
Abstract
We report an unusual case of human immunodeficiency virus (HIV) infection initially presenting with hypothermia and bradycardia associated with an HIV encephalitis. Searches reveal only five reported cases of spontaneous episodic hypothermia in the context of HIV infection. In our case, magnetic resonance imaging revealed the presence of a persistent cavum septum pellucidum (CSP), an anatomical and functional neuro-developmental abnormality, as well as changes compatible with an HIV encephalitis. Episodic hypothermia can occur in association with agenesis of the corpus callosum, known as Shapiro’s syndrome, and the presence of a persistent CSP in our case suggests it may have contributed to the clinical presentation.
Keywords
Introduction
Severe neurocognitive disorders associated with human immunodeficiency virus (HIV) have become increasingly uncommon. We describe an unusual case of HIV infection initially presenting with hypothermia and an encephalitis.
Case report
A 38-year-old Black African heterosexual man was brought to the Emergency Department following an episode of collapse in the street in daytime in the UK in May. The patient reported a six-week history of progressive confusion, in particular understanding commands as well as decreased co-ordination, dysgraphia, dropping objects, lethargy and weight loss (approximately 12 kg). He had no history of loss of consciousness, fever or excessive sweating, no significant past medical history and had never had an HIV test. The patient was previously fit and well, worked as a hotel receptionist and had not travelled outside of the UK in the last 2 years.
Upon admission, the patient was grossly hypothermic with a non-recordable body temperature, bradycardic at 38 beats per minute and hypotensive with a systolic pressure of 79 mmHg. Cardio-respiratory, abdominal and full neurological examination only elicited an ataxic gait whilst the Glasgow Coma Scale remained 15/15.
Laboratory investigations demonstrated pancytopenia, a raised total immunoglobulin G and a positive fourth-generation HIV test. CD4 count: 38 cells/μl (12%) and HIV viral load: 1,030,000 copies/ml. Auto-immune and endocrine screens were negative/normal. Electrocardiogram demonstrated sinus bradycardia with Osborn waves and ventricular standstill episodes of up to 6 s, which was later confirmed via telemetry, but echocardiography was normal and pacing was never initiated.
Chest x-ray was normal, as was a contrast-enhanced head computed tomography scan, except for the presence of a persistent cavum septum pellucidum (CSP). Cerebro-spinal fluid (CSF) showed protein 2.23 g/L, glucose 3.3 mmol/L, WBCs 48 and 95% lymphocytes. CSF bacterial and mycobacterial cultures were negative as were viral polymerase chain reaction (PCR) assays including cytomegalovirus (CMV), varicella-zoster virus, and John Cunningham virus, but there was no residual CSF specimen for HIV-RNA.
The patient received immediate resuscitation management with a forced air warming blanket, warmed fluids and broad spectrum antibiotics, causing the temperature to rise to 35.7°C and improve his blood pressure.
After a subsequent transfer to infectious diseases, the patient demonstrated fluctuating cognition and magnetic resonance imaging (MRI) confirmed the CSP (Figure 1) and verified subtle patchy increased T2/FLAIR signal in the cerebral white matter, consistent with an HIV encephalitis. Human Leucocyte Antigen-B5701 was negative and anti-retroviral therapy (ART) with abacavir, lamivudine and dolutegravir was commenced. With neuro-rehabilitation input, the patient clinically improved and was discharged with no further episodes of hypothermia or bradycardia. After 15 months of ART the patient is working full time, his CD4 is 142 cells/μl (13%) and HIV viral load is undetectable.
