
Abstract
This research aims to deepen our understanding of patients’ satisfaction with therapeutic patient education (TPE) in oncology. The research model proposed was tested, with structural equation modeling, on 207 French breast-cancer patients who participated in a TPE program. The results confirm that post-TPE empowerment and relational proximity to the TPE team are two major antecedents of patient’s satisfaction—and attitude and word-of-mouth toward TPE are two important consequences of this concept of satisfaction. However, the established relationships are moderated by the patients’ profiles (i.e., utilitarin believers, passionate followers, or holistic followers) in terms of the perceived value of their own experience of patient education. These results will enable stakeholders to adapt their TPE promotion strategies to the profiles of the patients. The study will also help to demonstrate and highlight the patient benefits of TPE to various stakeholders and thus will favor access to this personalized care practice, which is essential in the management of chronic diseases, but is still limited in oncology.
Keywords
Introduction
In recent years, the healthcare system has been forced to adapt to the increasing prevalence of chronic diseases and changes in patients’ health-related behavior. Providing guidance and encouraging patient autonomy, in particular, are becoming more prominent in a quest to increase patients’ involvement in the management of their diseases and to increase their empowerment—that is, the power to act and make decisions regarding their own health. 1 Therapeutic patient education (TPE) has an important role to play in addition to direct care.
According to the World Health Organization, 2 such patient-centered personalized care allows patients to acquire and maintain knowledge, skills, and adapted behaviors to enable them to better live with their chronic diseases, to achieve psycho-emotional balance, and to (re)take ownership of health standards and a life plan. Patient-centered personalized care involves organized activities, integrated into the patient’s care pathway (as needed) to raise awareness, provide information, teach self-management, and provide psychological support concerning the disease and treatments, care, hospital setting, organizational information, and health and illness behaviors. Patients, by being empowered and more autonomous (with self-monitoring, safety and adaptation skills), become actors in managing their own therapy, and patient–clinician communication is enhanced.2–4
Although TPE is already well developed in the management of chronic diseases (such as diabetes and asthma), it has recently emerged in oncology as well.5,6 TPE can benefit cancer patients by improving their quality of life as well as the management of toxicities and the effectiveness of treatments. However, a recent analysis of TPE literature 5 highlights the heterogeneity and methodological imprecision or limitations of experimental research conducted to evaluate the benefit of a therapeutic strategy incorporating TPE. Thus, the scope of the results of this research is limited. Research on patients’ experiences has often been overlooked because of the limitations of the incorporated qualitative approaches. Moreover, TPE evaluation, as required by health authorities, tends to focus on organizational aspects and less on the complex evaluation of their effects on patients. Evaluations of TPE effects are essentially based on assessments of learning, expected changes (knowledge and skills developed and implemented), and patients’ satisfaction with the various components of the system.3,4
To summarize, this research aims to build on the work devoted to the evaluation of the specific effects of TPE on patients by gathering their lived experiences, from their perspective, 7 and by adopting a quantitative approach. More specifically, it tests (in the French context) two antecedents (empowerment and relational proximity) and two consequences (attitude and word-of-mouth intention) of patients’ satisfaction with their lived experiences, together with the moderating role of the perceived value of TPE 8 on the relations stipulated in the research model. This research was conducted on breast cancer patients treated at the Institut de Cancérologie de l’Ouest.
Theoretical framework and research model
TPE: The pillar of patient-centered health management research
Among health professionals, a profound paradigm shift has led to the adoption of a new approach to care inspired by existential humanistic psychology: patient-centered care (PCC). 9 This relational approach emphasizes the importance of listening, consultation, support, and learning in collaboration with the patient, with the aim of co-constructing the treatment and the care pathway. Thus, the care teams interpret the care relationship in a more participatory manner (by drawing on the patient’s resources and capacities), and as a long-term collaboration.
Numerous studies have demonstrated the beneficial effects of this new caregiver–patient alliance both for the patient and for the care system as a whole. 10 Further, the PCC approach redefines intervention logics by targeting the patient’s standpoint. It also requires greater accountability and better patient education. TPE is a product of the evolution of the patient-centered approach in the healthcare system.
