
Abstract
The sharing of information and feedback directly from service-providing staff to healthcare organisational management is vital for organisational culture and service improvement. However, hospital doctors report feeling unable to communicate effectively with management to provide evidence and affect improvement, and this can impact job satisfaction, workplace relations, service delivery and ultimately patient safety. In this paper, we draw on data elicited from a Mobile Instant Messaging Ethnography (MIME) study involving 28 hospital doctors working in Irish hospitals, to explore the barriers preventing them from speaking up and effecting change, and the impact of this on staff morale and services. We identify three major barriers, consistent with previous literature, to effective feedback and communication: (1) organisational deafness, (2) disconnect between managers and frontline staff, and (3) denial of the narratives and issues raised. We draw these together to identify key implications from these findings for healthcare managers, and suggest policy and practice improvements.
Keywords
Introduction
Just as evidence-based medicine (EBM) is the hallmark of quality clinical care, evidence-based management (EBMgt) is becoming an increasingly common model in the healthcare sector. The core premise of EBMgt is that “using better, deeper logic and employing facts…permits leaders to do their jobs more effectively” 1 One of the critical competencies for EBMgt in obtaining those facts is an openness to feedback from stakeholders, 2 and ensuring the flow of information and feedback directly from service-providing staff is a vital evidence source for evidence-based management and service improvement in healthcare. 3 However, many studies of hospital doctors’ workplace experiences indicate that doctors report being unable to communicate evidence and affect improvement, due to feelings of apathy and inability to effect change, or fear due to the potential professional and personal consequences of speaking up. This has been described in the context of the Irish health system previously, 4 but has also been reported in the UK, 5 China 6 and Australia. 7
Efforts have been made by hospitals internationally to establish communication channels8,9 especially around direct patient safety issues. But communication availability is not always communication efficacy in healthcare10,11 – for example, while hospitals may have established systems like staff feedback forums, suggestion boxes and reporting mechanisms, feedback and information provided by staff through these channels may not reach the right recipients to affect change, or may go unactioned or unaddressed after receipt. The struggle to speak out has been documented in health systems internationally, even during the recent COVID-19 pandemic where organisational intelligence from frontline staff would have made a vital contribution to policy and practice which required rapid and fluid responses. 12 Communication between doctors and management has been flagged as a key factor to healthcare organisational success. 13 Poor communication and engagement are identified as major barriers to workplace relationships, service delivery 14 and patient safety. 9
This paper explores the communication problems preventing hospital doctors from speaking up and effecting change, and the impact of this on staff and services, based on the experiences and perceptions of hospital doctors working in the Irish public health system. Drawing on a theoretical ev-idence base from management theories of voice and silence, sociological factors of professional identity and culture, and communication studies scholarship of organisational communication, it identifies key organisational voice issues and their drivers, and outlines the significant risks and consequences of organisational deafness, disconnect and denial for healthcare organisations, offering insights towards potential solutions.
Background
