
Abstract
Throughout the early months of 2020, COVID-19 rapidly changed how the world functioned, with the closure of borders, schools and workplaces, national lockdowns, and the rapid normalization of “self-isolation” and “social distancing”. However, while public health recommendations were broadly universal, human capacity to accordingly transform everyday life has differed significantly. We use the example of South Africa to highlight the privileged nature of the ability to transform one’s life in response to COVID-19, arguing that the virus both highlights and exacerbates existing inequalities in access to infrastructure. For those living in urban poverty in South Africa, where access to basic infrastructure is limited, and where overcrowding and high density are the norm, it is frequently impossible to transform daily life in the required ways. The failure of global public health recommendations to recognize these inequalities, and to adapt advice to national and local contexts, reveals significant limitations that extend beyond this specific global pandemic.
Keywords

I. Introduction
This paper was written in the midst of the COVID-19 pandemic by two researchers situated in the global North and South, both with extensive fieldwork experience in urban South Africa. It responds directly to the potential of the ongoing COVID-19 pandemic to deepen existing inequalities. Using the example of South Africa, this paper draws attention to the ways COVID-19 highlights and exacerbates existing inequalities in access to infrastructure in the global South. This paper was initially written in April 2020 (with minor updates in July 2020), in the early stages of South Africa’s lockdown response to the global pandemic.
In December 2019 a “pneumonia of unknown cause”, later named “severe acute respiratory syndrome coronavirus 2”, or SARS-SoV-2 (now colloquially known as coronavirus) was first reported to the World Health Organization (WHO) country office in China. Over the following months, the virus spread rapidly around the world, causing large numbers of human fatalities, destabilizing the world’s strongest and weakest economies, and severely restricting the movements of global populations through lockdown, social distancing and travel restrictions.
While the origins of the virus are presently traced to China, this is inherently a global virus – not merely in terms of the epidemiological geographic spread, but equally in terms of the impacts across the world’s social, political and economic landscapes. However, as this paper demonstrates, those impacts are unevenly distributed, not just between countries with differing capacity to provide for example healthcare and socioeconomic support packages, but also within countries, where pre-existing inequalities are accentuated by public health advice framed by Euro-Asian contexts.
Specifically, global approaches that are largely led by what is feasible in high-income countries with strong governments overlook the enormous differences in the global capacity of governments to respond, the physical and financial infrastructure that allows societies to react, and inequalities in the ability of citizens to act in accordance with government responses and keep themselves “safe” during the COVID-19 outbreak. The uneven impacts of COVID-19 and its potential to deepen existing inequalities are increasingly raised in the media. Amaral et al.(1) and Doré,(2) for instance, warn against the unequal impacts of COVID-19 in Brazil, and Aguirre(3) calls to change the neoliberal agenda to prevent the widespread negative non-health impacts of the pandemic. Using the example of South Africa, this paper focuses specifically on the inequalities of access to infrastructure in South Africa and demonstrates how COVID-19 highlights and exacerbates such inequalities.
II. A Global Virus in The Global South: Public Health Strategies and Inequalities
COVID-19 is a global virus, but its impact is uneven. The virus initially predominantly affected China and other parts of Asia, but soon spread to Europe and North America, with the highest concentrations per capita typically identified in large cities (Northern Italy’s rural outbreak notwithstanding). While leaders beyond Asia were initially slow to acknowledge the severity of the pandemic, by March 2020 the depth of the crisis was self-evident. The world’s high interdependence and flows of goods, services and people allowed the virus to spread rapidly, particularly within and between countries with significant interconnectedness. In part because many in the world’s poorest countries cannot participate in international travel, it took the virus much longer to get a foothold there (likely augmented by a lack of testing to support data on infection). Because of the initial concentration of COVID-19 in Asia, Europe and the US, global public health responses have been heavily informed by the societal structures and lifestyles of countries with higher incomes and tax bases (e.g. Europe, US, Singapore) and more authoritarian regimes where extreme state surveillance is common (e.g. China, South Korea).
Two broad non-pharmaceutical interventions have been implemented to reduce transmission by reducing contact within the general population: mitigation and suppression. Both limit the spread of the disease, but they bring different challenges, particularly in the global South. Mitigation sets out to slow, but not necessarily stop, the spread of the epidemic, e.g. through decreasing peak healthcare demand while protecting people most at risk. This so-called “flattening the curve” requires a long-term commitment of medical infrastructure (hospital beds, beds in intensive care units, ventilators) and staff.(4) Such mitigation policies as quarantine or home isolation of those with a high likelihood of carrying the virus, and social distancing of those most at risk, are designed to reduce strain on the healthcare system and thereby reduce deaths. Many countries have resorted to temporary lockdowns, including closing schools, cafés/restaurants and other non-essential businesses, and in many regions and countries (e.g. Hubei Province in China, Italy, Spain, South Africa), there have been complete prohibitions on leaving home other than for buying groceries or medically related outings. Many other countries restricted movement but allowed daily exercise outings with restrictions on size of group, time outside, and distance from home. Although mitigation reduces deaths by spreading infections over a longer period of time to ensure continued access to healthcare, many people still die from the disease as the peak is moved out rather than the disease being stopped.
