
Abstract
Most medical, clinical and health education programs require students to complete quality improvement (QI) training. This curriculum expands on the biomedical model of healthcare delivery to a value-based one aligned with quintuple aim goals. While QI can offer immediate service enhancements, contributions to improve the broader health system at national and international levels remains limited. This paper addresses this issue by exploring how QI training can be reimagined through a translational research pathway or a Translational Health Service Improvement Program (THSIP) delivered in partnership between 4 Local Health Districts in New South Wales, Australia and 2 Australian Universities. Informed from a modified Delphi design, this study reports 12 elements for a THSIP. The THSIP ensures students have: organisational support to conduct research within required training timelines, access to translational research training and mentorship, and finally, structures to support evidence uptake. These aspects are addressed through the THSIPs program management, skills development, and implementation components. The THSIP equips students with skills to make systemic service enhancements relevant for other organisations, domestically and internationally.
Keywords
Introduction
Quality improvement (QI) is a required curriculum element for most medical, clinical and health-focused training (Bowes et al., 2023; Myers et al., 2020). Medical education accrediting bodies, including the Accreditation Council for Graduate Medical Education, and health training providers require students, with the support of a mentor, to complete QI projects aligned to their health service’s priorities. The goal is to reduce variability in quality of care, reduce health disparities, and improve health outcomes for patients and the broader population (Clinical Learning Environment Review Evaluation Committee, 2024). Whilst there is a distinction between QI and health services research (Eljiz et al., 2023), an empirical research pathway incorporating an improvement focus can advance trainee skill development to make immediate service enhancements, and broader systemic improvement through evidence dissemination. This justifies reviewing the QI curriculum for an improvement-focused translational research pathway.
Postgraduate students’, however, have been reported to experience four different types of challenges in conducting translational studies. These include knowledge acquisition, brokering relationships and managing dynamics, scoping projects aligned to industry need, and finally, navigating course timeframes (Cassidy et al., 2021). For knowledge acquisition, postgraduate students are researchers-in-training, so learning about translational methods is a new and emerging area for them (Cassidy et al., 2021). Their skill in conducting studies with both knowledge developers and knowledge users grows throughout their project. Therefore, there is a limited starting foundation with which to guide the completion of their studies (Lal et al., 2015). Similarly, as knowledge translation is still an emerging methodological discipline, the number of guidelines for ‘how-to’ conduct applied studies is limited (Gallant et al., 2023; Lal et al., 2015). This makes it further challenging for students looking for pre-existing methodological guidance for their research.
Brokering relationships and dynamics between academics and health professionals can be complex. Often students are external researchers or ‘outsiders to a health system or organisation with which the research is being conducted (Cassidy et al., 2021). This makes it challenging for students to understand the context and culture of the knowledge users. Particularly, students may not know how to adapt collaborative processes to accommodate health organisational cultures with academic ones (Cassidy et al., 2021; Newman et al., 2015). Additionally, there are often competing priorities for stakeholders in health organisations and universities (Lal et al., 2015). Without sufficient contextual knowledge and insight of these, it can impede capacities to effectively communicate with project team members. Students have also found it difficult to scope projects according to health practitioner and health organisational needs (Cassidy et al., 2021; Tait and Williamson, 2019). While review of strategic, operational and other organisational plans may provide some awareness of the organisations long and short-term goals (NSW Health, 2024), insider knowledge of the organisation’s culture and internal strategy to attain those goals, is also required to scope an applied and feasible study (Taylor et al., 2025).
Finally, project completion is also bound by academic timeframes (Cassidy et al., 2021). For Postgraduate students completing a Master’s research project, students may have a few months to 1 year to complete their research (Australian Government, 2025). Those timeframes, when combined with other competing priorities for health staff and academics, makes it difficult for students to feasibly complete the project (Lal et al., 2015). The program infrastructure required to support students to navigate the above challenges remains a key methodological gap for postgraduate research training focused on health service improvement. As those challenges span both academic and healthcare organisation and systems, it is important that any guidance is informed from both perspectives. This study aims to be our first step to address that gap. It aims to draw on the practical and contextual expertise of health practitioners and academics to identify the program infrastructure necessary to enable students to make both health system improvements and a contribution to knowledge.