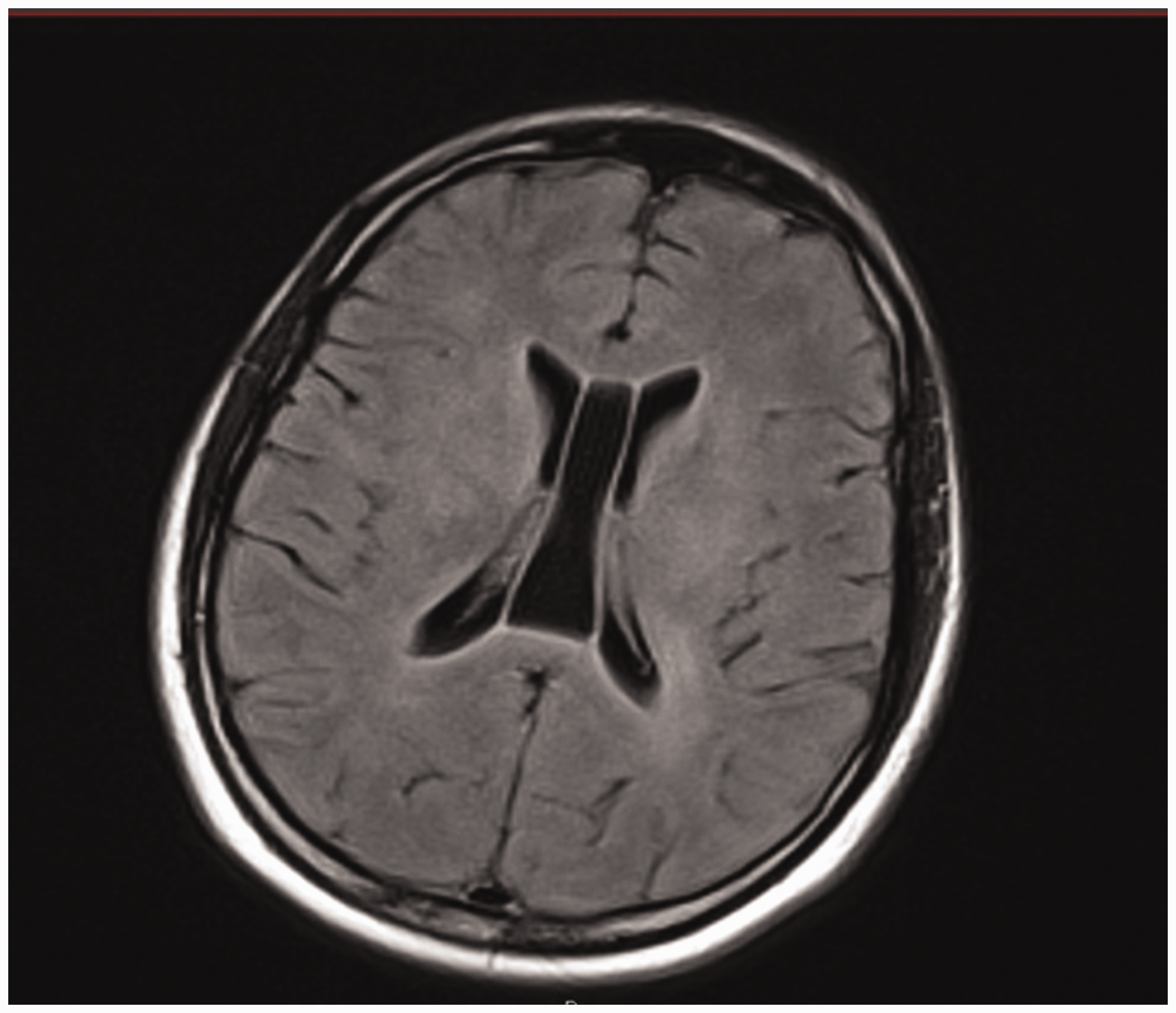
MR flair image, showing a persistent cavum septum pellucidum grade 4.
Discussion
There have been only five previously described cases of hypothermia in people living with HIV where there was no environmental exposure to low temperatures.1–4 One of these occurred in the setting of renal failure, a temperature of 32°C and CD4 count 317cells/μl, and serum CMV PCR assay was positive at 10,000 copies/ml. Imaging exhibited no evidence of HIV encephalitis, but MRI illustrated cortical atrophy. This patient clinically responded to intravenous ganciclovir and returned to normal body temperature. 1 Another case demonstrated untreated HIV infection presenting with spontaneous episodic hypothermia (SEH) <30°C, confusion and sweating. 2 This patient also had no evidence of encephalitis, but MRI showed brain atrophy and the episodes of hypothermia remitted with ART and virological control. Another case presented with a temperature of 32.7°C, untreated HIV infection, severe protein calorie malnutrition and hypothyroidism. 3 This patient also had no evidence of encephalitis, although MRI showed chronic ischaemic change in the peri-ventricular and subcortical white matter, and the episodes of hypothermia remitted with ART and virological control. Two further cases presented with episodes of excessive sweating where temperatures of 34.7°C and 35.2°C were recorded. 4 One case had no CNS abnormalities and one case demonstrated lacunar infarcts in the internal capsule. Some form of central nervous system abnormality was therefore demonstrated in four out of five of these cases. Clearly, there can be multiple or additive causes of hypothermia in HIV including HIV-related neurodegeneration causing hypothalamic dysfunction, uncontrolled HIV viral replication causing functional hypothalamic neurotoxicity, opportunistic infections such as CMV and malnutrition.
SEH accompanied by hyperhidrosis was described in 1969 in association with agenesis of the corpus callosum and is known as Shapiro’s syndrome. 5 Although rare, this often presents in childhood, hyperhidrosis is not always present, and a broad diversity of brain abnormalities are found. 6 Our case of HIV-associated hypothermia demonstrated the CNS abnormality of CSP. The septum pellucidum is a thin vertical partition of white matter composed of two laminae which separate the two lateral ventricles, and these laminae normally fuse during gestation. 7 Non-union is referred to as CSP and is a common neonatal abnormality which only persists in 1% of adults and has been associated with obsessive compulsive disorder, schizophrenia spectrum and bipolar disorders.7–9 In neurodevelopment, the septum pellucidum is closely linked to the corpus callosum, hippocampus and hypothalamus. CSP thus represents a limbic system abnormality, and our case demonstrates the most severe form, grade 4 (Figure 1). 7
Shapiro’s syndrome demonstrates that neuro-developmental abnormalities can be an underlying cause of hypothermia. We speculate that the CSP in the setting of HIV encephalitis may have functioned as a similar neuro-abnormality leading to this rare presentation with progressive hypothermia and bradycardia as presenting features of HIV disease.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.