
Abstract
Background
Gender-based violence in the form of domestic and sexual abuse represent a worldwide public health and civil rights issue. Healthcare and sexual health have a central role to play in prevention, particularly in the identification of sexual and domestic violence/abuse within a frontline service in which it often presents. Survivors of sexual violence and abuse commonly pass through sexual health services without being asked about their victimisation. Healthcare should be able to identify survivors, provide first line support, refer to specialist services and link to comprehensive post assault care.
Methods
In the first joint study of its kind, the Univeristy of the West of England worked with the British Association for Sexual Health and HIV (BASHH) and their Sexual Violence Specialist Interest Group (SVSIG). We report the findings of a snapshot, non-probability, exploratory survey of current comparative sexual and domestic violence/abuse enquiry practice in Genito Urinary Medicine services across the UK.
Results
Sixty-two responding services evidenced variable practice around asking, collating data, referral, training and staff supervision.
Conclusions
This benchmarking study of practice in the UK sets a bar against which all services can measure and improve current practice on gender-based violence identification, a crucial role of sexual health services in reducing the inequalities driven harm of undisclosed trauma.
Background
Sexual violence and abuse are commonly experienced but widely underreported. Data for 2020 estimated that 618,000 women and 155,000 men aged 16–74 experienced sexual violence (SV) or abuse in the UK. 1 However, this trauma remains hidden with only 17% of rape victims reporting their abuse. 2 Many survivors attend sexual health services 3 but do not disclose 4 with small scale studies documenting a sexual violence survivor rate of 17% in female clinic attendees. 5 Whilst barriers to reporting this type of trauma are complex, (shame, self-blame, rape myths) survivors are often simply not asked. 6 Screening for sexual violence within healthcare is WHO recommended 7 but practice is variable with some conflation of domestic, intimate partner and sexual violence (DV).8,9 A domestic violence ‘partner’ focus misses around half of reported rape offences recorded as perpetrated by friends/acquaintances (37%) or strangers (15%). 10 Crucially, we know that marginalised groups find it particularly difficult to report sexual violence11,12 despite evidence they are more highly targeted.11,13,14 Rates and barriers to reporting among men are also poorly understood. 15 Understanding these patterns of gender-based violence requires a civil rights and gender equality focus. Sexual health services can improve and expand enquiry to capture widely experienced sexual violence and abuse to address both unmet patient need and intersectional mediated inequality. 16
Sexual violence and the silence of delayed disclosure harms individuals’ capacity to work and participate in family and community life. 17 Survivors report poorer health and greater use of medical services, costing an estimated £10 billion a year. 18 Rates of sexual violence have tripled in recent years 19 projecting increased healthcare costs. Such demand could be reduced through earlier identification and treatment of sexual violence trauma.20,21
Proof of this concept has been established in more developed work around domestic violence enquiry. Systematic review studies evidence screening in healthcare increases the identification of intimate partner violence victims and asking about trauma did not increase harm. 22 Other studies show 84% of patients support face to face routine enquiry about sexual violence. 23
Although national strategies highlight survivors needs in healthcare24–26 there is an evidence gap around practice.3,4 We do know sexual violence is often conflated with domestic or intimate partner/ex-partner violence that takes place within an ongoing relationship. 27 Research shows negative or poor responses from healthcare professionals can silence future disclosure and reporting. 28 Health care practitioners’ capacity to respond relies on training, onward referral pathways 19 and supportive or restorative supervision.29,30
Therefore, improving identification of sexual violence in sexual healthcare demands a clearer picture of practice and access to supportive resources. The aim of this survey was to provide a national snapshot of sexual and domestic violence enquiry as a benchmark and a springboard for improved routine enquiry.