Accordingly, this study aims to address the question: ‘What are the essential elements of a University-Health Service Improvement program that enables translational health service improvement?’ The 12 elements below, informed from a modified Delphi study, offer a way for higher education training providers and health services to develop an improvement-focused research pathway for medical, clinical and health students. The elements are derived from translational health improvement initiatives delivered by two Australian Universities, which combined, worked in partnership with four metropolitan Local Health Districts in New South Wales, Australia. The students are health staff and enrolled in postgraduate health degrees. This positions students as insiders to the health system, who due to the partnership between their health organisation and the universities, have access to both academic and industry supervision for service improvement research training.
Combined, the 12 elements represent the THSIP model, and are arranged into three key areas. First, the program management elements detail the governance needed to integrate university research training in a health organisation. Second, the skills development elements explain how senior health and academic staff can partner to scaffold learning for applied research competency. Finally, implementation elements outline how health organisations can disseminate and translate student research findings, whilst retaining skilled alumni.
Methods
A modified Delphi design was adopted for the THSIP project. The Delphi technique is useful to develop expert-based judgement or consensus about an issue or topic (Barrett and Heale, 2020; Jünger et al., 2017; Niederberger and Spranger, 2020). This process can be useful for adding some practical validity to some evidence or results because it is informed from both the acquired formal knowledge about an issue or topic and experiential expertise of knowledge users (Jünger et al., 2017; Niederberger and Spranger, 2020).
Application of the Delphi technique allowed for consensus development about a translational health improvement model from academics and practitioners, who have direct experience with initiative implementation. While there is evidence for existing quality improvement patient safety programs for postgraduate medical, clinical and health service education, there remains little guidance offered regarding the management of improvement health service research programs in health degrees (Cassidy et al., 2021; Myers et al., 2020).
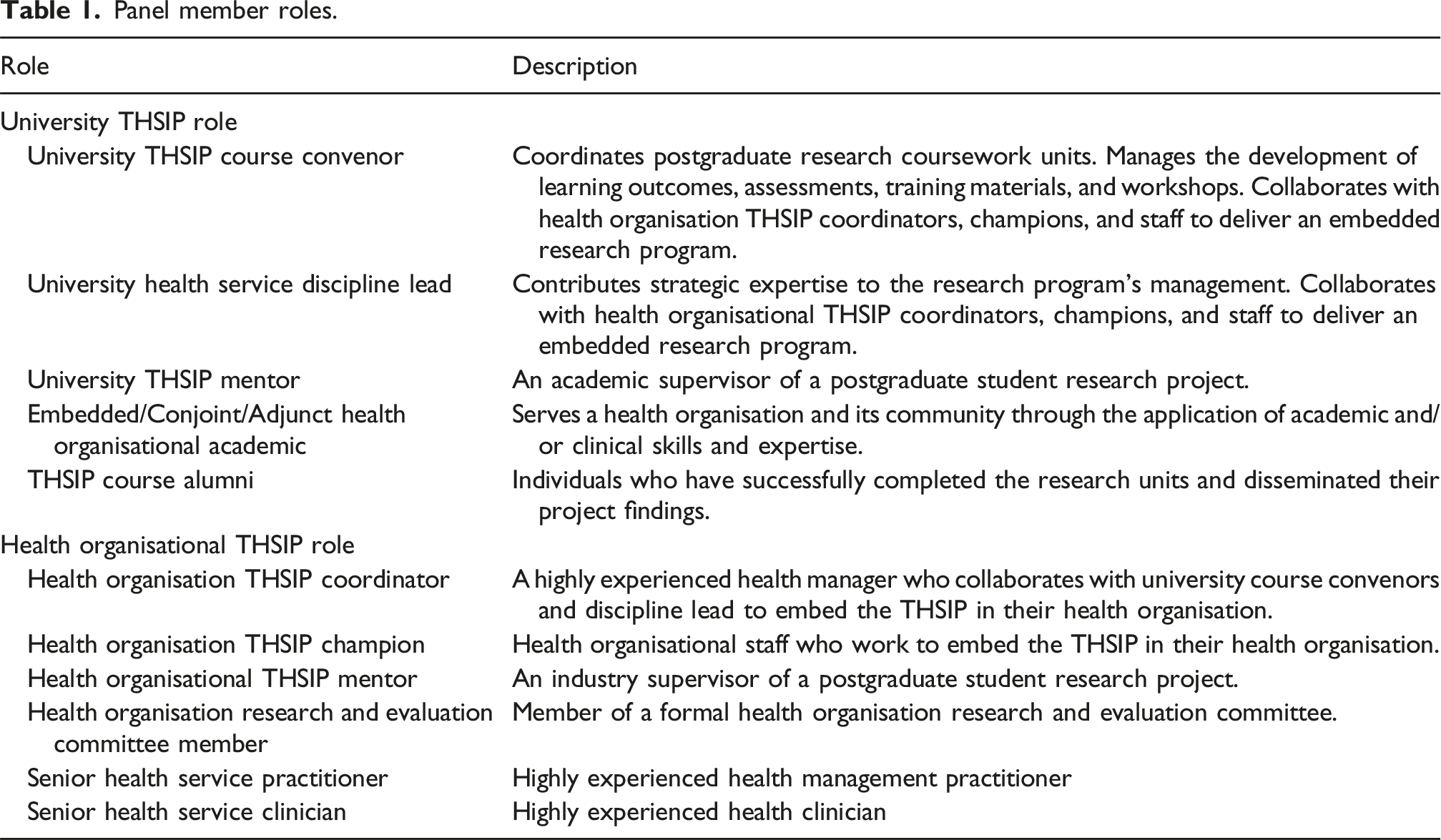
Panel member roles.