Employee voice refers to the various ways through which employees can have a say about, and influence, aspects of their work and their organisation’s functioning. 15 This paper focuses on communication from employees up to management, or upwards voice. Voice is a concept that covers a variety of practical manifestations. This includes formal feedback behaviours and channels (for example, in a meeting) to inform management decision-making, submitting suggestions through open mechanisms that actively seek feedback (like suggestion boxes or anonymous surveys), or filing complaints through official incident reporting and grievance procedures. It also includes informal feedback behaviours, such as making an informal direct request or complaint to a manager or supervisor, or complaining to colleagues or friends and family outside the organisation. It can also involve external feedback behaviours, like collective action and articulation of concern through unions, and whistleblowing or leaking information to external sources, such as the media or political representatives. 15 In this paper, we address both formal and informal voice behaviours and mechanisms, building on previous scholarship which focuses largely on the use of formalised feedback and speak-up systems.8,16
A good voice culture has been described as one in which opportunities to speak up are readily provided, broadly promoted and encouraged, and grievances and feedback not only influence management practices but are openly demonstrated to have been addressed. 17 Having good voice culture, practices and mechanisms has been shown to improve psychological safety, staff retention and job satisfaction, clarify workflows and responsibilities, and improve service quality. 17 However, poor voice culture and practices, and lacking or ineffectual mechanisms, lead to silence in the workplace; either out of an inability to deliver feedback effectively (acquiescent or apathetic silence) or an unwillingness to speak up openly (quiescent or fearful silence). 18 This silence risks employee dissatisfaction, disengagement and attrition, poor performance and service quality, and, in the case of hospitals, can have dangerous consequences for patients. 9
Methods
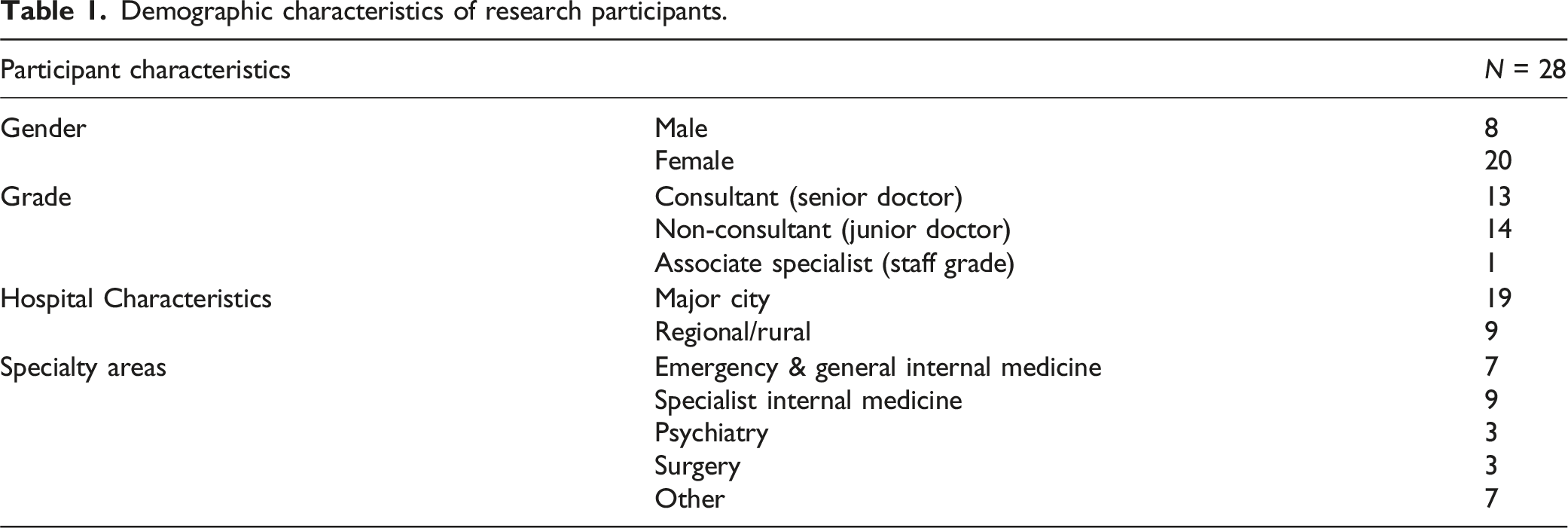
Demographic characteristics of research participants.
The MIME method has particular strengths for this research, as it is well suited to the everyday work communication patterns of doctors. 19 The method enables data to be collected over an extended period of time, instead of in an interview’s single moment in time, and can be relayed in real-time, or close-to-real-time, to events and interactions as the participant experiences them. It also allows for iterative and collaborative development and sensemaking of data. 19 The method does present some limitations to the potential findings; as text-based data, the message exchanges lack non-verbal cues, which may result in a loss of contextual information and may make it challenging to interpret the meaning behind some of the data. There is also the risk of self-presentation bias associated with online personas on social media, though every participating doctor was legitimately identifiable to the team within their professional capacity. Nevertheless, it offers a novel and unique way of providing rich, iterative and interactive insights into the day-to-day work experiences of these doctors, and the core issues with providing feedback and speaking up that they face.
An open call for participation was circulated on social media and online professional publications, through the mailing lists and internal communications of several Irish national medical training bodies and professional associations. Eligible participants needed to be currently employed in patient-facing roles in hospital care in the Irish public health system, of any specialty, nationality or professional grade. 28 participants self-selected to participate, and were assigned in roughly even numbers to one of three researchers. Participants were provided with detailed information sheets about the study, including guidelines about safe and productive WhatsApp™ communication, and electronically signed a consent form before participating. Participants were not offered any form of personal compensation for participation. Each researcher used a dedicated mobile phone and number for the purposes of data collection. A transcript of each WhatsApp conversation was downloaded from the mobile phone, and transcripts of interviews were generated and held on computer. All transcripts were de-identified, and sent to participants for final checking and approval. Ethical approval for the study was obtained from the Royal College of Physicians of Ireland research ethics committee.
