
Abstract
Sexual violence (SV) has significant impacts on physical, social and psychological wellbeing, with associated mental illness and suicide. Despite no specific guidelines regarding mental health and SV, recommendations suggest all patients should have the opportunity to discuss their mental health and be offered referrals for support. A service evaluation was performed at a large Sexual and Reproductive Health Service (SRHS) with n = 179 patient records reviewed between 30/07/2021 to 01/10/21, who had disclosed SV including n = 83 referred from Sexual Assault Referral Centres (SARC). Patient exclusions included duplicates and non-attendances. Data on patient demographics, mental health assessment and referral services were analysed. Referral services included Independent Sexual Violence Advisors (ISVAs), a specialist third sector organisation Rape and Sexual Violence Project (RSVP), and an inhouse specialist SV clinic, Abuse Survivors Clinic (ASC). Demographic analysis demonstrated that 43% of cases were aged over 25 years, 47% were 18–25 and 10% under 18. Females comprised 85% of cases. Mental health history was documented in 91% of SARC referrals, compared to 77% of patients who directly attended SRHS. Current mental health was assessed in 83% of SARC referral patients, compared to 75% of direct SRHS patients. RSVP was offered to 81% of patients, more than any other service. ISVA was offered to 40% of patients, and ASC was offered to 3% of patients. In total, 11% of patients were offered no service referrals. Findings suggest improvements should be made to ensure all patients have discussions around their mental health and are offered support services following SV disclosure. Further research is required to determine whether these changes improve patient outcomes.
Introduction
According to the Crime Survey for England and Wales, 20% of women and 4% of men have experienced sexual violence (SV) from age 16, with 773,000 cases reported in 2020. 1 Survivors of SV frequently develop mental illnesses as a result of their experience,2,3 including post-traumatic stress disorder (PTSD), anxiety, depression and substance misuse, with one in ten attempting suicide. 1 Following SV disclosure, patients should be offered the opportunity to discuss their mental health and wellbeing, and support service referrals offered. Accessing support has been demonstrated to reduce acute distress, aid recovery and if accessed soon after the assault, prevent PTSD.4,5
There are different pathways to accessing support depending on where the patient disclosing SV presents. Some individuals first attend a Sexual Assault Referral Centre (SARC) and are then referred to Sexual and Reproductive Health Services (SRHS) for follow-up whereas others attend SRHS directly in the first instance. Guidance on attending SARCs recommends individuals present within 7 days of the SV to ensure forensic evidence can be collected, however there is not a set-time frame and people can choose to attend the SARC at later time points. 6 Support services available include Independent Sexual Violence Advisors (ISVAs), Rape and Sexual Violence Project (RSVP) and Abuse Survivors clinic (ASC). These provide case-by-case support, offering emotional support, arranging onward counselling and helping victims to navigate the criminal justice system.
Recommendations in the literature suggest that all patients should be offered a discussion regarding their mental health and psychological wellbeing, and subsequently offered a referral for support.7,8 There are currently no recognised standards in which a clinical audit could be conducted, therefore a service evaluation was carried out.
This service evaluation aims, firstly, to collect data to understand the demographics of individuals disclosing SV when attending SRHS. Secondly, to evaluate whether mental health (past and current) is being assessed during the initial consultation after SV disclosure. Finally, to examine how many individuals are offered referrals to appropriate support services.
Methods
Sample and selection
The service evaluation was performed at University Hospital Birmingham (UHB) NHS Foundation Trust SRHS, Birmingham, UK (approval CARMS-17461). Electronic patient records (EPR) (n = 100) were extracted for patients that attended SRHS between 30/07/21 and 01/10/2021 and detailed current or past SV in a pre-consultation questionnaire. SARC referrals (n = 83) were also collected between this timeframe. SV in this study is referred to as any non-consensual sexual act or attempt at a sexual act which includes but not limited to rape, sexual assault, rape within marriage and relationships, and sexual exploitation.
In total, n = 77 SRHS referrals and n = 83 SARC referrals were included for analysis, after duplicates were removed between SRHS and SARC. Data on patient demographics, date of SV, mental health history and whether referrals services (RSVP, ISVA and ASC) were offered were extracted from the EPR.
Prior to analysis of mental health assessment data, patient records were excluded for the following reasons: if they indicated they did not want support from the service regarding SV (SRHS n = 33) or if SRHS was not attended following SARC referral (SARC n = 29). In total, n = 44 SRHS records and n = 54 SARC referrals were included for mental health assessment analysis.
