
Abstract
The article explains how the unprecedented pandemic management decision to lock down the country came about, using the case of Norway and drawing on unique interview material from political and administrative executives. Urgency and precaution were the government’s primary considerations in March 2020, with proportionality and due process only peripheral decision premises. Voices of moderation were drowned out at critical moments to pave the way for a lockdown. Moreover, Norway’s lockdown decision lacked distinct and official agency, with none of the key actors able to say precisely when, where and by whom this decision of unprecedented size and scope had been taken. An interpretation using Graham Allison’s analytical models shows that the rational policy model most accurately captures the case. The suggested implication is that when senior political executives take active control of an ultra-high-stakes process, decisions are unlikely to be the product of political resultants or organisational output.
Introduction
The article analyses crisis decision-making at the core of executive government, more precisely decision-making that resulted in a lockdown related to COVID-19 – the dramatic zenith of pandemic management during spring 2020 in countries around the world. We study the case of Norway, zooming in on the government’s decision on 12 March 2020 to enforce a historically unprecedented lockdown. Our interest is not in the effectiveness of Norway’s response to the crisis, rather, the question is what characterised the decision-making process resulting in enforcement of a lockdown. What characterised the activation process and the patterns of influence, and how was advice from bureaucrats and experts slanted towards political considerations?
Scholarship on government responses to the COVID-19 crisis has covered the expert advice going into (e.g. Cairney, 2021) and the regulatory decisions coming out of, the “black box” of decision-making at the core of executive government (e.g. Alemanno, 2020; Gaskell et al., 2020). Precisely how decisions on how to respond to COVID-19 came about has remained in the shadows. To fill this gap, this study offers an in-depth, qualitative study of crisis decision-making related to COVID-19.
Based on crisis management studies, we would expect to see a contraction in the authority of government to make decisions; political executives gaining greater power compared to legislators, civil servants and experts; and a shift in the balance between the bases for decisions, with political considerations becoming more influential and expert considerations less so (Boin et al., 2020; Kettl, 2004; Pierre, 2020). The expectation might well hold for most contexts, including countries with mature and well-functioning political and administrative institutions. Still, it is important to study the balancing between “chaos and order” in cases with some likelihood that decision-making in the run-up to the lockdown was rational, influenced by expertise and rule-bound. Norway is such a case, as the country was considered well-prepared to handle a health crisis prior to 2020 (Cameron et al., 2019) and received positive evaluations for its initial COVID-19 response (OECD, 2020; Plümper and Neumayer, 2020). Moreover, Norway has well-functioning government institutions that emphasise qualities that should be crucial when responding to a major crisis, such as protecting civil liberties (The Economist Intelligence Unit, 2019) and incorporating expertise in policymaking (Christensen and Holst, 2017).
To study Norway’s lockdown decision making, we analysed interviews and other data obtained by a government-appointed commission tasked with evaluating the Norwegian government’s response to COVID-19 (The Corona Commission, 2021a). A unique contribution of this study is the close study of leading politicians’, bureaucrats’ and experts’ situational interpretations, deliberations and interactions in the days and hours leading up to the decision to enforce the lockdown. Moreover, the research design suits our broader purpose, which is to contribute to the research agenda advanced by Dunlop et al. (2020: 6), connecting “detailed policy analysis which examines (…) the bureau at a granular level” to COVID-19 as an example of one of “the grand challenges of our world” today.
In terms of theory, Graham Allison’s “Essence of Decision” framework provides a structure for the analysis (Allison, 1969, 1971), enabling a nuanced and realistic interpretation of how rationality, bureaucratic politics and organisational processes play out inside the government’s decision machine when a major crisis occurs.
The article starts by outlining Allison’s framework, followed by background information on the political, bureaucratic and expert actors that occupy central roles in the case study. The data section and empirical study come next, closely narrating the timeline from 10 to 12 March 2020. This is followed by an interpretation using Allison’s models, and a concluding discussion. The final section contains a critical discussion of the study’s most surprising finding – the absence of distinct and official agency in the lockdown decision. Extraordinarily, none of the key actors could say with any degree of certainty who actually made the decision to lock down the country. A “shadow of hierarchy” (Scharpf, 1997) – essentially the Prime Minister’s shadow – hung over the decision situation, though. The case thus demonstrates the presence of hierarchy during crisis decision making, although not explicit, traceable, and overt control by hierarchical leaders.
Allison’s perspectives on decision-making in a crisis
The rational policy model’s basic unit of analysis is policy choices by the government, which is perceived as a rational unitary actor with a well-ordered set of goals and which takes decisions in a way that maximises value, selecting the highest ranking alternative in relation to the actor’s goals (Allison, 1969: 693–695). The actors involved in making a choice comprise a small number of highly positioned leaders, for example, cabinet members and top civil servants. Problems and solutions are well-defined in choice situations, with a rich supply of information. A close connection manifests between activation and definition (Christensen et al., 2020), meaning that hierarchical leaders control which alternatives are on the table and which course to take. This hierarchical control sometimes takes the form of leaders instructing subordinates in an explicit and formalized way; other times, subordinates anticipate leaders’ preferences without leaders needing to exercise power overtly (Ford and Zelditch, 1988). To Scharpf (1997), the latter type of control means that leaders influence subordinates through the shadow of hierarchy (see also Overman et al., 2021: 1762)
In the bureaucratic politics model, government decision-makers are not a monolithic group but rather participants in a competitive game, where the players are highly positioned politicians, bureaucrats and technical experts (Allison, 1969: 707–711). Government decisions are the outcome of such games. The players carry with them various organisational and personal goals, as well as their own views on which means will most effectively realise the goals. The fact that they occupy important positions and enjoy discretion from hierarchical instruction means that bureaucrats and experts are real participants in the decision situation, not just supporting actors for political executives. The basic unit of analysis is the outcomes of decision-making processes, viewed as the results of competition, bargaining and compromises. Decision outcomes sometimes reflect the dominance of one group and at other times the negotiating skills of the game’s participants and the weight of their arguments (March and Olsen, 1983). All the players have limited attention and capacity and therefore select issues that they think they can influence while disregarding other issues.
