
Abstract
Hybrid professionals have a two-fold – professional and managerial – role, which requires appropriate management skills. Investing on managerial training programs aims to empower professionals with managerial skills and competencies. Does this pay back? Assessing the impact of such training programs is still a limited practice. This paper explores whether participation in managerial training programs in healthcare can enhance the involvement of hybrid professionals (namely, clinical directors) in top management decision-making. The mediational effects of knowledge of performance information and its use are explored.
Survey data were collected from more than 3000 clinical directors of 69 public health authorities from five regional healthcare systems in Italy. Relationships between participation in managerial training programs, performance management practices (i.e., knowledge and use of performance information) and the level of clinicians’ involvement by the top management were studied using a three-path mediation analysis with structural equation modelling. Propensity score matching was also performed to mitigate selection bias.
Knowledge and use of performance information positively mediate, both independently and sequentially, the relationship between clinical directors' participation in managerial training programs and the level of their involvement in decision-making.
The results of the study suggest that managerial training can support hybrid professionals in engaging with managerialism and playing upward influence on top management decision-making.
Keywords
Aim of the study
The role of managerial training (MT) for professionals is a widely studied topic in literature. Training is associated with the creation of new roles, concepts, the development of skills and attitudes, the synthesis of tacit knowledge, 1 and it is believed to be a change-promoter mechanism.
In the public sector, MT primarily relates to strengthening employees’ engagement and promoting change, by increasing their capacity to meet existing and emerging demands. 2 In healthcare, the purpose of training is deeply related to the role of doctors–managers who are often referred to as hybrid professionals.3,4 Since important leadership responsibilities are given to professionals whose role is both clinical and managerial, clinicians are often asked to bridge the worlds of medicine and management 5 to ensure quality of care, clinical outcomes and financial sustainability, which are tightly interconnected rather than conflicting goals. 6
Besides, management practices related to the use of information and performance management tools by professionals have been found to predict organizational performance7–9 thus giving further support to the claim for having “clinicians on the board”.10,11 This refers to clinicians being actively involved in the planning, delivery and transformation of healthcare services and, more broadly, of the health systems they are fundamental parts of. 10 Involving doctors in management can help improve organizational performance by nurturing management practices in healthcare settings,12,13 and numerous strategies have been aimed at fostering collaboration between doctors and the top management. 14 The most institutionalized one is indeed through formal MT. However, the relationship between MT and the improvement of managerial practices is still lacking evidence-based investigations, especially when excluding so-called smile sheets-based analysis. 15
This study investigates the relationship between the participation of clinicians with management roles (i.e. clinical directors) in MT programs and their performance management practices, considering 69 public health authorities from five regional health systems (RHSs) in Italy. a We show how the participation in MT programs predicts a higher interaction of hybrid professionals with the top management. We explore the mediational effects of knowledge of performance information and use of performance information (UPI). Our comparative analysis also raises questions about the heterogeneity of these relationships across different RHSs.
The paper is structured as follows. The next section gives some preliminary considerations inferred from the literature on management practices and training within professional organizations. The subsequent section presents the research hypotheses and methodological issues. The results of the analysis are then discussed, highlighting the insights and limitations. Lastly, the conclusions and suggestions for further research are reported.
Background
HRM and MT in healthcare
Healthcare organizations are increasingly challenged by pressures on new ways of governance, improved efficiency and patient orientation. 14 Among the various change-promoting strategies available, those based on human resources management (HRM) are the most common in the public sector because of the people-centered nature of service-oriented organizations. Both scholars and practitioners have thus devoted great attention to these initiatives particularly after the new public management (NPM) reforms, based on the existing evidence linking HRM to performance outcomes in healthcare. 16
Traditional professional bureaucracies have evolved accordingly, leading to a managerial-like characterization of professionals and their competency models, namely throughout performance-oriented techniques.8,17 Performance management, indeed, is proved to be a supporting mechanism for organizational change in the public sector by means of goal clarity and purpose, strategic alignment, motivation and adaptability. 18
Training objectives depend on the training needs of the specific organization and the tasks involved. 19 In the Italian National Healthcare System (NHS), the laws (legislative decree 502/92 and presidential decree 484/97) require heads of department to accomplish an MT program of a minimum of 100 certified hours, in order to take charge of their role. The objectives of MT, as defined by Italian law, include: training in interpersonal skills, leadership, effective communication, conflict management, team building; training in cognitive skills and problem solving; tools and techniques concerning the managerial role (general management logic). The latter may include, for instance, the following: performance management, budgeting, goal setting and strategic planning, innovative organizational and operational schemes. MT programs are offered on a regional basis and involve multiple methods, including lectures in conjunction with discussions, simulations, business case studies, role-playing and team project work.
Hybrid professionalism: Implications for competency models and training
In healthcare, the role of management is to ensure strategy implementation through efficient and effective public service delivery. 7 In order to attain these goals, management requires a broad set of competencies, ranging from unit-specific technical skills to engagement-building capacity. 20 Indeed, managerial apex in healthcare organizations often corresponds to clinical leadership, 5 thus requiring the hybridization (not juxtaposition) of their clinical culture with a managerial one.3,21 The former is based on the strong patient–doctor relationship, collegial authority and personal responsibility for decision-making. In contrast, managers believe that their primary allegiance is to the organization, authority is hierarchical and responsibility for decision-making is shared. This implies a peculiar “inverted” power structure, where traditional hierarchy is unlikely to be effective. 22 Because of their “hybrid” function, 4 then, these roles need to encompass managerial values and cross-competencies: in the case of clinical directors, for instance, they need to handle not only high-level clinical competencies, but also organizational and relational skills in order to take charge of the overall clinical provision, organization and leadership of their departments and report to top management. This trend is also confirmed by the broad international attempts to redefine medical professionalism.23,24
The concept of competency is generally defined as the “capability of applying or using knowledge, skills, abilities, behaviors, and personal characteristics to successfully perform critical work tasks, specific functions, or operate in a given role or position” (Ennis, 25 p. 4). In the public sector, managerial competencies are multidimensional, contingent and dynamic, as a result of reforms and the particular context in which public organizations operate. Training is thus paramount to maintaining and developing employees’ competencies. It is defined as the set of organizational activities aimed at fostering the acquisition of knowledge, rules, concepts, or attitudes needed to build specific skills and professional competencies 1 which should result in the improved performance of the trainee. 26
To this end, there is an increasing demand for training programs in healthcare management, especially for medical professionals in leadership positions who need to acquire managerial and leadership skills. 27
Does MT matter? Research question and hypotheses
Assessing training requires the systematic collection and analysis of information on training programs, which can be used to plan and drive decision-making as well as to evaluate the effectiveness of the training components. Measuring the effects of training on an organization or individual behaviour is necessary to evaluate the return on investment and the value-for-money of the interventions provided 28 and to increase their accountability.
