
Abstract
Empathy, the ability to understand the feelings of other people, is critical for navigating our social world and maintaining social connections. Given that acute stress, and resulting increased glucocorticoids, triggers a shift in two large-scale brain networks, prioritizing salience over executive control, we predicted that acute psychosocial stress would facilitate empathic accuracy. We also investigated the moderating role of gender, given that men typically show a more robust glucocorticoid response to acute stress than women. As predicted, results from two independent experiments (N = 267 college-age participants; 2,256 observations) showed that acute psychosocial stress facilitated empathic accuracy for men, an effect related to their glucocorticoid response in the stress condition. Conversely, psychosocial stress had no effect on empathic accuracy for women, who also showed a smaller cortisol response to stress than men. Exploratory analyses further revealed that women taking oral contraceptives performed worse on the empathic-accuracy task than regularly cycling women. This research highlights the important, but complex, role of stress in cognitive empathy.
Keywords
Cognitive empathy—the ability to understand the emotions of other people—is critical to navigating daily life and plays an important role in the development and maintenance of social bonds (de Waal & Preston, 2017). To date, a great deal of research has been devoted to understanding the factors that can influence cognitive empathy. One factor that has received relatively little attention is acute stress, notwithstanding its ubiquity to the human experience.
Acute stress is a momentary response to an aversive or challenging situation that results in the activation of several biological and psychological processes, aimed at restoring homeostatic balance. Whereas the human stress response is complex and multifaceted, involving the interplay between numerous biological and psychological processes, the two biological systems that are frequently investigated are (a) the fast-acting autonomic nervous system, specifically its sympathetic branch, indicated by increased heart rate and release of catecholamines, and (b) the slow-acting hypothalamic-pituitary-adrenal axis, which results in an increase of its downstream marker cortisol. Although an adaptive response, arguably, necessitates the coactivation of these systems (Ali, Nitschke, et al., 2020; Andrews et al., 2013), of particular relevance to the present investigation is the stress-induced activation of the hypothalamic-pituitary-adrenal axis, thought to have important consequences for cognition and information processing. Through a negative feedback loop, cortisol reaches the central nervous system and is thought to induce a shift in neural activation to deal with the stressor. As Hermans and colleagues (2014) argue, immediately following the stressor, resources are reallocated from the executive control network to the salience network; this reallocation of resources facilitates vigilance to contextual cues, especially cues to salient contextual information, presumably to facilitate dealing with the challenge at hand. After the immediate stressor has passed, resources are shifted back to the executive control network. Meta-analytic data support the idea that these two neural systems are modulated in a reciprocal manner following stress: Performance on attentional vigilance tasks is generally better when such tasks are administered immediately following a stressor (within ~1 hr) and declines afterward, whereas performance on executive control tasks is typically poorer when such tasks are administered immediately following a stressor but improves as the time relative to stressor onset increases (Hermans et al., 2014). To the extent that cognitive empathy relies on the salience network, we might expect acute stress to have beneficial effects on this kind of information processing.
In the present research, we investigated the effects of acute psychosocial stress on cognitive empathy, specifically empathic accuracy, that is, the ability to dynamically track the emotional state of another individual over time. Furthermore, in line with prior theory and empirical work (Hermans et al., 2014; Putman & Roelofs, 2011), we investigated the role of stress-induced glucocorticoids. To this end, we conducted two studies in which we induced acute psychosocial stress with the Trier Social Stress Test (TSST; Kirschbaum et al., 1993) and then had participants watch videos of targets discussing negative autobiographical events and rate how they thought the targets were feeling. Critically, targets themselves also rated how they were feeling, which allowed us to calculate an index of empathic accuracy (cf. Zaki et al., 2008). Because empathic accuracy relies on the ability to update one’s representations on the basis of (often) subtle changes in the target’s affect, it should be particularly sensitive to glucocorticoid-induced changes in attentional vigilance for social-emotional information (Hermans et al., 2014; Putman & Roelofs, 2011).
We also aimed to investigate whether the effects of acute stress on empathic accuracy depend on gender. To date, women are underrepresented in stress research, largely because of the (perceived) complexity in women’s biology, which makes them methodologically difficult to study (Bale, 2019; Shansky, 2019). Importantly, as Kirschbaum et al. (1999) and Kudielka et al. (2004) report, compared with men, women typically show an attenuated salivary glucocorticoid response to the TSST (an effect that seems to be linked to ovarian hormones and, in particular, elevated levels of the corticosteroid-binding globulin, which reduces the availability of free unbound cortisol; for a recent meta-analysis on the differences in cortisol secretion for men and women, see Liu et al., 2017). Evidence indicates that this attenuated cortisol response is not because women find the TSST less stressful than do men; indeed, they typically show levels of psychological distress that are as high as or higher than those of men (Ali, Nitschke, et al., 2020; Childs et al., 2010). This difference in physiological stress reactivity could have important implications for the present study: If the aforementioned stress-induced shift in cognition is, at least partly, related to unbound cortisol, and women show a more blunted cortisol response to the TSST, women may be less likely than men to show facilitatory effects of stress on empathic accuracy. Indeed, preliminary evidence supports gender-moderated effects: Smeets and colleagues (2009) found that men who showed a high (vs. low; median split) glucocorticoid response to the TSST performed better on the Movie for the Assessment of Social Cognition (MASC), whereas women showed the opposite pattern. The MASC, however, assesses mentalizing more broadly, and does not target the kind of negative social-emotional information that is typically conveyed in empathy-inducing situations (e.g., sadness, anger), leaving this an open question.
Statement of Relevance
Stress is an inescapable fact of the human experience. Prior research has shown that acute stress can undermine our cognitive abilities, especially those involving executive functioning such as decision-making, problem solving, and goal-directed behavior. Less, however, is known about how acute stress influences social information processing. Indeed, research indicates that humans process social information differently from nonsocial information. Here, we examined the effect of acute psychosocial stress on cognitive empathy, that is, the ability to accurately track, over time, other people’s emotions. Results from two experiments showed that acute stress significantly improved performance on the cognitive-empathy task for men but had no effects for women. Moreover, the beneficial effects of stress, for men, were related to their cortisol response to the stress task. Finally, we also found that women taking oral contraceptives performed more poorly on the cognitive-empathy task than did regularly cycling women. This research highlights the important, but complex, role of stress in cognitive empathy and the importance of considering gender-specific effects.