The organisational process model is based on the notion that actions and decisions in governments are organisational outputs (Allison, 1969: 699–702). The capacities and procedures of several specialised organisations constrain what the government can do to resolve a crisis. Agency derives neither from a monolithic actor nor from a set of heterogeneous actors with competing goals; it derives from a loose alliance of organisations “on top of which leaders sit” (Allison, 1971: 80) and do their best to coordinate. Using specialists means that complex problems can be parcelled out and resolved separately. It also involves exposure to the danger of so-called organisational parochialism or local rationalism (March, 1994). The political leaders have limited influence on which aspects of a problem each specialised organisation focuses on, which aspects it disregards, and which procedures the specialists apply to the problem. Specialised organisations use selective information and recruit members with similar skills and attitudes. Moreover, they develop alliances with, for example, actors in elected bodies and lobby groups. The organisational output is an enactment of pre-established routines.
To sum up, the three models provide different lenses through which a major decision in response to a crisis can be analysed. While “rational policy” focuses on the top political executive level, “bureaucratic politics” focuses on a wider circle of actors, and “organisational process” focuses on heterogeneous actors that do not interact much at all. Furthermore, while “rational policy” perceives the actors as a homogeneous elite, “bureaucratic politics” describes fragmentation in the governing elite, and “organisational process” describes heterogeneity combined with institutional autonomy and a lack of coordination. “Rational policy” predicts that decision makers will view the problem in a unified, rational way, with few information problems. By contrast, “bureaucratic politics” predicts negotiations, conflicts, compromises and diversity in information, resulting in boundedly rational action. “Organisational process” presupposes that each specialised organisation chooses its own path and acts on the basis of its own biased information, creating challenges of coordination. To interpret the case study, we answer questions relating to each of the models: • Rational policy: Did the political executives possess relevant information when deciding on a lockdown? Did they feel it was up to them to take control of the situation? Did the government display a united front in the run-up to the lockdown? How controlled was the influx of expert advice into the inner circle of decision-making? • Bureaucratic politics: What kind of heterogeneity existed among actors in the decision situation; what resources did they have and use? Did the political executives struggle to explain the connections between goals and means and the consistency in the decisions related to the lockdown? Was the lockdown a result of several loosely coupled decisions or one unified decision? • Organisational processes: Was the lockdown decision shaped by the actors in the decision situation following their standard operating procedures and local rationality?
Background
In 2020, Norway had a minority centre–right coalition government with Erna Solberg (Con.) as Prime Minister. The Ministry of Health and Care (MoH) has overall responsibility for controlling infections. It can issue regulations in accordance with the Infection Control Act and it manages public hospitals and government agencies. Following the WHO’s declaration of an international public health crisis on 30 January 2020, the MoH defined COVID-19 as a dangerous, large-scale and infectious disease in Norway, thus authorising the use of extraordinary measures in the Infection Control Act.
On 31 January, the MoH delegated coordinating the government’s coronavirus response to the Directorate of Health (DoH). During the first 3 weeks of March 2020, the DoH had extensive extraordinary decision-making responsibilities due to emergency procedures in the Infection Control Act. During an outbreak of a communicable disease it is the DoH’s remit to provide the government with policy advice, inform the population and enact mitigation decisions pursuant to the Infection Control Act.
The Act stipulates that the DoH should base its assessments on information obtained from the Norwegian Institute of Public Health (NIPH), a public sector research institute under the MoH and the national centre for expertise in infection control. The NIPH provides practical assistance, advice and guidance on infectious diseases and infection control to governments at local, regional and national level, medical institutions and the general population. Further, the NIPH monitors the national and international epidemiological situation, conducts research and is responsible for vaccine supply. During a health crisis that has been declared by the government, the DoH is hierarchically superior to the NIPH, and the NIPH’s advice to the government is filtered through the DoH and a pandemic coordination committee led by the DoH.
Norway’s first case of COVID-19 infection was registered 26 February 2020. At that time, NIPH expected “fewer than 100 cases the next 6 weeks” (The Norwegian Institute of Public Health, 2020). The 100-cases mark was passed less than 1 week later, though, and on March 8, NIPH projected that 40% of the population would become infected (The Corona Commission 2021a: 132). The number of registered infections grew rapidly through March and into the first week of April (about 1000 new cases per week), after which the first wave subsided. The infection cases were unevenly distributed across the country, with relatively high numbers in the capital Oslo and the neighbouring region Viken, and few cases elsewhere, particularly in peripheral Northern and Western regions (The Norwegian Institute of Public Health, 2022).