However, organizations spend little time on evaluating the return on investment of MT programs, due to a lack of confidence in whether training has an impact on organizational performance, as well as a lack of resources, expertise and organizational support. Healthcare is no exception. Despite several significant examples, the impact of management training on healthcare professionals still needs to be explored.
In general, there are two important issues related to evaluating training. First, the assessment of training programs traditionally relies on the immediate feedback provided by trainees, e.g. “smile sheets” or satisfaction surveys. Second, measuring the effects of training on individual behaviors creates difficulties in empirically establishing the causal chain: the more time elapses between the provision and the assessment, the more likely latent intervening variables cannot be considered. Even when some kind of relationship emerges, it is difficult to explain its nature and to suggest improvement paths for training models. 2
In the face of the limited empirical evidence, our study aims to provide a deeper understanding of the relationship between participation in MT programs in the Italian NHS and some management practices by clinical directors. Based on Kirkpatrick’s model, 29 which assesses the effectiveness of training based on the nature of its effects (reactions, learning, behaviours, results), we adopt a threefold perspective dealing with learning, behaviour and results-related effects.
Within the “learning” dimension, we measure the outcomes of the training, focusing on the acquisition of performance information related to organizational goals and results: indeed, the spread of a “culture of measurement” in the Italian NHS30 followed an increasing need for timely and accurate information on care service provision, that has been also recognized by the law. b It is reasonable to expect management training to provide trainees with specific performance information, such as targets and feedback information on outputs and outcome, efficiency and effectiveness, needed to monitor and (re) orient their professional and managerial activities. However, a study recently carried out in the UK4 suggests that the mere acquisition of competences over management technicalities does not make a difference in terms of the enactment of hybrid roles.
Within the “behavioral” dimension, we then measure the capacity effects of training. Training, indeed, is expected to give trainees an increased individual decision-making capacity in order to meet new demands set by incumbent changes and reforms. 2 However, in order to provide “a basis from which leaders make capacity decisions” (Moynihan and Ingraham, 31 p. 430), performance information should be “usable”: to this end, information should be provided through performance measures that monitor multiple dimensions, in quantitative and aggregate format and are publicly disclosed, thus favoring benchmarking.32,33
With respect to “results-related” effects, which is the most distal and macro criteria, we focus on the level of involvement in decision-making of the clinical directors by the top management. Indeed, greater clinician participation in shared decision-making is a well-recognized key competence for clinical leadership34 and has been found to have broad potential benefits for health organizations,
35
such as the mitigation of professional conflicts, cost control, and quality improvement. Whereas management scholarship generally confirms a positive relationship between the involvement of doctors in clinical governance and several dimensions of performance, it seems quite blurry what this ‘involvement’ is about. A recent cross-country study
36
