
Abstract
The interim councils and medical workers operating in besieged cities in opposition-held areas of Syria have faced enormous challenges in providing services to citizens. Despite the extremely difficult operating environment, some semblance of organized government has been installed by anti-regime rebels, whose functions include provision of basic services. Data collected from interviews with interim councils and medical workers in four opposition-held areas suggest that despite the acutely constrained environment and overwhelming challenges, governance structures there demonstrate a degree of success in delivering basic services to civilian populations. Their provision of basic services constitutes more than a bargaining tool or legitimacy signalling, and is better understood as an integral part of revolutionary struggle. Although producing an objective picture of events on the ground is hindered by the conflict conditions and heavy propaganda, the Syrian experience of service provision under siege merits further exploration and has relevance for other conflict environments.

I. Introduction
There is a lack of empirical research on how local authorities, or any de facto governments, provide basic services to civilian populations under the extreme conditions of urban siege. This paper is based on data from interviews with interim council and medical staff in four besieged urban areas in opposition-held territory in Syria. These data were originally collected in 2016 for a separate research project(1) investigating first responders and civilian protection practices. This current paper is a preliminary exploration of the provision of basic services to civilian populations undertaken by the alternative forms of sub-national government that have emerged in Syria’s besieged cities. The work environment is probably the most dangerous and challenging in the world at present. In addition to frequent aerial bombing and use of proscribed weapons such as gas, these urban areas experience mass displacements of civilians; lack of food, fuel and water; and severe damage to infrastructure. There are critical shortages of materials and minimal access for international humanitarian agencies. The state of siege in Syrian cities has been prolonged and unparalleled, and the inhabitants have suffered the worst humanitarian deprivations of any population in modern times.(2)
In 2016, when our data were gathered, the Syrian opposition comprised various groups, some now defunct. Of the opposition groups, the National Coalition for Syrian Revolutionary and Opposition Forces (commonly known as the Syrian National Coalition – SNC) was the most significant. This umbrella group claimed to be the sole legitimate governing body for the opposition, but was based in exile in Turkey. The SNC established the Syrian Interim Government and the so-called interim Local Councils, which undertake some government responsibilities, such as education, healthcare and emergency relief in opposition territories. However, the lack of a centrally controlled political entity complicates governance and service delivery. As well, the political affiliations of the Local Councils fluctuate and their democratic underpinnings are somewhat rudimentary, as typically only the President and Vice-President of each council are elected.(3)
Many Local Council staff take seriously their responsibility to assist civilians. Revolutionary idealism appears to be a significant motivating factor as they consider this an integral aspect of their struggle against President Bashar al-Assad’s regime. The relations between these quasi-governmental offices and armed groups are contentious, overlapping and shifting, and there is no international agreement on how to distinguish an armed actor from an interim government worker. One result is a lack of international consensus on how to engage these interim councils, to support service provision, or even to provide humanitarian assistance, to civilians in rebel-held areas.
Within the besieged urban areas, the coordination and delivery of basic services are challenging for a variety of reasons: isolated geographical areas and blockades, lack of connection between different opposition-held territories, intermittent communications and financial support, destroyed or damaged infrastructure, and power struggles between armed groups. The overwhelming need for basic services is complicated by ad hoc implementation and a lack of planning. Under these circumstances, the distinction between basic services and emergency humanitarian relief becomes blurred. For example, under non-conflict conditions, the provision of emergency shelter or the clearance of rubble would not be considered a basic service, but in besieged cities these are fundamental aspects of the work.
The interim councils appear to operate with a large degree of autonomy. Their staff often present themselves as legitimate alternatives to the regime, with associations of service, resistance and sacrifice. They generally receive nominal salaries and some work as volunteers. The work environment necessitates close engagement with a wide range of stakeholders: armed groups, Civil Defence (the White Helmets), volunteers, local faith-based organizations, and other interim government offices and hospitals. The experiences within besieged Syrian cities provide insight into basic service delivery under extreme conditions. The international debate regarding support to alternative forms of local government in Syria for basic services, or any other type of support, has so far proved intractable. How external support can be provided is a separate question from whether it should be provided. In any case, interim councils and other non-state service providers operate with little consolidated international support, and what support they receive is highly politicized.
The opinions and experiences of government and medical respondents, presented here in their own words,(4) convey the lived realities and challenges of service delivery during siege. While conflict conditions prevent research methods as rigorous as the research team would like, obtaining the opinions of service providers in situ is a valuable endeavour that outweighs concerns about the paucity of data and lack of triangulation. Due to the research challenges, the findings reported in this paper are considered indicative and preliminary.
This paper is presented in eight sections. Following this introduction (I), an overview of relevant literature (II) and data collection methods (III) situates this research with respect to previous studies. The main body of the paper examines aspects of service provision (IV), inter-agency coordination mechanisms (V), specific challenges identified by respondents (VI), and the changes they would like to see in their work (VII). The conclusion (VIII) draws out some key themes emerging from the interviews. It suggests that service provision for war-affected populations should be more rigorously distinguished from mechanisms for cessation of political conflict.
II. Previous Research on Service Provision in Conflict and Siege
Siege is an extreme form of combat: described by Smith as “a process of political domination aimed at isolating an entire population as a means of imposing collective punishment on ordinary people”.(5) Living conditions under siege are an understudied aspect of modern conflict, and existing studies often focus on psychological wellbeing or emergency humanitarian relief. Less research has been done on the coordination and delivery of basic services in such conditions. Syria is the most relevant case for examining this, but research there is hampered by problems of access and insecurity.