Data
The basis for our data is the government-appointed Corona Commission’s detailed account of Norway’s lockdown of 12 March 2020, and the process leading up to it. The 12-person commission was appointed by the government in April 2020. 1 The Corona Commission Act of 2020 secured the Commission access to any information it deemed necessary (§ 1) from government organizations (e.g. protocols from cabinet meetings and e-mails and text messages between government officials – “more than 23.000 documents in all” (The Corona Commission, 2021a: 39)). The act lifted the duty of confidentiality for government employees to “provide the Corona Commission with information needed for its work” (§ 2); it regulated the commission members’ duty of confidentiality (§ 3) and the Commission’s use of personal data (§ 4); it banned the use of information obtained under § 2 for criminal prosecution or civil lawsuits (§ 5); and it regulated the archiving of the Commission’s data (§ 6). In addition, the Prime Minister issued a duty to explain to the Commission for all government employees – including making themselves available for a formal interview (The Corona Commission, 2021a: 36).
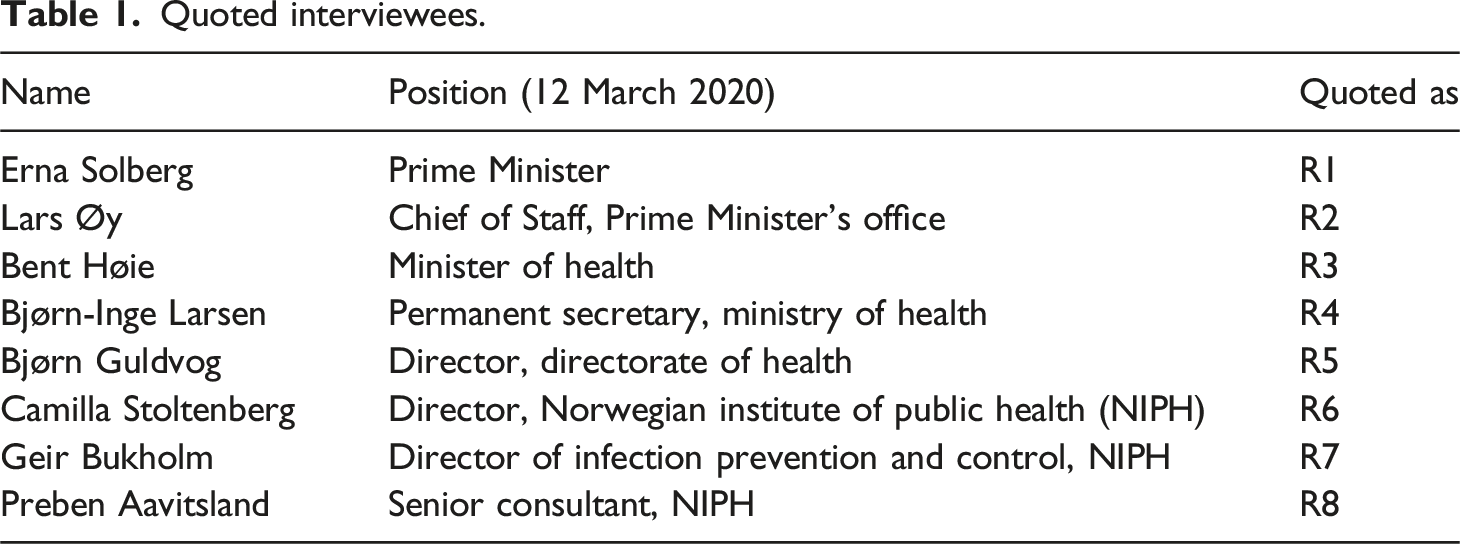
In April 2021 the Commission delivered its report (The Corona Commission, 2021a) describing and evaluating the Norwegian government’s response to the first wave of COVID-19 between February and July 2020. The report was 456 pages long and had more than 1000 pages of attachments. Our narrative of the March 12 lockdown is a concentrated version of the relevant parts this report, supplemented with evidence from the Commission’s interview material. The Commission interviewed 33 leading politicians and civil servants. The interviews took place in January 2021 with Commission members as interviewers and using an interview guide prepared by the Commission. The interviews were recorded and transcribed; the transcripts were read and approved by the interviewees. When the Commission’s report was released in April 2021, complete transcripts of the 33 interviews, more than 400 pages in all, were made available online for unrestricted access and use by, for example, journalists and researchers (The Corona Commission, 2021b).
Quoted interviewees.
Norway’s COVID-19 lockdown
Prelude: 10-11 March 2020
In the afternoon of 10 March 2020, the NIPH informed the Emergency Preparedness Committee for Biological Events (ECB) (a MoH-subordinate committee that advices the health authorities during communicable disease crises) that cases of infection had been identified that could not be traced to sources abroad. The NIPH considered the situation sufficiently serious to warrant using intrusive mitigation measures.
On 11 March, the Prime Minister met informally with the leaders of the political parties in the national parliament. The Directors of DoH and NIPH were also present and the DoH’s Director came away from that meeting with the understanding that the parliamentary leaders wanted the DoH to take stronger action to contain the spread of the virus (R5). The Prime Minister was also left with the impression that a united parliament urged the government to use stricter measures: “The unease I had felt was shared by the whole political community”, she said, alluding to unease about the inadequacy of the government response thus far (R1).
Later in the day, the Directors of the DoH and the NIPH discussed the situation again in a meeting of the Administrative Crisis Council (ACC) (the government’s highest bureaucratic coordination entity). The DoH’s Director encouraged the council members to propose mitigation measures, but the ACC members were not given any clues that a lockdown was to be effectuated the next day.