The second strategy is suppression, aiming to reverse growth of the epidemic by reducing to a minimum the average number of secondary cases that each case generates, thus keeping total case numbers low.(5) Examples of measures include social distancing (i.e. maintaining physical distance from non-household members), using bank cards instead of cash, avoiding crowds and practising good hygiene. These measures, extensively promoted through social media, television, radio, public health campaigns and government briefings/speeches, are designed to reduce transmission of the disease. The core challenge is that the measures need to be continued as long as the virus is active in the population, or until a vaccine is available.(6) This is problematic because, as Enserinck and Kupferschmidt point out, “long lockdowns to slow a disease have catastrophic economic impacts and may devastate public health themselves”. A balance needs to be found between “protecting health, protecting the economy, as well as protecting people’s wellbeing and emotional health”.(7) Crucially, the epidemic modelling done to predict health outcomes does not capture the social and economic implications, which are particularly acute in global South contexts where governments lack capacity to finance safety nets for the poor.
In addition, the mitigation and suppression strategies, public health interventions and media narratives related to COVID-19 have centred on the higher risk of fatalities amongst the elderly or people with co-morbidities, including the immunocompromised. Significant attention is given in high-income countries to protecting this relatively small part of the population from exposure to the virus, in particular through measures of shielding, social distancing and increased hygiene. While following these guidelines, in particular those of social distancing and lockdown, has been challenging in high-income countries, the challenges for those living in the global South are more significant.
In many global South countries, large (sometimes majority) parts of the population are vulnerable in these health terms, and their governments have less capacity to implement such targeted measures. Tuberculosis (TB), which is likely to leave people at greater risk of contracting COVID-19, illustrates this vulnerability. It is the world’s leading infectious disease killer, affecting nearly 10 million people worldwide, and it caused 1.5 million deaths in 2018.(8) (COVID-19, by contrast, infected 1.4 million people in its first four months and there were 79,385 deaths as of 9 April 2020.(9)) Given TB’s scale, it is therefore unsurprising that the WHO and other public health organizations have targeted those infected as potentially vulnerable and needing protection from COVID-19.(10)
In South Africa, a large part of the population is immunocompromised and therefore very vulnerable. An estimated 7.35 million people (approximately 13 per cent of the population) suffered from Human Immunodeficiency Virus (HIV) in 2018, and an estimated 89,000 people died from AIDS-related causes in 2017.(11) Similarly, according to the 2019 WHO Global TB Report,(12) around 322,000 people (just under 1 per cent of the population) fell ill with active TB in 2017; the majority of those infected were living in low-income communities. Roughly 78,000 people died from TB in 2017. Of these, 56,000 were HIV positive.
The South African population, with its high incidence of TB and HIV, could therefore be expected to be extremely vulnerable to a large-scale COVID-19 outbreak, and preliminary studies have suggested that those living with HIV and TB in the country have an increased death risk from COVID-19.(13) Although the reported effect seems relatively small, there remains a severe lack of data on how HIV and TB may interact with COVID-19. Furthermore, public health officials recognize that data based on global North contexts are not necessarily relevant in South Africa because, for example, “the South African population may differ in several ways from the Italian patients, including underlying medical problems, socioeconomic status, and access to health care”.(14) Consequently, while we know that immunocompromised people are at greater risk of COVID-19 complications, and that such people represent a higher proportion of populations in the global South than the North, the implications of this knowledge for how COVID-19 may play out in practice in South Africa remain uncertain.
Furthermore, despite widespread recognition that specific health/age demographic groups are more vulnerable to fatality from COVID-19, there is significantly less recognition that inequalities in access to infrastructure and resources can also affect a population’s exposure to COVID-19 or its ability to respond, and may exacerbate existing vulnerabilities and/or create new ones. Indeed, public health officials recognize, according to Corburn and colleagues, that “the most vulnerable groups [are] particularly those living in informal habitats and depending on informal livelihoods in the global south”.(15) It is these challenges and the ways in which they deepen existing inequalities that are the primary focus of the paper, which concentrates on South Africa as a global South case study.
III. COVID-19 Responses and The Privilege of Being Able to Comply in South Africa
a. South Africa’s virus and the government response
Once the coronavirus was detected in South Africa, the government responded rapidly to the threat in an attempt to limit spread and “flatten the curve”. This included promptly employing public health strategies seen elsewhere, and especially adopting a mitigation perspective. Following the first confirmed case on 5 March 2020 in a patient recently returned from Italy, on 15 March (when 51 people were infected but no deaths were reported) President Cyril Ramaphosa announced a national state of disaster and set in place school closures, travel bans and restrictions on public gatherings. One week later, the president announced a complete lockdown for 21 days, starting on 26 March, when there were 927 confirmed cases and no deaths had been reported. This was later extended by two weeks to 30 April (i.e. a five-week lockdown in total). During lockdown, people were allowed outside only for essential activities (groceries and medical outings), enforced by the military and police.