For patients, these developments reflect their heightened need for empowerment. Nowadays, patients aspire to increase their autonomy, and are demanding more balanced relationships, along with greater transparency and participation. 1 Moreover, they want to assert themselves as partners in care and to be actors in their own health. Patients’ empowerment transforms the care relationship into a new, more symmetrical alliance. Patients’ mastery of expert knowledge and the recognition of their abilities and autonomy are central to the new caregiver–client relationship.
TPE programs in France
Beyond the reference definition of TPE proposed by the WHO, 2 TPE covers practices that are heterogeneous and evolving. Thus, they vary by country and pathologies. 11 In France, TPE is included in the public health code (HPST law 2009). Programs must be developed by multidisciplinary teams trained in therapeutic education (physician, caregiver, paramedical staff, and patient partner), and co-constructed in compliance with the Haute Autorité de Santé (HAS) guidelines. Thus, even if their expectations and content vary according to the institutions and teams, their fundamental objectives and their common overall scheme guarantee homogeneity in the measures implemented.
TPE program (TPEP) is divided into four steps for each patient: (1) educational diagnosis (patient educational needs and priorities are identified during a personalized interview with a TPE practitioner); (2) educational-therapeutic-contract (the patient and a TPE practitioner set goals and according to the previous needs built the content); (3) educational session (the patient attend to active and interactive teaching sessions either collective or individual); and (4) assessment of educational activity for each patient (identification of acquired knowledge, developed skills, and behavioral changes; and readjustments provided, if needed).3,4
Research model
Satisfaction with TPE: Antecedents and consequences
In this study, which focuses on the cancer patients’ experiences (examined from their perspective), satisfaction with TPE is construed as a psychological state resulting from the patients’ experiences of TPE. This approach differs from the classic approaches to health satisfaction, which are based on evaluative judgements made by patients on the various components of the service, and not on the final result of the lived experience. The final result is later and relative (comparison between the subjective lived experience and a reference base specific to the patient, such as their expectations).12,13
Two antecedents of patients’ satisfaction with their experience of a TPEP will be tested: post-TPE empowerment, and relational proximity with the TPE team (Figure 1). These two antecedents of satisfaction (cognitive and affective), derived from the marketing literature,13,14 are also central to the TPE approach. The research model.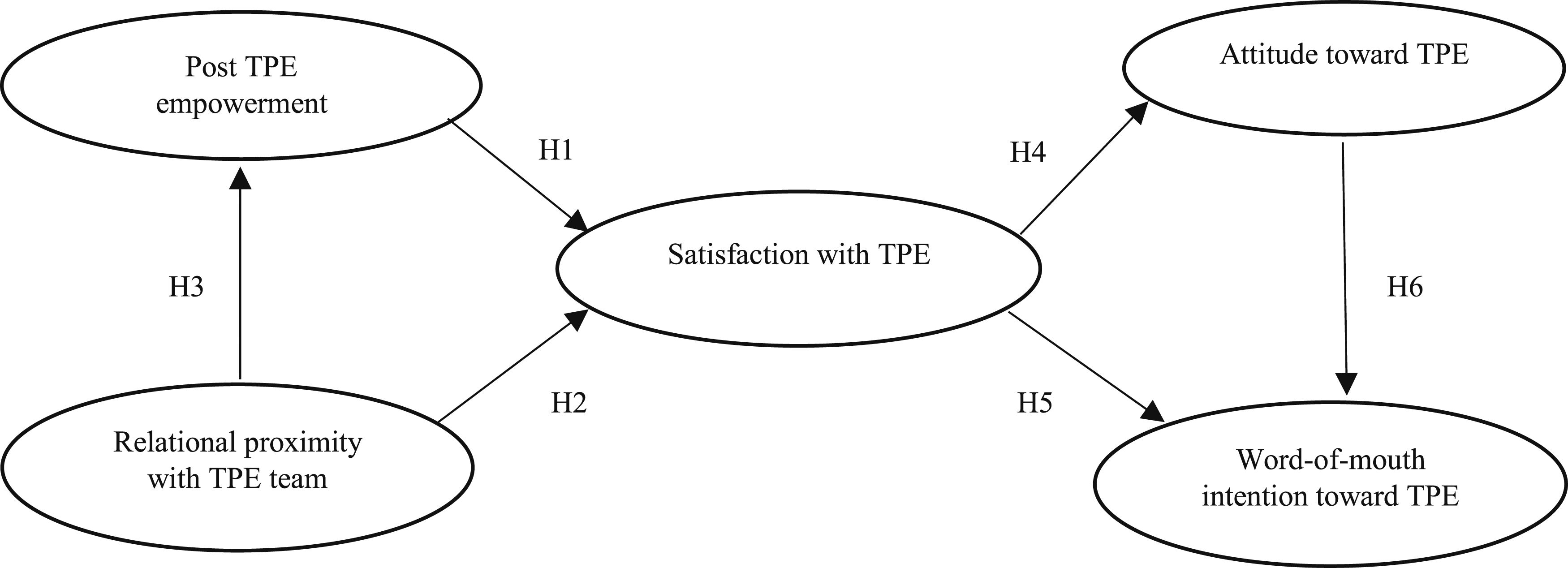
Empowerment is a concept that has been explored at several levels, in different fields, and from several angles, leading to different interpretations, particularly in terms of process or outcome.1,15 Referring to the dominant conception of empowerment in management, proposed by Spreitzer, 16 empowerment will be considered in this research as a psychological state resulting from “skill building” processes, such as TPE, pertaining to a task to be carried out (in this case, to optimally follow an oncology care pathway). More specifically, post-TPE empowerment is defined here as patients’ proactive state of mind regarding their care pathways, based on their skills and abilities and perceived self-confidence (self-efficacy) and autonomy (self-determination) after having participated in a TPEP.