To map key themes, similarities and variations across the large body of textual data generated within the MIME study, we utilised a codebook thematic analysis approach. 20 This approach is used extensively in qualitative health research for team-based research and large projects, and allows for the mapping of content across a dataset to uncover patterns in complex narratives and accounts. The researchers first familiarised themselves with the data by rereading transcripts, and inductively identified themes and sub-themes related to the topic of doctor-management upward voice, developing these into a codebook. Through an iterative process of discussing and agreeing on the themes which were most focused and relevant, one of the researchers [JPB] then coded the full dataset, applying these themes and sub-themes and looking for regularities and variations across the data. Another researcher [JC] cross-checked the coded data against the codebook and made additions and amendments in discussion with other researchers, and selected quotes that were most clearly illustrative of the identified sub-themes for use in outputs. All authors discussed these quotes and findings, and their foundations and implications, collaboratively to develop conclusions and recommendations.
Findings
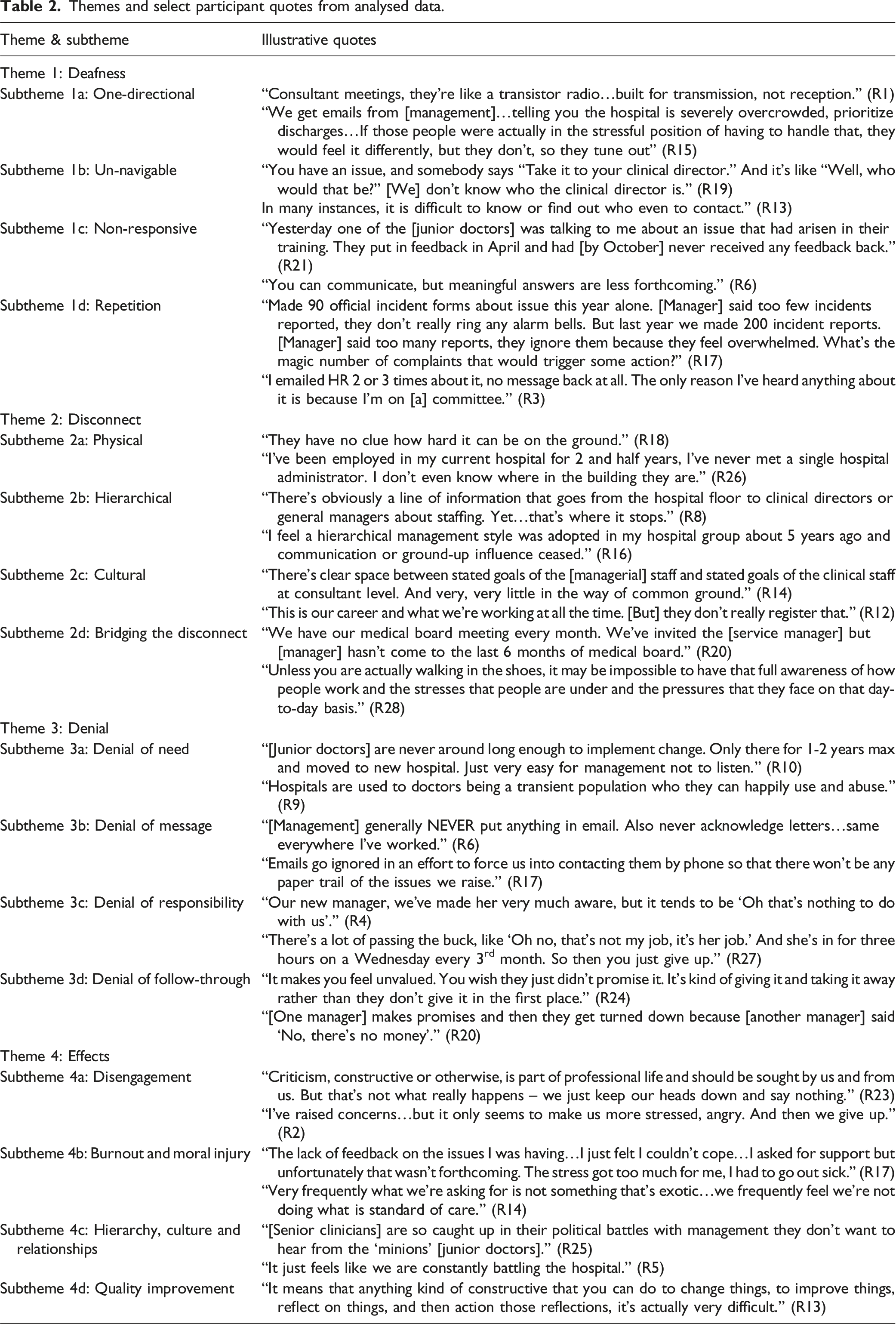
Four main themes were identified (Image 1). Theme 1, Deafness, incorporated sub-themes around the one-directional nature of communication, inability to navigate voice channels, lack of response, and voice repetition. Theme 2, Disconnect, incorporated sub-themes around physical disconnect, hierarchical disconnect, cultural disconnect, and attempts to bridge disconnect. Theme 3, Denial, incorporated sub-themes around denial of need, denial of message, denial of responsibility, and denial of follow-through. Theme 4, Effects, incorporated sub-themes around disengagement, burnout, hierarchy and culture, and quality improvement. Illustrative quotes in each theme and subtheme are detailed in Table 2. It should be noted that the interpretation of what “management” means in the context of participants’ words and experiences is subjective, referring to the participants’ own individual conceptualisations of who and what “management” entails for them, rather than any specific role, position or hierarchical model of healthcare management. Graphical representation of themes and sub-themes identified. Themes and select participant quotes from analysed data.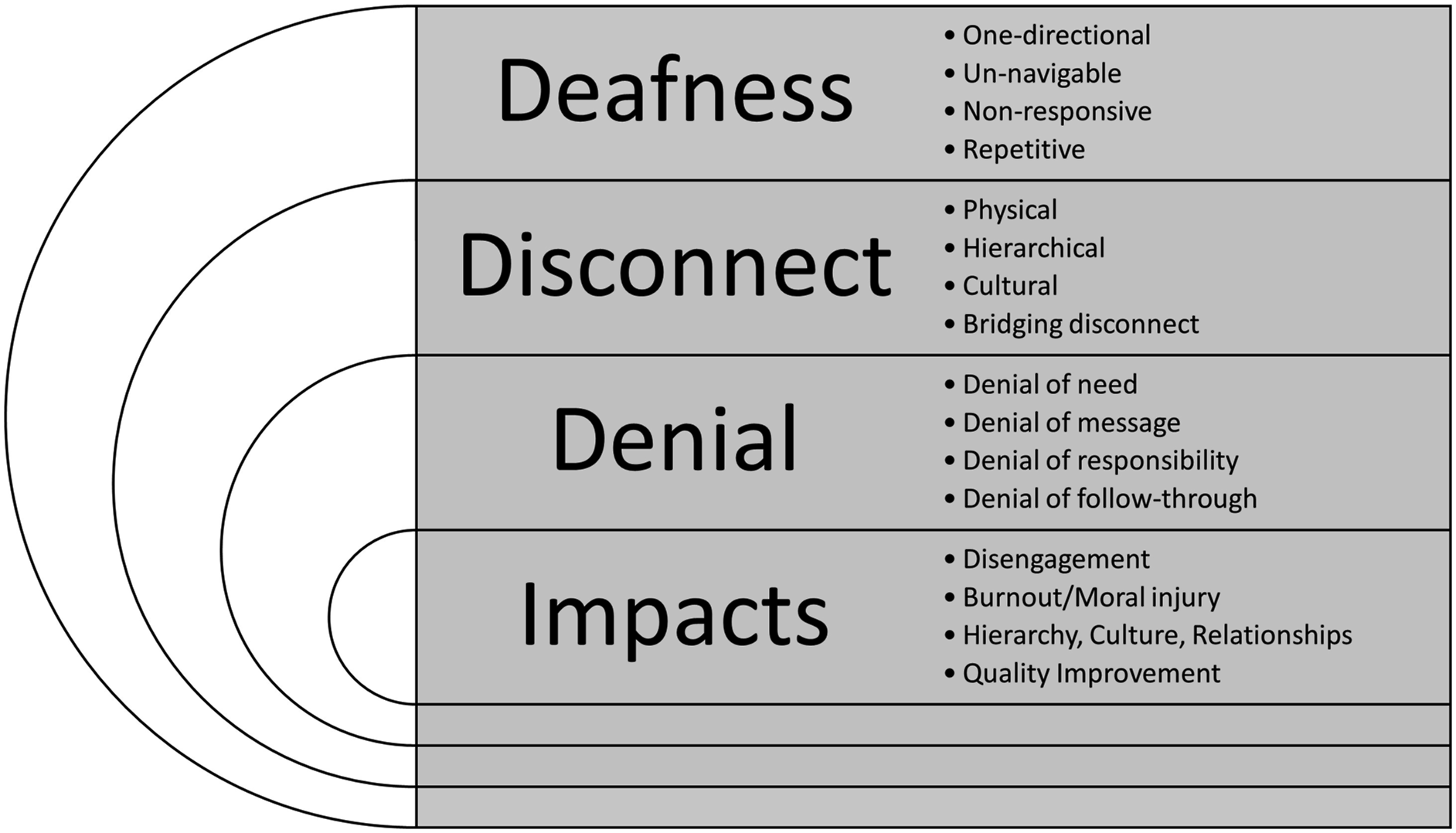
