ill with chest pains and had recently unsuccessfully tried to get admitted to an asylum, felt ‘tired with life’, and cut his throat at the back of a hotel (Anon., 1903).
Poor physical health was a second common issue, particularly in males. These were usually chronic illnesses, with many involving pain, physical dependence, frailty and associated feelings of depression. For example, a 70-year-old man living with his wife had been paralysed in his legs for 12 months and had become ‘tired of life’. He cut his throat and arm with a razor (Anon., 1895). Three had sustained injuries in falls and were left with chronic debility. In the absence of alcohol misuse, magistrates and judges tended to treat these cases leniently with most being discharged, some with sureties.
Severe mental illness was another issue, and 14 individuals were charged with lunacy, usually in the context of the person being psychotic. For example, a 71-year-old woman cut her throat in the context of having been ‘dull and in low spirits’ since the death of her husband nine months earlier. She was suspicious and delusional, and experienced hallucinations (Anon., 1885). Other individuals had symptoms of depression likely to be part of a clinical depression, such as a 73-year-old boarding-house resident who swallowed mercurial ointment and then cut his throat after being summoned for a minor offence. For some months he had threatened suicide because he was tired of life and depressed as he found it hard to get a living as a dealer. He was imprisoned for a few hours in the police cells (Anon., 1898). Such cases were not usually charged with lunacy. In this era, while there was growing recognition of late-life melancholia as a cause of insanity – as epitomised in the work of Emil Kraepelin (1905/1906: 1–10), lesser degrees of depression, that in modern practice is regarded as a mental illness, might not have received the same attention. Thus depressive symptoms, in the absence of features of insanity, did not seem to have any particular impact on the judicial outcomes.
Nearly 20% of the newspaper reports quoted the older person as stating that the reason they attempted suicide was because they were ‘tired of living’. Few of these individuals were also described as being depressed or despondent. For most, it seemed that their life circumstances appeared to be untenable and without an obvious solution apart from suicide. Modern research has shown that older people who are ‘tired of living’, but not clinically depressed or terminally ill, and wish to die may have a range of age-related losses (such as of health, meaning, self, connectedness or control); they may have experienced past traumas, have personality characteristics that impede their ability to adapt to life changes, and do not wish to be a burden on others and nor do they fear death. ‘Tired of living’ can be regarded as a metaphor for being physically and mentally fatigued such that there is no fight left, and it might also describe boredom with living (van Wijngaarden, Leget and Goossensen, 2014). These observations are likely to have also been relevant a century ago.
Various life events traumatised individuals. For example, a 70-year-old married woman’s experience of being washed down the sewer had been reported in the newspapers with a sketch causing her embarrassment with the neighbours (Anon., 1905). A 70-year-old caretaker was the victim of a hoax perpetrated by youths who told him that he had inherited a considerable sum of money in the UK and his presence in London was required as early as possible to prevent the money going into Chancery. He had already purchased his passage tickets to claim it when the hoax was revealed. In his disappointment, he cut his throat after drinking heavily for a few days (Anon., 1897a, 1897b). For 10 individuals, financial worries were attributed to being unemployed.
There were two broad groups of issues for residents of Asylums for the Destitute and the Aged. One was related to persistent despondency and depression; for example, a 60-year-old woman had been very disconsolate since moving to the asylum eight months ago after living with her daughter. She wanted to end her life as it had become unbearable to her and she made a number of threats that were ignored and put down to ‘the grumblings of senility’. She tried to hang herself with a mosquito net that was turned into a rope and was sent to the reception house for 21 days’ observation (Anon., 1894). A second issue related to reactions to institutional care; for example, a discontented 66-year-old man stabbed himself in the abdomen because he had not been put on the doctor’s list at the asylum. As he was sick and in pain, he thought that he would be ‘better out of the world’ (Anon., 1908).