This paper’s discussion employs the term “state”, although “quasi-state” or “nominal state” would be more accurate. Syria cannot be categorized simply as a failed or fragile state, and has descended into what de Rivero labels a “chaotic ungovernable entity”.(6) Significant (mostly urban) parts of the country are now territories where political authority is contested by various non-sovereign entities, including political wings of domestic armed groups and a range of international fighters. The term “fragile state” has been described as referring to “states that are unable and/or unwilling to fulfil basic governance functions”.(7) Many opposition-held parts of Syria, on the contrary, appear both able and willing to undertake some measures of service delivery, as well as other functions of government. This moves the debate far beyond discussions of greed and grievance as motives for rebel activity.(8) The evidence base regarding service provision in fragile and conflict-affected environments is generally scarce and lacking in rigour.(9) While there have been no objective assessments of service provision activities of the Syrian opposition, their armed activities have been accused of mismanagement and a lack of coordination.(10) It is unlikely that rebel groups’ capacities or motivations for coordinated service delivery outstrip their capacities for combat. But in opposition-held areas, the psychology of the “spirit of revolution” informs and strengthens identities and the armed struggle against the regime, and staff there feel duty-bound to assist civilian populations.(11)
The interim councils in Syria occupy a mutable area with respect to the literature on failed and weak states, and could be more accurately characterized as areas of limited statehood that function under intensely challenging conditions. Krasner and Risse note that “we know surprisingly little about…public service provision in areas of limited statehood…There is no linear relationship between service provision and the level of statehood or state capacity in areas of limited statehood.”(12) The exact nature of the relationship between interim councils and civilians in their territories is not well known, however much they claim to represent civilians’ rights, and gathering data on such a sensitive topic in situ would be impossible. However, it is possible to identify three interacting aspects of the social contract(13) in operation in rebel-held areas of Syria: the capacity of the state to deliver services (severely hampered), its political will to do so (often claimed as one goal of the revolution), and the expectations of citizens towards the state (currently unknown in any detail).
The Core Humanitarian Standard on Quality and Accountability,(14) the Grand Bargain(15) and the Humanitarian Accountability Report 2015(16) all call for greater recognition of the lead role of local organizations in humanitarian contexts. While Syria’s interim councils are not humanitarian organizations as such, they nevertheless fulfil many of the fundamental provisions of such agencies in supplying water, food and healthcare, which is particularly noticeable in the absence or limited presence of international actors.
For opposition-held areas of Syria, the issue of legitimacy is significant, particularly in relation to external actors’ rationale for withholding or providing support to the interim councils. It is unclear to what extent the opposition interim councils are providing basic services in order to bolster their legitimacy. Previous research indicates that armed groups fighting the state can increase legitimacy and local support through providing services and publicizing their humanitarian credentials,(17) and decrease the chance of spoiling (refusal to negotiate) and insurrection.(18) Insurgent organizations’ delivery of healthcare and social services increases the recruitment of other militants.(19) However, Brinkerhoff et al.(20) find a complex, non-linear relationship between perceived legitimacy and service delivery in fragile and conflict-affected states. Overall, there is no scholarly consensus on exactly how improved service delivery correlates with state legitimacy.(21) Mcloughlin(22) emphasizes citizens’ own perceptions of the functions and activities of basic service providers, and recommends a broad understanding of both legitimacy and service delivery. While opposition parties that also provide services have a greater chance of being involved in negotiations to end hostilities, and those negotiations have a greater chance of being stable,(23) this does not necessarily mean that the interim councils provide services as a bargaining tool to strengthen their post-conflict position.
There are precedents in Syria for the politicized withholding of basic services. Even before the civil war, the national government used the targeted provision of goods and services, particularly electricity, as a key mechanism to ensure political control and reward political loyalty.(24) The extent to which this pattern of favouritism may be replicated in opposition-held areas is not well understood.
Due to the highly politicized nature of international intervention in the Syrian conflict, there has been a lack of consolidated external engagement with the interim governance structures in opposition-held areas or recognition of the services they provide. The various actors in the international community have been unable to investigate or agree on the legal status of these structures. The interim council service providers therefore currently fall into a grey area: neither clearly state nor non-state, and not distinctly part of any state-building processes. This absence of international intervention or support occurs despite the stated humanitarian imperative: that saving lives in the short term should take precedence over solving complex political conflicts. By conflating armed insurgents with service providers, and humanitarian interventions with political and military interventions, the international community has missed numerous opportunities to adhere to any sort of humanitarian prioritization.
International policy discourse on these sensitive topics has been greatly influenced by the security focus of combatting terrorism and preventing extremists from taking power in Syrian territory. While the international community remains unsure what action to take, civilians and interim council staff are subject to the deliberate targeting of non-combatants and use of proscribed weapons. As a member of one discussion group states, “the regime, Russia and Iran are bombing everything: schools, hospitals, Civil Defence, and use internationally banned weapons: bombs, napalm and cluster bombs and do not abide by any international charters”.(25)
III. Research Methodology and Data Collection
The data for this paper come from 16 anonymous interviews and three focus group discussions with senior staff from Local Council offices and medical staff in four urban areas at the time held by opposition forces. (These were primarily in Aleppo and Eastern Ghouta; supplementary data were gathered in Madaya and Darayya. These latter three locations are all in the Damascus region.) The interviews were carried out in mid-2016 for a research project on Syrian first responders(26) by researchers from Afaq Academy, a Syrian advocacy and research organization headquartered in Gaziantep, Turkey, with support from the humanitarian organization Norwegian People’s Aid (NPA), and analysed by staff from Coventry University. The research framework was collaboratively designed by the three partners and the interview questions discussed extensively before data collection started. The partners agreed to focus on the perceptions of service personnel rather than civilians, given the specialized nature of the intended questions. Afaq Academy researchers were already engaged under a previous NPA project in Syria (“Conflict Preparedness and Protection”) and were experienced in data collection and storage, security protocols, information management and personal protection measures. The project management entailed particular challenges of coordination and reporting due to the extreme insecurity and the imperative to preserve the anonymity of both respondents and researchers.