Finally, we also took this opportunity to explore the role of women’s oral contraceptive use. Women taking oral contraceptives can show an even more blunted stress-induced cortisol response than regularly cycling women because of the higher availability of corticosteroid-binding globulin caused by exogenous estrogen administration (Kirschbaum et al., 1995). Very little is known about whether women taking oral contraceptives show different effects of stress on empathic accuracy. This is an important knowledge gap given the number of women taking oral hormonal contraceptives (i.e., approximately 14% of women ages 15–49 years in the United States and 28% in Canada; United Nations, 2019).
Experiment 1 (Between Subjects)
Method
In Experiment 1, we randomly assigned each participant to the TSST or control condition; participants then completed the empathic-accuracy task and tasks assessing other research questions (Nitschke & Bartz, 2020). To account for diurnal cortisol fluctuations (Goodman et al., 2017), we conducted testing sessions between 9:00 a.m. and 2:00 p.m. (see Fig. 1 for timeline). Cortisol (and other stress markers, i.e., salivary alpha amylase [sAA] and subjective distress) was assessed throughout the testing session (see below).
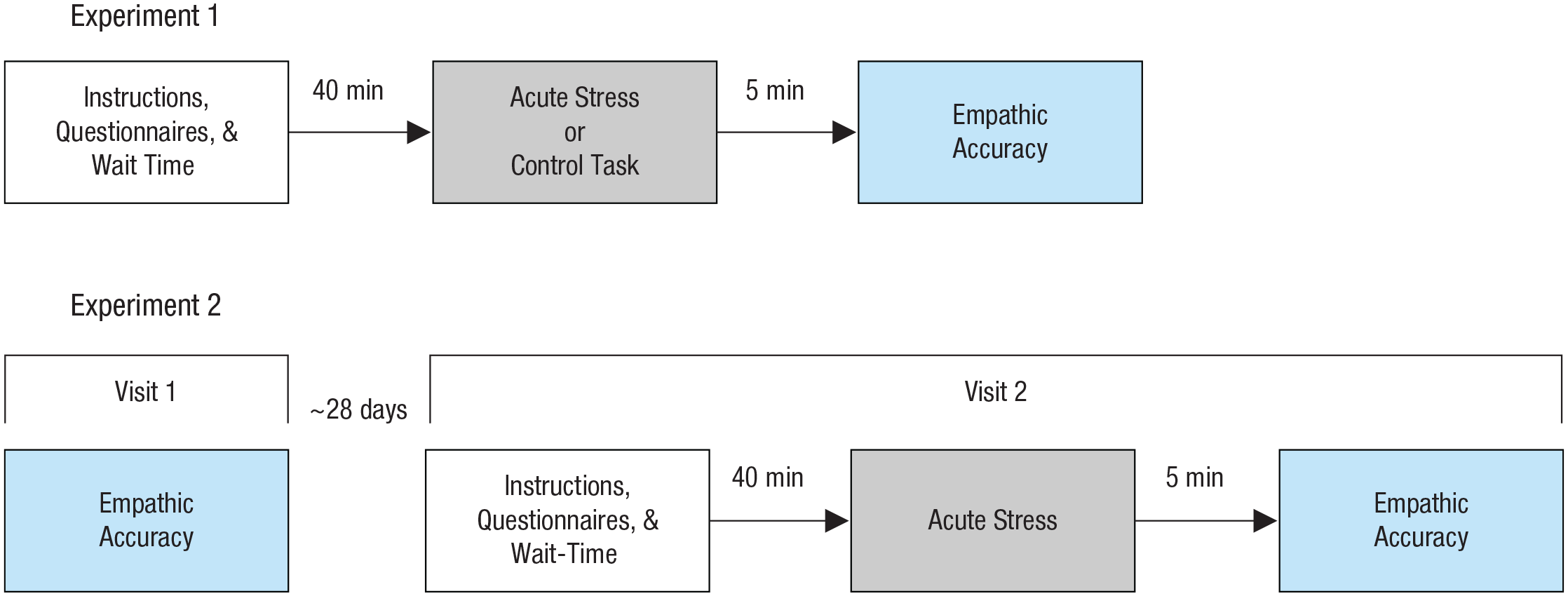
Study design for both experiments. Experiment 1 used a between-subjects design; each participant was randomly assigned to either an acute-stress paradigm or a control condition before completing the empathic-accuracy task. Experiment 2 used a within-subjects design; participants came to the lab on two separate occasions, separated by an approximately 28-day delay (or based on the menstrual cycle). During Visit 2, all participants completed a stress task before doing the same empathic-accuracy task as in Experiment 1.
Sample
To determine sample size, we referred to Smeets et al. (2009); on the basis of that study, we estimated that we would need a minimum of 26 participants per cell to detect a comparable effect ( f = 0.25, 1 – β = 80%; for detailed information, see the supplemental online material [SOM] available at https://osf.io/9h3pw/). Thus, we recruited 158 participants from classified ads and online advertisements; specifically, we recruited men, regularly cycling women, and women taking oral contraceptives. To reduce variance associated with cyclical changes in estrogen, we asked regularly cycling women to come during the luteal phase of their menstrual cycle (for details, see the SOM). Because of computer malfunction, there were no empathic-accuracy data for two female participants (one TSST, one control), and a third (female) participant opted out of the study following the TSST. Thus, the final sample consisted of 61 men (age: M = 22.4 years, SD = 3.43) and 97 women (age: M = 22.1 years, SD = 3.42; 48 regularly cycling and 49 taking oral contraceptives). There were 78 participants in the TSST condition (30 men, 23 regularly cycling women, and 25 women taking oral contraceptives) and 80 participants in the control condition (31 men, 25 regularly cycling women, and 24 women taking oral contraceptives; see SOM for participant demographics, see the SOM at https://osf.io/9h3pw/). Each session lasted 2 hr. Participants were instructed to refrain from consuming food as well as sugared or caffeinated beverages for 2 hr prior to their visit. The research was approved by the McGill University Research Ethics Board and conducted in accordance with the Declaration of Helsinki. Participants were compensated for their time and effort.