shows that the role of doctors in top management decision-making is often consultative, more than decisional, and that this is the case of Italy. Nonetheless, the same study shows a significant relationship of the involvement – whatever its intensity – with quality of management systems. Since clinicians' involvement can be considered an antecedent of both high-quality management systems and high-performing healthcare organizations, our study aims to investigate its association with participation in management training programs.
Sample and methodology
Sample
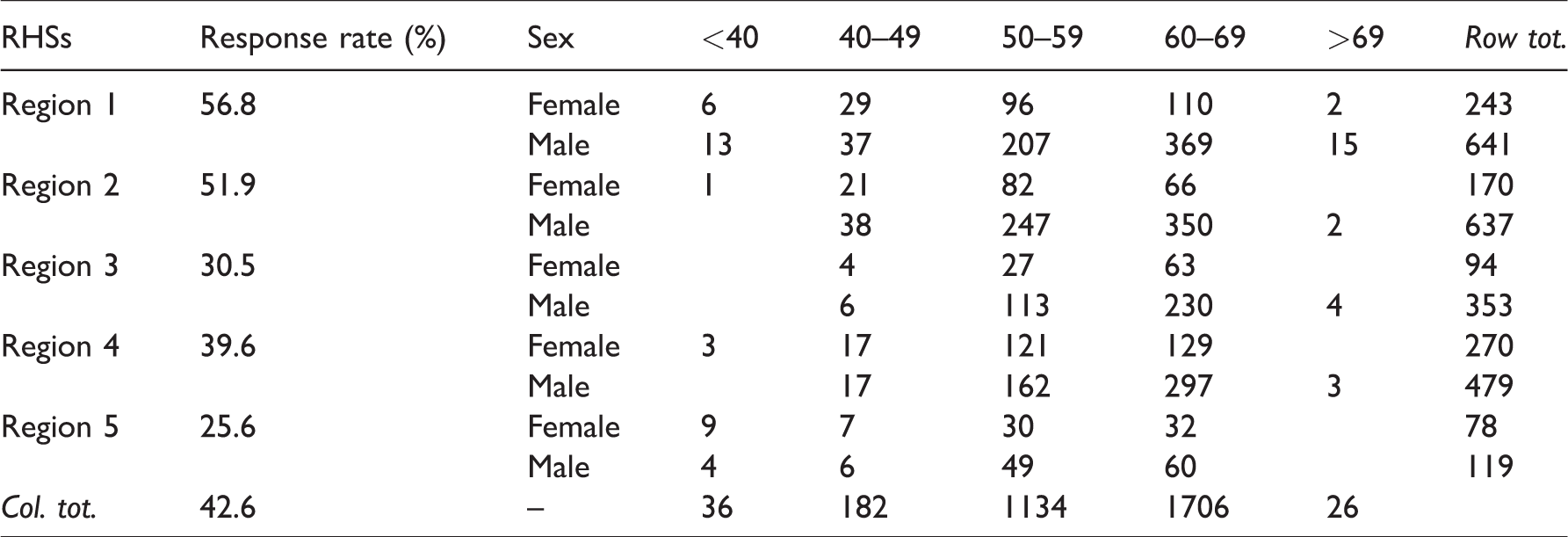
In order to test the four hypotheses, we used data collected from a routine organizational climate survey sent approximately every two years to the healthcare personnel and staff of 69 public health authorities from five Italian RHSs. The five Italian RHSs are a balanced representation of northern, central and southern Italy. The sample includes 14 teaching hospitals and 55 local health authorities. The organizational climate survey is an individual-based questionnaire with a specific item regarding attendance at an MT program and contains items related to on-the-job management and performance management behaviors and skills. The survey can thus be used to assess the learning and behavioural effects of MT. The organizational survey is administered via computer-assisted web interviewing (CAWI) on a census basis, 37 and its data contribute to the Inter-Regional Performance Evaluation System (IRPES). IRPES is an evaluation tool currently adopted and funded by a network of 13 Italian regional administrations on a voluntary basis, aimed at collecting the performance data of health authorities for benchmarking. 38 Surveys were administered between 2014 and 2017 involving 219,084 employees, of which 9095 were professionals with a managerial role; 4174 professionals with a managerial role took part in the surveys. To answer our research question, only medical personnel’s responses were considered in the analysis, though the authors acknowledge an extensive stream of research dealing with other health professionals’ managerial role, such as nurses’ managers 39 ; also administrative and technical managerial personnel were excluded; after this exclusion step, 3084 observations were considered (corresponding to 43% of the overall medical population). After controlling for listwise-deletion, all these observations were included as no incomplete responses were detected. The final sample was composed by 72% male and more than 90% over 50 years’ old respondents, with noticeable differences across Regions (see Table 1).
Response rate and composition of the sample.
Measures
This section provides an overview of all the measures included in the study (see Table 2). The independent variable is MT, a binary variable that measures participation, whenever in time, in an MT course by clinical directors (as defined by legislative decree 502/92 and presidential decree 484/97). The mediator variables are performance information knowledge (PIK) and use of performance information (UPI). The dependent variable is clinical directors’ involvement (CDI) in decision-making by the top management.
Composition of the variables.
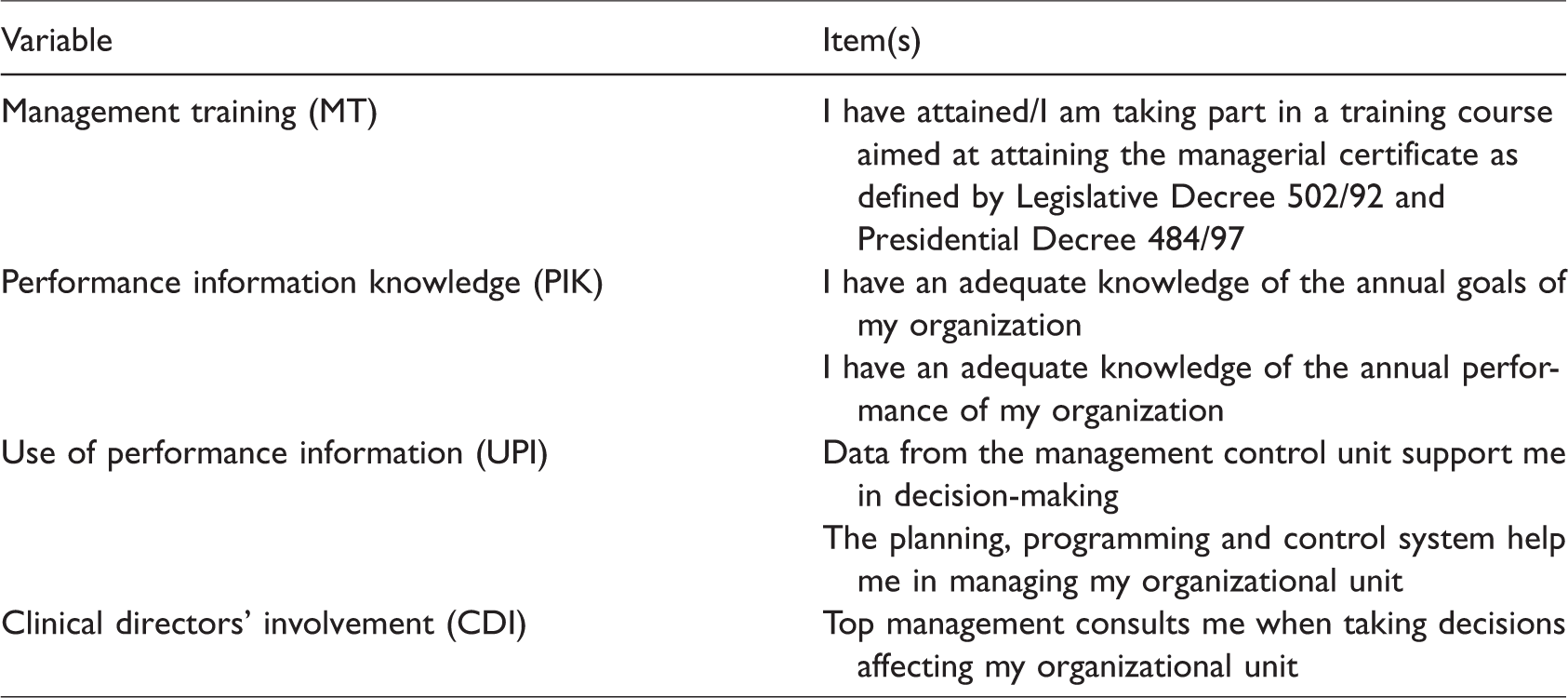
PIK is measured as a combined indicator of two items included in the organizational climate survey, addressing respectively the knowledge of annual organizational goals and performance results. UPI is measured as a combined indicator of two items reported by the organizational climate survey, addressing, respectively, the use of information on organizational performance provided by the management control system in supporting individual decision-making and budgeting in the daily management of the organizational unit under the respondent’s responsibility.
