
Abstract
With the aim of providing evidence about doctor-managers’ resilience during the Covid-19 pandemic, this study analyzes the characteristics of 114 doctor-managers operating within the Italian National Health Service (NHS). During the emergency, doctor-managers had to show adaptive capacities to deal with unexpected situations and develop new paradigms, procedures, and quick responses to patients’ needs. This is in line with resilience, and in this perspective, it is crucial to investigate resilience determinants. The paper, therefore, provides an identikit of the resilient doctor-manager. The research was conducted between November and December 2020. Primary data were collected through an online questionnaire consisting of six sections. Participation was voluntary and anonymous. Data were analyzed using quantitative techniques and employing Stata 16. Confirmatory Factor Analysis was employed to test construct validity and scale reliability. Results show that increasing levels of individual resilience are related to increasing levels of managerial identity. Moreover, physicians’ individual resilience has a positive association with commitment, knowledge diffusion, and Evidence-Based Medicine adoption. Finally, physicians’ individual resilience has a negative association with their role in the university, their specialty, and their gender. The study suggests some practical implications for healtcare organizations. In general, career paths are decided primarily on competency assessment, while an important role should be devoted to behavioral characteristics. Furthermore, organizations should take care of the levels of individual commitment and encourage professional networking because both help doctor-managers cope with uncertainty. The originality of the study relies on a fresh look at all previous work. There are currently few contributions in the literature to explore and investigate resilience elements in doctor-managers during the pandemic era.
Introduction
The Covid-19 pandemic has affected the entire world, putting a strain on healthcare workers involved in the frontline. 1 Healthcare systems had to reduce the risks associated with the emergency, implementing measures to protect the population’s health in the short and long term. The overdemand for care introduced the need to reorganize hospitals to manage large numbers of patients during the acute phase. All healthcare workers, allied health professionals, nurses, and physicians have been involved in these challenges. Scholars have widely documented that one of the main characteristics of healthcare organizations, especially those working in the public sector, is ask to professionals to participate in the design of organizational decisions.2,3 This is what is happened during the pandemic when to healthcare professionals have been asked to learn a ‘new normality’ imposed by the events.4–6 Although within a hospital, various managerial responsibilities can be assigned to physicians, nurses and administrative figures, 7 within the currently adopted organizational models, hospital CEOs decentralize the governance of clinical directorates and ward units to specific figures named Clinical Directors and Head of ward units. These are physicians who coordinates at different levels the activity of colleagues as primus inter pares.7,8 To them are assigned both clinical and managerial responsibilities,9–11 acting as “two-way windows”. 12 During the emergency although all the healthcare professionals dealt with the new virus, adapting their routines, converting physical assets and so on, 13 the designated managers of clinical directorates and ward units have been asked to completely exercise their managerial role. And for this reason, it is interesting to analyze how these specific roles behaved and reacted during the crisis.
They were forced to react and adapt to the Covid-19 struggle, with severe repercussions on their psychological capital, as well as on the departments’ organization and costs. As affirmed by Lega and Palumbo, 4 the new normality imposed a “transformation of conventional managing models and leadership styles… to make sense out of the new challenges faced by healthcare organizations and on their capability to act managerially, sticking to an empowering approach which enables followers”. During a crisis, resilience is one of the individual characteristics mainly involved. It is well known that resilience plays a fundamental role in facing adversities, 14 especially in disruptive and adverse work environments.15–17 Literature provides several contributions on the role of resilience in the healthcare system,18–21 mainly focusing on the organizational perspective, while research on individual-level resilience in healthcare is rapidly growing, as documented by the systematic review proposed by Robertson and colleagues 22 and by Rieckert and colleagues, 23 who provide practical recommendations on how to build and maintain the resilience among frontline healthcare professionals exposed to COVID-19. With the aim to contribute to this emerging debate the present paper empirically investigates determinants of resilience in doctor-managers during the pandemic era.