TPE is a comprehensive approach to strengthen patients’ skills, to support their actions, and to empower their health decision-making. This care practice is personalized and adapted to the educational needs or priorities of each patient—and is identified, co-defined, and shared with the TPE teams.3,4,11 Thus, conceptually,12,13 if patients’ expectations with regard to the TPE program are confirmed, and if they actually feel able to live their care pathway to the best of their ability, then they will be satisfied with the final result of their lived experience.
In the marketing field, previous research17,18 indicated that consumers’ empowerment is important in creating consumers’ satisfaction. Consumers who are empowered and participate in the marketing effort (e.g. by designing products or services that perfectly fit their specific needs) are likely to lead to superior customer-based profit performance in terms of developing a greater sense of belonging to the company, thereby increasing their satisfaction so that they give positive word-of-mouth intentions. Thus, one of the best ways to reinforce consumers’ satisfaction (so that they provide positive word-of-mouth intentions) is by empowering them. These findings support emerging research indicating that marketing should place more emphasis on consumers’ empowerment practices in order to enable them to participate in the marketing effort.
In light of the objectives of TPE,3,4 and drawing on work conducted on the evaluation of empowerment support projects 7 and on marketing research,17,18 we postulate hypothesis H1:
Post-TPE empowerment has a positive influence on satisfaction with TPE.
The specificities of the therapeutic relationship established in TPE3,4,11 suggest that the proximity of the interindividual relationships between patients and the TPE team also influences patient satisfaction. The patient is considered as a sensitive and vulnerable subject. The patient–TPE practitioner relationship is personalized, and is comprehensive (in personal, physical, psychological, and social dimensions) and adapted to meet the educational needs or priorities of the patient. This induced relational proximity to the TPE team should contribute to its satisfaction with the lived experience.
In the field of marketing, proximity is a major concept that plays an important role in establishing and maintaining relationships between a company and its consumers. 19 Research on proximity in this area also suggests that relational proximity, defined as the perceived affinity or connection between two people, positively influences satisfaction.20,21,22 For instance, the presence of a salesperson in a store to serve consumers and/or to give them information on the products, or the retailer having a positive influence on their satisfaction towards this retailer and its stores.
Hence, hypothesis H2:
Relational proximity to the TPE team has a positive influence on satisfaction with TPE.
A recent analysis of scientific literature (medical, sociological, psychological, and nursing fields) disentangling the often-confounded concepts of patient empowerment, patient participation, and patient-centeredness, highlights four major antecedents of patient empowerment: the improvement of patients’ skills, active patient participation, the particular dialogue between the caregiver and the patient, and the personalization of the relationship according to patients’ needs and circumstances. 1 This analysis highlights the importance of a personalized and comprehensive therapeutic relationship established in TPE.3,4,11 Thus, we assume that the relational proximity between TPE providers and patients also promotes patient empowerment. Hence, hypothesis H3:
Relational proximity with the TPE team has a positive influence on post-TPE empowerment.