CDI is based on the response values of a single item in the survey, addressing the level of involvement of the respondents by the top management in decision-making. Cronbach’s alpha was used to estimate the internal consistency of questions that comprised several items (Table 3). Age and sex of the respondents were included in the model as control variables. For all the accounted variables, with the exception of MT, age and sex, respondents were asked to respond to items on a five-point scale: from 1 (strong disagreement) to 5 (strong agreement). The individual responses were then transformed into a 100-point scale. All statistical analyses were performed with SPSS 22.
Descriptive statistics and correlation levels (overall).
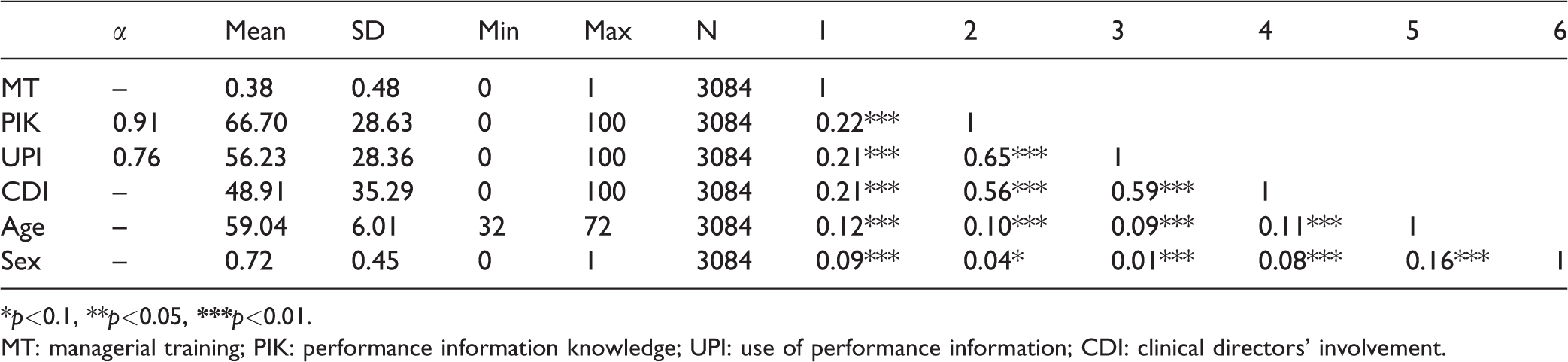
*p<0.1, **p<0.05,
MT: managerial training; PIK: performance information knowledge; UPI: use of performance information; CDI: clinical directors’ involvement.
Modelling
To model the different effects of training, we used a three-path mediation model, depicted as a path diagram in Figure 1. According to our research model, H1, H2 and H4 represent mediation hypotheses, which posit by what means an independent variable affects a dependent variable through mediators. The specific mediational effects, total mediational effects and direct effects were calculated.
Figure 1(a) describes the total effect of MT on the involvement of clinical directors in decision-making, c being the path coefficient of MT on CDI. This total effect can be arrived at via a variety of direct and indirect forces. 40 Specifically, in Figure 1(b), the total effect of training on the involvement of clinical directors in decision-making can be expressed as the sum of the direct and indirect effects, the latter being estimated by the product of the path coefficients for each of the paths in the mediational chain. The advantage of path analysis is that it isolates the indirect effect of both mediating variables, that is, the PIK (H1: a1b1) and the UPI (H2: a2b2). In addition, this approach analyses the indirect effects passing through both of these mediators in a series (H4: a1a3b2).
To test our mediation hypotheses, we used an analytical approach 40 aimed at testing the indirect effect between the independent and the dependent variables through the mediator via a bootstrapping procedure. This technique 40 estimates the mediation effect and overcomes the limitations of other procedures (such as the choice to free or constrain residual covariance). We then performed the above-mentioned analyses separately for the five RHSs, in order to highlight possible differences in the magnitude or significance of the effects across RHSs. We expect a positive relation between exposure to MT and interaction of clinical directors in decision-making with the top management, since training should improve awareness of performance information and capacity to use such evidence to support clinical directors’ leadership role.