The outcomes listed in Table 2 suggest that, when convicted, older people were likely to be gaoled (50/77; 65%), although many were kept for less than 24 hours. In 12 cases the period of imprisonment or remand was to be undertaken in the gaol hospital to facilitate recovery. Convicted males were more likely to be gaoled for three days or more (29/68; 43%) than females (2/10; 20%). Of those sentenced to two or more months in gaol, seven out of the 11 were noted to have alcohol problems, while 16 alcohol-related cases were imprisoned for over a month. The longest gaol sentence was for 9 months, without an obvious explanation for its length. It is possible, in an era when there were no formal alcohol treatment resources, that some magistrates and judges viewed imprisonment as the best alternative. Attitudes of the judges and magistrates towards sentencing could vary. One judge, in giving a sentence of 4 months’ imprisonment to an elderly married man who had cut his throat with a razor while intoxicated, commented that the Minister for Justice recently intervened in a similar case and ordered the accused to be discharged (Anon., 1889). In another example, a single old man, residing with his nephew in a rural property, stabbed himself five times in the chest and abdomen with a butcher’s knife, resulting in severe injuries requiring surgical attention. His nephew noted that the man had been quiet for two weeks before the incident. The old man told the police: ‘I am getting an old man and feel that I am not wanted’ and ‘I felt that I was in everybody’s way, so I decided to kill myself.’ Two weeks later, after being closely watched during his convalescence from his wounds and being regarded by the doctor as ‘rational’, he went before the local magistrate, pleaded guilty to the charge of attempted suicide and was sentenced to four months’ imprisonment with light labour. There had been no previous suicide attempts (Anon., 1902). Of the three individuals who made repeat attempts, two received a one-month sentence on a subsequent attempt. Interestingly, one man who made five attempts was discharged after his fourth and fifth attempts.
Referral to an Asylum for the Destitute and the Aged occurred in 11 cases. In addition, most of those who were already residing in such an asylum returned to one, sometimes a different one. This was not a solution welcomed by everyone. A 78-year-old man stated: ‘I don’t want to go to the benevolent asylum. I can get my living by working, and I don’t want charity.’ The magistrate then imposed a gaol sentence of two weeks (Anon., 1896).
Two individuals subsequently died by suicide within 12 months of their original suicide attempts, while the coroner’s inquest into the drowning of a third man four months after a suicide attempt could not determine whether it was accidental or suicide.
Medical casebooks from Hospitals for the Insane
The medical casebooks of 430 patients aged 60+ years admitted to Gladesville and Callan Park Hospitals for the Insane between 1870 and 1906 were examined. There were 49 admissions (11.4%) presenting with suicide attempts, while a further 43 (10%) had evidence of suicidal ideation. There was no significant variation in the proportion of admissions with suicide attempts or suicidal ideation between decades during the study period, although the highest proportion of suicide attempts (15.3%) was in the 1870s. Details of the cases are presented in Table 3.