Doctor-managers resilience during Covid 19 pandemic
The multifaceted challenges of the contemporary environment impose on organizations to develop the capabilities required to minimize the negative impact of unpredictable events. 24 The increasing frequency of disasters, including natural disasters, pandemics, and terrorism, stresses the relevance of the concept of resilience. Resilience can be defined as the dynamic ability to cope with and bounce back from stressful events. 25 From an organizational perspective, within the healthcare context, several contributions demonstrate how organizations deal with unexpected events in crisis situations. For example, some scholars identify hospital disaster resilience as the ability to withstand, absorb, and respond to disasters while maintaining critical functions.26,27 Instead, Mulyasari and colleagues 28 demonstrate that investments and preparedness, in general, increase the degree of resilience when a disaster occurs. From a psychological perspective, resilience is the individual’s ability to maintain equilibrium during and after difficulties, 29 continuing to grow and learn from traumatic experiences. 21 The main individual factors contributing to the development of resilience are self-efficacy, self-satisfaction, ability to adapt to change, problem-solving, governance, and recovery from negative emotions. 25 Resilient people are those who make sense of what is happening, learn quickly from experiences, and develop an effective response to changing situations, including tackling unexpected and emergency situations by reconfiguring existing routines, roles, rules, and resources. 30
Resilience is known to reduce depression and burnout levels and increase professionals’ well-being; 31 it also positively affects employee job satisfaction and happiness at work. 32 However, as widely demonstrated during the Covid-19 pandemic healthcare workforce has been strongly put under pressure due to the need to cope with stressful clinical practices 19 while trying to continuously adjust and adapt their behaviors to the job variability introduced by the emergency. 33 This is why the American Psychological Association recently stressed the importance of promoting psychological resilience in healthcare professionals to affect their well-being. 34
From this perspective, it becomes interesting to analyze healthcare professionals’ psychological resilience during the pandemic. Bozdağ and colleagues 33 reported a positive relationship between higher levels of psychological resilience and higher quality of sleep, positive affective state, age, and life satisfaction. Lin and colleagues 35 studied the resilience of non-local medical workers sent to Wuhan to treat Covid-19 patients. The authors reported that the highest level of resilience was found in physicians, followed by support staff, including healthcare assistants, technicians, and nurses. Resilience was negatively correlated with anxiety and depression but positively correlated with active coping styles, as well as training and support from the hospital. They concluded that resilience helped medical workers recover better from trauma and experience lower anxiety and depression levels in the face of public health emergencies. Finally, Liu and colleagues 36 described healthcare professionals’ experience in the epidemic’s early stages in a small sample of physicians and nurses. Despite the intense workload, healthcare professionals showed resilience and a spirit of professional dedication to overcome difficulties. As they usually do, but especially during the pandemic the roles to whom is currently decentralized the governance of clinical directorates and ward units, covered by the so named doctor managers, have been involved in critical decisions such as organize resources, logistics, patient flows. 26 For this reason they have demonstrated the need to possess a bundle of necessary competencies in terms of leadership, 37 but also the ability to combine the clinical competencies with the managerial ones with the aim to efficiently manage resources and achieve better organizational performance. 38
Doctor-managers are usually essential to support the definition and implementation of new strategies and to help improve hospital performance. 39 Doctor-managers are characterized by high versatility 40 and experience time pressures. 41 It has been reported that doctor-managers’ ability to successfully carry out their managerial responsibilities depends on their individual characteristics and managerial aptitude. 40 Also, empirical evidence suggests that technical knowledge and expertise contribute to shaping doctor-managers’ managerial competencies. 42 Both individual characteristics and technical knowledge have been necessary to address the ongoing Covid-19 pandemic.
Starting from March 2020, physicians holding managerial positions such as Clinical Directors and Heads of ward units faced stressful situations such as a lack of adequate capacity to handle the surging patient volume, the need for intensive care unit (ICU) beds and ventilators, and the staffing that far exceeded the maximum capacity. As a result, they had to make quick decisions in a climate of complexity and uncertainty that broke down preexisting routines and organizational processes. In addition, they needed to take care of frontline staff’s physical and mental health, providing personal protective equipment, and helping them cope with tremendous mental stress. Finally, doctor-managers had to properly handle patient care models’ capacity and real-time redesign, making critical staff reassignment decisions. In such a scenario, the dual role of physicians assumed a more challenging connotation, and it is crucial to identify individual characteristics, behaviors, and skills useful in making them capable of coping with stressful, difficult, and quick decisions.
During emergencies, Clinical Directors and Head of Ward units had to show all their adaptive skills to deal with unexpected situations and develop new paradigms, procedures, and quick responses to patients’ needs. 43 This paradigm is in line with resilience, and in this perspective, it is important to analyze the variables that can influence doctor-managers’ resilience. In order to provide evidence in this debate, the study focuses on exploring resilience in doctor-managers in the Covid-19 era.