At the end of this lockdown the government introduced the COVID-19 alert system to manage its gradual easing and move from a strong mitigation perspective towards suppression (Table 1). The alert system has five levels. It is based on a risk-adjusted approach and guided by several criteria including: (i) the capacity of health facilities to accommodate severely sick people; (ii) the level of infections and the rate of transmissions; and, as the government explained it, (iii) the “extent of public health interventions and the economic and social impact of continued restrictions”.(16)
Summary of alert levels
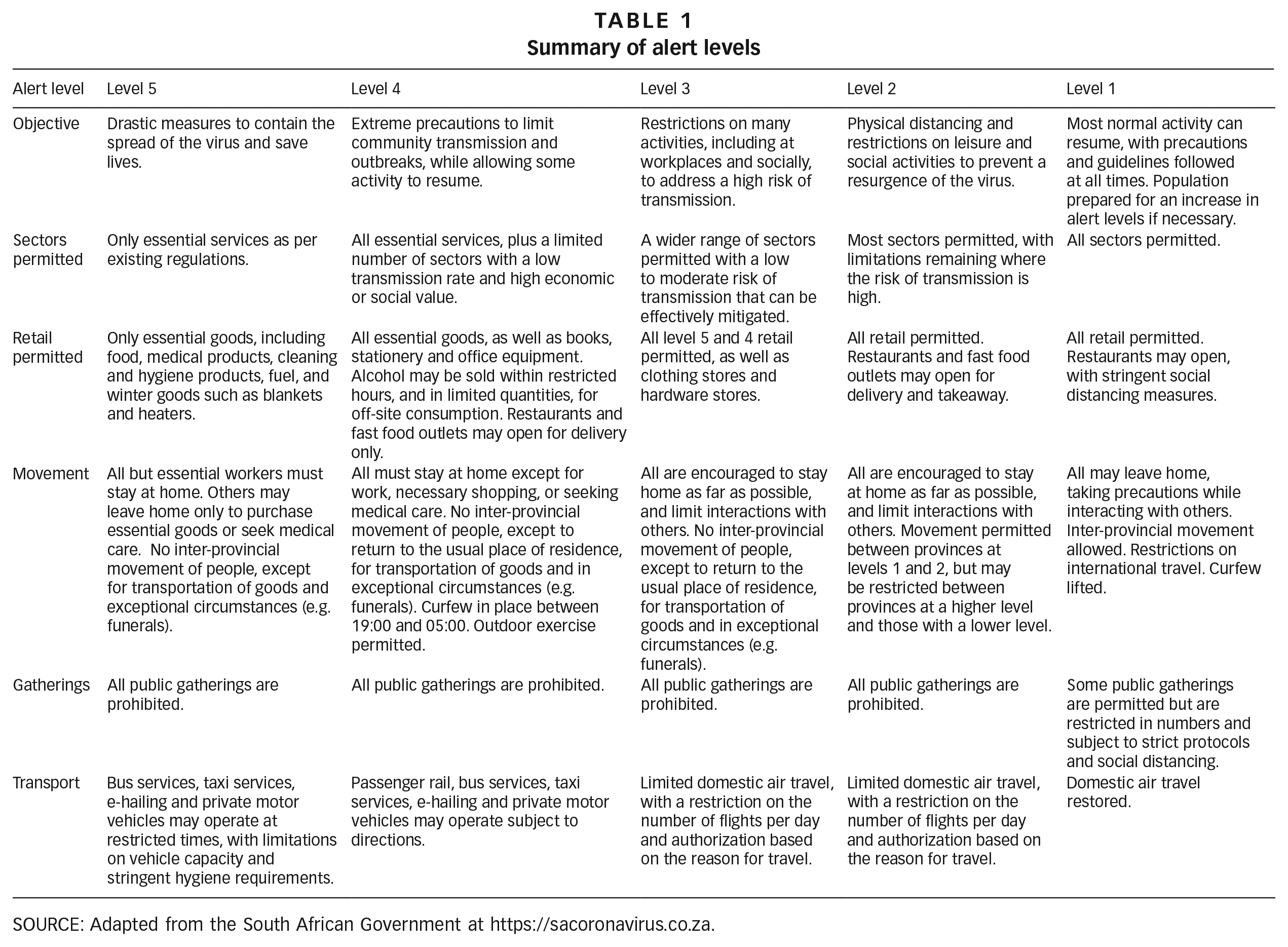
SOURCE: Adapted from the South African Government at https://sacoronavirus.co.za.