Since the data were collected, the security situation in Syria has changed significantly in some areas, including Aleppo after it was retaken by regime forces. Information in the interviews therefore represents a “snapshot” of events and conditions at that time. All interviewees are referred to by code to prevent their identification. (A detailed examination of the ethics, difficulties of translation and objectivity, and data collection constraints in besieged areas is contained in the report on first responders.(27)) The scope of this paper extends only to findings from interim council and medical staff in opposition-held territories, and not from regime-held areas. We could not interview any recipients of basic services, due to the sensitivity of the data and potential security risks.
Groups on all sides of the conflict are accused of flouting international humanitarian law, committing human rights abuses and preventing civilians from accessing basic services. These groups include the regime and its allies and the various armed factions fighting them and each other. It was thus important during the research to avoid references to blame, right and wrong, civil war genesis and cessation, and so on, and to focus on service delivery and support to civilians. The questions from the open-ended interviews and focus groups addressed the scope and nature of work being undertaken, particular challenges beyond the ongoing insecurity, coordination issues, partners and networks, sources of support, organizational strengths, changes the respondents would like to see, and training and equipment requested. The researchers had considerable autonomy to pose additional questions as appropriate, but questions challenging opposition staff or opinions voiced in support of the regime would have compromised access to respondents. Data collection, then, had to balance the potential for objective rigour and an unbiased overview with the opportunity to obtain insights into the experiences and opinions of respondents in their own words. All quotations from interview respondents are given in italics.
IV. Implementation of Service Provision in the Opposition-Held Territories
A document(28) partly translated into English from the Ministry of Local Administration, Relief and Refugees (MOLARR) of the Syrian Interim Government provides insight into the organizational structure of the interim Local Councils. The three primary sets of stakeholders for provision of basic services are:
Military: Militias on the ground of various factions, sizes and affiliations; these are considered to be highly significant for work progress.
Civil: Complements basic services and local coordination, including the Governorate Council and its different bureaus, including: Relief, Service, Media, and Legal.
Medical: Active medical associations.
The interim Local Councils in opposition areas generally follow an organizational structure comprising seven separate bureaus under the leadership of the General Services Directorate, or General Authority (Figure 1).
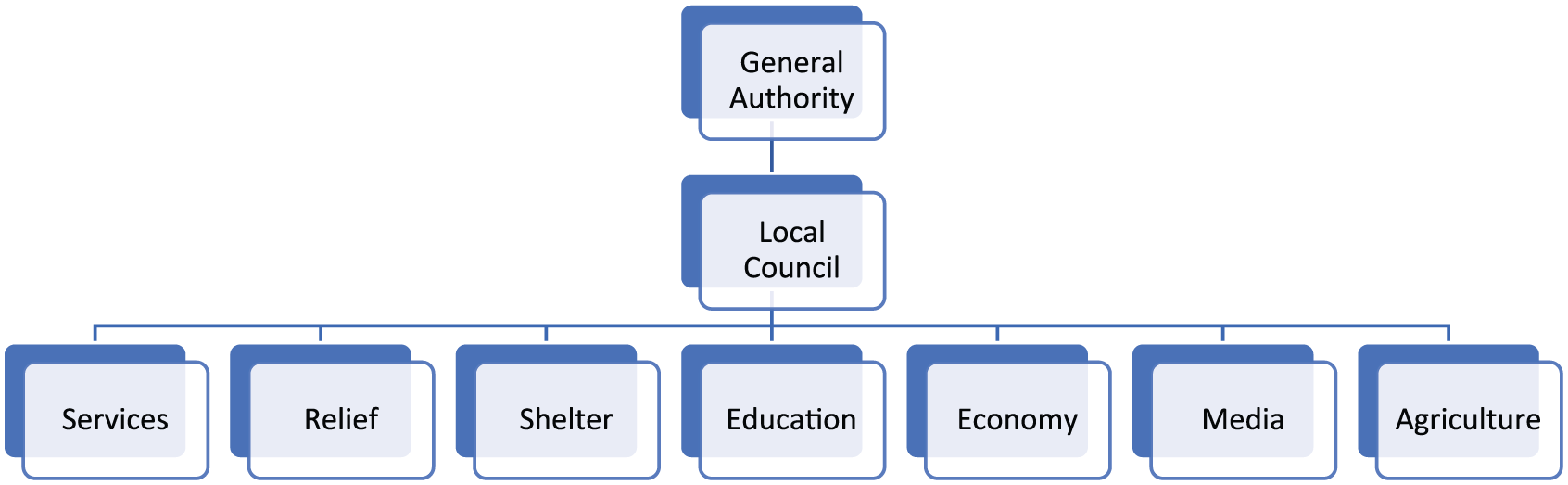
Basic structure of interim Local Council bureaus
A wide range of interim government sectors address aspects of service provision, including several non-military elements, although armed groups are listed first by MOLARR. The mechanisms of coordination and leadership across these various groups are contested and changing, and the numbers and types of civilians needing basic services in opposition-held urban areas are not representative of pre-conflict demographics. Those in dire need – the injured, disabled, chronically sick, elderly and children – far exceed the comparable peacetime numbers. Many younger able-bodied people have fled or been killed, and so service provision for this vastly altered demographic has to focus on emergency requirements and the needs of highly vulnerable individuals.