Methods
Sample and procedure
This research was conducted between November and December 2020. Primary data were collected through an online written questionnaire administered to a convenience sample of 150 Italian physicians enrolled in middle managerial roles. At the time of data collection, they were attending an online university management course.
The questionnaire, developed in Italian specifically for this study, consisted of six sections: (1) role identity, (2) individual resilience, (3) commitment, (4) spread of knowledge, (5) Evidence-Based Medicine (EBM) adoption, and (6) personal data.
The questionnaire was pre-tested and validated by a small sample of doctor-managers.
These doctor-managers were asked for feedback and to raise concerns regarding the questionnaire. This information allowed to detect any problem with the questionnaire design related to the ambiguity of words, misinterpretation of questions, or any other issue. Furthermore, doctor-managers were asked to sign an informed consent in accordance with applicable Italian data protection laws. Failure to sign the consent resulted in the automatic termination of administration. Participation was voluntary and anonymous. 114 completed questionnaires are returned, configuring a response rate of 76.00%.
Figure 1 summarizes the main characteristics of the sample. In detail, of the 114 surveyed doctor-managers included in the sample, most were male (62.28%), older than 50 years of age (88.60%, the Italian medical population average age is 51.3), and with a technique-oriented specialization (59.65%). Medical specialties can be classified into two broad categories: person-oriented and technique-oriented.
44
Person-oriented specialties focus on the holistic view of the patient and tend to emphasize the relational and empathic approach to the patient. In contrast, technique-oriented specializations are more focused on the technical skills, tools, and technologies needed to deliver healthcare processes and activities. In the sample, doctor-managers have been working in the I-NHS for at least 25–34 years (32.7%). Full sample sociodemographic characteristics.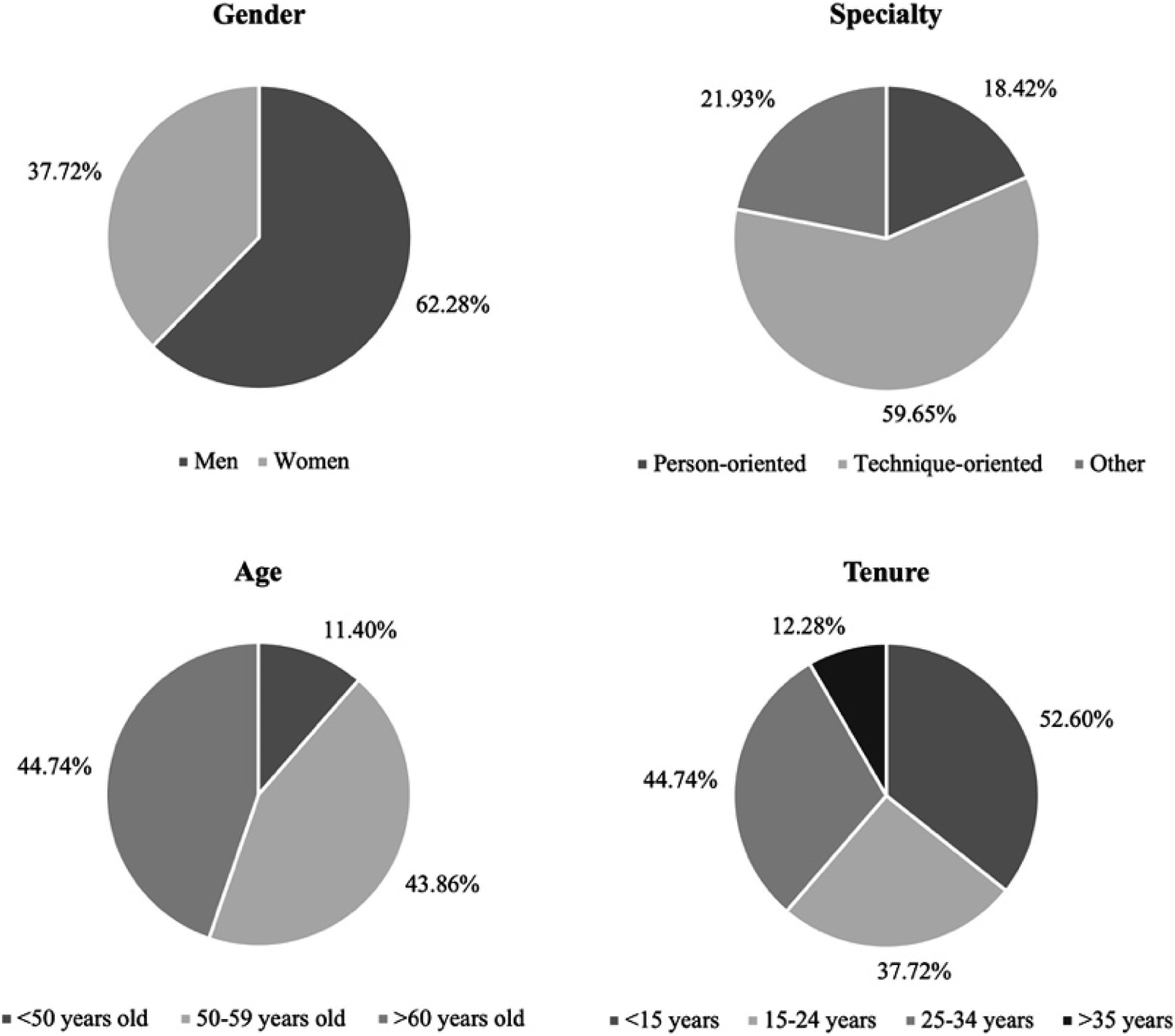
Variables
Managerial identity
According to Cicchetti’s scale, 45 the role identity area was based on 16 questions. A 6-point Likert scale was used to answer the questions. Responders had to specify their level of agreement with each question, ranging from 1 (complete disagreement) to 6 (complete agreement). The first eight questions measured physicians’ clinical propensity (an example question is: I’m prone to maintain a number of social and work interactions), while the second eight