Methodology
This survey of sexual and domestic violence enquiry in sexual health services was carried out in collaboration with the UK professional body for sexual health clinicians (BASHH) between May 2022 and March 2023. Patient and public involvement input came from clinicians via the BASHH Sexual Violence Special Interest Group (SVSIG) and a survivor lived-experience group who supported the concept of routine enquiry in sexual health services. An exploratory online survey was developed with the SVSIG and piloted with members and one service lead. As an anonymous exploratory survey of service provision, ethical approval was not required. Questions included a differential definition of sexual and domestic violence and asked for information on practice around when services ask about each (only if spontaneously disclose, only in target groups or when risk seen, routinely in various ways or routinely by standardised means). Questions extended to resource support for both domestic and sexual violence enquiry and a completion time of around 15 min for 55 questions was facilitated by skip routing. The survey link was circulated to sexual health service clinical and safeguarding leads throughout the UK via e-mail and relevant social media, newsletters, and national conferences. Clinical and safeguarding leads in all 200 sexual health clinics across the UK were sent invitation emails (with reminders for non responders). A total of 98 responses were secured in this non-probability sample. Data was cleaned to remove service/area duplicates. Initial data cleaning of the 98 responses removed 25 blank, incomplete (no partial response datasets were supplied) and clinic duplicates (identified by name/geographical location) resulting in a final sample of 62 (approximately 31% response rate). These are referred to variably as services, respondents or clinics. Data is reported here through descriptive frequency analysis with responses out of N = 62 stated and expressed as a percentage. As an exploratory survey of a non-probablity sample, standardised reporting guidelines were not applicable.
Results
Sample
Two BASHH branch areas logged no responses to the survey, Findings therefore do not represent clinic practice in these areas. The responding clinics reported generally high levels of routine enquiry about both sexual and domestic violence. As a non-probability sample, data may represent clinics already more engaged in these topics.
Asking and telling
Domestic violence was more frequently asked about routinely than sexual violence (54/62 or 87% vs 45/62 or 72%) and more often using standardised methods such as an electronic patient record or screening prompt (34/62 or 55% vs 25/62 or 40%), see Figure 1. Non-standardised enquiry about both sexual and domestic violence was reportedly triggered by variably defined target group characteristics including: - young people, sex workers, vulnerable adults, transgender patients, or indicators of sexual exploitation such as substance misuse, sexual assault, unusual behaviours and/or other wellbeing concerns. Marginalised identity (racially, sexually, ability minoritised communities) was not reported as a risk indicator or recorded by any services in relation to violence or abuse apart from transgender identity. 19% (12/62) of responding clinics reported only asking about sexual violence in patients presenting with risk indicators or disclosing spontaneously, a practice less common for domestic violence enquiry (8%, 5/62). Comparative enquiry of sexual and domestic violence.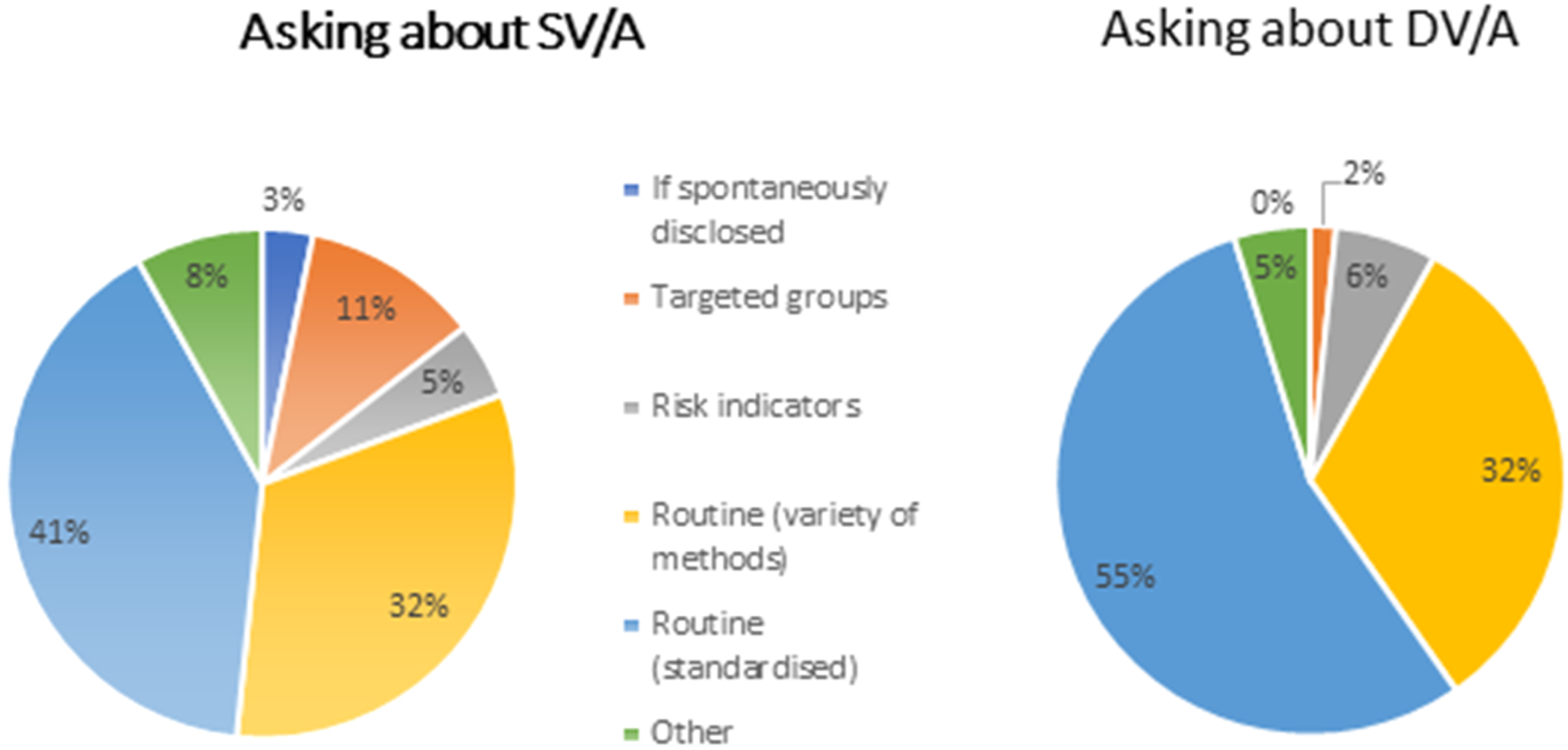
