
Abstract
Patients with transient ischemic attack (TIA) and minor stroke often struggle with long-term cognitive and psychological difficulties that impact their reintegration into work and leisure activities. The aim of the study was to evaluate the impact of a structured group-based stroke educational (SSGE) programme on patients’ ability to cope with a changed everyday life. Seven semi-structured qualitative interviews were conducted between February and March 2022 and analysed using thematic content analysis. The Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist was applied. The analysis uncovered three themes: ‘the existence of remaining challenges’; ‘the significance of support from resource individuals’; and ‘a sense of safety and confidence derived from the educational programme’. This study provides pivotal knowledge of how the SSGE programme supported patients’ long-term ability to navigate challenges after a TIA or minor stroke. The group-based format facilitated crucial exchanges of experience and knowledge with healthcare professionals and peers. However, the necessity for healthcare professionals to initiate post-support groups were underscored, as patients lacked the physical and mental strength to organise these on their own.
Keywords
Introduction
Stroke is a considerable cause of disability and mortality worldwide, contributing to a sizeable socioeconomic burden. 1 In Denmark, the annual incidence of stroke is approximately 16,500, with a slightly higher occurrence among men than women. 2 The number of people with stroke is expected to increase due to demographic changes, with the increasing number of older adults present in populations. 1 Stroke can be categorised into four subcategories: fatal (death); disabling stroke; minor stroke; and transient ischemic attack (TIA). 3 TIA and minor stroke account for 50%–65% of all stroke cases.4,5 A TIA is defined as the presence of a sudden focal neurologic symptom due to a temporary blood clot, lasting less than 24 h, typically resulting in no identifiable brain damage. 5 A minor stroke, also called non-disabling stroke, is commonly defined as a score ≤ 3 on the National Institute of Health Stroke Scale, yet a lack of consensus about the definition exists and real-world definitions are largely based on clinical judgement. 6 TIA and minor stroke are considered high-risk factors for secondary and more severe stroke events, with an estimated rate up to 17% after the stroke case.7–9 However, up to 80% of these events for patients with TIA and minor stroke may be prevented with appropriate and timely long-term intervention and lifestyle changes.9,10
The classic symptoms of TIA and minor stroke are sudden numbness/paresis (face, arm or leg), cognitive impairment/confusion, speech disturbances and challenges in comprehending language.11,12
Although it is commonly assumed that patients with TIA and minor stroke have short-lasting symptoms and recover fully, a growing body of evidence indicates that these patients experience continuing impairments, including cognitive and psychological difficulties.13–16 Moreover, these patients may exhibit atypical symptoms, such as recurrent headaches or a general sense of feeling ‘off’, which can persist beyond the initial stroke onset and present distinct challenges for their recovery.17–19 These challenges have serious implications for patients’ quality of life and their ability to reintegrate into work and social leisure activities post stroke.13–15
There have been major advances in the management of stroke in the last decades with early diagnosis and treatment with thrombolysis and/or thrombectomy in highly specialised units.20,21 The improvement of acute treatment has led to a decrease in the severity of strokes, enabling more patients to be discharged within a few days of hospitalisation. 20 Post-discharge care with follow-up and assessment by the early supported discharge team from the stroke unit or by municipal rehabilitation service (physical therapist, occupational therapist and/or speech and language therapist) has been implemented. However, a study revealed that patients discharged early after a minor stroke faced significant challenges in rebuilding a new everyday life while simultaneously battling with existential worries, mental exhaustion and the fear of experiencing another stroke. 13 Studies have also shown that patients have poor knowledge about stroke and its prevention, which can result in improper management of their health, increased risk of recurrent stroke and challenges in adapting to a changed everyday life. This lack of understanding can seriously impact their ability to return to work and engage in leisure activities post stroke.22,23 Furthermore, patients have expressed a need for improved access to healthcare professionals who possess specialised expertise in stroke as well as the opportunity to share their experiences with peers in similar circumstances after discharge. 13 A qualitative review has also revealed how lack of appropriate information and support after TIA and minor stroke can have a negative effect on patients’ psychological wellbeing and quality of life. 24 Therefore, it is pivotal to organise and tailor care interventions to ensure that patients are offered appropriate support and education to manage their condition and reintegrate into normal activities or work in a changed everyday life.