Measures
Empathic-accuracy task
In the empathic-accuracy task (Zaki et al., 2008), participants watched short (~2 min) videos of individuals (“targets”) discussing autobiographical events. For the present study, we used videos in which targets expressed negative emotions such as grief, sadness, apathy, and helplessness (topics included, e.g., losing one’s job, death of parents, rejection). Each participant watched six videos; to ensure that any effects that we observed were not due to the idiosyncratic nature of particular videos, we randomly assigned each participant to watch one of two video sets, with an equal number of male and female targets. Participants were asked to rate, throughout the video, how they thought the target was feeling using a 9-point Likert-type scale ranging from very negative to very positive. Following Zaki et al. (2008), ratings were unprompted, meaning that we left it up to participants to change their ratings when they perceived changes in the target’s affect (note that to ensure enough responses for data analyses, we asked participants to update their ratings every few seconds, even if they did not want to change their actual rating). Importantly, the targets also provided similar ratings of how they felt while discussing the events, on the same 9-point Likert-type scale. Empathic accuracy was operationalized as the correlation between the ratings made by perceivers and targets; specifically, following Zaki et al., we z-scaled ratings within participants (to account for individual differences). Ratings were binned for every 2 s and subsequently correlated with the target’s ratings to index empathic accuracy (r scores).
Trier Social Stress Test
In the TSST (Kirschbaum et al., 1993), participants deliver a mock job interview in which they present their qualifications to two “behavioral experts” (research confederates who, critically, are instructed to give no verbal or nonverbal feedback) and then perform a verbal arithmetic task in front of the judges. The TSST has been shown to reliably induce a stress response as indicated by cortisol (Goodman et al., 2017), sympathetic nervous system activation (Rohleder et al., 2004), and subjective stress measures (Ali et al., 2017). For participants in the control condition, we used the placebo TSST (Het et al., 2009), in which participants talk about a recent life event for 5 min and then count upward in 15-step increments in an empty room.
Stress markers
Throughout the testing session (see Fig. 1), we took saliva samples (i.e., Salivette; Sarstedt AG, Nümbrecht, Germany) in 10-min intervals (prior to stress [−10 min], 0, +10, +20, +30, +40, and +50) to assess cortisol; at these time points, we also measured sAA (a marker of sympathetic activation; Ali & Nater, 2020) and subjective stress using a visual analogue scale (i.e., “How stressed do you feel?”). Cortisol levels (nmol/l) were assessed using a time-resolved fluorescence immunoassay (Dressendörfer et al., 1992), and sAA levels (U/ml) were determined using the enzyme kinetic method (Engert et al., 2011) in this experiment and Experiment 2. As noted, our primary analyses concerned the main effect of our stress manipulation and cortisol given the aforementioned theoretical and empirical work highlighting the role of stress-induced cortisol in cognition; however, we also conducted parallel exploratory analyses with sAA and subjective distress. We summarize any findings from these exploratory analyses in the main text and provide a complete description in the SOM for interested readers (see https://osf.io/9h3pw/).
Analytic approach
We first sought to confirm successful stress manipulation. We conducted a repeated measures mixed-effects model (MEM; Gueorguieva & Krystal, 2004) to test for differences in stress responsivity (cortisol levels at each measurement time point) between the stress and control conditions. Condition (0 = control, 1 = stress), gender (men, regularly cycling women, and women taking oral contraceptives; see below), and sampling time were included as predictors, as well as all two-way interactions and the three-way Condition × Gender × Sampling Time interaction. Time was nested within participant ID as a random factor (see Note 1 in the SOM at https://osf.io/9h3pw/).
To test our main hypothesis—the effect of acute psychosocial stress on empathic accuracy—we ran a MEM (Holmes Finch et al., 2014) with empathic-accuracy scores as the dependent variable and the fixed factors of condition (0 = control, 1 = stress) and gender (men, regularly cycling women, and women taking oral contraceptives; see below); we also included the Condition × Gender interaction term to test for differential effects of stress on empathic accuracy for men, regularly cycling women, and women taking oral contraceptives. Akaike information criteria were used to test whether the inclusion of the interaction term resulted in a more parsimonious model fit (i.e., variance explained vs. model complexity; see the SOM at https://osf.io/9h3pw/; Cohen et al., 2003). Finally, we included two random factors, participant ID and video ID, in our model. For this and all subsequent analyses, the planned contrasts (Helmert coding) for the gender variable were defined as follows: Contrast 1, testing men versus all women (men = 1, regularly cycling women = −0.5, women taking oral contraceptives = −0.5), and Contrast 2, testing regularly cycling women versus women taking oral contraceptives (men = 0 [excluded], regularly cycling women = 1, women taking oral contraceptives = −1). Finally, we included a covariate to account for video sets in this and subsequent models.
As noted, in addition to the overall effect of our stress manipulation, we theorized that the effect of stress on empathic accuracy is, at least partly, related to stress-induced glucocorticoids. To test this, we first calculated areas under the curve (AUCs) for cortisol (i.e., changes from prestress levels until immediately after the empathic-accuracy task) using the formula described by Pruessner et al. (2003). We then conducted MEMs, as described above, but in addition included cortisol AUC (z transformed) as a fixed effect as well as the Condition × Cortisol interaction (i.e., to test the combined effect of acute stress and cortisol reactivity). 1 Of note, it has previously been reported (Nitschke et al., 2019; Smeets et al., 2009) that cortisol may have a nonlinear association with (social) cognitive abilities; thus, in an exploratory step, we included a second-degree polynomial effect of cortisol.
All confidence intervals (CIs) were bootstrapped. All statistical analyses were conducted in the R programming environment (Version 3.6.3; R Core Team, 2020) as well as the lme4 (Bates et al., 2015) and lmerTest (Kuznetsova et al., 2017) packages for MEMs. Significant interaction effects from the MEMs were decomposed using the emmeans package (Lenth et al., 2018). 2
Results
Manipulation check for stress induction: cortisol
The repeated measures MEM testing the effect of stress on cortisol revealed a significant Condition × Gender × Sampling Time interaction, F(12, 584.6) = 4.499, p < .001. Results showed significantly higher cortisol levels in the stress versus control conditions and, thus, successful stress induction; moreover, consistent with prior work (Kudielka et al., 2004), results showed that men had a higher cortisol response than women (Contrast 1) at Time Points 3, 4, 5, 6, and 7 (all ps < .05; for details and a depiction of the cortisol response, see the SOM at https://osf.io/9h3pw/). Finally, there were no cortisol differences between regularly cycling and women taking oral contraceptives (Contrast 2) at any time point. Finally, results also showed a significant effect of stress on sAA but no gender-specific effects, further supporting successful stress induction (see the SOM). Of note, parallel analyses investigating subjective distress showed significant effects for both men and women, which confirms that women were, indeed, stressed by the TSST even though they showed a more blunted cortisol response (see the SOM).