Use of electronic record prompts were commonly reported such as ‘history of sexual assault/violent abusive relationship'. Specific questions that focused on sexual violence included, “The recent sexual contact you’ve told me about, has that been sex that you wanted to have?” “Have you ever been made to do something sexual that you did not want or that you felt you could not say no to?” However, clinics also reported using domestic violence oriented questions such as “Do you feel safe/any current domestic abuse?” to reportedly identify both sexual and domestic abuse, suggesting some conflation of SV within DV.
Data collection can be seen as proxy measure for the importance of an issue. Services were asked “What data (if any) do you collect? For sexual violence, 28/62 or 45% of respondents described some form of data collection. More clinics said they recorded data on domestic violence (37/62 or 60%). The survey asked for information on sexual and domestic violence enquiry and disclosure rates. Only 11 respondents could supply this data. Reported enquiry rates ranged between 51 and 100% but conflated domestic and sexual violence using a mixture of referral numbers, descriptive accounts and audit data. A few clinics were able to provide disclosure/referral rates for domestic violence of between 0.4% and 4% but none were able to report on sexual violence disclosure/referral rates. One large city service recorded an annual rate of 44 disclosures of acute sexual assault, 93 non-acute, 12 disclosures of trafficking/exploitation and 109 cases of child sexual exploitation.
Resourcing enquiry
Domestic violence response training was reportedly more common than sexual violence response training (57/62 or 92% vs 30/62 or 48%) with 10 respondents indicating some conflation of sexual violence within general safeguarding or domestic violence provision.
Most clinics in this sample reported onward referral pathways for disclosures (62 for domestic violence and 59 for sexual violence). Referral pathways for domestic violence disclosures included 33 referred to safeguarding teams and 20 to a specialist Independent Domestic Violence Advisor (IDVA), nine did not specify. For sexual violence, 22 referred to safeguarding teams and 12 to a specialist Independent Sexual Violence Advisor (ISVA), a greater number (25) did not specify.
Most responding clinics reported receiving supervision around domestic (53/62 or 85%) and sexual violence (45/62 or 68%) with around half of this framed as purely clinical supervision and half including restorative support.
When asked about what services needed to support work in this area, suggestions included health advisor or dedicated ISVA and IDVA provision, more psychological supervision for the whole clinic team and greater acknowledgement of the emotional trauma that staff experience in handling disclosures.