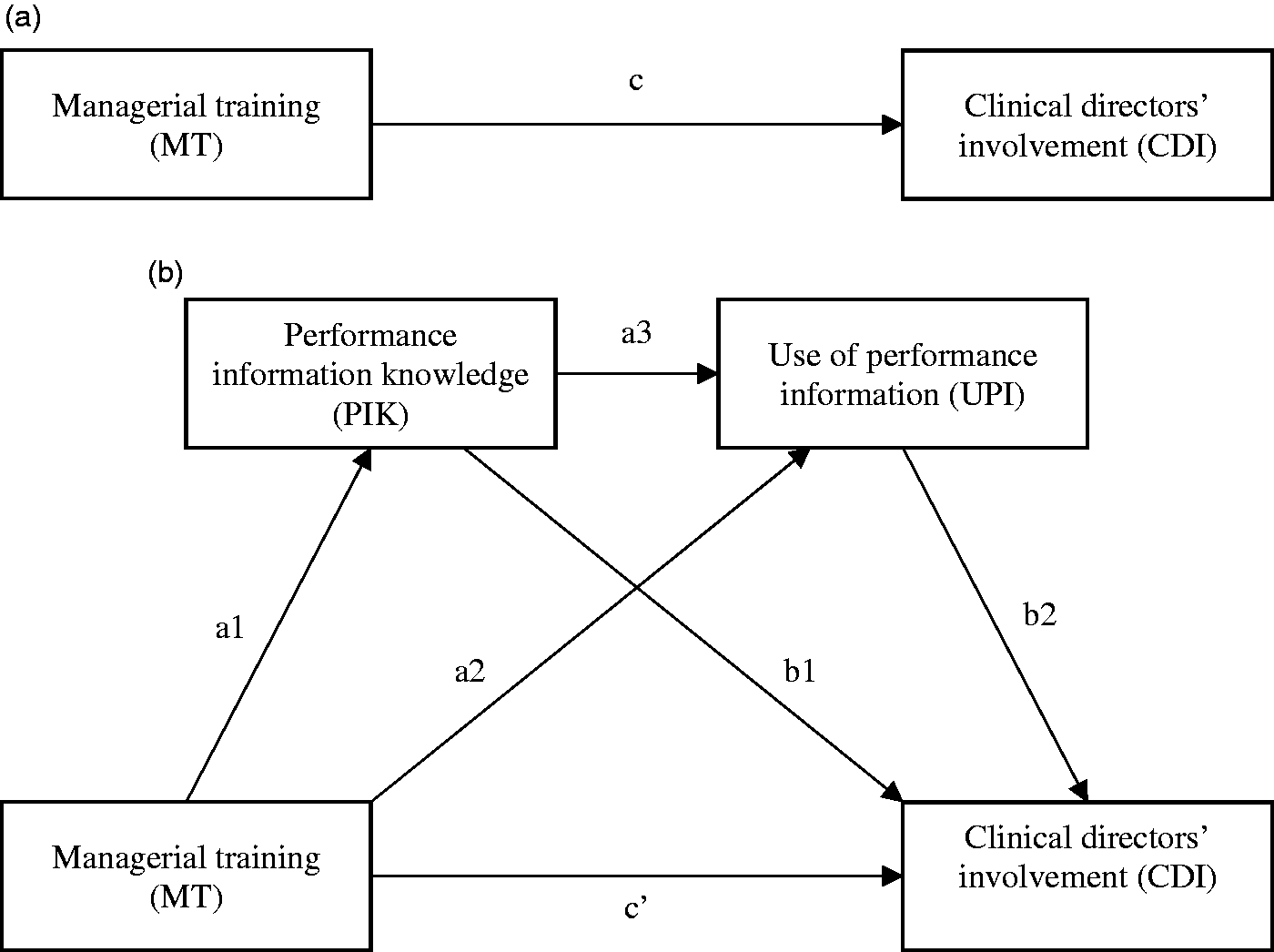
Relational model.
Results
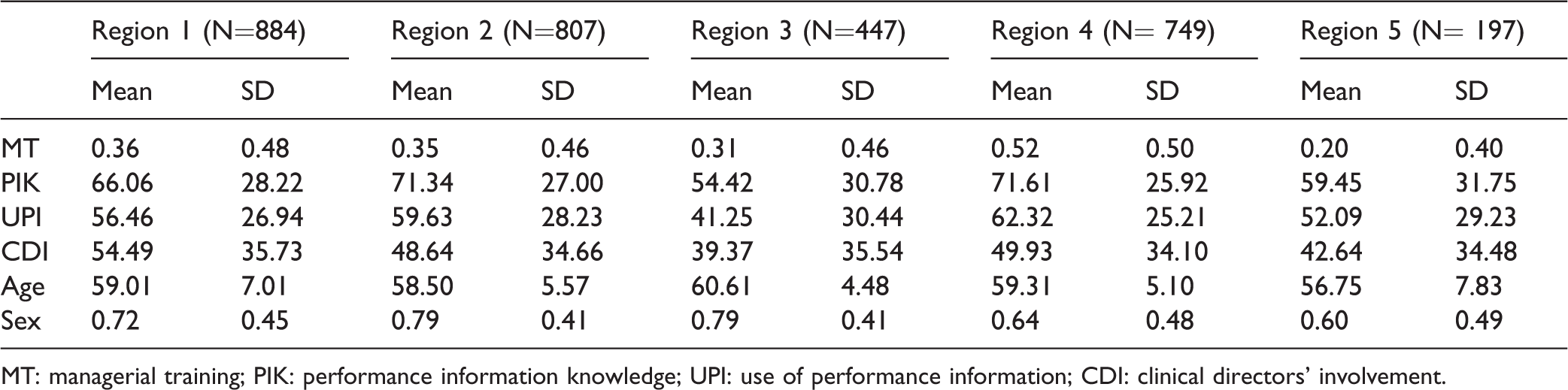
Table 3 provides descriptive statistics and correlation levels. Participation in MT programs ranges from 20% in Region 5 to over 50% in Region 4, with a mean participation rate of 38%. Though the available data does not allow for deductions for such a low and differentiated participation rate, compared to the underlying legal requirement, several possible reasons can contribute to explain it (e.g. formalization of the managerial role, appointment-accomplishment lag-time, law enforcement and control). The factor associated with the acquisition of strategic performance information registers an average a score of 66.70 out of 100 points; the UPI records a lower average score of 56.23 out of 100; involvement in decision-making by top management records a mean value of 48.91 out of 100 points. Significant differences, however, emerge from regional-level analysis (see Table 4), with Region 3 displaying a systematically lower average level for mediator and dependent variables
Descriptive statistics (by RHS).
MT: managerial training; PIK: performance information knowledge; UPI: use of performance information; CDI: clinical directors’ involvement.