Effect of stress induction on empathic accuracy
The MEM predicting empathic accuracy with condition and gender and their interaction as fixed factors, and participant ID and video ID as random effects, revealed a significant Condition × Gender interaction effect for Contrast 1 (men vs. women), b = 0.052, 95% CI = [0.003, 0.097], t(156.12) = 2.184, p = .030. Specifically, men in the stress condition had significantly higher empathic-accuracy scores than men in the control condition, b = 0.063, 95% CI = [0.006, 0.119], z = 2.195, p = .028. By contrast, there was no difference in empathic-accuracy performance between women in the stress condition and women in the control condition, b = 0.015, 95% CI = [−0.029, 0.059], z = −0.661, p = .51. Results also showed that, in the stress condition, men had significantly higher empathic-accuracy scores than women, b = −0.073, 95% CI = [−0.023, −0.124], z = 2.867, p = .004. Finally, there was no difference in empathic-accuracy performance between women and men in the control condition, b = 0.004, 95% CI = [−0.046, 0.054], z = −0.153, p = .878 (see Fig. 2; for a summary of the model, see Table S1 in the SOM at https://osf.io/9h3pw/).
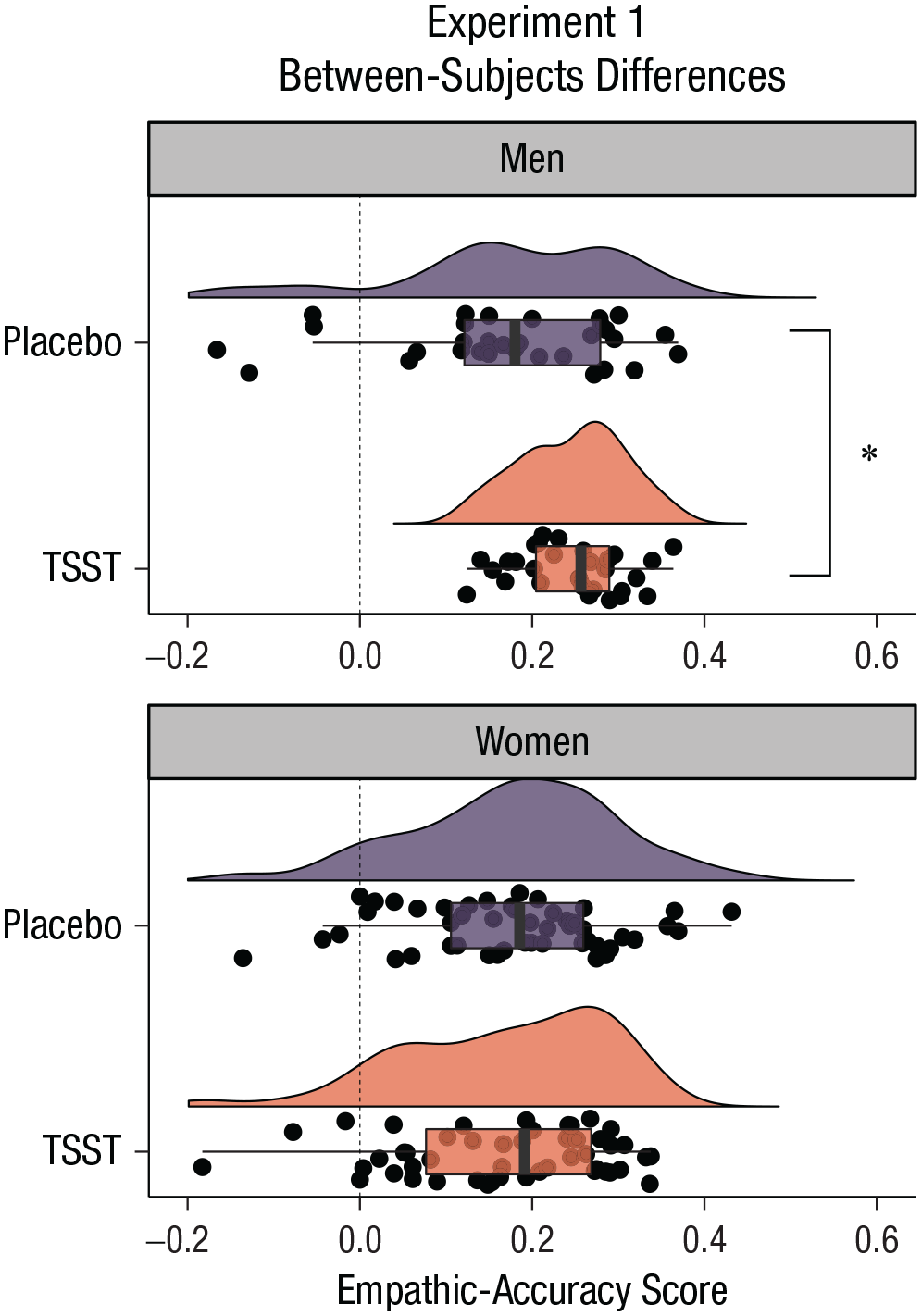
Experiment 1: effects of acute psychosocial stress on empathic accuracy in the control and the Trier Social Stress Test (TSST) groups, separately for men and women. Dots represent mean participant responses, and shaded regions indicate the density of the data. Boxes represent the first and third quartiles of the data, solid lines indicate group means, and whiskers mark 1.5 times the interquartile range. The asterisk indicates a significant difference between conditions (p < .05).
Regarding Contrast 2 (comparing regularly cycling women with women taking oral contraceptives), results showed no significant interaction, b = −0.032, 95% CI = [−0.07, 0.009], t(156.12) = −1.456, p = .147; however, there was a significant conditional effect for Contrast 2, b = 0.033, 95% CI = [0.005, 0.065], t(156.12) = 2.153, p = .033, indicating that women taking oral contraceptives performed worse on the empathic-accuracy task than regularly cycling women across the control and stress conditions (see Tables 1 and 2).