Further, we test two consequences of satisfaction (often addressed in the marketing literature) relevant to the promotion of TPE among patients: attitude (a psychological tendency expressing a degree of longer-lasting (dis)favor toward TPE), and peer-to-peer word-of-mouth intention (see Figure 1).
In the field of marketing, numerous empirical studies have found a positive and significant link between consumer satisfaction and attitudinal and behavioral loyalty.23,24 In addition, research has repeatedly shown that consumer attitude has a significant positive influence on their future behavioral intentions, such as their word-of-mouth intention.25,26 The more a consumer is satisfied with a lived experience (e.g., with a product, a service, or a store), the more their attitude towards the specific object is positive, as well as their word-of-mouth intentions (with a direct link, but also indirectly through the attitude). Similarly, health studies have established a positive link between patient satisfaction with the quality of communication with providers (such as empathy and responsiveness) at the heart of TPE and of word-of-mouth intensity. 27
Hence the following three hypotheses:
Satisfaction with TPE has a positive influence on attitude toward TPE.
Satisfaction with TPE has a positive influence on word-of-mouth intention toward TPE.
Attitude toward TPE has a positive influence on word-of-mouth intention toward TPE.
Perceived value of TPE: A moderator of antecedents and consequences of satisfaction with TPE
Patients’ informal (spontaneous feedback) and more formal (qualitative studies or self-evaluation questionnaires) feedback on the TPE usually indicates high levels of satisfaction with the experience. However, these evaluative judgments may cover different experiences of the care pathway and of the particular therapeutic relationship deployed in TPE, which is personalized, comprehensive, and patient-centered.3,4
To refine the analysis of potential differences in the links postulated in the research model (for different subgroups of individuals, and therefore patient profiles), the concept of perceived value of TPE will be introduced.8,28,29 The intensity, diversity, or hierarchy of the different benefits (cognitive, utilitarian, psychological, and relational) and costs (psychological and emotional) of a TPEP (as perceived by participants) 8 can alter the significance and/or strength of the associations between satisfaction with the lived experience and the antecedents and consequences studied. Hence hypothesis H7:
The relationships postulated in this research will be moderated according to the patient profiles established in terms of the perceived value of TPE.
Methodology
This research was carried out at the Institut de Cancérologie de l’Ouest (ICO) 1 with breast cancer patients who were enrolled in a TPE program. 2 Breast cancer, the most common cancer in women, is the leading cause of cancer death in women and its incidence is increasing. However, on a positive note, the 5-year survival rate in this group is increasing due to screening (early diagnosis) and improved treatment, although there is the risk of significant side effects. 3 The patient care pathway is complex and multidisciplinary (and depending on the case may involve initial surgery, chemotherapy, radiation therapy, endocrine therapy, and breast reconstruction). These treatments can lead to serious side effects that can impact the quality of daily, family, professional and social lives of patients and their families. Therefore, breast cancer TPE are the most common programs in oncology.
All patients who were enrolled in the ICO’s TPE/breast cancer program (at the Angers clinical site) during the selected reference period were asked to participate in the survey. The last 24 months was the reference period. A total of 470 patients were interviewed via a postal survey; of these, 233 patients responded. 26 incomplete or invalid questionnaires were discarded, resulting in a final database of 207 valid questionnaires, that is, an acceptable return rate of 44.04% for this type of study (in human and social sciences with cancer patients). The demographic profile of the 207 patients was as follows. Average age: 57 years; retired: 43.8%, active or other inactive: 56.2%; Angers site only: 16.2%, agglomeration: 26.7%, excluding Angers site and agglomeration: 57.1%. Note that regarding these three variables (age, occupation and dwelling place), no significant difference was found between the profile of patients who responded to the survey (and gave a valid questionnaire) and those who did not wish to participate or returned an invalid questionnaire.