After five weeks of full lockdown on level 5, largely focused on “flattening the curve” as part of South Africa’s mitigation measures, the lockdown was eased to level 4. At this point, the pandemic response slowly moved towards a combination of mitigation and suppression. This level, implemented between 1 and 31 May, allowed some key economic sectors to operate (e.g. agriculture and public works civil engineering projects).
At the time of writing, the country is in alert level 3, which was implemented on 1 June 2020. As of 25 July there had been 434,000 confirmed cases and 6,655 deaths.(17) As there is a range of hotspots (areas with more than 5 infected people per 100,000, or with a rapid increase in new infections), the government announced that a differentiated approach would be taken for specific areas, particularly in urban areas.
The initial lockdown in March 2020 received wide public support as a necessary strategy to prevent the spread of COVID-19 and allow the state to prepare for the rollout of other plans. However, the severe impacts of lockdown on the poor in South Africa (where the risk of starvation may be greater than the risk of dying from COVID-19) raise doubt about the appropriateness of the full lockdown (the mitigation strategy) for the South African context. Arguably, the suitability of the extreme lockdown is dependent on the specific measures that accompanied it, explored later in this paper. Specifically, these are the inability of the urban poor to comply with handwashing requirements, the irrelevance of remaining “indoors” for those without formal shelter, the impossibility of social distancing in overcrowded high-density settlements, and the impacts of overlooking the informal sector.
In addition to the alert levels, President Ramaphosa announced a socioeconomic response plan on 22 April 2020, to support the functioning of the economy under lockdown. The country’s response was to be based on four main interventions, including: (i) a large increase in the health budget to respond to the virus; (ii) relief of hunger and social distress; (iii) support for companies and employees; and (iv) a phased reopening of the economy. A corresponding economic stimulus package, worth R500 billion (£23.3 billion), was announced to (re)direct resources to pandemic response. Key measures of relevance for this paper included:
R500 (£23.30) increase per month in the child support grant for the next six months.
R350 (£16.30) unemployment grant per month.
A total of R200 billion (£9.3 billion) in loan guarantees, in partnership with major banks, the National Treasury and the South African Reserve Bank.
There have been mixed responses to the plan, including criticisms that it will, according to Ramantsima, be “exploiting the poor, deepening poverty levels and the shrinking middle-class poor”,(18) as well as increasing inequalities between South Africans and foreign nationals, who often struggle to qualify for state support.(19)
Within the context of the state’s response to COVID-19, the capacity of individuals to comply with government regulations is highly differentiated and reveals significant inequalities that predate the pandemic. In the next few subsections, we highlight these inequalities and how they impact (and are impacted by) COVID-19.
b. The privilege of “choosing” to follow public health recommendations
Globally, three specific public health recommendations dominated initial responses to COVID-19: handwashing, social distancing and lockdown (mask-wearing appeared later). All require citizens to change their behaviour. While the specifics of implementation and extent of state regulation differ between countries, these three interventions are globally recognized. We explore the assumptions inherent in each of these recommendations, for example regarding access to clean water, the practicality of infrequent shopping, and the physical space required to distance from others and remain indoors. These assumptions are hardly surprising given that WHO recommendations initially emerged to tackle the virus in countries/cities with well-developed physical and financial infrastructure networks. However, using the example of the daily lives of the urban poor in South Africa, we explore how these public health recommendations assume a privileged capacity to comply, effectively ignoring the prospect that compliance, far from being a matter of choice, is impossible for some. Indeed, when the South African president announced a national lockdown on 24 March, he stated that “the most effective way to prevent infection is through basic changes in individual behaviour and hygiene”.(20) This statement assumes universal capacity to change behaviour, and overlooks the vast inequalities in infrastructure access in South Africa’s cities. In this paper, we demonstrate the ways the pandemic highlights and exacerbates these existing inequalities, as well as how government advice fails to acknowledge the privilege of being able to choose to change one’s behaviour. The hardest-hit areas (in terms of the highest concentrations of COVID-19 infections) are in low-income, densely populated townships, where people cannot withdraw from social interactions in a single home, work remotely, buy large quantities of supplies to avoid regular visits to the shops, or drive alone in a car to secure supplies.
While we recognize that the South African government is largely following international “best practice” in an extremely challenging context, we argue that public health advice tailored to local contexts is urgently required. In this paper we reveal how a short-term pandemic highlights the long-term inequalities of access to infrastructure in South Africa.