Discussion
This survey provides an important benchmark of current practice in identifying sexual and domestic violence in patients attending sexual health services. The data gives insight into the volume of survivors passing through services without being offered the chance to get help and the resources required to improve recognition of different types of gender-based violence within sexual healthcare settings. Improving identification and management of disclosures in this setting could increase early intervention and begin to mitigate the health and economic costs of untreated sexual trauma.
Of the services responding, overall high levels of routine enquiry were reported for both domestic and sexual violence as recommended 8 with some evidence of a 15% lag in rates for sexual violence (72% vs 87%). More services reported relying on ‘targeted’ versus routine sexual violence enquiry using subjective ‘identifiers’.4,22 Bringing universal models for routine enquiry about sexual violence up to current NICE recommended levels for domestic violence 9 seems within reach.
Barriers to improved enquiry include indicators of some conflation of sexual violence within domestic violence, suggesting a lack of understanding of these distinct but often overlapping experiences. Although 18 respondents reported a dedicated sexual violence question, a further six used a single question to enquire about both domestic and sexual violence. Conflation may begin in training; services reported almost universal domestic violence response training provision, compared with less than half receiving similar training in relation to sexual violence. Following through to data reporting practices, no service was able to provide sexual violence disclosure rates. This lack of recording may stem from inadequate data infrastructure or a lack of tariff-based payments for safeguarding. The result is a gap in the evidence, limiting the ability to prioritise and plan relevant service provision at a national and local level.
Study limitations
The response rate and complexity of clinic/service delineation means that a minority of UK service areas are not represented in this voluntary study. It is possible that lack of engagement indicates lack of activity or ability to respond in an overstretched service. The survey was circulated during the mpox outbreak in 2022 the demands of which were challenging for already stretched sexual health services. However, if participation in the survey is a proxy of engagement with sexual and domestic violence, it might be that the disparity found here could indicate lower enquiry in non-responding services.
Estimating a response rate (31%) from the 200 BASHH listed clinics was complicated by difficulty in identifying duplicates between clinic site and overarching service level. Data was cleaned using service name and geographic location to remove duplicate service responses. Responses given by clinic leads may indicate ideal practice, rather than necessarily a reflection of what happens on a case-by-case level. Inclusion of the gender-based violence (both sexual and domestic) topics in a national audit, benchmarking current practice against published guidelines, 8 could overcome this complexity.
Conclusions
This snapshot of sexual and domestic violence enquiry practice in the UK evidences variability in practice and suggests many survivors will not be given the opportunity or prompted to disclose DV or SV Services can compare and improve their current practice around gender-based violence enquiry with the benchmarking data presented. The building blocks or facilitators of enquiry were not always available with gaps in standardised approaches to enquiry, dedicated sexual as well as domestic violence response training, basic data collection and reporting and restorative supervision. Sexual health services need to better understand the overlapping but related nature of gender-based violence present within their services through targeted work on both sexual and domestic violence. Improvements in identification of domestic violence/abuse from current or previous partners abuse has not been matched with the equivalent for sexual violence/abuse. Our study evidences conflation of sexual and domestic violence which may reflect a wider societal silence or myth informed understanding of sexual abuse. Best practice should be user-led through collaboration and co-production as evidenced to the Women and Equalities Committe by BASHH President Dr Claire Dewsnap 31 , including workwith local specialist sexual violence organisations. 32
Supplemental Material
Supplemental Material - Sexual and domestic violence enquiry: A national exploratory survey of asking and telling in sexual health services in the UK
Supplemental Material for Sexual and domestic violence enquiry: A national exploratory survey of asking and telling in sexual health services in the UK by Jane Meyrick, Amy Bennett, Kyle McGovern and Charlotte Kite in International Journal of STD & AIDS
Footnotes
Acknowledgements
The authors wish to thank the NHS Bristol, North Somerset and South Gloucestershire Integrated Care Board (ICB) for contributing funding and SARSAS (Somerset & Avon Rape & Sexual Abuse Support), for their voice groups input into the work. The full support of the BASHH Sexual Violence Special Interest Group was invaluable.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by BNSSG ICB (RCF 21/22-1JM).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.