Given the various and complex impacts of stroke on patients’ everyday life, registered nurses (RNs) play a vital role in the care and rehabilitation of patients with stroke. They work alongside other healthcare professionals to assess patients’ needs, coordinate care, provide education and support, and facilitate rehabilitation. 25 Therefore, it is essential for RNs to have a comprehensive understanding of the experiences and needs of patients after stroke to provide optimal nursing care.
Research on educational programmes for stroke patients has primarily been quantitative and focused on outcomes such as mortality rates, risk factors such as hypertension and sedentary lifestyle, and prevention of recurrence.5,23 A recent scoping review revealed that follow-up care for individuals after a minor stroke primarily focuses on secondary prevention, with less attention given to hidden impairments and life adjustments post stroke. This highlights the need for more person-centred interventions that address the unseen challenges and support adjustments to a changed everyday life. 26 In addition, previous research has mostly focused on patients experiencing severe and disabling stroke. 27 However, the experiences and needs of patients with a TIA or minor stroke can vary significantly from those with more severe and disabling strokes. Tailoring healthcare services to address the specific challenges and needs of patients with TIA and minor stroke is crucial to improve outcomes and overall quality of life. 28 A structured stroke group-based educational (SSGE) programme was designed to enhance patients’ knowledge of stroke, prophylaxis and recovery to help them cope with altered aspects of their daily life. By understanding patients’ experiences and needs, RNs can develop and implement tailored interventions to provide effective care and support. 25 The aim of this study was to explore patients’ experiences after TIA and minor stroke to evaluate how the SSGE programme impacted their ability to cope with a changed everyday life.
Methods
This qualitative study employed a phenomenological hermeneutic approach with semi-structured interviews to explore patients’ experiences of the SSGE programme. 29 The term ‘stroke’ is used to refer to both TIA and minor stroke in this paper. The study was conducted between February and March 2022. The Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist was applied to ensure comprehensive and accurate reporting. 28
Setting
The SSGE programme was designed by multidisciplinary healthcare professionals from Aalborg University Hospital and the largest municipality in the north Denmark region, drawing on insights and experiences from previous research, practices in cardiac rehabilitation and people affected by stroke. Patient experiences were gathered through three focus group interviews with 16 patients and eight individual interviews. The aim was to provide advice, support, and knowledge of stroke prophylaxis (diagnosis, stroke risk, lifestyle change, preventative medication) and recovery (residual challenges and management strategies related to return to usual activities or work). The programme targeted patients after stroke, of whom the majority were discharged to their homes from the hospital within 72 h after stroke onset. The SSGE programme was conducted over a 4-week period and consisted of four sessions, lasting 2 h each. The sessions were taught by multidisciplinary healthcare professionals who possessed specialised expertise in the field of stroke, i.e. neuropsychologist, brain injury coordinator, stroke RN, stroke physician, dietitian, physiotherapist and social worker. The study participants also received standard care, including follow-up by the interdisciplinary stroke team from the hospital, the rehabilitation teams from the municipality and/or their general practitioner. The content of the SSGE programme can be acquired upon request to the corresponding author.
Participants
Out of 45 patients and their relatives, 10 were selected through a purposeful sampling to participate in the SSGE programme approximately 2 months after their first or recurrent stroke. 24 The patients were selected based on factors such as age, sex, socioeconomic status, educational background and occupational status to ensure a representative sample comprising individuals with diverse demographic characteristics. Nine patients participated in the SSGE programme after one patient declined to participate. All nine patients were invited for individual interviews 5–6 months after the SSGE programme; of them, seven patients (age range = 48–77 years) agreed to participate and were included in the study. Two patients had a TIA and five patients had a minor stroke. Five of the patients attended the SSGE programme with a relative. One patient received thrombolysis and thrombectomy. Patient characteristics can be seen in Table 1.
Patient characteristic.