Handwashing
On 9 March, just days after the first confirmed case of coronavirus in South Africa, Health Minister Zweli Mkhize used a press briefing(21) to urge South Africans to regularly wash their hands to limit the spread of the virus. Two weeks later, the president, in his national lockdown speech, urged citizens to “wash hands frequently with hand sanitisers or soap and water for at least 20 seconds”.(22) These recommendations are in line with WHO guidelines, as well as the public health advice issued in many other countries at that time. However, this blanket statement on handwashing belies the realities of water access in South Africa. While official statistics indicate almost universal (98 per cent) piped water access for urban households, in practice this “access” is seriously undermined by service interruptions and affordability.(23)
As part of South Africa’s constitutional right to water, the Free Basic Water (FBW) policy mandates that municipalities provide low-income “indigent” households(24) with a small amount of free piped water within 200 metres of their home.(25) With over one-fifth of South Africa’s population (22 per cent) registered as indigent,(26) this represents a significant number of households. In the City of Cape Town, households that register as “indigent” (itself a complex and paperwork-heavy process that excludes many low-income households(27)) receive 350 litres of free water per day, managed via a compulsory water demand management device (WMD).(28) Since Cape Town’s 2015–2018 drought, WMDs have been widely installed as a state tool to monitor consumption (high consumers are threatened with installation for monitoring purposes), but they remain compulsory only for those registered as indigent. Since 2007, approximately 250,000 WMDs have been installed in the City of Cape Town, the vast majority most likely in low-income households, meaning that around one-fifth of the City’s households have their daily water capped at 350 litres.(29) For these households the WMD operates as a tool that both delivers and limits water supply, automatically cutting off water supply when the daily ration is reached, and reopening the valve at 05:00 the next morning.
In many low-income formally planned housing settlements (as distinct from “slums”/informal settlements), multiple households occupy a single plot. In some cases there are multiple backyard dwellings, each housing a separate household; in other cases multiple households share a single property; and in yet other cases, the single “household” is large and multi-generational, extending well beyond the assumed nuclear composition of “parents plus children”. The 350 litres of free water is delivered to the plot, rather than the household per se. That a single plot accommodates large and multiple households is the norm rather than the exception in South Africa’s low-income urban settlements.(30) Consequently, 350 litres of daily water is grossly insufficient to meet the water needs of most plots. Even in ordinary circumstances, indigent households are acutely aware of their daily water consumption. Indeed, it is standard to view households queuing at 05:00 to fill buckets/bottles from the plot’s external standpipe before the valve closes at 05:30. Supplies are then rationed between households and stored for consumption and use throughout the day. The challenges are described by a backyard tenant:
“Every morning you’ve got to stand up early so that you could fill up your water bottles/buckets because you only get a certain amount of water per day. Even though the landlord charges R200 [approx. £8.60] per month for the water. It’s hard on us because I’m only allowed to fill four 3-litre bottles for the day – which is 12 litres – we’ve got to wash, do dishes and do washing, with 12 litres it’s extremely hard . . . Every night after we are done bathing, I use our bath water to wash our clothes.” (Single-parent household with two children aged 2 and 3, 11 February 2019(31))
The government message to wash hands regularly must be considered within this pre-existing context. While appropriate from a public health perspective, it overlooks the realities of limited and precarious access to water for the vast majority of low-income urban households, which are highly dependent on access awarded by those in control of water taps. In effect, the government’s advice on handwashing fails to acknowledge the differentiated access to clean water throughout South Africa’s cities. It also places the burden of compliance on households, without a concomitant commitment by the state to provide sufficient water. While the state responded by delivering communal water tanks in informal settlements (announced in the Cape Times newspaper in early April, about 10 days after lockdown started),(32) this “sticking plaster” solution fails to acknowledge the depth of water precarity within and beyond informal settlements. Notwithstanding the problematic provision of a resource that encourages communities to congregate rather than distance, it fundamentally overlooks the massive underinvestment in service infrastructure, and the inability of households to access services in both informal and formal low-income settlements. While coronavirus is a temporary pandemic, lack of access to water (and other services) is a permanent feature of life for many South Africans.
This example of water access highlights how pre-existing inequalities in accessing basic infrastructure can be exacerbated by the virus, and how the capacity to respond to public health advice is highly differentiated and often privileged. Crucially it demonstrates the need to provide local contextualization for global public health advice. Furthermore, as the virus spreads throughout areas with poor infrastructure, there is a risk that those unable to adhere to public health recommendations will be demonized for their inability to “choose” to prioritize handwashing over other water-based needs.
Social distancing and social grants
The WHO advice on social distancing to limit spread of the coronavirus has been applied in South Africa, initially through indirect measures, such as the ban on gatherings of more than 100 people as part of the pre-lockdown, and subsequently through a suite of more direct requirements such as full lockdown, curfews, and mandatory wearing of masks outside the house. For example, the president’s national lockdown speech demanded that “everyone must do everything within their means to avoid contact with other people”.(33) There soon followed news reports that soldiers were using violence (including rubber bullets and whips) to enforce social distancing amongst low-income urban dwellers standing close together whilst queuing for food supplies.(34) As with handwashing, the public health advice to remain socially distant from other humans is an ideal, not tailored to the actual living conditions of most urban South Africans.