questions estimated physicians’ managerial propensity (an example question is: I’m action-oriented and I do not need to schedule my activities in advance). Higher values in this variable represent more intense physicians’ managerial propensity. This area allows us to evaluate a clinical director’s aptitude to consciously perform this dual role (i.e., clinical and managerial) while considering individual characteristics.
Individual resilience
Individual resilience was measured this variable using the short version (10 items) of the Connor-Davidson Resilience Scale (CD-RISC). 46 A 5-point Likert scale, ranging from 0 (strongly disagree) to 4 (strongly agree), was used to answer the questions. This is an additive scale and scores range between 0 and 40. Higher scores indicate higher levels of resilience. An exemplary item is “I am able to adapt when changes occur.”
Commitment
This area has been developed based on Bergami and Bagozzi’s 47 approach. A 5-point Likert scale was used to answer the questions. Responders had to specify their level of agreement with each question, ranging from 1 (complete disagreement) to 5 (complete agreement). This area allows us to evaluate a physician’s commitment to the organization. According to the rating scale used, more positive values represent higher levels of commitment.
Knowledge diffusion
The diffusion of knowledge was measured through the 12 Knowledge Management Behavior Assessment provided by Shamim and colleagues. 48 A 7-point Likert scale was used to answer the questions. Respondents were asked to specify their level of agreement with each question, ranging from 1 (rarely) to 7 (very frequently). This area allows us to evaluate a physician’s capacity to share knowledge, accept suggestions, collaborate with other colleagues, and exchange ideas and opinions with his/her own team and other colleagues. According to the rating scale used, more positive values represent higher levels of integration, information sharing, and communication with other colleagues.
EBM adoption
According to Sammer and colleagues, 49 the EBM area was based on one question. Respondents had to specify how often they refer to the literature in clinical practice. A high level of physicians’ self-reported propensity to use new treatments, procedures and EBM based on scientific evidence indicates the importance of doctor-managers’ professional updating in their daily routine.
Personal data
This area included gender, age, job role, and specialty (i.e. technique-oriented or person-oriented).
Analysis
CFA results for the reliability and validity of the measurement items.

Results
Descriptive statistics and Spearman’s correlations.