A meeting at 20.00 proved decisive for implementation of the lockdown on the following day. The MoH’s Permanent Secretary called the meeting that same afternoon, attended by himself, the DoH’s Director, and the Minister of Health, who had informed the Prime Minister that the meeting would take place. The Director of the NIPH was not invited because, according to the Permanent Secretary: NIPH “is not an executive authority in this scenario, [simply] a supplier of knowledge. (…) [NIPH] do not have a seat at the table when [the DoH Director] decides what the response is to be” (R3).
The purpose of the meeting was for the Minister of Health and the Permanent Secretary to hear what the DoH’s Director was thinking and to indicate that he had backing to implement intrusive measures. “The main theme of that meeting was the necessity to hit harder” in terms of migration measures (R3). Once the meeting was over, the Minister of Health received a call from the Prime Minister who urged decisive action. The Minister relayed “a clear message that significantly stronger measures would come the next day” (R1). Simultaneously, the DoH’s Director instructed a group of employees to put together a proposal for a package of measures that could be discussed the next day. At midnight, after an hour of brainstorming, the group emailed the Director a four-page menu of measures.
Other events that occurred on 11 March piled pressure on the decision-making process. These events included the WHO declaring the outbreak a pandemic and the European Infection Control Agency (ECDC) urging all countries to immediately introduce strict measures. Furthermore, the Danish government announced that all schools and kindergartens were to close and that government employees should work from home. “That did have an effect” on the decision process, said the Prime Minister’s Chief of Staff (R2). Denmark’s announcement reinforced the DoH Director’s conviction that it was necessary to do the same in Norway (R5). Also, using their powers according to the Infection Control Act, Oslo, Bergen, and other local governments had implemented local mitigation measures, for example, kindergartens and schools had already been closed or were about to be closed. Finally, several Norwegian newspapers published editorials on 11 March advocating stricter measures.
Lockdown: 12 March 2020
Early on 12 March, the Prime Minister’s Chief of Staff sent an email to the Minister of Health and the Prime Minister urging them to “press the big button.” The Chief of Staff, who was unaware the Prime Minister had met with the Minister of Health and the Director of the DoH the previous night, proposed a list of specific measures inspired by ECDC recommendations and by Italy’s experience. His reading of reports the Prime Minister’s Office had obtained from Norway’s embassy in Rome, was that “an incremental introduction of mitigation efforts caused confusion and frustration” in the population; that closing schools without mandating parents to work from home meant that “children were left in the care of grandparents” who were “vulnerable to serious illness” if they became infected; and that that Italy experienced challenges of coordinating the mitigation efforts of central and local governments (R2). Therefore, the Chief of Staff advised that Norway, instead of introducing measures incrementally, should implement multiple mitigation measures straight away. The minister replied that the measures the Chief of Staff mentioned “were on the list the DoH was working on” (R3).
At a meeting at 07.45, the DoH’s Director informed his management team that he had decided that the DoH should prepare a major package of infection control measures. He presented a list of topics the measures would concern. The NIPH’s Director was invited to the meeting with 1 hour’s notice and without being told what the meeting would be about. She did not make it to the meeting as she could not find a taxi in time (R6).
Immediately after the meeting, the DoH’s Director informed the MoH’s Permanent Secretary by phone about the measures the DoH planned to enact. The Permanent Secretary passed the message on to the minister, who was relieved to see that the package had “a scope similar to what we expected from the political side” (R3).
At 08.00, the NIPH’s Director arrived at the DoH’s premises for a scheduled ECB meeting and was surprised by what she saw: “There were people in meeting rooms writing lists of mitigation measures on the boards (…). I realised something was going on that we [NIPH] ought to take part in. I got hold of Geir Bukholm [NIPH’s Director of Infection Prevention and Control] and said I wanted him to get involved while I was at the ECB meeting” (R6). Bukholm was presented with the list of measures the DoH planned to introduce, and he forwarded this by email to colleagues in the NIPH, who were given 15 min to respond. He relayed that the NIPH supported most of the measures, but that they advised against closing schools and kindergartens and questioned the appropriateness of banning public events. However, the DoH staffers believed that all the measures were needed to suppress mobility. Bukholm said, “it was difficult to garner support for modifications. It appeared that the DoH and its Director had already made up their mind up about which measures to enact” (R7).
The ECB meeting started at 8.30 a.m. Immediately prior to the meeting, the Minister of Health emailed the Prime Minister’s Chief of Staff to say that he had asked the DoH and NIPH: “[W]hether we ought to introduce the strict social distancing measures nationally today. My position is that we should, but I must get their advice [first]. They know what I think, though.” (R3). In her own account, the NIPH’s Director never received that query (R6).
The Prime Minister and the Minister of Health participated in the meeting to “meet the people on the decision-making frontline” (R1). While heading into the meeting, the Prime Minister discreetly asked the DoH’s Director if this was the day they would “press the red button.” Although surprised by the Prime Minister’s wording, the Director “immediately understood what she meant.” (R5). He took her question as a sign of political backing and confirmed that they would indeed press the button; he said that the DoH would decide on forceful measures targeting many areas of society. During the meeting, the Minister of Health “passed me a note about pressing the big button,” said the Prime Minister. Her concern at this time was not the details of the measures: “Each specific measure was perhaps not that important to me. What was most important was to prevent people from meeting, thereby stopping the infection from spreading. (…). Assessing which measures were prudent would have to be up to [the DoH’s Director] Guldvog” (R1).