Mean Empathic-Accuracy Scores for Men and Women
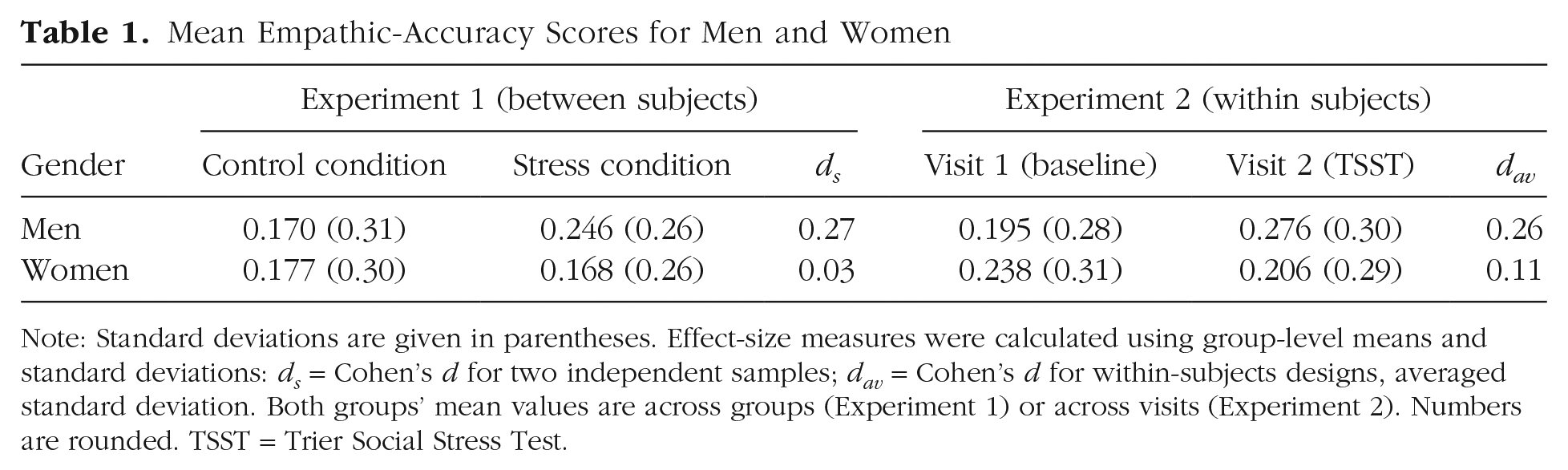
Note: Standard deviations are given in parentheses. Effect-size measures were calculated using group-level means and standard deviations: ds = Cohen’s d for two independent samples; dav = Cohen’s d for within-subjects designs, averaged standard deviation. Both groups’ mean values are across groups (Experiment 1) or across visits (Experiment 2). Numbers are rounded. TSST = Trier Social Stress Test.
Mean Empathic-Accuracy Scores for Regularly Cycling Women and Women Taking Oral Contraceptives
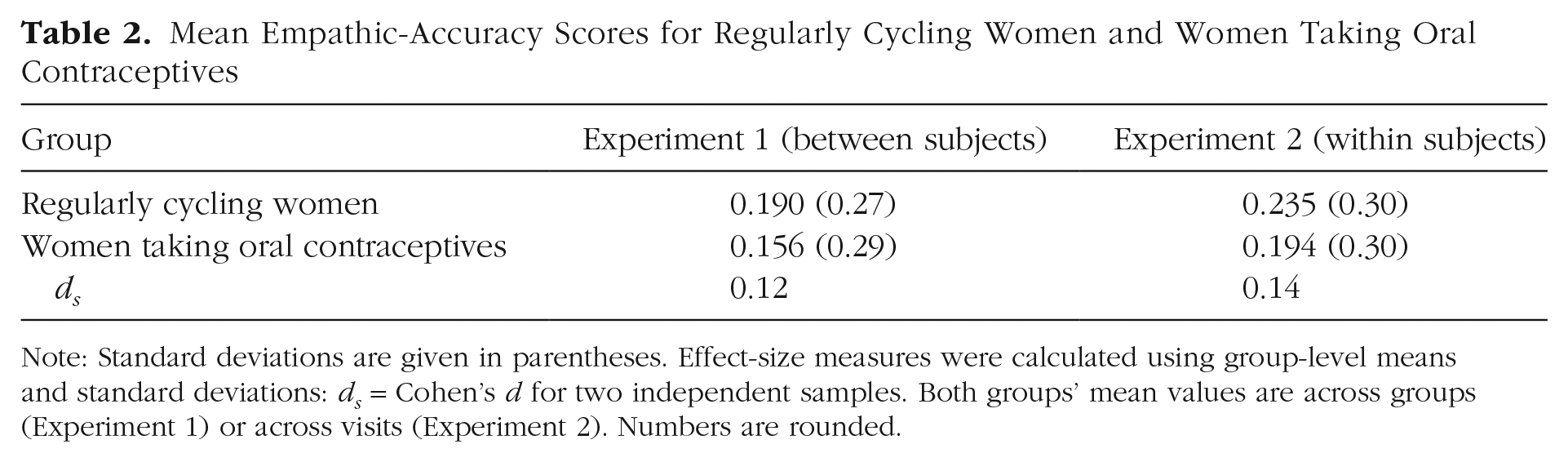
Note: Standard deviations are given in parentheses. Effect-size measures were calculated using group-level means and standard deviations: ds = Cohen’s d for two independent samples. Both groups’ mean values are across groups (Experiment 1) or across visits (Experiment 2). Numbers are rounded.
Effect of cortisol on empathic accuracy
We next investigated the effects of cortisol (AUC, z transformed) on empathic accuracy. Because the previous analyses indicated a differential effect of stress on empathic accuracy for men and women, and a significant difference in cortisol response to the TSST for men and women, we ran separate models for men and women (we combined the regularly cycling and women taking oral contraceptives given that our main analyses showed no differential effects of stress for these two groups). Note that if we run the model combining men and women, the Condition × Gender × Cortisol interaction is also significant (see the SOM at https://osf.io/9h3pw/). The MEM for men showed a significant interaction between condition and cortisol on empathic accuracy, b = 0.068, 95% CI = [0.012, 0.126], t(56.00) = 2.270, p = .027; as predicted, for men in the stress condition, cortisol was positively associated with empathic accuracy (b = 0.034, 95% CI = [0.004, 0.065], z = 2.267, p = .023), whereas for men in the control condition, there was no association between cortisol and empathic accuracy (b = −0.033, 95% CI = [−0.085, 0.018], z = −1.298, p = .194). The MEM for women did not result in a significant slope, b = −0.015, 95% CI = [−0.061, 0.033], t(92.99) = −0.647, p = .519, indicating no association between cortisol and empathic accuracy. Finally, the inclusion of a polynomial cortisol effect did not show any significant result, suggesting that the association between cortisol and empathic accuracy is linear. Regarding our exploratory analyses, there was no significant interaction or conditional marginal effect of sAA on empathic accuracy for either men or women, nor was there a significant interaction or conditional marginal effect of subjective distress on empathic accuracy for men or women (see the SOM at https://osf.io/9h3pw/).