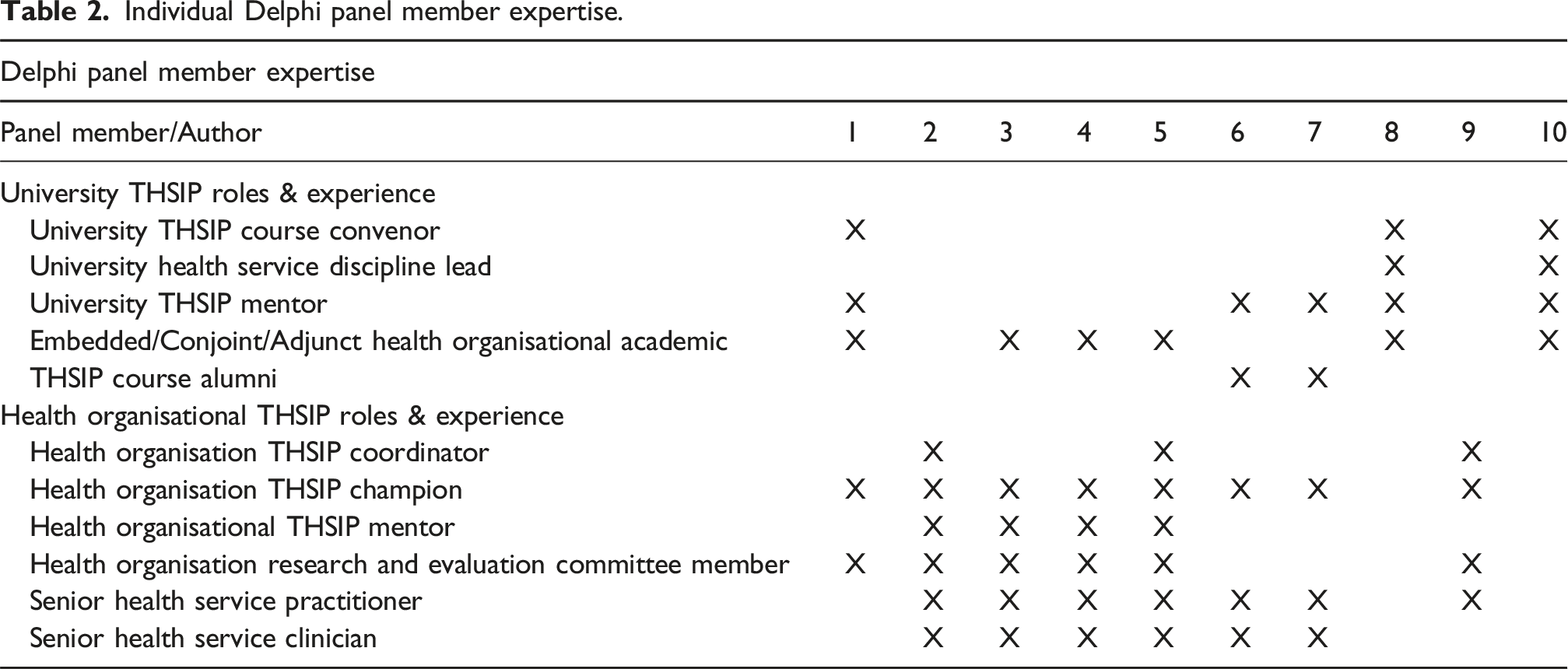
Individual Delphi panel member expertise.