The DoH’s Director made his de facto decision on exactly which lockdown measures to implement while in the ECB meeting (R5). On the way out of the meeting, the Minister of Health, flanked by the Prime Minister, asked the DoH’s Director if it would be accurate to say that Norway was heading for “the most intrusive measures in peacetime.” The Minister wanted to shelve the button-pressing expression as that could “create an impression that the government can fix the problem by pressing a button.” (R3). The DoH’s Director confirmed that the Minister’s expression fitted the package of measures he envisaged. The phrase was then used by the Prime Minister immediately afterwards when she addressed journalists waiting outside the premises (Office of the Prime Minister, 12 March 2020).
At 10.30, the cabinet members received a text message from the Prime Minister’s Office stating that the Prime Minister would present dramatic mitigation measures at a press conference at 14.00.
The DoH’s list of mitigation measures was ready at 13.00. The Prime Minister, the Minister of Health, the MoH’s Permanent Secretary and the Directors of the DoH and the NIPH met to prepare for the press conference. The DoH’s Director presented the list of measures, following which there was a “review of how much disagreement there was between NIPH and DoH.” On the need for a review, the MoH’s Permanent Secretary said: “Everyone was aware that there was a disagreement between DoH and NIPH related to kindergartens and primary schools. (…) NIPH says that (…) the knowledge we have indicates that children and young people do not play a significant role [in the spread of infection], and that they therefore believe that we should not take that step. However, Stoltenberg said that that if that [closing schools and kindergartens] was the decision, [NIPH] would back it” (R3).
Norway’s 12 March 2020 lockdown.
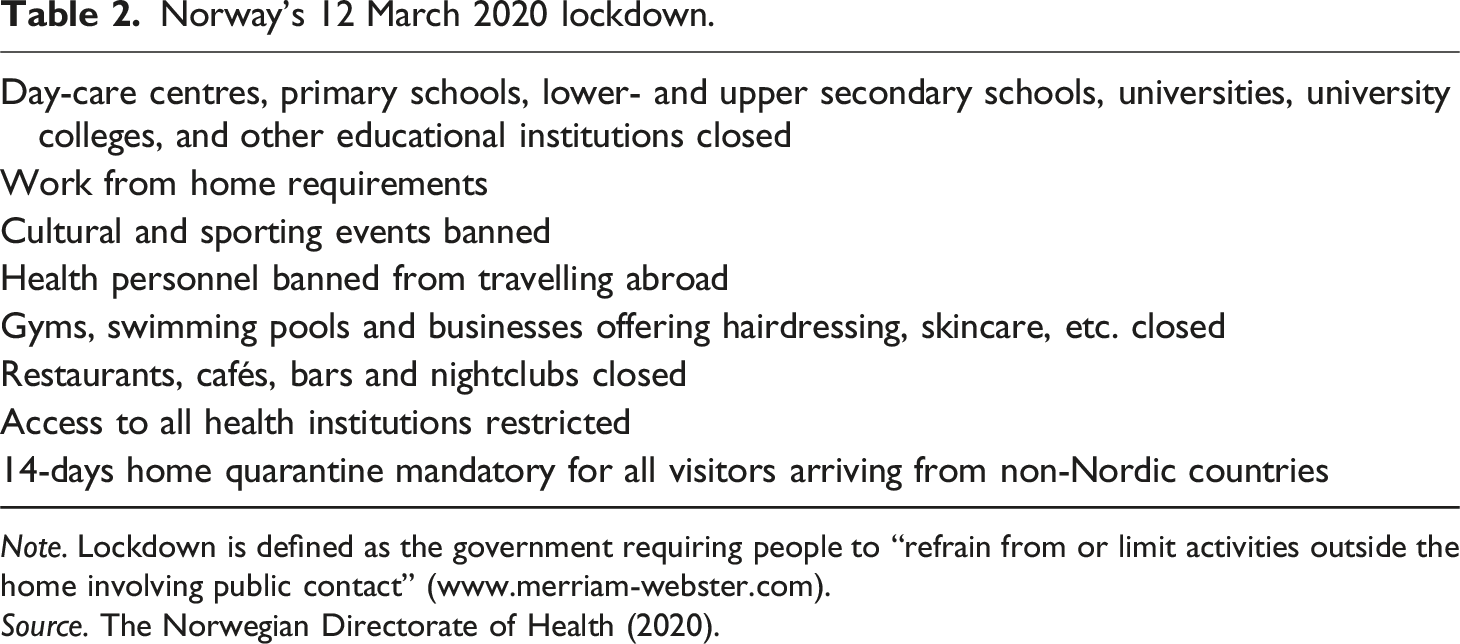
Note. Lockdown is defined as the government requiring people to “refrain from or limit activities outside the home involving public contact” (www.merriam-webster.com).
Source. The Norwegian Directorate of Health (2020).
Who made the decision?
The Prime Minister did not convene the cabinet on 12 March, and it appears to have been a conscious choice on her part that, using its emergency powers, the DoH rather than the cabinet should make the decision to lock the country down. The Prime Minister said: “We had given the authority to DoH and therefore depended on them making the decision” (R1). In hindsight, the Prime Minister demonstrated a pragmatic attitude to due process. She said: “It is possible the cabinet ought to have made the [March 12 lockdown decision]. It played out how it did due to time pressure, delegation and the system that was in place. But what is most important, I think, is that we gave [DoH] our backing [and showed] there was political agreement (….); that this [course of action] had the support of the country’s leadership” (R1).