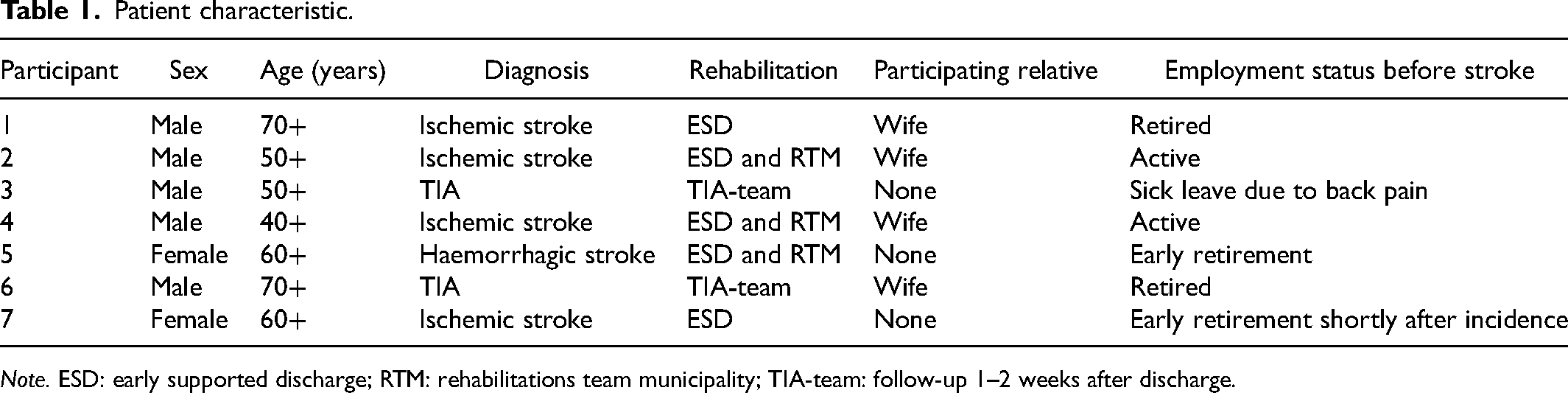
Note. ESD: early supported discharge; RTM: rehabilitations team municipality; TIA-team: follow-up 1–2 weeks after discharge.
Patient characteristics
Data collection
Data were collected using a semi-structured interview guide, allowing patients to express their experiences in their own words. 29 The areas explored covered topics such as the impact on daily life, challenges faced, coping strategies, support received, and the perceived effectiveness of the SSGE programme. Examples of questions in the interview guide are as follows: What challenges did you face after your TIA/minor stroke? How did you cope in the period after your TIA/minor stroke? How did participating in the SSGE programme impact your understanding of stroke, recovery and management of daily life? What was helpful or lacking in the information and support provided in the SSGE programme? and How do you consider the role of healthcare professionals in supporting individuals after a TIA/minor stroke based on your own experiences? The interviews were conducted by two female researchers: an associate professor and a Master of Public Health, who were both experienced interviewers. The interviewers had no prior knowledge of the participants. The interviews were conducted by telephone and lasted approximately 29 min each (range = 23–38 min). All interviews were digitally recorded and transcribed verbatim.
Data analysis
A phenomenological hermeneutic approach and content analytical steps were used by the authors, who are all RNs: one specialised in stroke care and two had a background in clinical nursing research.30,31 The interviews were initially read and re-read by each of the three authors to get a sense of the whole and overall content. Based on this process, significant meaning units were identified. Subsequently the three authors performed a common interpretation and latent meanings were extracted. At this stage, the analysis transitioned from focusing on the explicit content of what was said (‘what was in the data’) to interpreting the underlying subject matter of the data (‘what the data was about’), reflecting a deeper understanding. The analysis involved a continuous back-and-forth process where each of the researchers’ pre-understanding was considered by questioning each other's interpretations until consensus was achieved.30,31 An example from the analysis is illustrated in Table 2.
Example of the process of content analysis.