Relational proximity was evaluated by five items adapted from Schultz’s scale. 22 Post-TPE empowerment was measured by six items adapted from Spreitzer’s scale, 16 validated in French 30 for the two sub-dimensions: skills (3 items) and autonomy (3 items). Satisfaction was measured by three items adapted from Oliver’s scale. 25 Attitude and word-of-mouth intention were measured respectively by two items adapted from Rosenberg and Hovland’s scale, 31 and by one item inspired by the work of Zeithaml and colleagues. 32
Lastly, the perceived value of TPE was measured by 36 items, 8 which encompasses eight dimensions of this concept. Five dimensions measure the perceived benefits of the TPE experience: support and guidance (5 items), useful knowledge for the care pathway (5 items), skills and resources available (5 items), self-management (5 items), and relationships with family and friends (3 items). Two other dimensions focus on the perceived costs associated with TPE: efforts to counter sources of anxiety (4 items), and efforts directed at other patients and/or stakeholders (5 items). Finally, 4 items measure the overall perceived value of TPE.
For each of the measurement scales used, the patients interviewed were asked to indicate (on a 7-point Likert scale) their degree of agreement or disagreement with each item (from 1 –strongly disagree to 7 – strongly agree).
Results
In this research, we used structural equation modeling, specifically partial least squares (PLS-SEM) with a bootstrapping procedure with 5000 replications. 33
Tests of the research model
Results of the structural equation model.
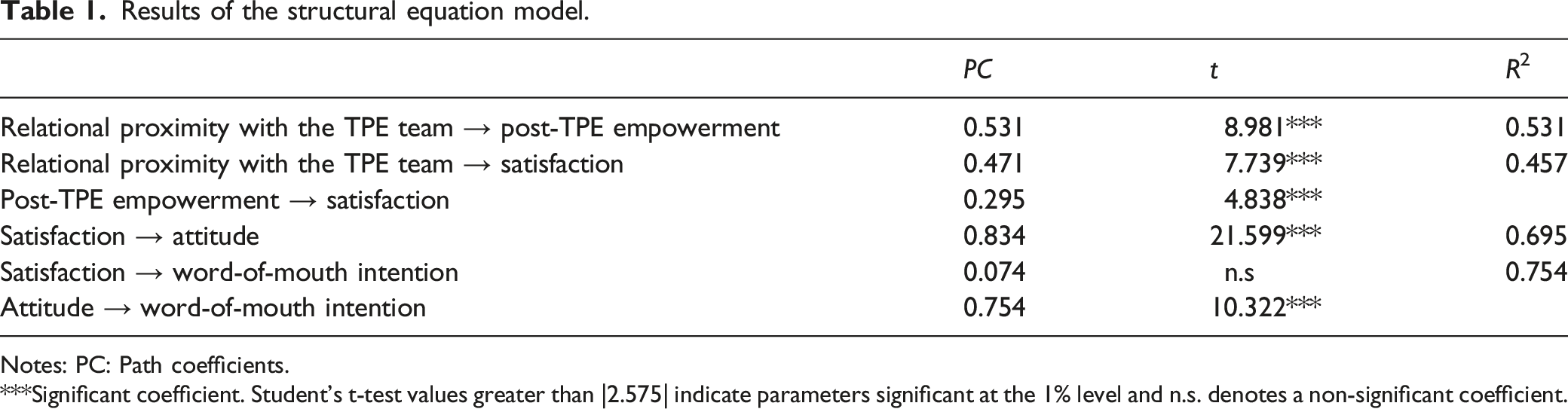
Notes: PC: Path coefficients.
***Significant coefficient. Student’s t-test values greater than |2.575| indicate parameters significant at the 1% level and n.s. denotes a non-significant coefficient.
Analysis of the moderating role of the perceived value of TPE
The Rebus algorithm 34 was used to identify potential differences in the intensity and significance of the links established by the structural equation model tested on the 207 patients. The aim was to highlight the existence of several groups of patients. Three subgroups of patients were highlighted, and the concept of perceived value of TPE was used to characterize them.
Three patient profiles.