Theme 1: Deafness
Participating doctors expressed that communication channels in hospitals were predominantly one-way; management put much effort into giving doctors organisational information, but did little to receive it back – as one participant put it, like a transistor radio. Some participants described having no real meaningful systems in place for doctors to provide information back to management.
Others found pathways and channels to actively provide information to management, but these could not be effectively navigated because of inaccessibility, unavailability or a lack of clear responsibility. For others, communication pathways were provided and promoted by hospitals, in the form of feedback phone lines and web forms, meetings, surveys and staff fora. However, these systems often produced no response, or provided stock responses with no follow-up action, despite rhetoric from the hospital declaring these pathways were dedicated to listening to staff.
Some participants managed success, or at least a response, by repeating feedback through these channels over and over again, often on top of their regular workload and in their own time. The majority, however, reported simply giving up and finding workarounds for issues, taking on extra work or normalising problematic conditions for themselves, their colleagues and their patients.
Theme 2: Disconnect
Participating doctors also found that communication in the hospital suffered from a clear and ever-present disconnect between clinical and managerial staff. Often this manifested as a physical distance, since hospital managers were not present on the wards or departments or in clinical spaces, and so were not in a position to witness the issues doctors were communicating, and did not see the effects of issues on hospital staff or patients. In larger hospitals, or regional hospital networks, this physical disconnect seemed to be even more pronounced, as hospital managers and administrative staff were not located in the same building, or sometimes even the same town, as the clinicians providing patient care.