In sum, we show that acute psychosocial stress improves empathic-accuracy performance for men but has no effect on empathic accuracy for women. This finding does not appear to be due to ceiling effects on the empathic-accuracy task for women—our results show no gender difference in the control condition; rather, men’s performance improves in the stress condition. Additional analyses reveal that the effects of stress on empathic accuracy for men are, at least partly, dependent on their enhanced cortisol response. That is, men who showed a more robust cortisol response to the TSST also showed greater improvements on the empathic-accuracy task. These findings are consistent with the notion that acute stress-induced glucocorticoids facilitate attentional vigilance (Hermans et al., 2014; Putman & Roelofs, 2011). Finally, intriguingly, we found that women taking oral contraceptives performed significantly worse than regularly cycling women on the empathic-accuracy task, regardless of stress condition, suggesting a potential link between exogenous estrogen administration and cognitive empathy.
Experiment 2 (Within Subjects)
Method
In Experiment 2, we aimed to replicate the findings from Experiment 1. Although some prior work led us to expect that gender might moderate the effect of stress on empathic accuracy, these findings warrant replication. Moreover, in Experiment 1, we used a between-subjects design; however, this design is vulnerable to the influence of individual differences (e.g., in stress reactivity, endogenous hormones, and/or empathic-accuracy performance). Thus, in Experiment 2, we used a within-subjects design to control for these sources of influence. During the first visit (Visit 1), participants completed the empathic-accuracy task in the absence of stress as well as other tasks and questionnaires reported elsewhere (Nitschke & Bartz, 2020; Nitschke et al., 2020). Participants returned to the lab approximately 3 to 4 weeks later (or according to the menstrual cycle; see the SOM at https://osf.io/9h3pw/) for Visit 2; they first completed the TSST and, immediately after (same duration as in Experiment 1), completed the empathic-accuracy task (see Fig. 1 for timeline). Again, cortisol, sAA, and subjective distress were assessed throughout the testing session (see below). As in Experiment 1, all sessions were conducted between 9:00 a.m. and 2:00 p.m. The research was approved by the McGill University Research Ethics Board and conducted in accordance with the Declaration of Helsinki.
Sample
We recruited men, regularly cycling women, and women taking oral contraceptives (see the SOM at https://osf.io/9h3pw/) and applied the same inclusion and exclusion criteria as for Experiment 1. Sample-size determinations were based on those used for Experiment 1 (~26 participants per cell). We recruited 119 participants; however, 10 female participants did not return for Visit 2, so the final sample consisted of 109 participants (men = 30; women = 79: 54 regularly cycling, 25 taking oral contraceptives). Participants were compensated $10 per hour for their time ($10 + $20).
Measures
Empathic-accuracy task
We used the same empathic-accuracy task, with the same videos, described in Experiment 1. To avoid practice effects, we had participants watch, in random order, different videos on Visit 1 and Visit 2 (again, we included a variable to account for differences between video sets in our statistical analyses).
Trier Social Stress Test
We again used the TSST to elicit a stress response during Visit 2 and followed the same stress marker protocol; all measures (cortisol, sAA, and subjective stress) were taken at seven time points throughout Visit 2, starting 20 min before the stress induction, prior to stress (−10), and following stress at 0, +10, +25, +40, and +50. Again, we summarize the main findings from these exploratory analyses in the main text (for a detailed description, see the SOM at https://osf.io/9h3pw/).
Analytic approach
We followed the same analytic plan as in Experiment 1, adjusting for the within-subjects design. We first ran a repeated measures MEM (Gueorguieva & Krystal, 2004) to test the effects of acute stress induction on cortisol levels for Visit 2 (stress day); we included gender (same coding as Experiment 1), sampling time, and the interaction between gender and sampling time as fixed effects. Time was nested within participant ID as a random factor.
Next, we ran a MEM predicting empathic accuracy. Visit (0 = Visit 1, 1 = Visit 2) and gender (men, regularly cycling women, and women taking oral contraceptives) were entered as fixed factors. We included an interaction between visit and gender to test for differential effects for men, regularly cycling women, and women taking oral contraceptives. Participant ID and video ID were entered as random factors. Visit was nested within participant ID.
Finally, as in Experiment 1, we followed up these analyses with MEM analyses that also included cortisol AUC (z transformed) as an independent variable. Note that these analyses are restricted to Visit 2 because we did not measure cortisol on Visit 1; thus, whereas in Experiment 1, we predicted that condition would moderate the effect of cortisol on empathic accuracy (i.e., the magnitude of the glucocorticoid response in the stress condition would be associated with better performance on the empathic-accuracy task), in Experiment 2, we predicted a main effect of cortisol on empathic accuracy at Visit 2 (i.e., a stronger cortisol response to the TSST would be associated with better performance on the empathic-accuracy task).
Results
Manipulation check for stress induction: cortisol (Visit 2 only)
The repeated measures MEM testing the effect of stress induction at Visit 2 on cortisol levels revealed a significant interaction between gender and sampling time, F(12, 373.09) = 2.474, p = .004, indicating that gender moderated the effect of the stress induction on cortisol; specifically, consistent with prior work and as observed in Experiment 1, men had a higher cortisol response compared with women (Contrast 1) at Time Points 3, 4, 5, and 6 (all ps < .05; see the SOM at https://osf.io/9h3pw/). We did not observe cortisol differences between regularly cycling and women taking oral contraceptives (Contrast 2) at any time point (for plotted cortisol curves, see the SOM). Again, as in Experiment 1, additional analyses on subjective distress indicate that women were, indeed, stressed by the TSST even though they did not show a strong cortisol response (see the SOM). We found a significant stress-induced increase in sAA, similar to that in Experiment 1 (see the SOM).
Effect of stress induction on empathic accuracy
The MEM with empathic accuracy as a dependent variable and visit, gender, and the Visit × Gender interaction entered as fixed factors revealed a significant Visit × Gender interaction for Contrast 1 (men vs. women), b = 0.047, 95% CI = [0.007, 0.083], t(108.13) = 2.467, p = .015. As in Experiment 1, men showed a significant increase in empathic-accuracy performance from Visit 1 to Visit 2 (stress induction visit), b = 0.060, 95% CI = [0.013, 0.108], z = 2.516, p = .012. By contrast, for women, there was no difference in empathic-accuracy performance from Visit 1 to Visit 2, b = −0.01, 95% CI = [−0.039, 0.020], z = −0.64, p = .523. Results also showed that men had significantly higher empathic-accuracy scores than women during Visit 2, b = 0.064, 95% CI = [0.012, 0.116], z = 2.418, p = .016. Finally, there was no difference in empathic-accuracy performance between men and women at Visit 1 (baseline), b = −0.01, 95% CI = [−0.041, 0.054], z = −0.266, p = .791 (see Fig. 3; see also Table S2 in the SOM at https://osf.io/9h3pw/).