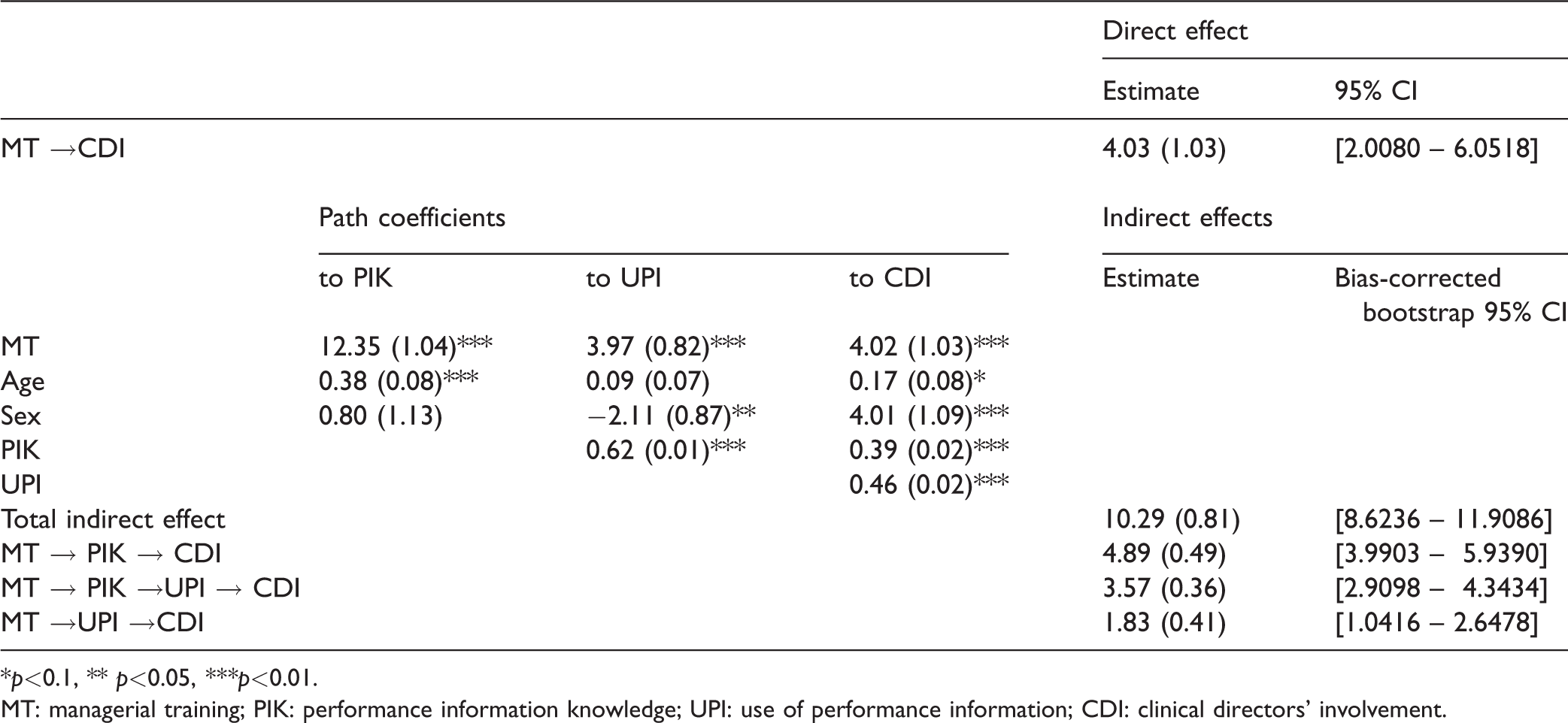
In the structural model analysis, we estimated all the path coefficients, simultaneously controlling for respondents’ age and sex (Table 5). We tested for a three-path mediation effect and the structural model fitted the three-path mediation model reasonably well. Although the χ2 value was significant (χ2 = 14.46; p<.05), this could be related to the sample size 41 and, in the end, should not be considered as impedimental. Goodness of fit indexes showed encouraging values, with CFI higher than 0.95 (0.998) and RMSEA lower than 0.05 (0.027).
Results (overall).
*p<0.1, ** p<0.05, ***p<0.01.
MT: managerial training; PIK: performance information knowledge; UPI: use of performance information; CDI: clinical directors’ involvement.
Results provide strong support for all the suggested hypotheses (Table 5): participation in MT among clinical directors has an indirect effect on CDI, which is mediated by PIK (H1) and UPI (H2). This relationship is also sequentially mediated by the two mediator variables (H4), suggesting that in our sample, participation in management training provides participants with crucial organizational and performance-based information and, thus enhances their ability to capitalize on this information in order to play a role in top management decision-making. The direct effect of the independent (MT) on the dependent variable (CDI) confirms H3, and the fact that it remains significant after adding the mediators enabled us to identify a partial mediation effect. Each lower and upper bound value for the 95% confidence intervals around each indirect effect failing to contain zero supports the mediation hypothesis.