MOLARR identifies five priority areas of service provision:
For staff selection, the same council member clarifies, “after the head of the Local Council has been elected in coordination with the General Authority, he has to choose the offices’ managers who run the service, relief, educational work and others”.(32) The isolating effects of the conflict, whereby opposition-held areas are geographically separated, prevents large-scale programme implementation and consolidated delivery mechanisms. Service provision is undertaken in short timeframes and at a small scale. What follows is an overview of MOLARR’s five priority areas of service provision.
a. Food
The shortage of food, especially nutritious food, is a major challenge in the besieged areas. Staples such as wheat flour can be locally produced, stored and distributed, but there is a severe lack of specialized foodstuffs like baby milk that need to be produced in a factory: “we suffer from a lack of… food for children and infant formula”(33) and “we need children milk, vitamins and food improvers [sic] for babies”.(34) Children are repeatedly described as the primary victims of food shortages: “[due to] the ongoing war, many mothers and children suffer from malnutrition”.(35) Food availability and supply vary significantly across locations, and one doctor states that “there was no healthy food for the patients, for breakfast we gave them only jam, while for lunch we offered them rice or couscous”.(36) Yet the same doctor claims that “we offer the patients all that they need from food, drinks and medicine in these difficult conditions, from the moment after their operation until the end of the period of treatment…whether it is a day, a week or even a month”.(37)
The production and storage of nutritious but perishable foodstuffs like vegetables and fruit is highly problematic: “We don’t have any kind of healthy food or vegetables….People are eating unhealthy foods”(38) and “During the siege there is no healthy food for the [hospital] patients…even bread is impossible to obtain and there are no vegetables in the markets. Then what can we offer them?”(39) One Local Council member highlights the importance of safe storage: “Under this siege, we have to store more essential food supplies for at least three months. Unfortunately, people do not have enough money to buy this food and store it.”(40)
Price gouging appears widespread: “The majority of people are unemployed. Traders, unfortunately, are taking advantage of the situation and have increased the prices.”(41) The medical staff discussion group concludes, “after the siege, our choices and sources in food became very limited and it is very expensive for locals”.(42) Pessimism is evident in discussions about food: “civilians cannot protect themselves because there are no basic things of life, such as food”.(43) In response to the inflated costs, the Economic Office “buys food commodities and sell them to the people at a cheaper price up to 60 per cent”.(44) In response to funding shortages, the Local Council undertakes to “cultivate and reap crops and sell them so that we can cover the council expenses and distribute profits to the townspeople at a fixed rate per month”,(45) and various local agricultural projects supply additional foodstuffs.(46) However much the de facto local government assists in supplying food, civilians run a risk while obtaining it as “they still need to go outside to secure their daily needs for food”.(47) One discussion group of Local Council staff mentions their distribution of food baskets to displaced people, presumably from other opposition areas, who are referred to as “guests in our town”.(48)
b. Relief
The Relief Office claims to distribute “relief baskets” impartially to recipients “without considering whether they are rich or poor”,(49) but “has great difficulty getting aid for displaced people…because the goods are really expensive”.(50) It is not clear what is contained in these relief baskets.
Supplying potable water is a major challenge: “We need heavy equipment for electricity and water projects. We need spare parts necessary for water.”(51) “Another challenge is…finding sterile water.”(52) “[We] the council failed in digging more water wells to overcome the issue of water shortage.”(53)
A member of another council reports that “we need a lot of equipment and lighting…Water shortage is another challenge, we rely on well water…The main water network does not work in our town due to the lack of pumps and the destruction of a large section of the pipes and plumbing…”(54) It is not clear to what extent respondents distinguish relief activities from service activities, or how much these services reflect MOLARR’s priority areas.
c. Services
The Service Office deals with debris, street cleaning and drinking water supply. “It provides the heavy machineries and equipment to clear rubble, bring fresh water to the town, drill wells and install compressors to extract water that is used only for cleaning because the water of the town is contaminated and undrinkable.”(55) Several respondents refer to the need for additional water pumps,(56) and medical staff experience “difficulties providing the patients with filtered water in the case of water cuts”.(57) As one group explains, obtaining medically sterile water is a considerable challenge,(58) and requires careful coordination between the Local Council and Medical Offices.(59) Water is also required for growing crops: “we need to…dig channels to bring sanitation water to irrigate the agricultural lands”.(60)
Discussions of water shortages are often accompanied by simultaneous references to the lack of fuel and electricity, and respondents are highly aware of the interlocking relationship between these services. One Local Council, for instance, explains that the high price of fuel has left it deprived of electricity for five years, which means it relies on well water, as wells do not require electricity for pumping.(61) Council members identify the need to “provide electricity for the citizens who are paying exorbitant amounts for only three hours a day”.(62) As one group of medical workers laments, “we lack medicines and medical tools…but there is something else more important which is fuel. How can we continue without electricity all the time?”(63) One project researcher reports that the group meeting was held “in very cold and frozen weather in front of a wood fireplace”(64) due to a lack of alternative fuel.