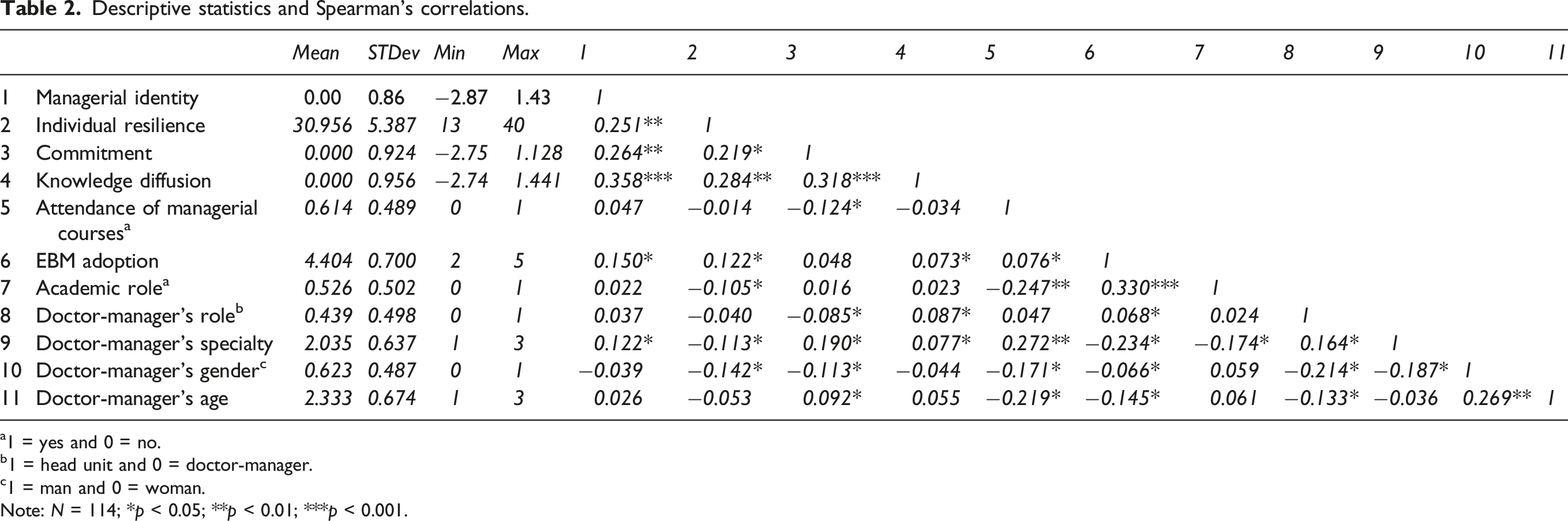
a1 = yes and 0 = no.
b1 = head unit and 0 = doctor-manager.
c1 = man and 0 = woman.
Note: N = 114; *p < 0.05; **p < 0.01; ***p < 0.001.
Spearman’s Rank-Order Correlations were useful in measuring the strength and direction of the association between continuous and categorical variables. Regarding the variables of interest (i.e. Managerial identity and Individual Resilience), the results show a weak positive association between them (r = 0.251, p < 0.01).
Results underline that increasing levels of physicians’ individual resilience are correlated with increasing levels of managerial identity (r = −0.251, p < 0.01), work environment commitment (r = 0.219, p < 0.05), knowledge diffusion (r = 0.284, p < 0.01), and EBM adoption (r = 0122, p < 0.05) showing that the higher levels of individual resilience the higher the levels of managerial identity, commitment, knowledge diffusion, and EBM adoption. Furthermore, physicians’ individual resilience has a weak negative association with the fact that physicians cover an educational role in the university (Figure 2(a), r = −0.105, p < 0.05), their specialty (r =−0.113, p < 0.05), and their gender (Figure 2(b), r = −0.142, p < 0.05). In detail, Figure 2(a) illustrates that high levels of individual resilience (scores higher than 30) are mainly owned by doctor-managers not having an academic role. Instead, Figure 