Suicide attempts and ideation, and admissions to Callan Park and Gladesville Hospitals, aged 60+ years, 1870–1906.
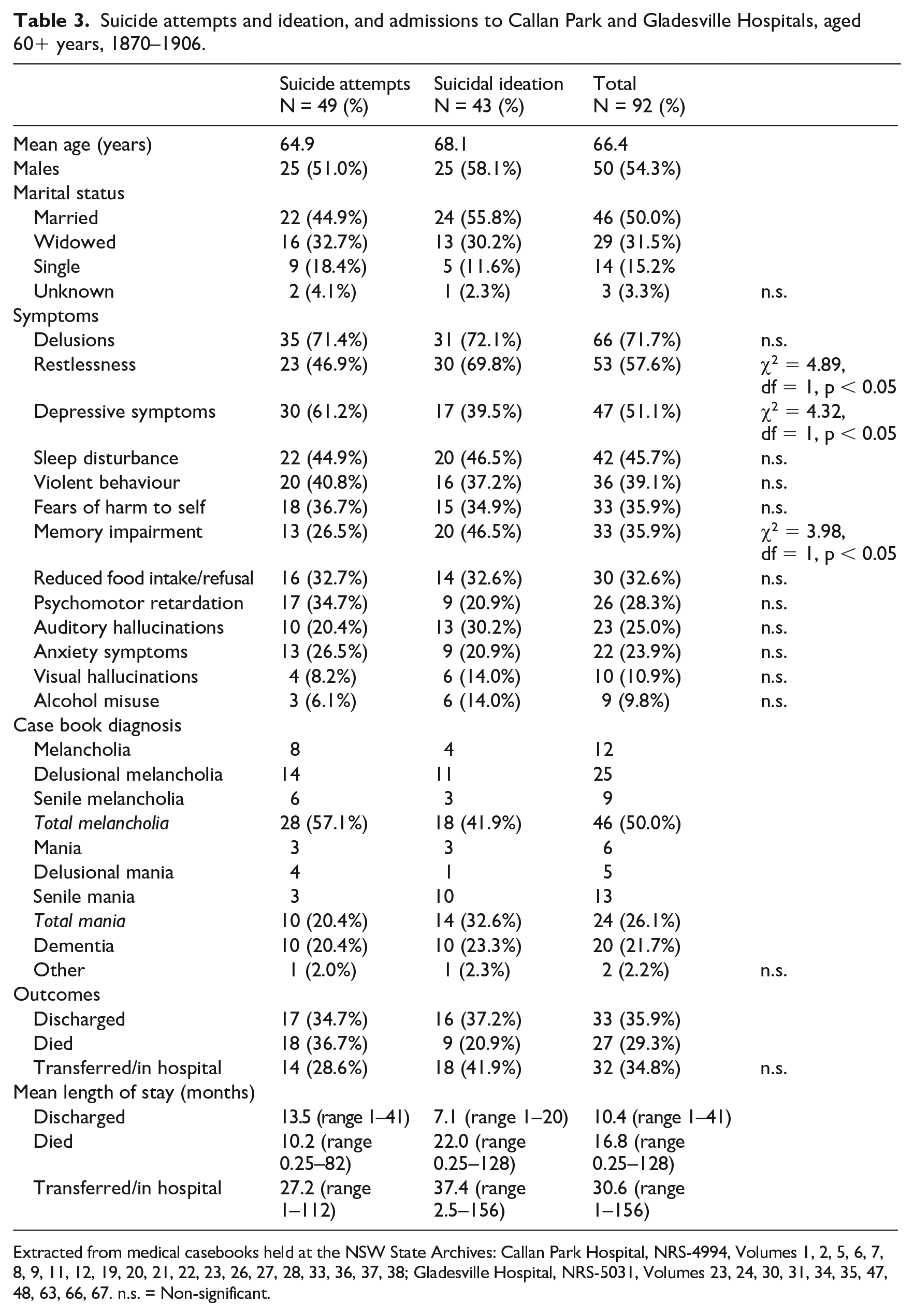
Extracted from medical casebooks held at the NSW State Archives: Callan Park Hospital, NRS-4994, Volumes 1, 2, 5, 6, 7, 8, 9, 11, 12, 19, 20, 21, 22, 23, 26, 27, 28, 33, 36, 37, 38; Gladesville Hospital, NRS-5031, Volumes 23, 24, 30, 31, 34, 35, 47, 48, 63, 66, 67. n.s. = Non-significant.
In the suicide attempts there was a significant variation in marital status, with males being more likely to be single and females to be widowed (χ2 = 18.71, df = 3, p < 0.001). Three patients who attempted suicide and one with suicidal ideation were transferred from an Asylum for the Destitute and the Aged. Four admissions from the 1870s (two with suicide attempts, two with suicidal ideation) were former transported convicts, transportation having ended in 1840 to the east coast of Australia (Barnard, 1963: 244).
Prominent symptoms and behaviours are noted in Table 3. When defining psychosis as being the presence of delusions and/or hallucinations, 37 patients with suicide attempts (75.5%) and 33 (76.7%) with suicidal ideation were psychotic. There were some significant differences in symptoms: patients who attempted suicide were more likely to have depressive symptoms and those with suicidal ideation were more likely to be restless and their memory impaired. This is largely reflected in the casebook diagnoses that had a higher proportion of melancholia diagnoses in patients with suicide attempts and mania diagnoses in those with suicidal ideation (see Table 3).
Delusional melancholia, a diagnosis largely equivalent to the modern diagnosis of major depression with psychosis, was the most frequent diagnosis made in both groups (Draper, 2021). An example was a 63-year-old single surveyor with a three-month history of being melancholy and morose, lacking in volition, with little interest in his usual activities, hypochondriacal delusions that various bodily organs were not working, and persecutory delusions about his closest relatives. In this context he made two suicide attempts by cutting his throat and a few weeks later by hanging. He remained melancholic in hospital over the next 20 months before being placed on leave for 12 months prior to discharge (ID542). Senile mania, a diagnosis without a specific modern equivalent but most frequently translating to dementia with agitation, was a prominent diagnosis in patients with suicidal ideation (Draper, 2021). One example was an 83-year-old widow who for the previous three months had been unable to take care of herself, was wandering about and walked into a creek. The medical certificate stated that she was suicidal, but without further detail. In the reception house and later in the hospital she was garrulous, restless, roaming about the ward, incoherent in speech and conduct, and required constant supervision. Over the next year her cognition and function continued to decline before her death (ID561).