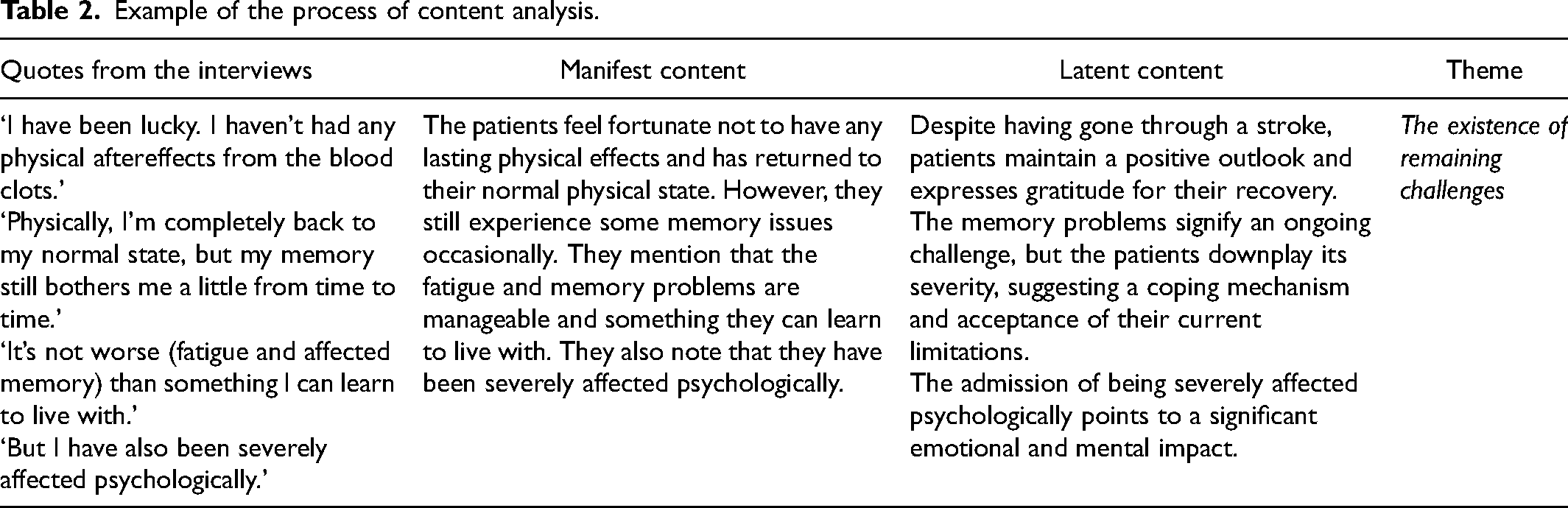
Example of the process of content analysis
Ethical considerations
The study has been registered at the Danish Data Protection Agency (ID number 2021–174). In accordance with Danish regulations, the study did not require additional ethics approval as qualitative studies are not subject to ethical clearance from the Danish National Committee on Health Research Ethics. 32 The patients signed informed consent before they were enrolled in the study after receiving verbal and written information about the study. Furthermore, they were informed of their right to withdraw from the study without consequences. The data were handled anonymously in all stages of the study. Ethical standards and guidelines for research involving human subjects were strictly adhered to.33,34
Results
The analysis resulted in three themes: 1) ‘the existence of remaining challenges’, focusing on how patients manage their everyday life 6–8 months after stroke and how their symptoms decreased over time; 2) ‘the significance of support from resource individuals’, focusing on the necessity of ongoing support from others to manage persistent challenges in everyday life; and 3) ‘a sense of safety and confidence derived from the educational programme’, focusing on both benefits and areas in need of improvements in the SSGE programme.