Prior to analysis of support service referrals, patient records were excluded for the following reasons: patient was taken to hospital mid-consultation (n = 1) and patient moved out of area (n = 1). Additionally, some patients already had pre-existing support/referrals prior to the consultation. SRHS had pre-existing referrals for n = 5 RSVP and n = 1 ISVA, and SARC had RSVP n = 17 and ISVA n = 4. These were removed prior to referral analysis.
Statistical analysis
Descriptive statistics were performed for those that presented to SARC and SRHS. Differences between the two groups were identified using Pearson’s Chi-square test for categorical variables (significance at p < 0.05). All analyses were performed using GraphPad Prism 6.
Results
Demographics of SV disclosure
Demographics and time frame of sexual violence disclosure in service evaluation participants.
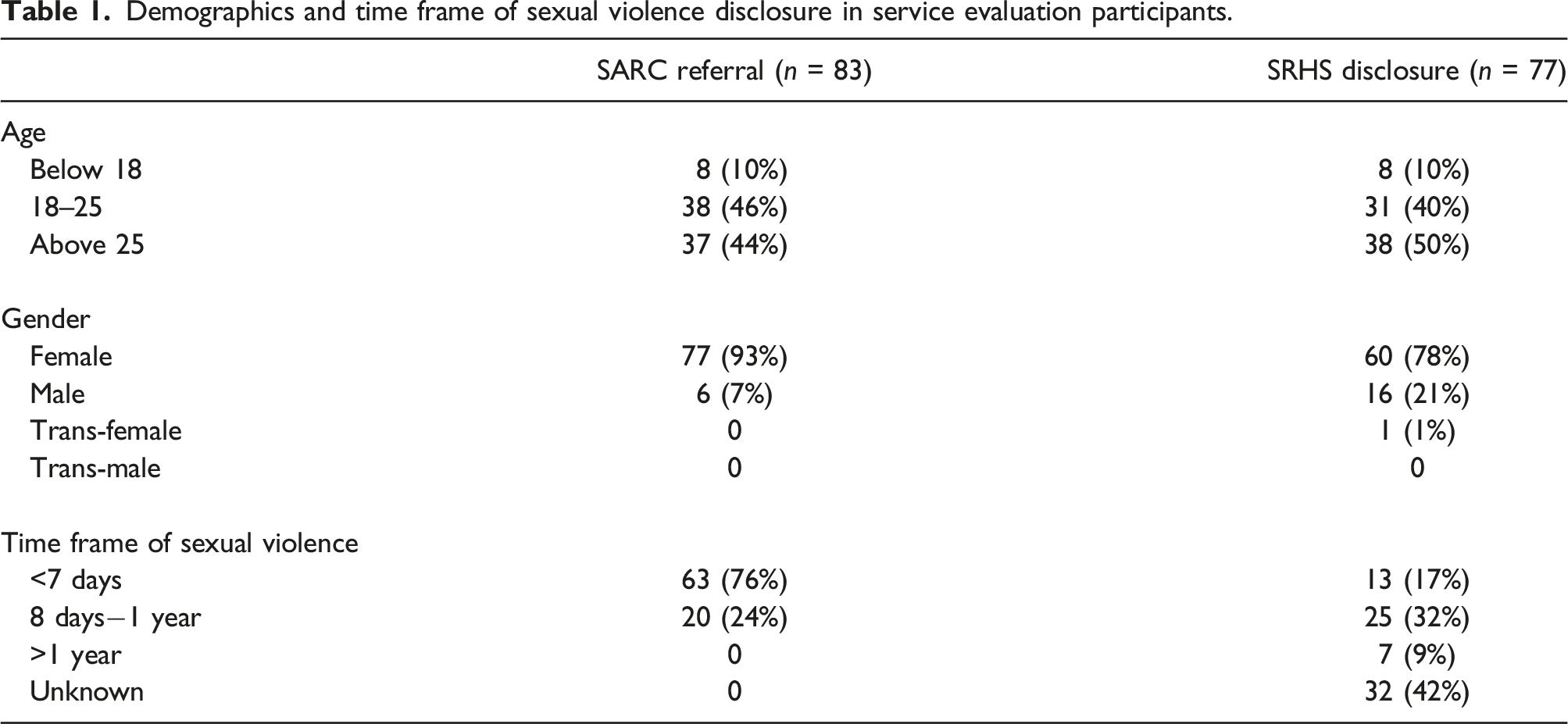
Disclosures of SV within 7 days were significantly more likely to be at a SARC, rather than at SRHS (X2 = 19.40, p < 0.05) (Table 1). There were no disclosures of SV to SARC that occurred over 1 year ago, in comparison to 9% of cases at SRHS (Table 1). 42% (n = 32) of cases had no date documented for the SV at SRHS, but it should be noted that n = 24 of these were in the cohort that requested no further support.