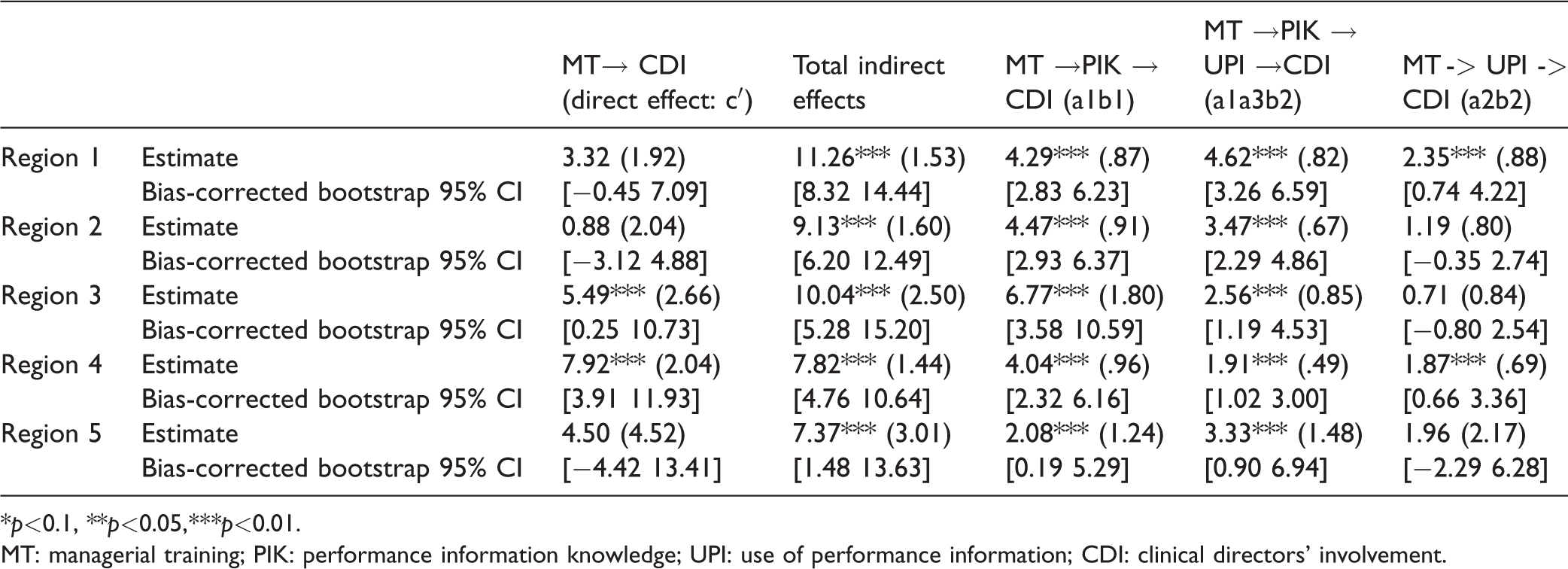
Several interesting insights emerge from the region-based analyses (Table 6). In addition to differences affecting the size of the indirect effects among regional contexts, only two out of the five RHSs in the sample (Regions 1 and 4) showed a significant mediation effect of the use of performance-based information in the relationship between the independent and the dependent variables. In the remaining RHSs, only the first mediator’s (PIK) indirect effect and the sequential path remained significant, thus reducing the second mediational effect (H2).
Results (by region).
*p<0.1, **p<0.05,***p<0.01.
MT: managerial training; PIK: performance information knowledge; UPI: use of performance information; CDI: clinical directors’ involvement.
Limitations
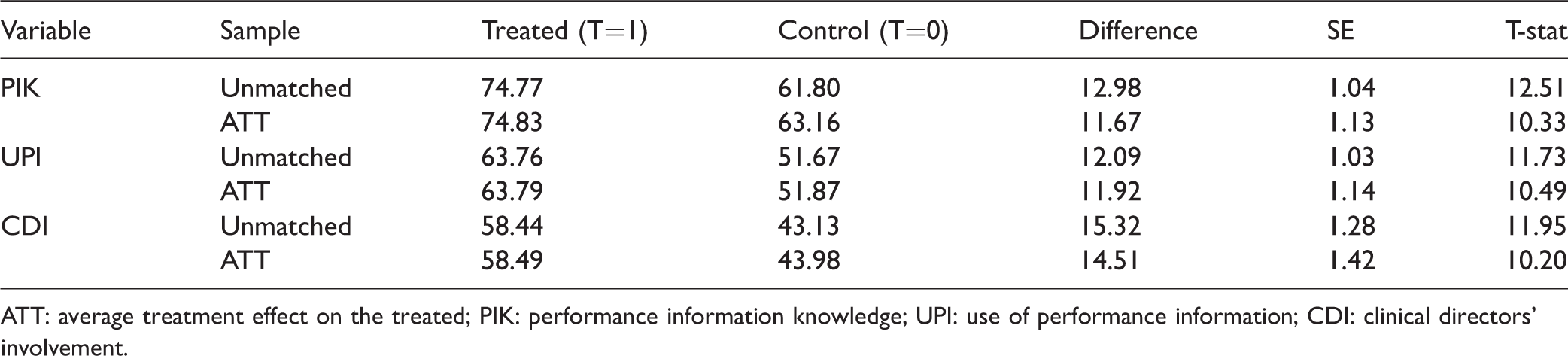
The usual limitations of cross-sectional survey research should be kept in mind when generalizing from this study. One limitation is selection bias, i.e. the possibility that medical professionals with a higher interest in performance information and budgeting use were more likely to participate in training. To reduce this bias, we performed a t-test analysis adjusted for propensity score matching 42 based on respondents’ characteristics (age, gender, organizational affiliation). c
When computing the propensity score, all variables considered at some stage in our model as dependent (including the mediators) showed a significantly different mean value between the two groups defined by the participation in management training, after matching the samples over individual characteristics (Table 7). This seems to mitigate the selection bias.
Propensity score matching.
ATT: average treatment effect on the treated; PIK: performance information knowledge; UPI: use of performance information; CDI: clinical directors’ involvement.
In addition, the observational nature of the data did not allow to test the causal relationships between the variables. The present study, therefore, must limit itself to describing the association between participation in MT programs and individual outcomes of hybrid professionals (such as learning, behaviours and results).
Also, due to data availability, in the relational model, we did not include contextual factors (favorability of the post-training environment in the performance of learned skills), trainer effects (characteristics of the training partner), quality of the training content, and trainee effects such as motivation, cognitive ability, self-efficacy and goal orientation. 19 The context in which hybrid professionals apply the MT skills, indeed, tends to promote or hinder such acquired capacity. Management scholarship broadly acknowledge how management capacity at the level of the single public sector organization is fundamental in explaining adoption and use of managerial tools. 43 Health organization is indeed rather heterogeneous, and our sample is no exception in this regard. In addition, our results are limited to a sample of management training programs promoted in 5 of the 21 RHSs in Italy, due to data availability.
Discussion
The literature on training evaluation extensively adopts Kirkpatrick's 29 taxonomy, considering reactions to training, learning effects, behavioural effects and results. Our results provide various important insights: at the level of learning effects, participants in management training (regardless of regional affiliation) showed a sounder knowledge of performance-based information, such as annual goals/targets and indicators for goal achievements compared to their counterparts. Training encouraged professionals to consider performance information as an important component of their management expertise and to make sense of numbers and in identifying meaningful indicators. In terms of behavioural effects, this led professionals to use information more systematically to support decision-making and, thus, to an increased interaction with top management. As already mentioned, the latter is recognized to be a predictor of organizational performance in healthcare. 10
Overall, trained medical professionals tend to be more aware of organizational goals and results, declare to adopt a more systematic use of managerial operating systems (e.g., budgeting and strategic planning) and performance information to support day-to-day decision-making and to get more involved by the top management in decision-making, compared to their untrained colleagues. Gaining performance information-related capacity can thus contribute “to create a common ground for decision-making based on a common language” 5 between professionals and the top management.