The existence of remaining challenges
The patients’ immediate reaction during the interviews was great relief and they vocalised the shared experience of having had an easy recovery from the stroke. When asked to elaborate, they describe it as being lucky, to be able to be as before or as not being hit harder, which all refer to the fact that they had recovered without serious physical disabilities and motor impairments. However, further on in the interviews and maybe on additional reflection, the patients described how they at this time in their recovery still battled to fully recover from a cognitive and psychosocial perspective. These deficits were described as lapses of memory and mental fatigue. I've been hit hard psychologically. (7) …I’m completely back to my normal physique, but my memory still teases me occasionally. (5)
As demonstrated by the latter quote, patients’ physical health seemed to be in the forefront and the main determinator for measuring their recovery, while the remaining cognitive and mental deficits were vocalised as secondary. For some patients, the deficits were a constant reminder of their stroke and affected the quality of their daily lives, whereas for others the deficits were mild and transient and appeared in relation to, for example, not being able to do crosswords or accounting as before. It (the fatigue and memory lapses) is not worse than what I can live with. (5) I don’t feel like I am the master of my own life anymore. (7)
As the latter quote shows, some patients had difficulties mastering and regaining control over their lives, yet they described a change to the better as times has passed. The difficulty of regaining control could be connected to how they were used to plan and structure their everyday life before the stroke, as described by this patient: In my world, there shouldn’t be too many new things happening unless I’m told in advance, so I can plan, but if suddenly something (like this) happens it disturbs me, and I don’t even know which leg to stand on. (3)
The stroke event affected this patient's normal habits to a degree where the patient lost the ability to fully manage and control their own life. However, in the 6–8 months that had passed since their stroke event, the patients expressed that they had become better at listening to their bodily signals and the necessity to do so. The symptoms with fatigue I have had after (the stroke), well those signals I must listen to. I can feel how my body can’t participate anymore, and that I need to take a break. (2)
The patients described how their symptoms improved over time, which, combined with changes in lifestyle and medical treatment, alleviated their anxiety about experiencing a new stroke. However, a lingering worry seemed to become a constant companion as described by this patient: I’m not worried about getting another stroke, or yes you are always a bit worried. But I’m pretty sure I won’t get another stroke because I’ve changed my diet and I do a little exercise every day. So, I have done the things I can, which helps prevent this from happening again. (3)
The patients told how they limited themselves in their everyday life in relation to exercise and diet. Limitations in exercise were most pronounced soon after their stroke event and became less pronounced as time passed. The following quotes illustrate limitations shortly after the patients’ stroke events: …if I went on walks, I always made sure it was somewhere I knew people would come. (7) In the beginning, I kept sitting in my chair afraid of what would happen if I lifted heavily or got my heart rate up. (6)
Progress in their recovery was measured by looking backwards and being able to see improvements, which encouraged the patients to maintain their plan of recovery. …In the beginning I had a chair in the kitchen, now I’m cooking, I’m boiling eggs, toasting bread, making rolls and things like that STANDING. I think: ‘Stop it! Now I can stand and juggle things again.’ After all, there was a long period where I could only do one thing at a time. (5)
Hence it seemed as if self-registration of progress became a tool for these patients, which helped them manage and adapt to their new normal daily lives.
The significance of support from resource individuals
Most patients reported that they benefitted from support from others to help them adapt to a changed everyday life. Four patients attended the educational programme with a relative and three without. All but one patient expressed having great support from one or more near relatives. During the programme, the relatives supported the patients by being additional listeners, posing relevant questions and engaging in discussions about the educational content. I asked my wife to join the programme with me as my ‘memory secretary’ because when I hear the information it goes in one ear and out the other, information doesn’t get stored as quickly as before. (2)
The patients underlined how their near relatives experienced similar feelings of insecurity and worry to themselves, and that the relatives needed the programme just as much as they did. The relatives supported the patients, e.g. by making sure that the patient kept following the stroke-friendly diet or was the one dragging the patient on daily walks. I would like to mention that my wife has listened well to the information they gave on the courses, and it has actually produced good results, now, e.g., milk has been changed from regular to low fat milk and that is quite a lot less calories in terms of fat percentage. (6)
Although support from relatives was appreciated, it could also be annoying, as illustrated by these quotes: My daughter likes to throw salad leaves on my plate. I don’t really want people to interfere with what I eat. (6) My wife was nervous too, and I was not allowed to do certain things like lift heavy objects and so on. (1)
Despite occasional annoyance, patients conveyed an understanding that the relatives’ persistent reminders stemmed from genuine concern for their loved ones’ health and wellbeing. In addition to this support from their near relatives, the patients expressed a need for reassurance and someone with whom they could share existential worries, fear of relapse and fear of never regaining the everyday life they had before the stroke. Like one patient described it: What happened? How do you move on from this? (4)
But also, minor topics that disturbed or troubled them in their daily lives were discussed: Well, I have discussed this thing with my practitioner. I don’t know if it is normal. I think it might be caused by the medication I have to take. I ‘m not short of breath but suddenly my heart is pounding. (7) I had to take these pills; however, I couldn’t open the blister pack without crushing them. Then I talked to the foreman of our swimming club, and he told me to insert my nail in the package and tip it, now I can get them out without crushing them. (6)
The patients sought resource individuals in their network to help them manage a changed everyday life. As the above quotes show, these resource individuals could be an acquaintance from the local sports club, a deputy member of the trade union or a general practitioner. Both the near relatives and other resource individuals had very different competencies and bases of knowledge.