The example of social grants is also relevant here. According to Stats SA, more than 17 million people, or one in five South Africans, depend on the government’s social welfare grants,(35) a figure that is expected to grow after the COVID-19 outbreak. Social grants, which are generally collected in person due to low levels of banking amongst the poor, are usually paid at the beginning of the month, but were moved forward two days because of the lockdown.(36) Consequently, social grant beneficiaries flocked to post offices, ATMs and retail stores on 30 and 31 March 2020, when the elderly and disability grants were paid out, and on 1 April for other social grants. They not only had to break social distancing rules, but also to disproportionately expose themselves to the virus by standing in slow-moving queues for hours. While in some areas social distancing was observed, in areas with high building density and limited open space, people could only stand in tightly packed queues waiting for their turn. Grant recipients, primarily those with increased vulnerability to COVID-19 fatality (i.e. the elderly, the disabled), also had to compete with others stocking up on groceries during the lockdown. The impossibility of maintaining social distancing in these situations again highlights the impractical nature of the government’s initial advice, which failed to consider the specificities of the South African context.
c. The practicalities of a lockdown for low-income households
On 24 March 2020, the president in his national speech called for a strict lockdown. Similar to the social distancing procedures, the practicalities of the five-week lockdown demonstrate the highly unequal ability of South Africans to comply. In this subsection, we describe the realities of overcrowded and high-density housing, as well as food insecurity.
Overcrowding and high-density housing
Due to the legacies of the apartheid system’s unequal access to the built environment, there is significant demographic and spatialized disparity in both the density and occupancy rates of housing structures in South Africa’s cities. In Cape Town, for example, centrally located low-density suburbs where large houses with spacious gardens accommodate middle-class nuclear families contrast with overcrowded high-density settlements on the city periphery, where often multi-generational households reside in cramped houses and shacks, cheek-by-jowl with other similarly high-occupancy housing structures.(37) In this context, the ability of household members to remain indoors and to socially distance from neighbours is highly uneven. Indeed, approximately half of South Africa’s population live in low-income housing, whether in informal settlements (13.1 per cent of South African households),(38) state-subsidized housing settlements (13.6 per cent)(39) or townships (24.4 per cent).(40) In all these settlements, a significant proportion of households live in (backyard) shacks, colloquially named “bungalows” or “hokkies”, which share perimeter “walls” and are built from brick, zinc and corrugated iron. Not only are neighbouring structures too close to satisfy social distancing requirements, but residents risk exposure to inhumane temperatures if they remain indoors (as non-brick materials magnify outdoor temperatures). Some of these pre-existing housing problems were highlighted by homeowners in a state-subsidized settlement in Cape Town (all quotes from March 2016).
“Here in the house is me, my wife, my daughter and son – we all stay in a one bed room. And outside I have three bungalows. I sleep in bedroom and my kids sleep in kitchen. It’s very crowded.” “My sister and husband died, so their 2 kids live here now. I had to make space for them. My son lives in the bungalow and the other two live with other people because these houses are too small … They didn’t measure the boundaries so the bungalows are on each other’s yards.” “This house is 27 sq m. Living here it is four adults (me, my husband, granny, my daughter); and three children (my kids). Someone is sleeping in front (lounge) because it’s not enough [space in the house].” “We had a fire at our house – in the house there were 3 adults (grandma, son, daughter-in-law) and 5 children. Then there were also 4 bungalows also destroyed by the fire; in those there were: a) 2 adults and 1 child; b) a couple and 3 children; c) a lady and 1 child; and d) a couple and 2 children. The fire spread so quick because we all live on top of each other.”
As these quotations demonstrate, it is common to have up to eight people living in a one-bedroom house, and multiple additional/extended households living in close proximity in the yard. Meanwhile, UN-Habitat defines overcrowding as anything over three people per habitable room.(41) Remaining indoors for five weeks and maintaining social distance from other households is impossible in these conditions, and the blanket government advice demonstrates a lack of official recognition of the realities of everyday life for those living in urban poverty in South Africa.
We do not contest the benefits of strict social distancing measures in curbing the pandemic, and the history of COVID-19 infections in South Africa has shown that in the initial stages of the pandemic, the spread was successfully limited. As Lippi et al. indicate, “In fact, such measures may be said to be a ‘necessary evil’ in tackling the COVID-19 pandemic”.(42) What we question is the overly simplistic nature of the global health advice in its blanket recommendation of a lockdown. In fact, the WHO is very clear about the health risks of overcrowding and states: “For communities, inadequate shelter and overcrowding are major factors in the transmission of diseases with epidemic potential such as acute respiratory infections, meningitis, typhus, cholera, scabies, etc. Outbreaks of disease are more frequent and more severe when the population density is high.”(43) Similarly, other overcrowded areas such as transportation, health facilities, shopping facilities, places where social grants can be collected, and basic services can be accessed (e.g. ablution blocks and standpipes) represent a concentration of germs.(44) Decisions about when and how to ease these measures require thoughtful attention to their effects on wellbeing, public health and the economy.