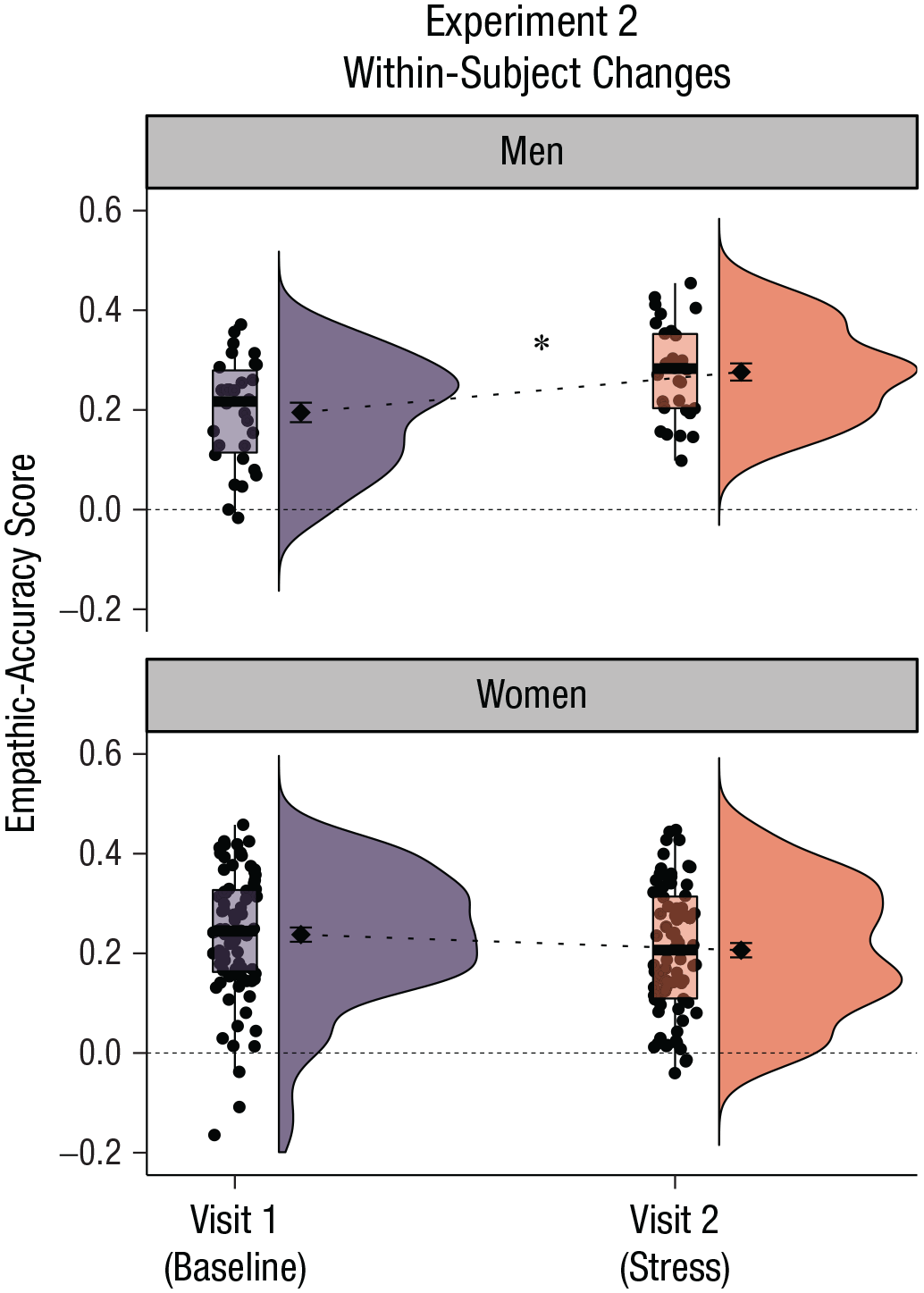
Experiment 2: effects of acute psychosocial stress on empathic accuracy at Visit 1 and Visit 2, separately for men and women. During Visit 1, participants completed the empathic-accuracy task in the absence of stress; during Visit 2, all participants completed the Trier Social Stress Test before redoing the empathic-accuracy task (with different videos; counterbalanced). Dots represent mean participant responses, and shaded regions indicate the density of the data. Boxes represent the first and third quartiles of the data, solid lines indicate group means, and whiskers mark 1.5 times the interquartile range. The asterisk indicates a significant difference between visits (p < .05).
The interaction for Contrast 2 (regularly cycling women vs. women taking oral contraceptives) was not significant, b = −0.015, 95% CI = [−0.044, 0.015], t(108.03) = −0.970, p = .334. However, as in Experiment 1, we observed a significant conditional effect for Contrast 2, b = 0.029, 95% CI = [0.004, 0.056], t(108.34) = 2.252, p = .026, indicating that, again, women taking oral contraceptives performed worse on the empathic-accuracy task than regularly cycling women across both visits (see Tables 1 and 2).
Effect of cortisol on empathic accuracy
We then assessed the impact of stress-induced cortisol (AUC with respect to increase) on empathic accuracy during Visit 2. Again, because the previous analyses indicated a differential effect of visit (i.e., stress) on empathic accuracy for men and women and a significant difference in cortisol response for men and women, we ran separate models for male and female participants. As predicted, and replicating the findings from Experiment 1, the MEM for men showed a significant effect of cortisol on empathic accuracy, b = 0.046, 95% CI = [0.013, 0.083], t(27.28) = 2.501, p = .019, whereas the MEM for women did not show a significant association (although the pattern was in the same direction), b = 0.024, 95% CI = [−0.003, 0.050], t(77.24) = 1.758, p = .083. The inclusion of this curvilinear effect did not result in a significant predictor for either men or women, indicating a linear relationship between cortisol and empathic accuracy for men. As in Experiment 1, there were no effects of sAA or subjective distress on empathic accuracy for either men or women (see the SOM at https://osf.io/9h3pw/).