A sense of safety and confidence derived from the educational programme
The patients expressed great satisfaction and gratitude to have been invited to attend the SSGE programme. They agreed that it contributed to increase their knowledge base about various topics, such as dieting, exercising and what to expect after a stroke. They described it as feelings of being helped on the way, being held by the hand and being helped to hold it together in a time characterised by uncertainty, insecurity and worry in a situation that was not in their control. Yes, [the programme provided] good information, which helped me clarify and confirm what happened. (1) Just being told what’s normal and that others also feel this way [made me realise] I’m not alone. This is how it is, but over time it will become better. (3)
Referring to the time before the SSGE programme, the patients experienced a lack of knowledge of stroke physiology, and they sometimes misunderstood what was happening with their body. For example, a patient thought that the blood clot was moving inside his body waiting to get stuck elsewhere after the stroke. I had the impression that it [the transient blood clot] was still running around inside me and then suddenly it could settle somewhere else in my brain or heart or somewhere else. (3)
As this quote demonstrates, the knowledge provided by the healthcare professionals in the SSGE programme helped patients ease their worry.
The increased information also helped the patients make stroke-friendly decisions, e.g. regarding their diet and exercise plan, with clear results. [Before the stroke] my weight was 116 kg and in the last 6 months I have lost 18 kg. (3) Thinking back to before the stroke, my body is actually in better physical shape because I’ve kind of stuck to training three times a week. (4)
The patients agreed on the benefits of attending the programme in a group as the group dynamics were important. They described how new questions appeared when they spend time with others in similar situations. Furthermore, they found that other patients’ inquiries provided answers to questions that they, themselves, may not have been able to articulate. … it’s one thing to read it on a piece of paper – it’s another thing to sit face-to-face and talk about it in person. Other questions appear, and I got instant answers to my questions. (2) When you are with a group of people who are all in the same situation, and hear what they voice, and it's actually THE SAME problems I have. No matter how annoying they are [the problems], it’s actually nice to hear others feel the same way. (7)
Meeting and talking to peers in the same situation as themselves seemed to help the patients understand what was normal and help them better accept their new reality.
The patients had different requests to what could have improved their benefit of the SSGE programme. Additional time was requested to provide opportunities for more dialogue between peers as well as more time for revisiting topics covered in previous lessons and for asking clarifying questions. Even though the patients reported that they appreciated and benefitted from the group dynamics, no lasting connections to other participants in the group were established. The patients clearly needed a network of fellow stroke survivors as it would provide an informal space for an exchange of experiences, but they seemed to lack the bandwidth to initiate contact, as exemplified in this quote. Unfortunately, I don’t have the bandwidth for it myself, because then I would have done it [build a network]. But it is also the situation I have ended up in, where I’m not able to work and concentrate for long at a time. So, it probably wasn’t the right time to set about trying to build a network. (4)
The patients found it difficult to know where to get answers to their questions after the programme was terminated. Suggestions were made as to how to organise such networks in which questions that appeared and became relevant over time could be addressed. Yes, a place where we can meet occasionally. Or have a platform where we could communicate in the group and say: ‘We go for a walk Thursday next week, if you’re up for it’. Well, it's an opportunity to touch upon what we have learned, or what we have experienced, so that we could help each other. (2)
The patients expressed feeling reassured by the presence of the healthcare professionals and experts in their fields during the programme. However, after the programme was terminated, the patients felt left on their own/alone again. Some things you need a long time to process. And this was one of those. We attended the programme four times. And before I knew it, they were finished and then I was kind of left alone again. (4)
The latter quote points to the importance of acknowledging that recovery after a stroke takes time and support from healthcare professionals may be needed at different time points during the recovery phase.