Assessment of mental health
Assessment of the patient’s mental health history was documented in 91% (n = 49) of SARC referral cases and 77% (n = 34) of patients directly attending SRHS. Evaluation of the patient’s current mental health was assessed in 83% (n = 45) of patients who were referred from SARC and 75% (n = 33) of patients directly attending SRHS. There was not a significant association between route of SV disclosure and mental health assessments.
Referrals to support services
Rates of referral to the three different support services were examined. RSVP was offered more than any other service (81%, n = 60) (Figure 1(a)), including 91% (n = 32) of those attending after SARC and 72% (n = 28) directly to SRHS (Figure 1(a)). 40% (n = 36) of all eligible patients were offered a referral to an ISVA (Figure 1(a)). The ISVA service was offered more when patients directly disclosed SV to SRHS (49%, n = 21) in comparison to after SARC referral (31%, n = 15) (Figure 1(a)). ASC was offered to 3% patients (n = 3) (Figure 1(a)). Patients could be offered referrals to one or more services, however 53% (n = 18) of patients attending after SARC were offered a referral to only one service (Figure 1(b)). Comparatively more patients directly disclosing to SRHS were offered dual service provision (54%, n = 21) (Figure 1(b)). Patients were more likely to be referred to RSVP and ISVA when directly disclosing to SRHS in comparison to RSVP alone if attending after SARC (X2 = 3.30, p < 0.05) (Figure 1(b)). 11% of patients (SARC n = 1, SRHS n = 7, total n = 8) were offered no referrals to any support services (Figure 1(b)). All patients were offered referral services verbally, with 13% of cases also being given written information about support services. (a) Percentage of patient referrals to each support service (RSVP, ISVA and ASC) and (b) Breakdown of which services were offered to SARC referral patients and SRHS patients.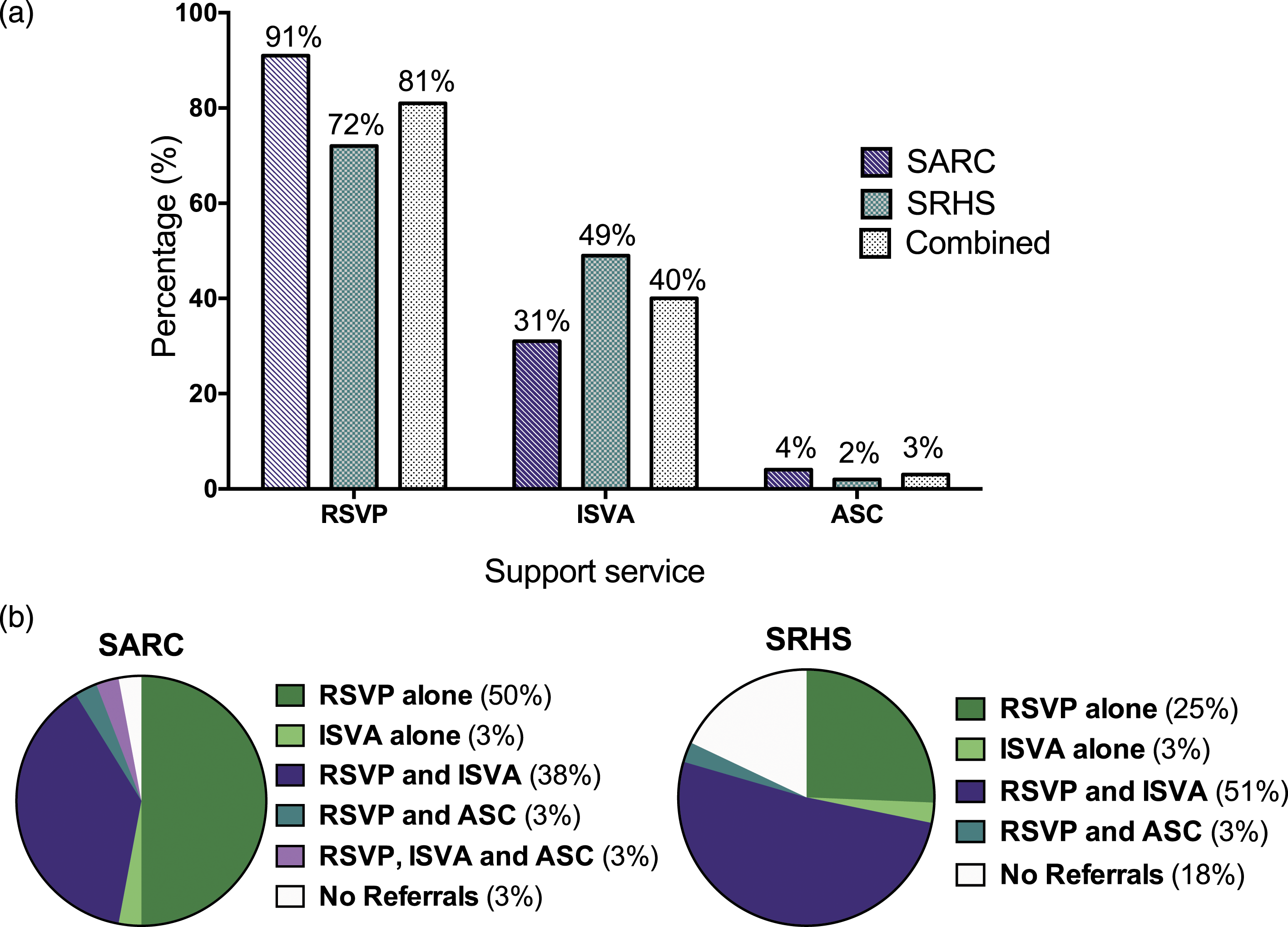
Discussion
In this service evaluation, 85% of patients had a discussion regarding their mental health history, and 80% discussed their current mental health and wellbeing. Of those eligible for referral, 97% of patients attending after SARC were offered a referral to at least one support service, compared to 82% of patients directly disclosing to SRHS. In this SRHS, a proforma document is used in all consultations to document discussions of mental health and referrals to support services. All consultations should complete the SV proforma document, therefore it is expected 100% of patients would have the opportunity to discuss their mental health and be offered referrals. It was also anticipated that there would be no difference between patients attending after SARC or directly to SRHS. However, this service evaluation suggests that the rates of mental health enquiry and referrals were lower if disclosing directly to SRHS.
This SRHS has an in-house ISVA service that can provide on the day support which is not present in all SRHS, this service evaluation provided an opportunity to assess how well utilised the ISVA service is. There was lower than expected use of ISVAs, with only 40% of patients being offered this service. As the role of ISVAs is relatively new to this SRHS, this could offer some explanation for these results. Additionally, due to these patients presenting during the COVID-19 pandemic it may have had an impact on service provision by ISVAs.