Another major operational challenge is clearing rubble, which blocks access and compounds the difficulties of finding survivors after shelling incidents. Heavy equipment is lacking, although the Local Council staff can sometimes borrow diggers from the Civil Defence. “The Service Office provides heavy machineries and equipment that help us to raise the rubble, bring fresh water to the town, drill wells and install compressors to extract water.”(65) Due to the intensity of the fighting, “our office had new responsibilities and started to clear the rubble and prepare basements and shelters to protect the rest of the people who stayed in the town”.(66) One council worker claims that “we prepare underground houses to achieve the necessary protection for everybody inside the town”.(67) To enable surviving buildings to protect and accommodate more people, “we have to strengthen the ground floors…with layers of soil bags”.(68) As a result of the destruction, “there are families living in houses that are not suitable…unfit even [for] livestock in other countries”.(69)
d. Medical
Newborns, children, lactating mothers and pregnant women have urgent medical and nutritional needs. Vitamins, children’s supplements and baby milk are all desperately required, as well as many medicines and drugs. “We suffer from intense shortages of drugs and vaccines and we do not have medical clinics…this situation in the town caused specialist clinics to close and move to safer places outside the town, causing troubles for all civilians.”(70) Yet information can be inconsistent; according to the director of one Medical Office, “the clinic section consists of three clinics, well-equipped with the best medical equipment where doctors work in shifts covering all 7 days a week within a recognized programme agreed between all the medical centres, which include 10 specialists such as internal medicine, gastroenterology, children, women, bones, hernia, chest, general surgery, skin and physiotherapy.”(71) He also refers to the “free pharmacy which issues more than 700 types of medicine to patients free of charge”.(72)
The Medical Office “distributes milk cans to children from time to time”(73) and coordinates closely with the Civil Defence units. For patient transport, “the Medical Office has an ambulance that transfers the wounded to hospital during shelling [and] is used by people…to transfer their family members to clinics when necessary”.(74) Medical staff advise against focussing entirely on emergency medicine. For example, dentistry is also much needed, along with other non-emergency treatments, such as for hypertension and other chronic ailments. Staff also express concern over the health impacts of living conditions: “refugees live in underground houses in nearby towns, so we advise them to take their children outside and expose them to sunrays…to prevent asthma, shortness of breath and other diseases”.(75) However, emergency life-saving interventions are inevitably prioritized: “…we work in the calm days when there are just one or two raids by…warplanes or a few artillery shells, but when there is a significant escalation on the area, the hospital stops all operations and all the doctors and nurses mobilize to rescue the wounded people”.(76)
In Eastern Ghouta, the Unified Medical Office has drawn up a schedule for doctors to work in different hospitals and medical points, facilitating coordination. A doctor refers to experience gained during the years of siege: “we have a distinct medical staff and nurses who have long experience gained through revolution time [sic], which spanned five years. Most nurses in the hospital have been practicing this career since the beginning of the revolution so now they have a considerable experience in surgery and dealing with cases of amputations.”(77) Another doctor has a less optimistic view: “We need to increase the training of nurses so that they can work better to compensate for the absence of experienced doctors”,(78) as many of the trained doctors have fled or been killed. A doctor in another health centre likewise states, “We seek to add an emergency section…to develop nurses’ expertise”.(79)
In terms of patient type (civilian or rebel), one Medical Office mentions that “we receive both, because the attacks do not distinguish between civilians and armed people and we, as a medical aid organization, see our human duty to receive all, not to receive some and refuse others on the basis of their political party or whether they are armed or not”.(80)
e. Education
Bombing has almost totally destroyed the existing schools in the besieged areas, and this lack of physical facilities dominates discussions about education. “We replaced [schools] with basements and apartments…They need a lot of equipment and lighting, which we are working to provide.”(81) As in other sectors, staff routinely work on an almost voluntary basis: “The Education Office in the Local Council is responsible for providing all the supplies to…the only school in the town…[whose] teachers are sometimes given symbolic salaries”. The Directorate of Education in Damascus Countryside Province “provides a portion of the teachers’ salaries working in the town’s schools”(82) and “provides school supplies like stationery”.(83) A Local Council member explains, “We would like to develop the Education Office since it is the basis of the progress and development.”(84) In one town, all the schools have ceased to function except one, which now has over 1,500 pupils.(85)
One of the doctors, discussing the lamentable state of educational provision, says, “What is being implemented at school is only letting children play…without any real benefit”.(86) One Local Council member explains, “a large number of students drop out of school as a result of the harsh conditions of war and because parents fear to send their children to schools. In addition, there is a problem of child labour for school students whose circumstances forced them to leave school for a living.”(87) The accountant from one local NGO suggests that “education and protection projects [are more] important at this time than relief projects, [as] many organizations are working in…relief”.(88) Several interviewees explain that adult education is also required, especially for sector-specific training such as first aid.
V. Inter-Agency Coordination
The interviews overall suggest a significant level of coordination between different sector offices, along with the need to strengthen it. Given the lack of physical access and damage to telecommunications infrastructure, the coordination, at whatever level, across different sectors and between different offices is striking. This may be a reflection of the shared revolutionary spirit and the will to work together efficiently. Specific to Aleppo, “MOLARR established an emergency operation room with the participation of the Local Council [and] Assistance Coordination Unit… defining the essential needs and [to] secure a strategic stockpile of these needs to be sufficient for six months to face this potential siege and its consequences.”(89)
The closest coordination is in the medical sector, between different hospitals and medical posts: “there is a high coordination between all hospitals and medical points operating in Al-Ghouta, whether they are charitable, military or civilian”.(90) Another senior doctor explains, “we coordinate with other medical centres to see if they can give service to the patient. If one of the centres can, we transfer the patient to them. If not, we coordinate with the armed political parties to send them to the western sector [or] the patient can go to the capital under his own personal responsibility.”(91) As well, “The Ambulance Department in the hospital in coordination with the Civil Defence Department and the medical points operating in the hospital divided the area into sectors so that the ambulance system in the hospital is responsible for evacuating the wounded ones and the search for survivors under the rubble according to each specified area.”(92)
“There is full cooperation in the process of referring patients because we have sections that [other hospitals] do not have and vice versa. This process and connection is between all the administrative and medical staff.”(93) Doctors working in medical points “coordinate with medical centres to organize training and workshops”.(94)
There is similarly close operational coordination between the medical teams and the Civil Defence teams. One doctor highlights that “we consider [the Civil Defence] as complementary members of our work and we build a special relationship with them”.(95) A council member says, “the Medical Office cooperates directly with the neighbouring medical points and the Civil Defence point”.(96)