Discussion
The aim of this study was to explore patients’ experiences after TIA and minor stroke to evaluate how the SSGE programme impacted their ability to cope with a changed everyday life. The main findings were: ‘the existence of remaining challenges’; ‘the significance of support from resource individuals’; and ‘a sense of safety and confidence derived from the educational programme’. These findings collectively highlight the importance of a structured SSGE programme, facilitating exchanges with both peers and healthcare professionals, to enhance patients’ coping abilities. This will be further discussed in the following.
The study showed that even though patients were relieved that they had recovered without serious physical disabilities and motor impairments, the experience of having had a stroke had markedly changed their everyday lives. The patients continued to experience different degrees of psychological and cognitive residual problems in the long term after the stroke. The patients’ main problems were memory failure, mental fatigue, uncertainty, anxiety and difficulties in reasserting control over their lives; some to the degree where it affected their wellbeing and the return to former activities in their everyday life, while for others it only had minor consequences affecting them in relation to specific tasks. Similar to our findings, other studies found that TIA and minor stroke can have a negative impact on patients’ everyday life and wellbeing, which are in contrast to the previous assumptions that patients with minor stroke and TIA recover rapidly without disability and cognitive residual problems after the event.11,35,36 Hence, the residual symptoms patients experienced 6–8 months post stroke can be challenging and negatively affect their rehabilitation and recovery process. 37 The battling of existential concerns, mental fatigue, cognitive deficits and the fear of another stroke, as found in previous studies for patients after 2–4 weeks and 3 months post stroke, remains comparable for patients in this study at 6–8 months post stroke.13,38 However, our data suggest that the patients at this stage of recovery had become better at listening to their bodily signs and had increased their knowledge of stroke compared to earlier stages after their stroke. This improvement in the patients’ awareness and knowledge suggests a positive progression in their recovery, potentially enabling them to cope better and make more informed decisions regarding their health and wellbeing.
The patients perceived that participation in the SSGE programme contributed to the increase in their knowledge base, which helped them to better understand their condition. For example, the patients increased their knowledge about the connection between stroke and nutrition, daily exercise and normal reactions post stroke. Furthermore, the patients experienced that participating in the SSGE programme prepared them with knowledge and strategies to reduce psychological distress. Hence, it helped them regain control, which eased their feelings of insecurity and worry about a new stroke. This is an important achievement, as previous studies have shown that many patients and their relatives are dissatisfied with information from healthcare professionals and have limited knowledge of stroke and important associated issues. 39 Therefore, our study underscores the crucial role of providing an educational programme to assist patients in managing their condition in their daily lives.
Patient education has been shown to improve health literacy and reduce symptoms of depression, which are common problems after a stroke. 40 Post-stroke depression is known to affect approximately one in three individuals after a stroke. Patients with post-stroke depression have a higher risk of suboptimal recovery, diminished quality of life and increased mortality. 41 Hence, it is important that healthcare professionals are aware of patients experiencing residual symptoms and difficulties in their return to usual activities, as these challenges may potentially contribute to depression and other negative outcomes. 11 It remains unclear which methods are most appropriate and effective for the delivery of information to patients after stroke. However, evidence suggests that approaches actively involving patients are favourable compared with providing information passively, and that the latter may even risk worsening anxiety and depression after stroke. 39 Similarly, our study showed how active involvement supported patients to feel in charge of their life and reduced their anxiety regarding a recurrent stroke. Based on our findings, we cannot conclude that patients with severe symptoms require more education and support compared to patients with mild symptoms. Nevertheless, we argue that tailoring education and support to the specific needs of these patients are essential for their return to everyday life and wellbeing.