As well as physical distance, participants spoke of a cultural or ideological distance or disconnect between the two groups, who had different perspectives on the care delivery experience, seeing patients and staff in terms of numbers and flows rather than individual cases and experiences. They identified different priorities between clinical and managerial staff, such as their different ways of measuring performance (e.g., key performance indicators) or articulating needs within different frameworks. Doctors felt that management was disconnected from the experiential and evidence-based knowledge arising from direct patient contact, and that managers valued this below corporate forms of knowledge.
Some doctors spoke about making deliberate efforts to bridge these disconnects, physically and culturally. This included volunteering on committees arranged by management, inviting managers to attend clinical team meetings, and articulating their needs in managerial formats, such as via business plans. However, the different roles, responsibilities and schedules of the two groups often made mediation and understanding impossible, even when goodwill was intended and invested on both sides: for example, workloads prevented meeting attendance, or business plans were not able to be actioned by the relevant department
Theme 3: Denial
Many participants complained that, if and when they managed to communicate with management, their concern was denied, diluted or dismissed by management. Some reported that responses they received from management denied that the need identified by the doctor was a priority or that it would benefit the patient, the department or the hospital. This was particularly a problem for issues relating to working-conditions, and those relating to locums or junior doctors on short term employment contracts. Other doctors reported that, although they had made reports or supplied feedback or information, managers sometimes denied that a key piece of information had been received, sending the doctor back to repeat their enquiry or collate their feedback over again. This relates to deafness, as outlined earlier, though it also represents a shirking practice by actively pushing the responsibility for successful communication back onto the doctor.