In its evaluation, the Corona Commission argued that allowing such important decisions to be made by a body other than the Council of State constituted a breach of the Constitution (The Corona Commission, 2021a: 26, 147–148). The matter was raised in parliamentary debates in 2021, but it did not lead to any parliamentary consequences for the Solberg government.
When asked if he made not only the formal, but also the real, lockdown decision on March 12, the DoH’s Director replied: “That was my experience but (…) the government (…) can say that ‘as long as the DoH’s Director makes [policy] proposals that are in line with our expectations, we can allow the Director to continue to [shoulder] these decisions’. I could understand it, if the government said, of course they made the decision. They could have told me at any time that I could not proceed [with my plans for measures]”. (R5).
Answers from the other top executives varied. The Director of the NIPH said, “[i]t is still not clear to me” who actually made the March 12 decision (R6). The Prime Minister’s Chief of Staff said, “Formally, [DoH] made the decision. But they had very clear political backing.” (R2). The Prime Minister said, “The real decision was taken by the DoH. However, they knew at the time that we [the government] supported their decision.” She also said, “Clearly, our giving [political] backing for, and in a way pushing for strict measures, made it easier [for DoH] to cut through and do it.” (R1).
Regarding the urgency of the decision, the Prime Minister said, “The notion that this was something we could gradually adjust to, turned out to be wrong. (…) We had a novel, accelerating situation, which had to be handled there and then. (…) Sometimes you have to cut through and make decisions, even if [you] do not have the best foundation in the world for the decisions. Because not making decisions can make the situation worse” (R1).
Interpretation
Rational policy
Did the political executives have access to relevant information when deciding on a lockdown? In March 2020, the epidemiological and virological science concerning COVID-19 was thin, and the government’s expert bodies were drawing partly diverging conclusions from the evidence that existed. The lockdown decision was thus made on a thin and confusing evidence base. To improve their knowledge base, the political executives sought ad hoc to learn from others by eliciting supplementary information from neighbouring countries, international expert organisations and diplomatic stations. This emboldened the Norwegian executives and helped them suspend disbelief that “pressing the big button” was needed on their part. Of particular importance were Denmark’s closing schools, the ECDC’s recommending a long menu of measures to “flatten the curve”, and indications that Italy’s incremental approach to implementing measures was flawed.
Next, did the political executives feel it was up to them to step up and take control of the situation, as political leaders often do in a crisis (Boin and Lodge, 2021)? The answer is yes; Norway’s political executives clearly saw it as a prerogative and an imperative to try to take control of the situation, thus differing from, for example, their Swedish counterparts (Askim and Bergström, 2022). The Prime Minister and the Minister of Health, in particular, felt that it was up to them to rapidly force through whatever measures were necessary to make people stay at home, even at the cost of suspending normal and mandatory decision-making procedures, such as carefully assessing each measure’s proportionality. As the Prime Minister said, this was a time to “make decisions rather than engage in extensive studies and planning” (R1). The normal procedures that were suspended also included convening the cabinet and allowing the Directorate with the requisite mandate to make the de facto decision about the lockdown.
The political executives’ conception that it was up to them to take decisive action was exacerbated by their realisation that the government had failed to prepare a relevant plan for a government lockdown in the weeks prior. Although the idea had been floated in February that a lockdown might become necessary, no relevant plan had been prepared, for example, by involving the Ministry of Education in preparing a possible school closure. That the lockdown plan had to be virtually improvised by DoH staffers during the closing hours of March 11 chimes poorly with Allison’s rational policy model and it was a point of substantial criticism by the Corona Commission (2021a).
A next question based on the rational policy model is whether the government displayed a united front in the run-up to the lockdown or if disagreements surfaced. During 10–12 March, all the central government bodies spoke outwardly with one voice, including NIPH, which had the greatest expertise and which had reservations against important lockdown measures. Once the lockdown decision had been taken, the NIPH fell into line; it did not, for example, openly question the effectiveness and proportionality of closing schools. The political executives knew that the NIPH director was prepared stand behind a decision the NIPH believed to be unwarranted (R3). It appears that the political pressure the government exerted for a certain course of action made it practically impossible not to have a united front. The pressure was epitomised by the Prime Minister gathering the top executives in a “huddle” minutes before the lockdown was publicly announced – to iron out last-minute reservations.
How free-flowing or controlled was the influx of expert advice into the inner circle of decision-making? On certain topics, the NIPH’s advice deviated from that of the DoH and MoH, with the latter two aligned in a “hawkish” pro-lockdown position. This divergence was openly presented to the cabinet, to the parliamentary leaders, and to coordinating bodies at bureaucratic level. However, in the hours before the lockdown decision, the “doves” at NIPH were excluded and their advice drowned out. Bias was thus mobilised by means of organisation (Schattsschneider, 1960). Sacrificing a diversity of decision premises for the sake of unambiguity made it easier for the Prime Minister and her inner circle to reach a decision. At the same time, it does not accord with the rational policy model that the milieu with the greatest expertise was kept out of the loop at critical moments.