In sum, in Experiment 2, we replicated several key findings from Experiment 1. Specifically, acute stress improved empathic accuracy for men but had no effect on empathic accuracy for women (either regularly cycling or taking oral contraceptives). Again, it was not that women performed better overall; there was no difference in empathic accuracy between men and women at Visit 1 (the baseline testing day). Rather, men showed selective gains in empathic accuracy following the stress induction. We also replicated the finding from Experiment 1 that women showed a more blunted cortisol response to the TSST compared with men and that the effect of stress on empathic accuracy, for men, was related to the magnitude of the stress-induced cortisol response. Finally, we replicated the intriguing oral contraceptives effect observed in Experiment 1: women taking oral contraceptives performed worse on the empathic-accuracy task, in general, than did regular cycling women. 3
Discussion
In two independent experiments, we show that, for men, acute psychosocial stress improves empathic accuracy, that is, the ability to accurately track another individual’s emotional experience over time. Moreover, results show that men’s empathic-accuracy performance following stress was related to the magnitude of the stress-induced cortisol response. In contrast to men, stress had no effect on empathic accuracy for women (an observation that underscores the importance of including women in stress research). This was not because women were better at the empathic-accuracy task because there was no difference between men’s and women’s empathic-accuracy performance in the control condition (Experiment 1) or at baseline (Experiment 2; note that other research using the task described here similarly has not reported gender differences in empathic accuracy; Bartz et al., 2019; Zaki et al., 2008, 2009).
These findings are consistent with recent accounts suggesting that acute stress triggers a phasic shift in two large-scale neural networks, prioritizing the salience over the executive control network, at least immediately following the stressor (Hermans et al., 2014). If stress facilitates vigilance to salient contextual cues, then one would expect enhanced attention to, and processing of, the emotional experiences conveyed by our empathic-accuracy targets. Importantly, our analyses showed that it was stress-induced cortisol, not cortisol in general, that facilitated empathic accuracy (i.e., there was no effect of cortisol in the no-stress condition). This is consistent with the hypothesized role of glucocorticoids in the stress-induced shift in information processing and with prior empirical work (Smeets et al., 2009). Indeed, the lack of an effect of acute stress on empathic accuracy in women may be, at least partly, due to the fact that women did not mount a strong cortisol response to the TSST (even though they reported high levels of psychological distress). In both Experiments 1 and 2, men showed a stronger cortisol response to the TSST compared with women, and the effect of stress on empathic accuracy, in men, was related to stress-induced cortisol. If the rebalancing of the salience and executive networks following acute stress is driven by stress-induced changes in neurotransmitters and hormones (Hermans et al., 2014), then the absence of a strong cortisol response in women may explain the lack of an effect—indeed, the association between cortisol and empathic accuracy for women was positive and, in fact, fell just below our statistical significance threshold in Experiment 2 (see the SOM at https://osf.io/9h3pw/).
Of note, we did not find an association between TSST-induced changes in subjective stress and empathic accuracy (nor did we find an association between sAA and empathic accuracy). As outlined before, the human stress response involves multiple signals (e.g., changes in cortisol, sAA, and subjective stress, as measured here, as well as changes in heart rate variability and even neural activity) that each interact in complex ways to produce functionally nuanced outputs (Ali, Cooperman, et al., 2020; Hermans et al., 2011; Kukolja et al., 2008). Moreover, these signals are often dissociated (e.g., cortisol and subjective distress are often unrelated and may even function to compensate for one another; Ali et al., 2017; Ali, Nitschke, et al., 2020). Whereas the lack of an effect of subjective stress may have been due to measurement (i.e., use of single item self-report measure), it suggests that the effect of our stress manipulation on empathic accuracy was not due to feelings of increased threat in response to the TSST. Indeed, this is further supported by the fact that women—who reported higher levels of subjective stress—did not show improvements in empathic accuracy.
We believe that our findings are consistent with Hermans et al.’s (2014) theory with respect to stress-induced shifts in information processing (above). An alternative, but not necessarily mutually exclusive, hypothesis is that acute stress increases motivation. Although recent research has linked stress to cognitive effort avoidance (Bogdanov et al., 2021), it still may augment task engagement more broadly. In this scenario, stress, as indexed by cortisol, may reflect a “challenge” orientation (Dickerson & Kemeny, 2004). Relatedly, it is possible that those highly motivated or challenged participants were trying harder to read the judges’ faces during the psychosocial stress task, which resulted in a face-reading priming effect that was carried over to the empathic-accuracy task. Future research is needed to probe the mechanism by which acute stress and, specifically, cortisol influence empathic accuracy. For example, using an empathic-accuracy task that includes narratives about positive experiences would allow us to address whether the effects observed here are restricted to threat-based processing or social information processing in general (cf. the face-reading priming effect alluded to above). Future research could also use other manipulations to induce stress that do not involve a psychosocial evaluative component to disentangle physiological “stress” from social processes (such as threat perception or social evaluation).
Finally, in addition to providing evidence for our primary aim regarding the effects of stress on empathic accuracy, we also observed, in our exploratory analyses, that women taking oral contraceptives performed worse on the empathic-accuracy task than did regularly cycling women (regardless of stress), an effect that was replicated in Experiment 2. Evidence regarding oral contraceptive use and social cognition is mixed (Montoya & Bos, 2017); some studies have shown an effect (Hamstra et al., 2014), but others have not (Radke & Derntl, 2016; Shirazi et al., 2020). Our findings are consistent with the former. Interestingly, Hamstra and colleagues (2014) found that hormonal contraceptive use impaired emotion recognition abilities particularly for negatively valenced emotions (cf. Pahnke et al., 2019); this is noteworthy given that our task involved negative experiences. Thus, valence may be an important factor to consider in future research. Future research should also include women outside the restricted range of the current sample (i.e., college-age individuals) and especially women going through naturally occurring hormonal transitions.
In sum, the ability to understand the emotional states of other people is a cornerstone of human social-emotional experience. Our findings show that acute psychosocial stress and, specifically, the stress hormone cortisol facilitate empathic accuracy for men, but they have no effect on empathic accuracy for women. This research adds to the growing body of literature showing that cognitive empathy is not only influenced by our psychology but also tied to our biology.
Footnotes
Acknowledgements
We thank all students who assisted with data collection and especially Cecile Sunahara and Emma Galarneau for their considerable work. We also thank Haran Sened for help with processing the empathic-accuracy data.
Transparency
Action Editor: Daniela Schiller
Editor: Patricia J. Bauer
Author Contributions
J. P. Nitschke, J. C. Pruessner, and J. A. Bartz developed the study concept, and J. P. Nitschke and J. A. Bartz developed the study design. J. P. Nitschke oversaw and assisted with the data collection and conducted the data processing and data analyses under the supervision of J. A. Bartz. J. P. Nitschke drafted the manuscript with the help of J. A. Bartz; J. C. Pruessner provided critical revisions. All the authors approved the final manuscript for submission.