Some doctors reported that, with the complexity of hospital administration and management systems, when they gave feedback to a specific individual within their management or administration network, they were often met with a denial that the receiving party was responsible for the issue at hand. They reported that responding managers, management divisions and committees often directed the doctor to another party or team within the organisation to give their feedback to, but these third parties often pushed the doctor back to the original feedback recipient, or onto yet another part of the organisation or system. Ultimately, for many participating doctors, even when they managed to navigate the organisational feedback system, give their feedback and have it received, and obtain an appropriate response or action that is agreed to by their managers, that action or follow-through could still be overruled and denied by other parts of the organisation.
Theme 4: Effects on staff
Battling this deafness, disconnect and denial had a serious negative effect on doctors who had become disengaged from their management and disinclined to engage in further communication or healthcare improvement work. They physically avoided managers or administrators where possible, and disengaged from committees or other similar roles. The constant and ultimately futile fight to have their feedback heard (never mind actioned) and improvements made gave rise to poor psychological wellbeing and, for many, led to burnout. It also sometimes caused moral injury, feelings of distress when being forced to perform and witness behaviours that go against personal and professional values and morals, where they saw their failure to be heard manifest in compromised patient care and safety.
Interpersonal relationships in the clinical environment suffered – not just poor relationships between managers and doctors, but worsening peer-to-peer relationships between doctors and their juniors or seniors, other members of their multidisciplinary teams, and non-clinical colleagues in the hospital. Poor communications and interactions between management and doctors, even in so-called “flat hierarchy” models where there are fewer levels of middle-management between executives and frontline staff, also seemed to negatively reinforce hierarchies as staff build their understanding of the way that power manifests within the organisation on communication dysfunction. They also reinforce the less helpful and less desirable cultures of the organisation and the profession by being deaf to or denying attempts to challenge them, normalising and entrenching the cultural status quo. Lastly, a poor culture of voice makes for a poor culture for improvement, not only by making improvement challenging for doctors to call for and action, but actively deterring them from following management-driven improvement initiatives.
Discussion
The stories shared by participants around their attempts to communicate with healthcare management and address identified needs to initiate service improvement reflect a system beset by dysfunction — both in terms of healthcare practice and systems of labour. Drawing from a sample of doctors across different grades, specialisations, locations and hospital types, our findings raise many issues that cannot be simply dismissed as “other hospitals’ problems” — these issues echo those in healthcare organisations and systems around the world.6,7,12 Admittedly, under-resourcing and weak staff retention present particular challenges in a strained health system like that in Ireland, and there are often higher volumes of sick patients, and sicker, more complex patients, than are allowed for in standard service framework calculations. 21 This goes partway towards explaining why there are problems, and why often management and administrators cannot give doctors what they want. But it does not explain why deafness, denial and disconnect are the standard response.
One main reason is the different logics about what drives healthcare work and role definitions and lines of peoples’ responsibility. Doctors are driven by the scientific theory, detail and application of their professional knowledge base, with a goal of providing healing, for which they are ultimately responsible. Managerial and administrative staff conversely are driven by organisational performance and hard market imperatives (e.g., KPIs), with a goal of keeping the service or system functioning and financially stable, and this is where their bottom-line responsibility lies. 22 At play are also different professional identities and cultures, which bring about a sense of tribalism and internal solidarity through external antagonism. 22 This all reflects wider trends in the way health and social care, particularly organised healthcare, is run and governed, the “separation of hand and brain”, 23 and the general de-professionalisation of systems 24 under a neoliberal capitalist model of public services that exists in many countries.