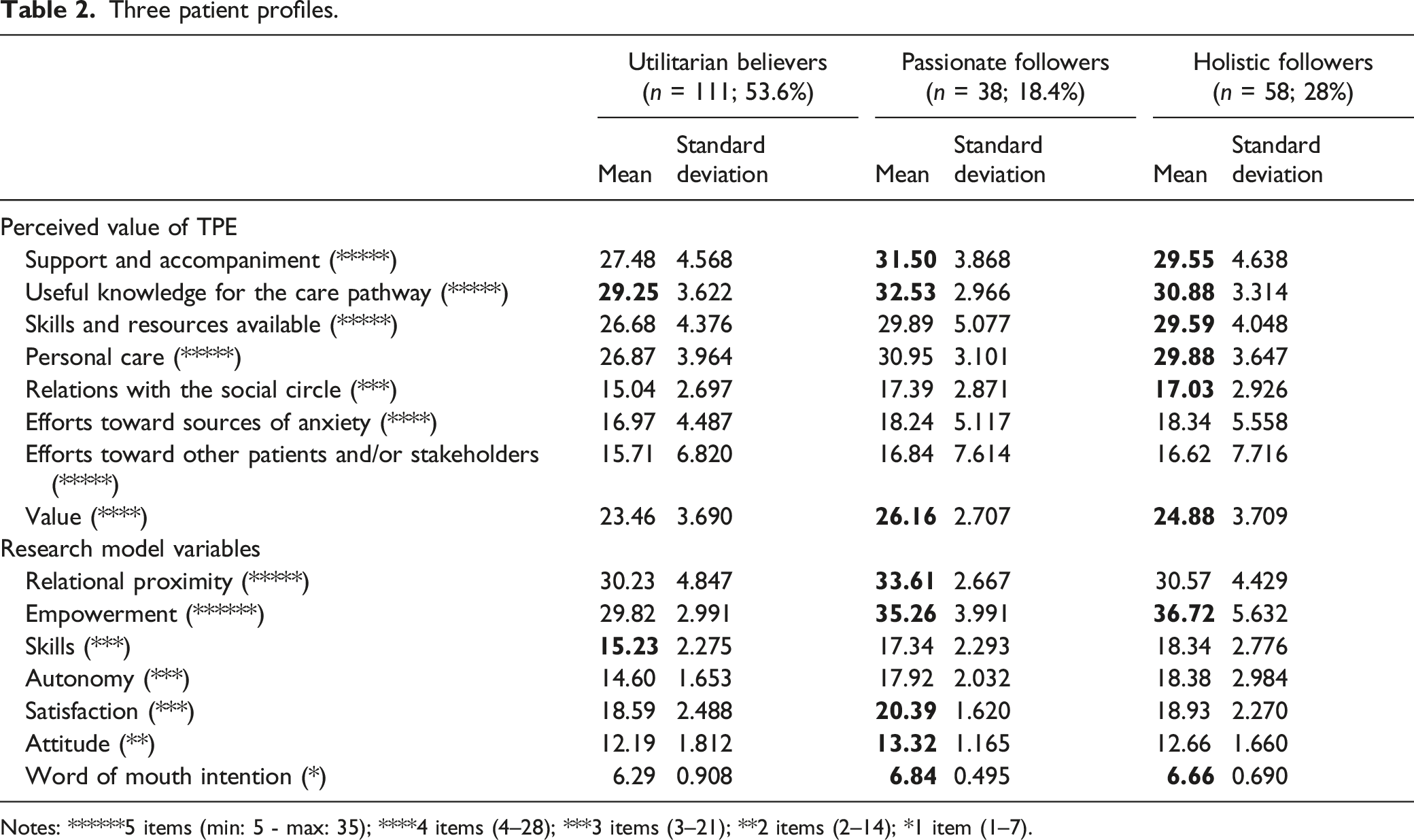
Notes: ******5 items (min: 5 - max: 35); ****4 items (4–28); ***3 items (3–21); **2 items (2–14); *1 item (1–7).
Results of the structural equation model for the three patient profiles.