Bureaucratic politics
An initial question based on the bureaucratic politics model is what kind of heterogeneity existed among actors in the decision situation (March and Olsen, 1983). For a start, the actors in the decision-making ecology had different resources. The government’s political power meant that it could and did influence every actor and every step of the process. The main resource of the MoH’s Permanent Secretary was his proximity to the political level; his ability to direct the decision-making process relied on him acting as the extended arm of the Minister of Health. The DoH had an extraordinarily extensive decision-making capacity and retaining this resource depended on its Director listening intently for cues from the Minister of Health and the Prime Minister and following their preferred line of action. The NIPH’s resource was scientific and practical knowledge of infection prevention and having a broad international overview of the COVID-19 crisis. However, this expert body’s access to the inner decision-making circle was regulated by the Ministry and the DoH, and it consequently had less leeway for exerting direct influence on the decision outcome.
Next, did the executives struggle to explain the connections between goals and means and the consistency in the decisions related to the lockdown? In our interpretation, the most difficult communication task the government faced during these critical days in March 2020 was defending a wait-and-see strategy. The pressure for decisive action came from all sides, including from the political opposition, the media, local authorities, hospitals, outspoken medical doctors, and teachers’ unions. It thus seemed politically opportune to be criticised for doing too much rather than too little. The proportion of the population that trusted the government’s handling of the crisis rocketed from about 50% to 90% once the lockdown had been implemented (The Corona Commission, 2021a: 140). The general mood of fear, urgency and uncertainty made explaining the lockdown easy pickings; it was sufficient for the Prime Minister and the DoH to say it was necessary to suppress mobility and that showing precaution was of the utmost importance, without having to clearly justify the measures.
Was the lockdown a result of many loosely coupled decisions or a single unified and consistent decision? The March 10–12 process was undoubtedly under tight political control, with the Prime Minister and the Minister of Health omnipresent and well-coordinated. There were numerous minor decision points, but the political executives controlled the agenda by calling and participating in meetings and by eliciting information about conclusions reached in arenas where they had not been present. Consequently, even though decision authority had been delegated to the bureaucracy, the government had no problem in “sounding the dog whistle”, providing cues regarding which course of action they preferred and which they opposed and, if necessary, would put a stop to.
There were instances of disorder, with the DoH brainstorming a lockdown decision close to midnight and the NIPH being asked to comment on the lockdown package at short notice and well into overtime. However, this was not systemic chaos; rather, it was a hectic but still relatively unified decision process, with a constant stream of fundamentally consistent cues from the political executives and a deliberate drowning out of dissenting voices.
Organisational processes
Was the lockdown decision shaped by the actors involved in the decision-making following their standard operating procedures and local rationality? The Prime Minister’s sidelining of the cabinet short-circuited the involvement of most cabinet ministers and their associated ministries and bureaucratic “silos”. Authorities in the education, social affairs and employment sectors might have put their respective standard procedures to work if allowed, but their role was reduced to that of implementor in the period under study.
Within the health sector, three quite different bureaucratic organisations deployed their preestablished repertoires to factor problems, process information and define options: MoH, essentially a secretariat for the minister; DoH, essentially an implementing agency; and NIPH, essentially a highly specialised knowledge organisation. In any hierarchy, units are increasingly specialised the further down you go, and when a problem is elevated to a higher level, additional premises are added to the decision (Egeberg, 2012). Presumably, when shaping the response to a pandemic, the lowest-ranking and most specialised contributors to the decision-making process will only consider premises relating to infection control while those further up the hierarchy will add premises such as the capacity of the health system, adverse side-effects for vulnerable groups, restrictions on civil liberties, and costs to the economy. Due to organisational parochialism, Norway’s Covid-19 lockdown process saw deviations from this expected pattern. The DoH had a policy advice function alongside the NIPH, whose expertise was vastly superior. Rather than simply relaying the NIPH’s assessments directly to the MoH, the DoH added its own, slightly different, assessments. This illustrates Rubin et al.’s (2021) point that experts drew different conclusions from the limited knowledge base during COVID-19.
For its part, the NIPH took it upon themselves to consider premises that went beyond those pertaining to its expert knowledge. As a result, MoH and DoH executives felt that the NIPH had overstepped its role, whereas NIPH executives felt that the MoH and the DoH had neglected their responsibility to assess the adverse side effects of a lockdown. A leading expert at the NIPH said: “it is unresolved who is actually supposed to make proportionality assessments. (…) Is it our task … or the responsibility of those that makes the decisions? We chose to (…) assess the burdens the measures would cause; (…) someone had to” (R8).
Even though organisational parochialism did feature in this case, we do not interpret Norway’s March 12 lockdown decision as organisational outputs. According to Jones (2017), the organisational processes model has more purchase in explaining low-salience decision-making dominated by bureaucrats than high-salience decision-making dominated by high-level officials. Our study supports that argument. As has been made clear, once they had decided on a lockdown, the top political executives had little patience for anything that kept them from enacting it, be it due legal procedure, bureaucratic politics or, indeed, standard operating procedures.
Concluding discussion
In opening the “black box” of decision-making at the centre of the core executive, this study complements input- and output-oriented research on government responses to COVID-19. This crisis’ magnitude and character clearly made it difficult to handle in any system. In the words of Boin et al., the COVID-19 crisis “crept up on countries, cities, and hospitals. It arrived in full view, yet still surprised politicians, hospital administrators, pundits, businessowners, and citizens” (Boin et al., 2020: 117). Still, we have argued that Norway should be considered a case with some likelihood of rational, expertise-influenced and rule-bound decision-making in the run-up to the COVID-19 lockdown. In the light of this, the study produced some surprising findings. Urgency and precaution were the government’s primary considerations in the run-up to enacting a lockdown on 12 March 2020; proportionality and due process were only peripheral decision premises. The government’s crisis response epitomised a pragmatic approach, not a principled one (Boin and Lodge, 2021), and the case thus displays some features also found in other European countries’ COVID-19 experiences (Alemanno, 2020), only this time based on direct evidence and illustrated with quotes from political and bureaucratic executives.