Implications for healthcare managers
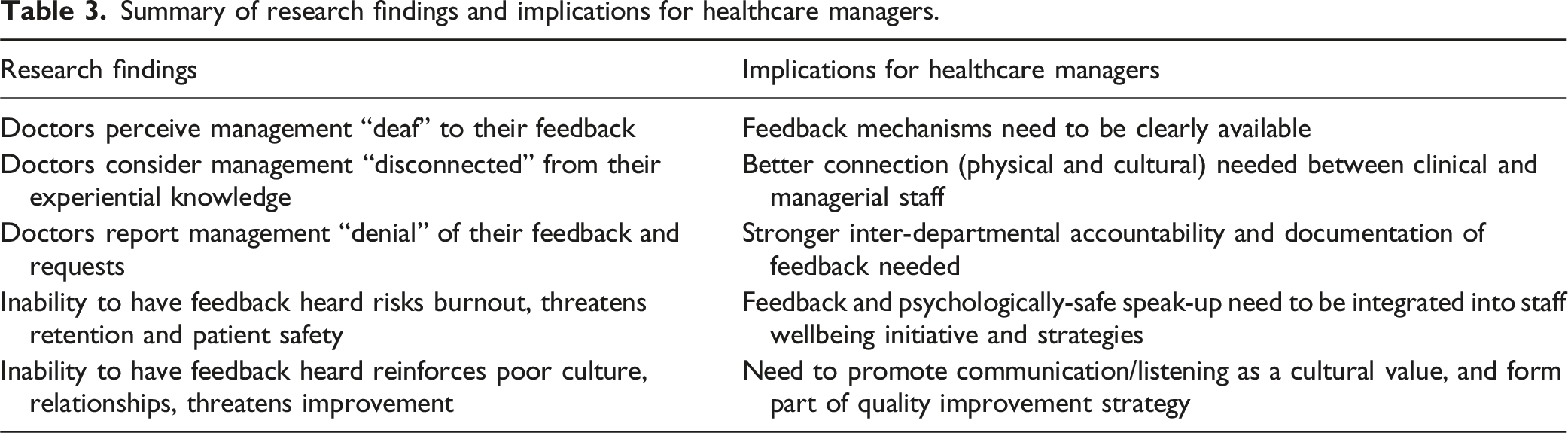
Summary of research findings and implications for healthcare managers.
Organisational deafness also poses a risk to the psychological safety of staff. Psychological safety, defined as “an interpersonal climate in which individuals feel able to take interpersonal risks without fear of negative consequences”, 26 has direct implications for patient safety. Hospital environments with climates of poor psychological safety, as reflected in our findings, have correspondingly higher levels of critical patient safety incidents, as errors cannot be effectively reported, detected and prevented before patients are harmed. Low psychological safety also has secondary effects of poor organisational learning and staff satisfaction and wellbeing. 26
Without the ability to connect with the process of work, or how the process should be, or to have their creative and quality improvement input heard, doctors are experiencing a sense of alienation. 27 On a practical level this alienation negatively affects engagement, intention to leave and intention to implement policy. 28 On an emotional level it causes feelings of powerlessness and meaninglessness, loss of hope, emotional separation and emotional damage. 29 This is made worse, arguably, because as a profession, doctors’ work identity is also so strongly a personal identity; the “medical self”. 30 Hence the emotional damage can fill the total life space; this may lead to low morale, job satisfaction and burnout, which has implications for doctors individually and collectively, and for the profession as a whole.
Thus, effective feedback mechanisms matter —to quality and safety and effective integrated care, and to retention and staff wellbeing. Mechanisms for upwards and sideways voice, feedback and inputs must be established and then barriers to their effective use must be identified and removed through change in policy and practice at a local, organisational and institutional level. In addition, listening must be paired with action. Doctors and managers need to be encouraged to reach a better understanding of each other’s “worlds”, observing each other’s spaces, priorities, logics, and feeding this into decision making on both sides. In order to action feedback better across the broad spectrum of hospital activity, stronger accountability and inter-departmental connection is crucial. Finally, a long-term view of the work needs of temporary staff, such as locum doctors and training doctors on rotation, should be taken; although improvement processes take time and individual staff members may move on from the hospital before they can benefit directly from changes, the needs and issues identified by these staff within their roles are also likely to affect others coming into the same roles in the future.
Conclusion
For dynamic, responsive, and evidence-based healthcare management, it is crucial for managers to be able to tap into the so-called “soft intelligence” 3 of upwards voice directly from staff on the frontlines of patient care. However, as this study has demonstrated, communication between hospital doctors and managers can be marred by deafness to feedback, disconnection physically and professionally, and denial of reports, issues or responsibilities. These communication barriers, if unaddressed, contribute to staff burnout which compromises workforce retention and patient safety, and jeopardises quality improvement. But healthcare organisations may address these issues by fostering clear and responsive feedback pathways, regular and genuine connection between managers and the work of clinical staff, and an organisational commitment to accountability, psychological safety and listening as part of a cultural ethos of quality improvement. This would benefit doctors’ sense of purpose, value and well-being, but it would also benefit hospital functioning, patients and society in general.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Health Research Board of Ireland [grant number EIA-2017-022]. The funders had no role in the design of the study, in the collection, analysis and interpretation of data, or in writing the manuscript.