Our study highlighted the advantages of sharing experiences with peers during the SSGE programme, complementing the formal information and support provided by healthcare professionals. The significance of peer support, rooted in shared backgrounds and experiences, aligns with recent findings in a review indicating that peer support benefits patients’ wellbeing and health outcomes. 42 This form of support diminishes feelings of isolation and offers opportunities for information and experience exchange.43–45 Peers can provide specific practical, emotional and affirmational knowledge and support to each other, which differs from professional knowledge being theoretical and segmental.45–47 The patients in our study requested additional time and space to share thoughts and experiences with peers. After the termination of the SSGE programme, the patients expressed feelings of being on their own again and a need for ongoing connection and networking with peers facing similar challenges as themselves. However, none of the patients in this study had the bandwidth for building this network themselves. This suggests that there may be a need for assistance from healthcare professionals to initiate peer support groups after the educational programme. Previous research findings also suggest that interventions requiring patients to seek help on their own, such as giving a telephone number to a patient or their family at discharge after a stroke, may appear to provide follow-up but are ineffective, as patients often do not take the initiative themselves. 16
The patients in our study saw relatives as resource individuals and appreciated their attendance, which patients considered supportive, incentive and reassuring for their recovery. In particular, the relatives played a valuable role in assisting them to remember, comprehend and apply the provided information into their everyday life. The importance of the attendance and support from relatives may be attributed to the fact that memory impairment and difficulties with retaining new information are well-known symptoms for stroke patients.48,49 However, the involvement of relatives was occasionally seen as nagging and annoying for some patients. This is in line with research showing how relatives’ overprotective behaviours or excessive worries can cause the patient to feel more physically inert and dependent.50,51 Hence, the involvement of relatives presents an inverse relationship between benefits and drawbacks; although relatives provide support to the patient, the patient may also perceive them as being overly protective. Furthermore, our study underlines how the relatives were equally insecure and nervous and needed knowledge of stroke and stroke-friendly behaviour just as much as the patients. Previous research describes how stroke is a disease that affects not only the patient but also those close to the patient.52–55 This demonstrates the need for an educational approach where both patients and relatives are provided with sufficient knowledge of stroke and rehabilitation to facilitate their engagement in positive health behaviour. All patients in this study, except one, found support from their close relatives, but they also found support from other persons in their network, e.g. a swimming club foreman. The question is if these relatives and random individuals possess sufficient competencies and knowledge to provide the needed support. This clearly emphasises the need for and relevance of the SSGE programme taught by healthcare professionals with specialised knowledge in stroke as well as the necessity of tailoring the programme to the specific needs of the individual patient.
Limitations
The study is limited by being confined to a single hospital, which limits generalisability of the findings. Moreover, two researchers conducted the interviews, which potentially may have introduced variability in the data collection process. To address this concern, both interviewers adhered to a semi-structured interview guide and engaged in discussions to ensure consistency in their approach throughout the interview process. Furthermore, the study had a limited population of seven participants. However, further data collection was considered unlikely to yield significantly new results as no new or additional insights and themes reoccurred during the last interviews. Hence, the results demonstrated a comprehensive and in-depth knowledge of the patients experience of stroke and how the SSGE programme positively impacted their ability to cope with a changed everyday life.
Conclusion
The findings indicate that the SSGE program appeared to enhance patients’ ability to navigate challenges persisting in the long term after experiencing a TIA or minor stroke. The format of group-based education facilitated crucial experience and knowledge exchange with both healthcare professionals and peers. Moreover, our findings emphasise the necessity of allocating additional time within the programme for meaningful dialogue with healthcare professionals and peers, allowing for comprehensive exploration of topics covered in previous sessions. Our findings underscore the significance of involving multidisciplinary healthcare professionals with expertise in stroke in organising such programmes. In addition, we identified a critical need for ongoing support from healthcare professionals to establish post-programme peer support groups, as many patients lacked the bandwidth to initiate this themselves due to physical or mental constraints. We believe that these insights will significantly inform the continued refinement and advancement of educational initiatives for post-TIA and minor stroke patients, both domestically and internationally.
Footnotes
Acknowledgements
We extend our sincere gratitude to the participants for their invaluable contributions in sharing their experiences of stroke and how the SSGE programme affected their ability to adapt to a new daily life. We would also like to express our appreciation to Sara Jacobsen, Master of Public Health, for her involvement in conducting the interviews.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.