The decision-making process was centralised, leading to a short-circuiting of a localized response regime (Askim and Bergström, 2022; see Troisi and Alfano 2022 for a counter example), and it was concentrated, with the Prime Minister and the Minister of Health keeping a tight rein on the process while the cabinet was on the sidelines – an unusual feature in Norway, where prime ministerial dominance is uncommon (Christensen, 2003). Political and bureaucratic executives were exposed to divergent views, reflecting a general dedication to knowledge-based policymaking (Christensen and Holst, 2017). However, at critical moments, voices of precaution and moderation were actively drowned out in order to pave the way for a draconian response. The study thus illustrates Yang’s (2020) argument that COVID-19 demanded that political executives trade evidence-based decisions off against effectively tackling time pressure, competing interests and difficulties in comprehending the situation.
More studies are needed into exactly how government responses to COVID-19 came about in different countries, including the level and form or involvement of the top political executives. In-depth evaluations in Norway’s neighbours Sweden and Denmark showed opposite patterns. Sweden’s government opted to leave active leadership of the crisis management during the first wave of COVID-19 to autonomous government agencies and subnational levels of government (The Swedish Corona Commission, 2022: 2). In Denmark, the decision-making process was even more concentrated around the Prime Minister than what was the case in Norway (Christensen et al., 2021). Our focusing on the first wave of the COVID-19 pandemic means, moreover, that the insights the study provides are limited to the period when the crisis “has burst into view and political attention has peaked” (Boin et al., 2020: 125). Most governments likely changed their mode of decision making when COVID-19 developed onto a “slow motion” crisis, the type of crisis that “wears out political attention spans, picking up speed again as societal and political stamina wanes” (Boin et al., 2020: 126).
Our theoretical interpretation of the Norwegian case study derived from Allison’s (1969) analytical models. Clearly, the limitations to the information base reduced the potential for rational decision-making. Still, the rational policy model was useful in interpreting the case. Senior executives deciding it is up to them to take action, the chain of command being actively guarded, and a collage of actors eventually displaying a united front, are all important facets of the case studied, and also key elements in the rational policy model. As is supplementing a weak evidence base by imitating others (Berry and Berry, 2017), which Norwegian executives did in keeping a keen eye on Denmark, Italy and the ECDC. Achieving a deeper understanding of the role of international policy learning in crisis responses is a promising avenue for future research on COVID-19 and pandemic management more generally (Sebhatu et al., 2020).
The bureaucratic politics model was useful in that it highlights key actors encroaching on each other’s turf. The organisational process model had limited purchase on the case. Our theoretical takeaway, echoing Jones (2017), is that in a high-stakes process like an unprecedented lockdown, with top political executives taking active control of the process, decisions are unlikely to be either the product of political resultants (as per “bureaucratic politics”) or generated by organisational output (as per “organisational process”).
On a normative note, contracting power and suspending normal decision processes may be considered necessary by those tasked to solve the crisis and avoid the “stuttering defense” image frequently associated with a creeping crisis (Boin et al., 2020: 119). However, from a democratic perspective, these tendencies are problematic; they challenge not only evidence-based policymaking but also democratic accountability (Boin et al., 2020). As a consequence of the in-depth research design, the study has found a lack of distinct and official agency in the lockdown decision. Surprisingly, none of the key actors could say with certainty who owned the decision to lock the country down.
It appears the “shadow of hierarchy” (Scharpf, 1997) hung so heavily over the decision situation that, in hindsight, the leaders themselves struggled to describe exactly when, where, and by whom a decision of unprecedented size and scope had been made. Despite their being in the thick of it, they simply could not tell, because the decision-making process was so opaque and convoluted. One could argue, similarly to the Prime Minister, that whoever made the lockdown decision was aware of the preferences among political and administrative leaders and that lower-level, non-elected officials acted under the supervision of hierarchy and – correctly – anticipated political preferences when they locked Norway down. That means that in one sense, the case demonstrates the presence of hierarchy, although not explicit, traceable, and overt control over the decision process by hierarchical leaders. Were it not for the Norwegian government’s after-the-fact allowing an independent evaluator deep access to document what occurred and how, voters would likely not have known that the political leaders dictated the process. Therefore, the “shadow of hierarchy” argument is no saving grace in a normative sense; it does not provide an answer to those who argue that explicit and documented political presence is critical to accountability and transparency. The “shadow of hierarchy” is certainly not a constitutional arrangement and it is not formal delegation. In the case of Norway’s COVID-19 lockdown, it would have taken some hours to assemble the cabinet, put proportionality assessments to paper, and relieve a Directorate of a decision mandate too heavy for a bureaucratic organisation to shoulder. It is likely that taking those hours would have cost lives, but it would have justified and legitimised the extraordinary measure that a lockdown represents.
Footnotes
Acknowledgements
The authors are grateful for comments to an early version from participants at the panel on “The Politics of Bureaucratic Crisis Coordination: Covid-19 in Hindsight” at the 2021 ECPR General Conference (30 August – 3 September 2021, Virtual event).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.