Food security and purchasing of essential goods during lockdown
Many people living in South Africa’s urban areas are food insecure. In Cape Town, for example, Battersby(45) found that 80 per cent of the sampled households in a baseline survey could be classified as moderately or severely food insecure. In the run-up to the lockdown, while the country’s wealthier citizens stockpiled food and other essentials to avoid having to leave the house regularly during the lockdown period, those with low/irregular incomes, no financial reserves and/or a reliance on social grants were unable to buy sufficient additional supplies. While lockdown regulations do not prohibit daily shopping, crucially, in urban areas the main catalyst of food insecurity is not unavailability, but households’ limited capacity to access food shops, which is directly related to income for both groceries and travel costs. In urban South Africa, low-income households typically rely on roadside informal traders and small-scale spaza shops that are dispersed throughout settlements for daily shopping, with larger trips to more distant supermarkets undertaken only weekly or monthly.(46) The informal food sector, then, is essential for the food security of the urban poor, and for their capacity to comply with a lockdown.(47)
In the early days of the lockdown, food security was thus severely threatened by a prohibition on informal food vending. Roadside sellers and small-scale and spaza shops were locked down, while the formal venues, such as supermarkets, registered spaza shops and food delivery companies, were allowed to stay open. For wealthier households, typically reliant on chain supermarkets, this was “business as usual”. For low-income households this was hugely problematic, particularly as it coincided with the cash-lean end of the month or week, the so-called “hungry season”.(48) While supermarkets have successfully penetrated many low-income areas, they are frequently incompatible with the consumption and food security strategies of the poorest households (e.g. their lack of electricity to refrigerate bulk items), and they typically require low-income households to walk long distances and/or pay for transport, both of which are problematic in the context of lockdown.(49)
Only after significant pushback from a range of stakeholders was the informal food vending system allowed to operate again under strict regulation – and even then only the small minority of vendors that had a permit.(50) On 6 April, the Government Gazette stipulated that all vendors of uncooked food items could operate, albeit subject to increased safety regulations and pending temporary permits. Even the temporary lockdown, however, had negative implications for the health and nutrition outcomes of already vulnerable households. In the brief period when informal food markets were prohibited, concerning trends were observed. For instance, many people in poor communities were unable to purchase fruit, vegetables, dairy and meat,(51) for two reasons: (i) the ability to reach only one shop, rather than visiting multiple shops and markets to make the most of a limited budget; and (ii) the need to focus on calorie-providing carbohydrates in times of hardship.(52) The shutdown directly threatened the food security and dietary needs of many South Africans, but also resulted in enormous loss of livelihoods among those working in the informal food sector (such as fruit and vegetable vendors).
While the government’s rapid U-turn on allowing some informal food vendors to operate demonstrates some capacity to respond of the realities of urban poverty, the original lack of knowledge on the daily lives of the urban poor and their food purchasing patterns was itself of grave concern. It again revealed the reliance of the South African government on global public health advice, and further demonstrated the problematic application of these global health standards without local adaptation.
Although actively responsive to the needs of the formal sector and those depending on social grants (e.g. by making grant collection simpler, expanding social grant coverage and relief packages for those in the formal sector that are affected by COVID-19), the South African government did not initially cater for the informal sectors of the economy, and to some degree the concerns have been ongoing. This has been an enormous shortcoming in South Africa’s COVID-19 response, with consequences that will likely deepen inequality in South Africa, including along dimensions of gender, income, and intergenerational and racial inequality. Around 2.5 million people, and around 30 per cent of the labour force, operate in the informal economy in South Africa, in every part of the labour market.(53) These include about one million domestic workers (mostly women), and a range of workers including carers (mostly women), farmworkers (around 650,000, most of them women), waste recyclers, transport workers, hairdressers and barbers, street and market traders, and home-based production workers. They may be self-employed or informally employed. They cannot earn a living if they are mandated to remain at home, and there are few options for support from the government.(54) For example, where the government arranged support for formal businesses in the form of payment holidays, with Unemployment Insurance Fund (UIF) funding for the unemployed, no provisions were made for those in the informal sector. As a result, poor households with limited or no income were most affected by the lockdown.(55) Many community action networks and soup kitchens were set up by local residents to support those in need through the provision of meals.(56)
For informal businesses in urban areas, the impacts are likely to be severe.(57) Informal spaza shops may have been eligible for a licence to continue operating, but most lacked the capacity to apply or to demonstrate eligibility. Yet in a context where mobility is limited, local shops are more critical than ever. These businesses and employees have been mostly unable to operate. Appropriate support needs to engage with the reality of informality. The spaza relief fund, for example, comes with strict formalization requirements. As du Toit and Mitlin have written, “It is a cruel paradox for informal entrepreneurs to have to formally apply for formal support for informal activities. Now is the time for government departments to engage with informal traders’ associations to co-design new approaches for this sector. Covid-19 is an opportunity in this respect”,(58) demonstrating the imperative for informal provision to be recognized rather than viewed as a nuisance.