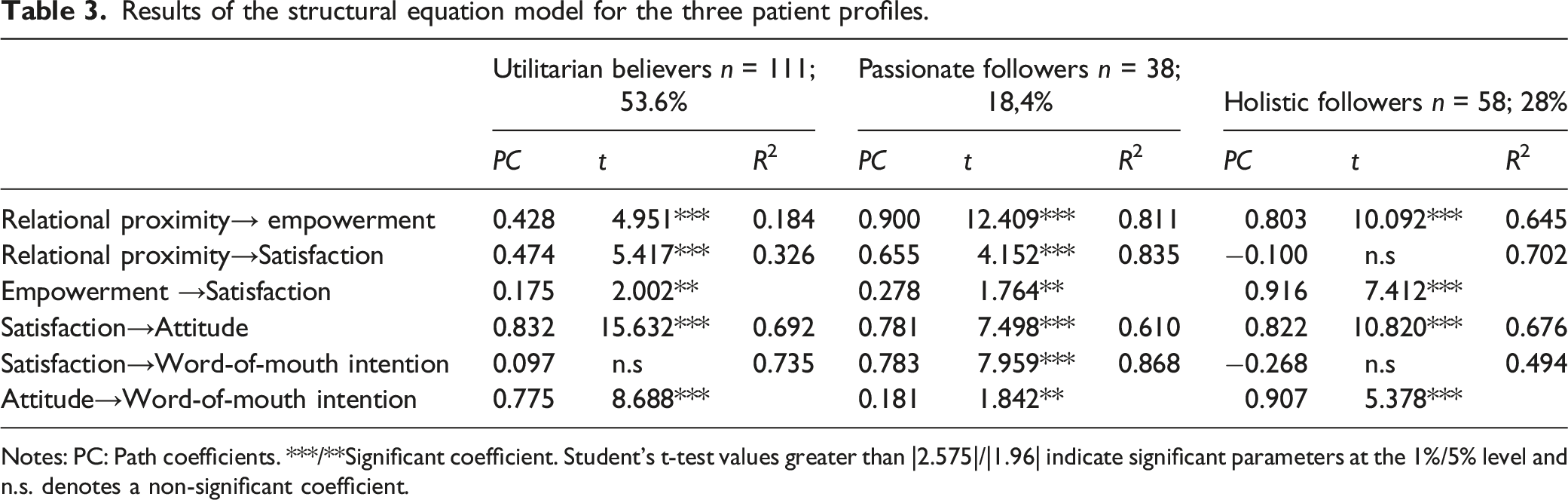
Notes: PC: Path coefficients. ***/**Significant coefficient. Student’s t-test values greater than |2.575|/|1.96| indicate significant parameters at the 1%/5% level and n.s. denotes a non-significant coefficient.
Group 2 patients, called passionate followers (18.4% of patients surveyed) prioritize the benefits of acquiring useful knowledge for their care pathway along with of support and guidance, which they rate very highly. In contrast, all other perceived benefits are also rated highly. Hence the overall perceived value is very high. In this group, post-empowerment is high and relational proximity to the TPE team is very high, along with their attitude and word-of-mouth intention toward TPE and satisfaction with TPE.
Further, relational proximity has a major positive influence on satisfaction in this group (PC = 0.655; t = 4.152***), both directly and indirectly via empowerment (PC = 0.278; t = 1.764*), which it favors strongly (PC = 0.900; t = 12.409***). In contrast, empowerment has only a weak, insignificant influence on satisfaction with TPE (0.278 < 0.655). Satisfaction again has a strong direct positive influence on attitude toward TPE (PC = 0.781; t = 7.498***) along with word-of-mouth intention (PC = 0.783; t = 7.959**). The relationship between attitude and word-of-mouth intention is only marginally significant in this group (PC = 0.181; t = 1.842**).
Group 3 patients, called holistic supporters (28% of the surveyed patients), all perceived benefits of TPE as being high and close hierarchically, together with overall perceived value. Post-TPE empowerment, relational proximity to the TPE team, attitude, and satisfaction with TPE are rated highly, and word-of-mouth intention is rated very highly. In this group, post-TPE empowerment has a major positive influence on satisfaction with TPE (PC = 0.916; t = 7.412***) (R2 = 0.702). However, relational proximity does not directly influence satisfaction with TPE (PC = −0.100; n.s.), but it strongly favors patient empowerment (PC = 0.803; t = 10.092***). The relationships established between satisfaction and attitude (PC = 0.822; t = 10.820***) and word-of-mouth intention (PC = −0.268; n.s.), as well as between attitude and intention (PC = 0.907; t = 5.378***), are similar to those seen in the utilitarian believers group.