There are repeated mentions of the close working relations among medical services, Local Councils and armed groups. One doctor explains how “we document the names of patients, wounded, martyrs, number of visits…we do the documentation and data and send them to the Unified Medical Office in Eastern Ghouta”.(97) A Local Council representative explains how the staff coordinate “with Civil Defence centres and with the medical centres that are near the town to receive the injured…we also coordinate with medical centres of military factions because the town became the frontline and all factions have service ambulances and frankly, all factions help us and their cars are always under service and their nurses are alert to serve civilians during direct bombing”.(98) Another Local Council representative makes the same claim: “As for local organizations, we work with the Civil Defence forces, opposition parties, medical providers, and free police…to monitor the prices at the local market, we get in touch with opposition brigades… [and] the Civil Defence when we need to remove rubble.”(99)
The interview respondents express frustration with armed opposition groups, but also refer to their charitable behaviour: “The rebels controlled the fodder store…and sold its contents and gave the money to the Board of Trustees who have distributed…money to the people, in addition they built a school and medical dispensary [equipped] with first aid equipment and paid the salaries of the dispensary medical cadres. The rest of the money was given to the Economic Office that supplies the town’s agricultural projects with the necessary equipment.”(100)
VI. Specific Challenges
All respondents refer to repeated bombardment and the routine danger of death, but the siege conditions give rise to extreme operational constraints beyond the physical insecurity. Work challenges result from a lack of staff, destroyed infrastructure, transport difficulties and equipment shortages, as well as weak standing capacity of staff. Storage of goods and equipment is highly problematic, and there are huge fluctuations in availability of materials and foodstuffs. This leads to widespread use of provisional substitutes and improvisation, for instance with heaters, generator fuel and furniture. Secure protected warehouses for foods and other goods are lacking. Constructing them in scattered locations puts them less at risk, but compounds problems of access and delivery. Many respondents explain that they store items underground, which adds damp to other problems.(101) Machinery suffers from a lack of spare parts and fuel, and the need to reuse, repair and improvise is repeatedly mentioned.(102) Regarding the need to “establish enormous projects like preparing water networks and huge electrical generators to bring electricity for civilians”,(103) under current circumstances this is completely impossible and would only be feasible in an environment with a minimum of basic security established.
There is a severe lack of specialist medical staff, medical equipment and drugs, especially vaccines. Staff in one hospital explain that their main doctor was originally trained as a veterinarian and their two dentists have not graduated.(104) “We suffer from a severe shortage of…sterilizers, gauze, serums, balms and ambulatory supplies…but more important is fuel.”(105) “We are using the bed covers and pillows, because bandages are not available.”(106) “We have appealed [for] full vaccinations for children because they are not a party in the war.”(107)
Interim Council workers are paid irregularly and receive little remuneration, but in the besieged areas there is little paid work of any type. “Our workers receive only symbolic salaries.”(108) One fully trained doctor states, “since I was hired there has been no fixed salary…And it is always decreasing.”(109) “The head of the Local Council and…all the office managers in the council…are all working hard and free of charge to serve the people of the town.”(110) In many offices, people perform work they were not trained to do: “Inexperienced technical staff means we have to perform work that’s not within our duties.”(111) Cross-sectoral specialists are needed, particularly to develop medical skills such as first aid among the council staff: “We seek to send young clerks…to medical courses in specialist hospitals and emergency centres.”(112)
Although some small-scale international support does exist, respondents often refer to feeling totally unsupported and abandoned by the international community: “There is no real international body that supports us”,(113) “nobody supports us”(114) and “Our Local Council suffers – like other councils do – from the lack of support.”(115) In many interviews the respondents’ despondency and pessimism are tangible, not only due to day-to-day difficulties and dangers, but from the sense of being ignored by the rest of the world.
While most interviewees refer to their coordination as a strength, the lack of communications is highlighted as a constraint. “We need to find more effective ways to increase the communication between the council and its customers…[to respond to] customer’s complaints quicker and more seriously….We need to further our internal monitoring…[we need] quicker response and better communication between staff and officials…they have poor technical performance due to poor communication [which] impacted the performance of the council.”(116) Wi-Fi is sporadically available, but normally “we face the challenge of non-availability of the internet”(117) and “[our office] does not have modern communication equipment”.(118) “We suffer from difficulty of moving and communication…90% of the roads are out of use…During this difficult siege, we suffer big difficulties bringing medical equipment that the Medical Office needs.”(119)
VII. “What Changes Would You Like To See in Your Work?”
This interview question produced some of the most interesting responses. All respondents focus primarily on the cessation of hostilities, but many also refer to coordination and improved collaborative working practices. Other key responses draw attention to professional anxieties. Feelings of inadequacy and distress about the limitations on their work are palpable and emotionally wrought. “This is a huge question and you can write whatever you think… in such non-normal [sic] circumstances where everything is difficult.”(120)
A focus group of Local Council staff produced several suggestions: “[We need] effective cooperation among all medical institutions…implementation and support of joint service projects… the media to effectively coordinate and unify their efforts…Dialogue and cultural sessions to increase people’s awareness…We would like to modernize and develop work mechanisms [and] records to know all of our data.”(121) Another Local Council representative emphasized the need for improved inter-agency collaboration: “We need to have good and effective coordination with all the internal offices [and] with civil society organizations and other institutions working in the…besieged areas.”(122)
“We want to have administrative coordination between the Local Council members and other revolutionary institutions to improve the work…we need to establish new projects that enable us to achieve self-sufficiency during this blockade and the high prices.”(123) Similarly, “we need to develop the work through increasing the coordination with all the revolutionary activities”.(124) Medical providers refer to the need for improved “specialization in work, and separating administration and financial work”.(125)
Respondents repeatedly highlight the importance of learning from other urban areas and other professional sectors to develop their own work and organizational capabilities: “We aspire to have high coordinating [sic] with hospitals and Medical Offices in other liberated provinces to take advantage of their expertise…to develop ourselves with the benefit of their experience.”(126) “[We require] human and administrative development courses…in our town.”(127) “…to develop the administrative, financial, media and medical sector in the council”.(128) “…to modernize and develop the mechanisms of our work”.(129) “We hope to get technical and financial support to develop ourselves.”(130)“We hope that the international community takes civilians out [of] the conflict, brings the necessary medicine, achieves the modern medical devices…which help us treating the civilians.”(131)
VIII. Conclusions
Service provision under urban siege in Syria is an extreme case, but provides insights into government activities in an emergency setting, particularly at the municipal level. This conflict forces a re-examination of basic service provision in urban areas in the context of enormous deprivation. What regulatory and support frameworks should be developed to facilitate service provision in the future, and how can impartial humanitarian support be kept separate from the politics of civil conflict? More empirical investigations are required on the emergence of alternate governance structures in conflict, how they approach and implement service delivery, and the range of non-state actors’ roles(132) in these processes.