Stressors precipitating the suicidal behaviour were infrequently identified in the casebook notes, with only 12 of the suicide attempters and eight with suicidal ideation having issues mentioned, which included financial concerns, death of spouse, poor health, relationship difficulties and carer stress. For the most part, the suicide attempts and ideation occurred in the context of a severe psychosis and driven by delusions or command hallucinations. For example, a married butcher in his sixties took an overdose of liniment ‘to get away from his worries’ because he believed he was ‘a great swine’ and that he was ‘not at peace with God’, as he had done the wrong thing, would not be forgiven and feared punishment at God’s hands (ID520).
The casebook notes give no indication that any special precautions were taken to reduce the risk of suicide in the hospital. There was no mention of any episodes of self-harm in the hospital ward, and none died by suicide in hospital. Four patients (three suicide attempts, one suicidal ideation) had to be force-fed with stomach pumps; two died, one with a gangrenous lung which was probably caused by the tube being inserted into the lung instead of the stomach.
The outcomes indicate that a minority were discharged. Twelve (four suicide attempts, eight with ideation) were discharged while on leave, a period included in their length of stay. Some were discharged with little evidence of improvement. For example, a 60-year-old married farmer, who had cut his throat and then tried to drown himself while in a melancholic delusional state after his daughter died, showed no significant improvement over six months but was discharged on request of his family (ID495). Transfers were mainly to other hospitals for the insane such as Parramatta and Rydalmere which specialised in long-term care. Most of these patients would have remained there until death.
Some deaths occurred in the acute phase within three months of admission, due to concurrent physical ailments such as dysentery, hospital-acquired complications such as from injuries sustained after being attacked by another patient, from complications of tube feeding, and infections such as pneumonia and influenza. Others died after long admissions, often in the context of age-related physical and cognitive decline.
According to a newspaper report pasted in the file, one 65-year-old woman with chronic persecutory delusions, who had attempted suicide by hanging and was discharged after an 18-month admission, died by suicide six years later at Parkside Hospital for the Insane in Adelaide (ID592). It is not known whether there were any other suicides in this cohort.
Discussion
This is the first examination of attempted suicide in older people during the late nineteenth and early twentieth centuries, and it has brought together information from NSW government statistics, newspaper reports, and medical case notes for those who had suicidal behaviour and were admitted to hospitals for the insane. The key findings are that a large majority of older individuals who attempted suicide were males and were dealt with in the legal system, with those admitted to hospitals for the insane invariably having severe mental illnesses, usually with psychotic features. There is also evidence that persons aged 60+ years were apprehended and convicted for attempted suicide at around twice the proportion of older people in the NSW population. Furthermore, the proportion of older convictions that were imprisoned was higher than for younger adults, albeit in many cases these were short sentences for medical attention.
Before discussing these findings there are a few limitations to note. The Statistical Registers of NSW were incomplete for the period under study and information about persons aged 60+ years was not presented in every year. Thus it is unclear whether the age-related findings were present throughout. Newspaper reports of suicide attempts had variable amounts of information, so the features compiled for the cases only represent those that were mentioned in the hearings and police reports, and what was deemed newsworthy by reporters. Thus it is most likely that these represent underestimates of the relevant issues. With the medical casebooks, the selection, extraction and interpretation of the case notes was solely the work of the present author. The quality of the case notes varied, and key information was often lacking. Some information, such as the registers for seclusion and restraint, were not available, and there were no nursing notes.
Across the age range, males were disproportionately apprehended for attempted suicide, although this gradually declined between 1870 and 1908, which may well have reflected the increasing proportion of females in the NSW population. This male predominance was more prominent in old-age cases seen in the judiciary but not in those admitted to hospitals for the insane where the proportion of females was greater than the corresponding proportion of females aged 60+ years in NSW (Australian Bureau of Statistics, 2006: Tables 21 and 22). These data contrast with the experiences in late nineteenth-century England where suicide attempts had become more common in young females, who were not necessarily trying to kill themselves (Anderson, 1989). It might well have been that in NSW persons who were obviously not trying to kill themselves were not being apprehended and prosecuted, an observation supported by the relatively low number of apprehensions throughout the period. The newspaper reports of the older people support that contention, as there were only four individuals where the self-harm was obviously without suicidal intent. It might also explain the male predominance and the higher rates of apprehensions in older people, as this would reflect the contemporary observations that suicide rates were higher in males and in late life (Knibbs, 1912). Modern research has shown that suicidal intent is more likely to occur in older people than in younger people (Draper, 2014).