It was reassuring that a large proportion of total patients were offered discussions regarding their mental health and offered support. However, gaps are highlighted in the service where there is no record of enquiry about mental health or offer of onward support. Follow up research to investigate how many patients attended support services following referral and what the relative impact of this was on their mental health would be beneficial. Additionally, this study revealed that 35% of individuals did not attend their follow-up appointment with SRHS following SARC attendance. There is limited information on the potential factors that may contribute to an individual attending for follow-up care. Further work to understand barriers to care and to explore patient characteristics and, in particular, those associated with social inequalities, mental illness and marginalisation (e.g. sexual and gender minority communities) should be considered.
There are a number of limitations to these findings. Poor documentation was noted; the EPR showed that the health care professional (HCP) had discussed support services but had not indicated which service was offered or whether a referral was made. Patients may have declined any support from the service in regard to SV disclosure which was not documented in the EPR. Additionally, this service evaluation only included one patient who identified as transgender. Literature suggests that people in the LGBTQ+ community are at increased risk of SV, 9 therefore further work in this area is crucial. Recent national surveys in the UK found that in 50%–60% of cases, the survivor was in a relationship with the perpetrator and reported domestic abuse. 10 Additional support for domestic abuse can be co-ordinated, for example through independent domestic violence advisors (IDVAs). 11
The findings from this evaluation have resulted in suggestions for service improvements. Firstly, healthcare professionals have been encouraged to document all aspects of the consultation. The service should also ensure that staff are up to date with training regarding SV consultations and that there are clear and robust pathways for accessing the different support services. Specifically, the service should continue to provide training in a trauma-informed approach, this has been demonstrated to be effective and beneficial to both trauma survivors and staff. 12 Finally, the service could consider increasing the offer of on the day support from the ISVAs that are located within the service. Above all else, patients’ choices in accessing or declining support remains paramount. Future studies may determine whether these changes enhance outcomes for the patients which would be crucial in development of future standardisations and guidelines. The authors would suggest the findings and suggested improvements are transferable from this SRHS to others in the United Kingdom, and services should assess and ensure responses to disclosure of SV are safe and supportive.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.