IV. Conclusions
This paper responds directly to the potential of the COVID-19 pandemic to deepen existing inequalities. We focus on the differentiated societal capacity to transform everyday life in response to COVID-19, using the example of South Africa to highlight some of the specific ways in which being able to transform is a privileged ability.
Although to date no direct links have been established between inability to follow global public health recommendations and COVID-19 infection/mortality levels, in South Africa there has been a shift where initially the virus spread in wealthier neighbourhoods (as a direct consequence of European travel), but over time began to have a larger impact in low-income communities. This highlights the fault lines in access and care for those on the margins, and we have shown how some of South Africa’s COVID-19 responses could exacerbate existing inequalities. Specifically, we have shown that cramped living conditions and a lack of access to basic infrastructure that provides water and food hinder the ability of the often already vulnerable urban poor to transform their everyday lives and make behavioural changes in response to public health advice. This is particularly visible in relation to indigent households’ capacity to adapt to even to the most basic and essential hygiene requirement of increased hand washing. For households already functioning with extremely limited water, in which daily rations are eked out and reused, any decision to increase water use for handwashing has a direct impact on what is available for drinking, cooking, laundry and washing. Whichever of these uses households prioritize, the outcome is increased vulnerability to the virus and other health impacts. Similarly, high-density settlements and overcrowded housing severely hinder urban dwellers’ capacity to practise social distancing and remain indoors. The increased risk brought by the proximity of neighbours is compounded by the need to collect social grants alongside thousands of other South Africans, and to frequently visit local shops to purchase daily essentials. The government lockdown rules (including the initial closure of informal food markets) had an immediate impact on poor people’s diets, with longer-term implications, thereby further reducing peoples’ physical resilience to the virus. Furthermore, disaster response plans focused on protecting the economy have often failed to acknowledge the informal sector, which causes further harm to the poor given their reliance on the informal sector.
Two core arguments are put forward by this paper. First is the way state responses to COVID-19 have not only highlighted existing inequalities, for example regarding access to basic infrastructure, but also exacerbated these inequalities, for example in distorting access to food (closure of informal markets resulting in reduced diet quality) and water (increased demand on unchanged water rations). As the paper demonstrates, for those living in urban poverty in South Africa, where access to basic infrastructure (e.g. water, food) is limited, and where overcrowding and high density are the norm, it is frequently not possible to transform daily life in the ways required and expected by the state.
This points to the second core argument of this paper: that public health recommendations devised at the global scale, led by the experiences and capabilities of countries with for example robust tax bases, universal access to infrastructure and strong government, require contextualization. When the COVID-19 pandemic started, governments such as South Africa’s were following international “best practice” and WHO advice. Although in principle, this is excellent advice, in practice there are significant problems with compliance for many in South Africa. While each country implements public health measures with differing intensity (e.g. severity of lockdown), there has been a lack of specific attention to the needs of those most vulnerable (beyond health determinants such as age and pre-existing disease) in terms of their capacity to adhere to public health advice. Also neglected has been the capacity of different countries to support their populations in adhering to these core transformations necessary for survival. The examples presented throughout this paper indicate that broad public health advice needs to be adapted to the specific empirical context of each country, and that reproductions of Euro-American/East Asian narratives are not just inadequate, they are actively harmful.
While it is easy to criticize rapid-response public policy for overlooking the needs of low-income populations, it is much harder to recommend alternatives. Clearly, it is essential that more realistic advice be prepared, tested and provided for both COVID-19 and future pandemics, with strategies that are feasible for those living in cramped housing conditions where access to water and other basic infrastructure is limited. Specific, tailored practical supports (e.g. termination of water caps, fresh food subsidies, support for the informal sector) are urgent. It is vital that more participative processes ensure that policies intended to support populations do not unwittingly exacerbate marginalization. There is an opportunity here to draw on disaster planning and management expertise. Furthermore, there is an urgent need for global financial support to those countries (likely to be concentrated in sub-Saharan Africa) where the economic impacts of COVID-19 are aggravating the health impacts.
In concluding this paper, we stress two factors that are most concerning about the (highly predictable) ways a global pandemic exacerbates existing infrastructure inequalities. First, that public health recommendations have failed to be based on a recognition of these inequalities, and to adapt advice accordingly; and second, that even in a crisis of this magnitude, the needs of the urban poor, which extend well beyond this specific global pandemic, remain largely overlooked. For while COVID-19 is temporary, unequal access to infrastructure is a permanent feature of urban life for many. The uncertain resolution of this pandemic, not to mention the inevitability of future pandemics, presents an additional compelling reason for addressing this inequality.