2(b) shows that woman doctor-managers especially hold higher levels of individual resilience (scores higher than 30). Individual differences. (a) Doctor-manager’s individual resilience differences and academic role. (b) Doctor-manager’s individual resilience differences and gender.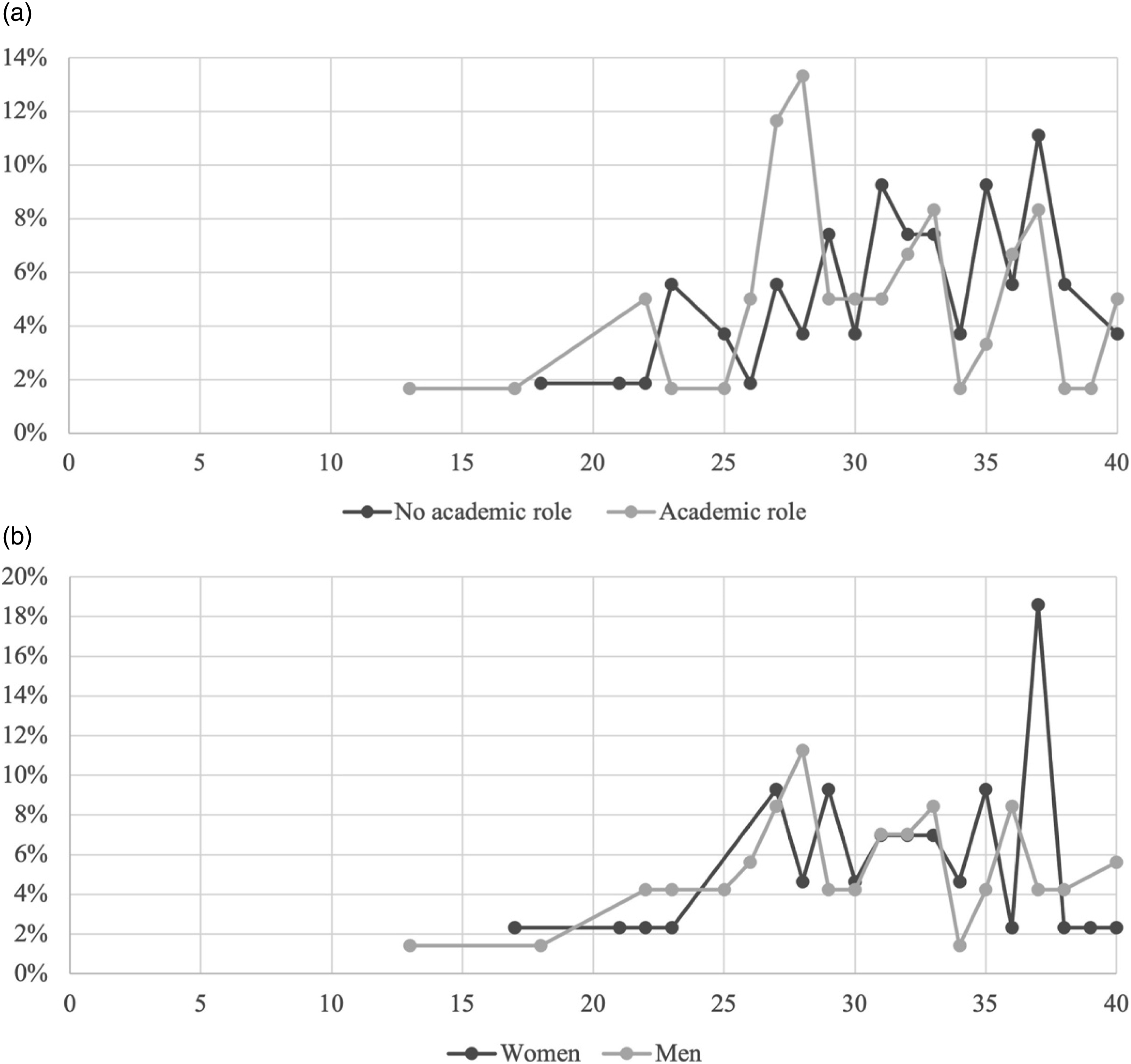
Discussion
Aiming to explore doctor-managers’ resilience during the Covid-19 pandemic, this research provides some preliminary evidence useful in shedding light on the main characteristics that can help them deal with a very unexpected and stressful situation.
The Covid-19 pandemic involved doctor-managers in the first line of intervention, with severe repercussions on their psychological capital. They had to take care of patients affected by an unknown condition and make organizational and managerial decisions at the same time. There is very little evidence about doctor-managers’ degree of readiness and the strategies they adopt to cope with uncertainty. During the Covid-19 era, doctor-managers have learned a ‘new normality’ imposed by the ongoing events, 4 which forced them to react and adapt to struggles. The analysis of the 114 doctor-managers’ answers provides a picture of the main characteristics a resilient doctor-manager should own. In the study sample, the degree of resilience is generally high, and a high level of managerial identity accompanies it.