Discussion
Theoretical and managerial contributions
On a theoretical level, this research validates most of the research model hypotheses relating to satisfaction with TPE proposed in reference to the objectives and specificities of this personalized care practice and to previous scientific work in health, TPE, and marketing. The findings provide insight into patients’ evaluative judgments regarding their experience of a TPEP, and confirm the contributions of the concept of perceived value to enrich the analysis of the links between satisfaction, its antecedents, and its consequences. Indeed, post-TPE empowerment, and relational proximity with TPE teams, are two major direct and/or indirect antecedents of satisfaction with the experience. However, nuances were observed according to the patients’ profiles in terms of perceived value of the TPE.
From a managerial standpoint, this research highlights the strong performance of a TPEP in terms of patients’ satisfaction with the experience and derived benefits. Thus, the actors of TPE teams will be able to improve the promotion of TPE contributions to various stakeholders (establishments, health professionals, caregivers, authorities, associations) as well as the development of this care service, which is still limited in oncology, due to several difficulties: administrative constraints, organizational complexities, but also representations of TPE and its benefits for patients vary greatly according to health professionals.
This research also suggests approaches for adapting the TPE to the profiles of the patients to enrich their experiences and derived benefits.
It might, therefore, be appropriate to strengthen the involvement of utilitarian believers in the management of their care pathway in order to better support them in developing their empowerment. In addition to relational proximity with the team, which is important for these patients, it would be advisable to communicate more about their potential needs, which may change during the course of their care. TPE could also be promoted to these patients as a specific source of empowerment to complement the services of other actors in their care pathway (including health professionals, patient associations, family, and friends).
For the patients who are passionate followers, it may be appropriate to reinforce the contribution of their post-TPE empowerment in their evaluation of their lived experience (which is largely influenced by their relational proximity with the TPE team), by valuing not only their cognitive, but also their conative, gains from their participation in a TPEP. Their empowerment skills could thus be developed by the TPE teams during the individual educational assessments integrated into their TPEP. These skills could also be enhanced by the referring physicians involved in their care pathway during their follow-up visits.
For holistic followers, for whom individual empowerment is the major antecedent of their satisfaction with the experience, an approach that highlights the overall benefits of TPE should be favored.
Finally, upstream, the awareness-raising actions implemented by the TPE teams to recruit patients into their programs should emphasize all the cognitive, utilitarian, psychological, and relational benefits of TPE that patients’ peers have derived. Patients can thus better understand and accept TPE, which is an important prerequisite for their decision to participate in this system that remains little known.
Limitations and research avenues
On a theoretical level, further research could be devoted to other antecedents of patients’ satisfaction with TPE: patients’ commitment in their care pathway, and the perceived quality of communication (e.g. empathy and responsiveness) with physicians and the TPE team of caregivers, and direct care services. Similarly, other consequences could be considered: (1) the adoption of tertiary prevention practices (physical activity and diet); (2) patients’ intention to become TPE patient ambassadors for health professionals and new patients; (3) patients’ intention to become partners in health institutions. Patients’ intentions might reflect patients’ social well-being in their post-care pathways.
Regarding the methodology, it might be worthwhile replicating this research with patients who have participated in a breast cancer TPE program in other healthcare institutions. Indeed, a multicenter approach, conducted with larger cohorts of patients, would allow us to control for the influence of other moderating variables related to the modalities of the programs. For instance, the mode of recruitment of patients (referral by the oncologists and/or approach of the TPE teams), the composition of the teams (e.g. involvement of patient partners), or the patients’ profiles (e.g. their personal environment or course of care).
This research could also be replicated with patients treated for other types of cancer, and the protocol could also be applied to other patient-centered oncology care services that contribute to these patients’ therapeutic education or support, such as supportive care. For better quality health care and services, the study findings also be used for e-health devices that promote patient empowerment, 35 particularly in oncology, through dedicated applications or platforms, intended specifically for patients whose visits to the facilities are limited (e.g. oral therapy, outpatient services, and geographical remoteness) to strengthen their participation in their care pathway and promote the co-creation of value.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.