It is to note, for instance, that our sample includes RHSs that adopt a well-developed Performance Measurement System (IRPES) that yearly discloses multidimensional healthcare performance indicators from financial viability to quality and patient satisfaction, through a systematic and publicly disclosed benchmarking. 38
Beside these effects, being referred to by Kroll & Moynihan 2 as informative and capacity-building, the cross-regional analysis also raised questions regarding institutional alignment effects. Indeed, differentiated paths emerged in the relationship between MT and managerial practices. This underlines, on one hand, the important role of the features of regional training models: for example, the two RHSs in which empirical data show a mediational circuit through the UPI are – based on the composition of their curriculum d – those with a stronger orientation to the use and discussion of multidimensional performance indicators as a learning practice. Indeed, Regions 1 and 4 devote a very large proportion of their training to peer discussion of multidimensional performance indicators, related to both national (National Outcomes Program e ) and regional (IRPES f ) performance evaluation systems. On the other hand, it is reasonable to expect that not only features of the training models impact the nature of the described mediational effects, but also that institutional conformity and convergence matter. 44 Though this study only partially look at this aspect, available research reports how training can be considered a socializing setting where perceptions and expectations about the organization, social norms and institutional values are formed and communicated. 45 Further investigation would be much needed to illuminate these relationship under the lenses of institutional isomorphism. 44
Another result of this study that opens room for additional investigation concerns the nature of the role of clinical directors and their capacity to span organizational and professional boundaries 46 : evidence has been collected on the increased involvement in top management decision-making, for doctors undertaking MT programs. However, the results of this study provide no indications about the effects of MT on how this role could be played by hybrid professionals with their reports or peers. In other words, it seems quite clear that clinical doctors with management training play their role to “exert upward influence” (Detmer, 46 p. 471), but not as much if and how they play it downwards.
McGivern et al. 4 propose a useful distinction in this regard, categorizing incidental and willing hybrids: the former refers to professionals who represent and protect traditional institutionalized professionalism, while temporarily in hybrid roles, and the latter describes those who engage with managers and managerialism, “disrupting traditional professionalism […] and reconceptualizing [it] in terms of delivering the best care for patients collectively” (Mcgivern et al., 4 p.15). The results of this study seem to suggest that those taking part in MT tend to better master performance management tools, thus leading to their higher involvement in top management decision-making processes compared to their untrained colleagues. This increased involvement seems to indicate a first clue for a reconceptualization of professionalism, towards a blurry combination of their role. Nonetheless, further investigation is much needed to understand how hybrid roles evolve in relation, especially, to the professional component of their work identity.
Last, we can argue that those clinicians attending MT programs overcome resistance towards management by experiencing how management practices can also enact their professional role. In other words, management may get more appealing for clinicians through MT, by virtue of a sense-making effect.
Conclusions and future directions
The healthcare sector needs to tackle a particular level of complexity when dealing with the different mutual stakeholder relationships: the function of top management is to “enable” professionals’ role,47 and support clinicians in identifying care pathways that respond properly to the needs of patients. In this context, healthcare professionals shape, through their clinical practices, the most of the cost structure of the organizations and, only by means of their job, organizations can achieve long-term health outcomes and sustainability.
Internal communication of performance information is thus key to effective clinical governance, as well as the adoption of shared codes, languages and culture. Kippist and Fitzgerald pointed out that among “barriers to the effectiveness of the role of hybrid clinician manager,” it is well recognized “the lack of management education and skill” (Kippist and Fitzgerald, 48 p. 647]. Based on these premises, our study explores the role of MT in facilitating clinicians’ involvement in management.
In particular, the analysis shows how MT has a positive effect on the knowledge and UPI system, emphasizing improved dialogue and discussion with top management. Besides, MT can be the arena where to support hybrid professionals in overcoming resistance towards management issues21,49 and to bridge the gap across professions and roles. Based on existing research carried out by other scholars, this could also relate to a certain extent to reputational effects: when embedded “in a social process of collegial competition” (Bevan et al., 50 p. 12), the UPI can create peer group pressures to aspire to higher performance. Focusing on those very performance measures similarly used in day-to-day management activities, training can prepare clinical directors to really dive into benchmarking techniques in a simulation environment meant to recreate reality-close decision-making dilemmas, similar to those they are required to cope with in their managerial role.
Despite the aforementioned limitations, evaluating the effects of training over time is an important step towards the adoption of an evidence-based approach in management training. In line with a recent research strand 27 aiming to overcome so-called smile sheets-based approach to training, 15 this study describes healthcare professionals’ management practices and relate them to participation in MT programs. We pursue this research objective by using large-scale empirical evidence drawing on primary data collected in five Regional Health Systems in Italy. Technological instruments and information technology (for instance, CAWI) can also help to foster this trend. Future research should attempt to identify how factors such as training delivery methods, quality of training content, trainee effects and post-training environment could influence the observed effectiveness of management training and foster the conversion of trained skills into increased capacity of hybrid professionals. Furthermore, research should also investigate the association between MT and organizational performance, by exploring the indirect effects of enhanced performance management competencies among professionals.
Footnotes
Acknowledgments
The authors wish to thank Dr. Nicola Bellé and Prof. Milena Vainieri (Scuola Superiore Sant’Anna, Pisa) for their precious comments on previous versions of the paper and all the researchers of the MeS Lab (Scuola Superiore Sant’Anna, Pisa) for their valuable support. The authors also wish to acknowledge the regional administrators and staff of the five Regions involved in the study taking part in the IRPES. Eventually, the authors wish to thank the editors and reviewers, whose comments and suggestions significantly contributed to the improvement of the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.