Despite research limitations in this environment, and even assuming that the responses we have are guarded, some key findings emerge from this investigation. Firstly, there is little indication that basic service delivery in the besieged opposition-held areas is undertaken primarily to increase local legitimacy, or to strengthen the position for post-conflict negotiation. These may be implicit aspects of the work, but are not discussed as explicit objectives. The range of activities currently undertaken to deliver basic services of various types are presented as more process- than goal-oriented. The provision of external support to Syria’s service providers should reflect this fact.
Interestingly, none of the interviewees refer to how local people perceive them or the work they perform. They seem to assume that local governance and service provision are perceived as taking place in partnership with the armed struggle. The responses often come across as earnest and somewhat idealistic. Both interview respondents and key informants outside Syria(133) present service provision for besieged civilians as an integral part of their revolutionary struggle. Yet this is coupled with intense weariness of the continued violence and destruction of life.
The need for improved inter-agency coordination and communications is mentioned frequently, second only to the need to stop the war. The medical centres and hospitals report closer collaboration than other sectors, but there are repeated references to the need for better coordination among armed groups, Civil Defence, interim councils and medical workers. The available data suggest that a reactive, responsive approach to service provision is widespread; respondents seldom refer to any contingency planning or preparedness measures to ensure continued provision of key services.
Given the illegality of urban siege as a weapon of war, the belligerents are unlikely to listen to calls for humanitarian access. But emergency service provision should be distinguished from attempts to cease political conflict. Although many respondents claim to receive no international support, others are aware of external financial assistance, particularly from Gulf state donors and international NGOs. Some institutions report having several donors, and others report having none. Staff morale would be strengthened if they felt more supported internationally, and if this support could be more standardized and equitable.
Given the manifold difficulties of providing basic services under such conditions, it may be unrealistic to suggest mechanisms to improve it. But some requests from interview respondents can be highlighted. They recommend that mitigation be approached at a communal level, with multiple sectors and stakeholders involved in the planning process. Sustainable and appropriate initiatives such as household agriculture and water storage could be encouraged to promote self-sufficiency. There are multiple requests from staff to develop their skills in human resources, administration and organizational management, and for better cooperation between civilian offices. Particularly at the city or municipal level, external assistance could be facilitated to support service providers while maintaining some neutrality from political efforts to halt the conflict.
Footnotes
Acknowledgements
Sincere thanks are due to the many respondents who gave their time to answer our questions under extremely difficult circumstances. We extend a huge thank you to the various researchers from Afaq Academy, to Ahmed Tannira and Mahmoud Soliman from Coventry, and to Norwegian People’s Aid.
Funding
This paper uses data collected for a separate research project titled “Civilian Protection in Urban Sieges- Capacities and Practice of First Responders in Syria”, funded by the UK Department for International Development (DFID) through the Urban Crises Learning Fund. The fund is part of DFID’s Urban Crises Programme, managed by the International Institute for Environment and Development (IIED) and the International Rescue Committee (IRC). The Grant Agreement Number is 719.10/13. Norwegian People’s Aid co-funded that research.
1.
Morrison, Chas (2017), “Civilian protection in urban siege: capacities and practices of first responders in Syria”, International Institute for Environment and Development working paper, London, available at ![]() .
.
2.
UNHCR (2016), “Syria conflict at 5 years: the biggest refugee and displacement crisis of our time demands a huge surge in solidarity”, 15 March, available at ![]()
3.
Aljundi, Ghias (2014), Local Governance Inside Syria: Challenges, Opportunities and Recommendations, Institute for War & Peace Reporting, London, available at ![]() .
.
4.
Although translated from Arabic into English.
5.
Smith, Ron J (2015), “Healthcare under siege: geopolitics of medical service provision in the Gaza Strip”, Social Science & Medicine Vol 146, page 332.
6.
de Rivero, Oswaldo (2001), The Myth of Development: Non-Viable Economies of the 21st Century, Zed Books, London and New York.
7.
Brinkerhoff, Derick W (2011), “State fragility and governance: conflict mitigation and subnational perspectives”, Development Policy Review Vol 29, No 2, pages 131–153, page 131.
8.
Vinci, Anthony (2006), “Greed-grievance reconsidered: the role of power and survival in the motivation of armed groups”, Civil Wars Vol 8, No 1, pages 25–45; also Regan, Patrick M and Daniel Norton (2005), “Greed, grievance, and mobilization in civil wars”, Journal of Conflict Resolution Vol 49, No 3, pages 319–336; Collier, Paul and Anke Hoeffler (2000), Greed and Grievance in Civil War, World Bank, Washington, DC; and many other works.
9.