This research contributes to the current debate in the literature in several ways. First, the paper contributes to the research on disasters or health emergencies, analyzing the main characteristics a doctor-manager should own to face adversity successfully. This stream of research is in its primitive stage and more studies are needed to better understand clinical skills and, more importantly, the behavioral dimensions useful for managing unexpected challenges. 52 The results of the paper suggest that individual resilience is associated with a combination of multiple variables, both at individual and organizational level.
Second, the study contributes to the literature on doctor-managers, underlining the importance of some personal characteristics that could help them perform their work better. In fact, results underline that doctor-managers who are resilient cope better with adversity. To the best of our knowledge, this is one of the first studies analyzing single professionals’ resilience.
Also, the paper contributes to the literature on individual resilience, depicting the leading individual and background characteristics positively and negatively correlated to it. Results show that resilience is positively related to the degree of commitment, demonstrating that sharing goals and developments within the organization increase workers’ willingness to overcome stressful events. Moreover, resilience is positively related to EBM adoption and the behaviors aimed at spreading knowledge. Physicians who are more naturally predisposed to share their know-how, interact, and exchange ideas and opinions, have created a network. They know they can ask other colleagues for advice and suggestions, thus reducing feelings of isolation and increasing resilience. These results are in line with previous studies showing that knowledge spread and EBM adoption should be enhanced during stressful events; sharing experiences in the hospital, exploring lessons learned and strategies to manage the stress of uncertainty and/or fear of the pandemic, bouncing back and strengthening their adaptive capacities. 53
Furthermore, in terms of individual characteristics, results show a significant correlation between the female gender and individual resilience, confirming previous evidence. 54 Professional background positively correlates with the degree of individual resilience. Compared to more standardized academic tasks, the non-academic position positively correlates with the degree of individual resilience due to the habit of dealing with unplanned activities.
Finally, results illustrate a relationship between individual resilience levels and specialty: higher levels in person-oriented specialties and medium levels in technical specialties. Person-oriented doctor-managers such as cardiologists, neurologists, etc., are used to working directly with patients and with diseases that, by definition, are constantly changing and variable. This makes them more confident in their adaptive abilities and, therefore, more resilient than doctor-managers with a technique-oriented specialization. 44
Conclusions
The aim of this paper was to provide a frame of doctor-managers’ resilience during Covid-19 pandemic. A survey has been conducted within a sample of physicians staffed into managerial roles operating into the Italian NHS. Results provide a picture of individual characteristics associated with resilience, and specifically highlights the role played by commitment, propensity to EBM adoption and knowledge diffusion, specialization and demographics. Based on these results, this study provides some practical managerial and policy-making implications. Regarding skills, career path decisions are mainly based on competency assessment, while an important role should be given to individual characteristics. Moreover, HRs should propose training and coaching activities to improve and increase doctor-managers’ individual resilience. From a managerial perspective, organizations should take care of commitment. As the results of this paper show, a sense of belonging satisfies the highest levels of motivation and increases the strength with which people face problems. Moreover, organizations should propose activities facilitating the establishment of professional networks. These might help professionals feel stronger even in the face of uncertainty.
Our findings should be interpreted in light of several limitations, each of which indicates a clear direction for future research. First, the data used in the analysis are self-reported. However, this was intrinsic in the purpose of the study, which is to assess the feelings and behaviors adopted by physicians involved in managerial roles during the COVID-19 pandemic. Future studies should be aimed at combining self-reported data with publicly available information, thus allowing us also to reduce the potential for same-source bias. Second, the sample is quite limited and does not encompass all medical specialties. However, physicians come from public and private healthcare organizations, belonging to all institutional arrangements in the Italian NHS. Therefore, data provide a comprehensive picture of doctor-managers’ resilience during the COVID-19 pandemic. In addition, the survey is still open-ended, and future study development will incorporate further evidence. Third, the healthcare context in which this study was conducted may not appear to be generalizable. However, since the pandemic occurred worldwide regardless of health system characteristics, it may be of interest in future studies to compare experiences coming from different countries. Despite these limitations, this study provides a new perspective on the understanding of resilience during the COVID-19 pandemic.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.