As reported in the newspapers, the older people prosecuted for attempted suicide were experiencing a range of issues similar to those that have been identified in modern research. These include alcohol misuse, poor physical health, depression, insanity, being ‘tired of life’, financial problems, relationship difficulties, and loss events such as the death of a spouse (Draper, 2014). Simon Cooke, in his examination of late-life suicide in Victoria between 1841 and 1921, also found that the issues identified in the coronial inquests resonated with modern research and included physical illness, insanity, dependence on others, a need for welfare, and living alone in rural areas. There was no single stereotype of issues, but various combinations of factors (Cooke, 1995).
The peaking of newspaper reports in the 1890s coincided with the economic depression and the crisis in aged care in that period. Around two-thirds of the reported suicide attempts in the 1890s had financial problems or were unemployed. Others had chronic health problems and required assistance, but had no one to turn to. In the main, these individuals were treated compassionately by the magistrates with some being referred to an asylum for the destitute and aged, while others were imprisoned or remanded with a specific recommendation of medical treatment, or were discharged into the care of family or friends. Thus, while the criminalisation of suicidal behaviour might seem extreme from a twenty-first-century perspective, it is noteworthy that in 2021 there were still 20 countries that had laws against attempted suicide, and the impact of these laws upon rates of suicidal behaviour was unclear (Lew et al., 2022). Perhaps the key issue, as implied by the current study, is whether the judiciary uses a compassionate or punitive approach to administering the law.
Although the final outcome from the newspaper reports of the legal process was not available for all of the older individuals, at least a quarter were discharged after conviction. However, over 15% were imprisoned for a month or more. Taylor (2022) observed that there were four classes of case where mercy was not necessarily provided in the legal system: after repeat attempts, those without family or friends to support them, those who endangered others, and those who encountered a tough judge. Examples of each of these classes were apparent in the newspaper reports. The current study indicates that alcohol misuse was a fifth class of case likely to result in a heavier sentence. Perhaps a long sentence was regarded by some magistrates as a way to help the older man achieve sobriety.
The asylums for the destitute and aged were implicated as both a factor contributing to suicide attempts as well as part of the solution after the attempts. Conditions in the asylums were notoriously poor, being overcrowded, short staffed, and dilapidated in maintenance (Garton, 1990: 58). For some, the institutional routines precipitated suicide attempts, and for others it was the despondency of the miserable lifestyle that they were forced to live, without hope of improvement. Yet for some impoverished individuals in poor health, who were often homeless or living without any supports, these asylums offered a form of support after their suicide attempt, although not all of them desired that route, perhaps with good reason. Two of the 11 people placed in one of the asylums died within the next year, one by suicide in the asylum, the other in a suspicious drowning after he had discharged himself.
It was striking that none of the admissions to the hospitals for the insane recorded evidence of self-harm or suicide ideation in the continuation notes, and nor was there any evidence that special precautions were taken to address suicide risk. Further, there was no routine recording of suicide risk on admission. This is in contrast to practice and experience in England, where from the early days of the asylum system in the nineteenth century, the ‘Statement of Particulars’ at the reception house asked explicitly for every patient whether they were ‘suicidal’. Through this process, around 25% of admissions were judged to be suicidal (Shepherd and Wright, 2002). However, George Savage (1884), an asylum medical superintendent, believed that only around 5% of admissions were actively suicidal and required close watching by the attendants. Shepherd and Wright (2002) examined suicidal behaviour of inpatients at Brookwood and Buckinghamshire asylums in the period 1853–81 and found that it peaked in 50- to 59-year-olds. Management of suicidal cases often involved sedation with opium, chloral hydrate, bromide or digitalis. At the Oxford asylums Warneford and Littlemore, while the rates of suicidal ideation recorded in the continuation notes were low, there were four suicide attempts (1%) of inpatients aged 60+ years (Yorston and Haw, 2005). Presumably, inpatients of NSW hospitals for the insane were not immune from ongoing suicidal behaviour in hospital, and this may reflect poor record keeping.
Modern suicide research has shown that suicide attempts in late life are a risk factor for suicide (Draper, 2014). Three of the cases described here are known to have died by suicide and a fourth was a possible suicide. Information on the cause of death of the majority of the sample is unavailable, and so this is likely an underestimate. While the short-term risk of suicide in persons who attempted suicide was recognised in this era, it is not so clear that the medium- to long-term risk was known.
In conclusion, this examination of attempted suicide in older people has identified associated clinical and socio-demographic factors similar to those identified by current research. Most cases were dealt with in the legal system, albeit one that ensured adequate medical care was provided and that for the most part some short-term support was provided by family and friends, an asylum for the destitute and aged, a hospital for the insane, or a gaol.
Footnotes
Acknowledgements
I would like to thank the helpful staff at the NSW State Archives.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.