Carpenter, S, R Slater and R Mallett (2012), “Social protection and basic services in fragile and conflict-affected situations: a global review of the evidence”, Working Paper 8, Secure Livelihoods Research Consortium; also Schuberth, Moritz (2017), “To engage or not to engage Haiti’s urban armed groups? Safe access in disaster-stricken and conflict-affected cities”, Environment and Urbanization Vol 29, No 2, pages 425–442.
10.
Heger, Lindsay L and Danielle F Jung (2017), “Negotiating with rebels: the effect of rebel service provision on conflict negotiations”, Journal of Conflict Resolution Vol 61, No 6, pages 1203–1229.
11.
Personal communication from several ex-Syria Civil Defence cadres during a workshop in Gaziantep, Turkey in February 2017.
12.
Krasner, Stephen D and Thomas Risse (2014), “External actors, state-building, and service provision in areas of limited statehood: introduction”, Governance: An International Journal of Policy, Administration, and Institutions Vol 27, No 4, pages 545–567, pages 546–547.
13.
17.
Flanigan, Shawn Teresa (2008), “Nonprofit service provision by insurgent organizations: the cases of Hizballah and the Tamil Tigers”, Studies in Conflict & Terrorism Vol 31, No 6, pages 499–519.
18.
See reference 10.
19.
See reference 17.
20.
Brinkerhoff, Derick W, Anna Wetterberg and Stephen Dunn (2012), “Service delivery and legitimacy in fragile and conflict-affected states”, Public Management Review Vol 14, No 2, pages 273–293.
21.
See reference 20.
22.
Mcloughlin, Claire (2014), “When does service delivery improve the legitimacy of a fragile or conflict-affected state?”, Governance Vol 28, No 3, pages 341–356.
23.
See reference 10.
24.
De Juan, Alexander and Andre Bank (2015), “The Ba’athist blackout? Selective goods provision and political violence in the Syrian Civil War”, Journal of Peace Research Vol 52, No 1, pages 91–104.
25.
Focus group discussion, Local Councils.
26.
See reference 1.
27.
See reference 1.
28.
Ministry of Local Administration, Relief and Refugees (2014), Emergency Plan to Encounter a Potential Siege on Aleppo, General Administration of Local Councils, Directorate of Development and Local Projects.
29.
See reference 28.
30.
Local Council 5.
31.
Local Council 1.
32.
Local Council 1.
33.
Medical Services 8.
34.
Local Council 2.
35.
Doctor 1.
36.
Doctor 2.
37.
Doctor 2.
38.
Focus group discussion, Medical Services.
39.
Doctor 2.
40.
Local Council 3.
41.
Local Council 3.
42.
Focus group discussion, Medical Services.
43.
Medical Services 1.
44.
Local Council 2.
45.
Local Council 5.
46.
Local Council 2.
47.
Doctor 4.
48.
Focus group discussion, Local Councils.
49.
Local Council 4.
50.
See reference 28.
51.
Local Council 3.
52.
Focus group discussion, Medical Services.
53.
Local Council 3.
54.
Local Council 1.
55.
Local Council 2.
56.
Focus group discussion, Local Councils.
57.
Doctor 2.
58.
Focus group discussion, Medical Services.
59.
Doctor 10.
60.
Local Council 2.
61.
Local Council 1.
62.
Local Council 1.
63.
Focus group discussion, Medical Services.
64.
Medical Services 8.
65.
Local Council Al-Shifuniyah.
66.
Local Council Al-Shifuniyah.
67.
Focus group discussion, Local Councils.
68.
Local Council Al-Shifuniyah
69.
Focus group discussion, Local Councils.
70.
Focus group discussion, Local Councils.
71.
Director of Medical Office.
72.
Director of Medical Office.
73.
Local Council 5.
74.
Local Council 5.
75.
Local Council 2.
76.
Doctor 3.
77.
Doctor 3.
78.
Medical Services 8.
79.
Focus group discussion, Local Councils.
80.
Director of Medical Office.
81.
Local Council 1.
82.
Local Council 1.
83.
Local Council 5.
84.
Local Council 1.
85.
Local Council 5.
86.
Doctor 3.
87.
Local Council 1.
88.
Focus group discussion, Masrat NGO.
89.
See reference 28.
90.
Doctor 3.
91.
Director of Medical Office.
92.
Doctor 3.
93.
Medical Centre 2.
94.
Doctor 1.
95.
Medical Centre 2.
96.
Local Council 5.
97.
Medical Centre 2.
98.
Local Council 2.
99.
Local Council 3.
100.
Local Council 5.
101.
For example, Local Council 2.
102.
For example, focus group discussion Local Councils, Doctor 3 and Local Council 2, among others.
103.
Local Council 2.
104.
Medical Services 1.
105.
Focus group discussion, Medical Services.
106.
Medical Centre 2.
107.
Focus group discussion, Local Councils.
108.
Focus group discussion, Local Councils.
109.
Medical Centre 2.
110.
Local Council 5.
111.
Local Council 3.
112.
Local Council 2.
113.
Local Council 1.
114.
Focus group discussion, Local Councils.
115.
Local Council 5.
116.
Local Council 3.
117.
Medical Services 1.
118.
Local Council 2.
119.
Local Council 2.
120.
Doctor 2.
121.
Focus group discussion, Local Councils.
122.
Local Council 1.
123.
Local Council 2.
124.
Director of Medical Office.
125.
Doctor 6.
126.
Doctor 3.
127.
Local Council 1.
128.
Local Council 5.
129.
Focus group discussion, Local Councils.
130.
Local Council 5.
131.
Focus group discussion, Local Councils.
132.
Twigg, John and Irina Mosel (2017), “Emergent groups and spontaneous volunteers in urban disaster response”, Environment and Urbanization Vol 29, No 2, pages 443–458.
133.
For example, at the post-project workshop in Gaziantep, Turkey in February 2017.