Combined panel member expertise and experience.
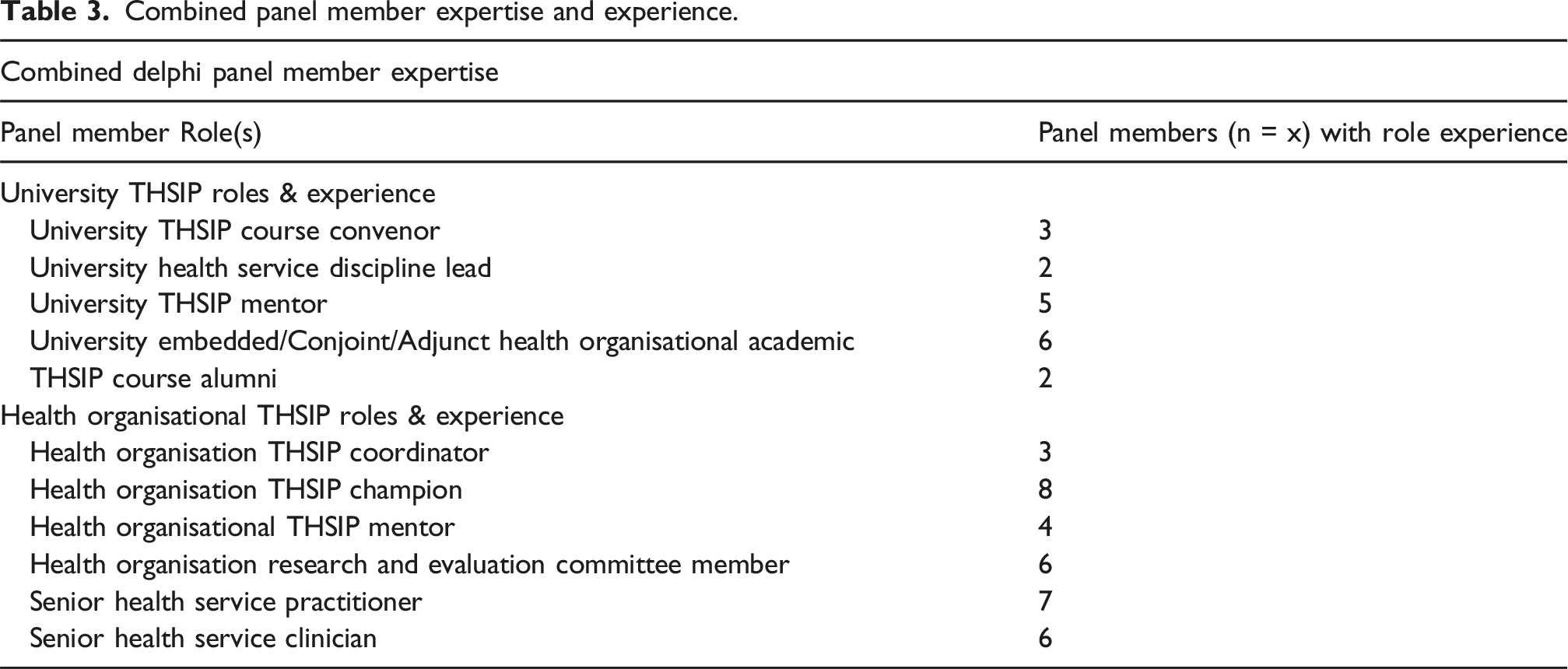
The combined roles and experience of panel members for each of the categories is reflected in Table 3.
In phase 1, panel members were invited to complete an electronic survey to identify the essential elements for the THSIP model. The survey contained four categories: (1) translational program governance, (2) academic infrastructure and support, (3) Industry infrastructure and support, and (4) implementation and retention. Each category contained between 5 and 8 related elements which had been adopted in the program’s co-delivery. An ‘other’ option was included in each category to capture elements which had not been reflected in the 5-8 elements. Panel members were invited to identify the 3 most significant elements within each of the four categories for the THSIP. The elements which recorded the highest overall results, and which were essential to the program’s delivery formed the THSIP model. Those 12 elements were then re-categorised under the three areas: program management, skills development, and implementation as shown in Figure 1. THSIP elements.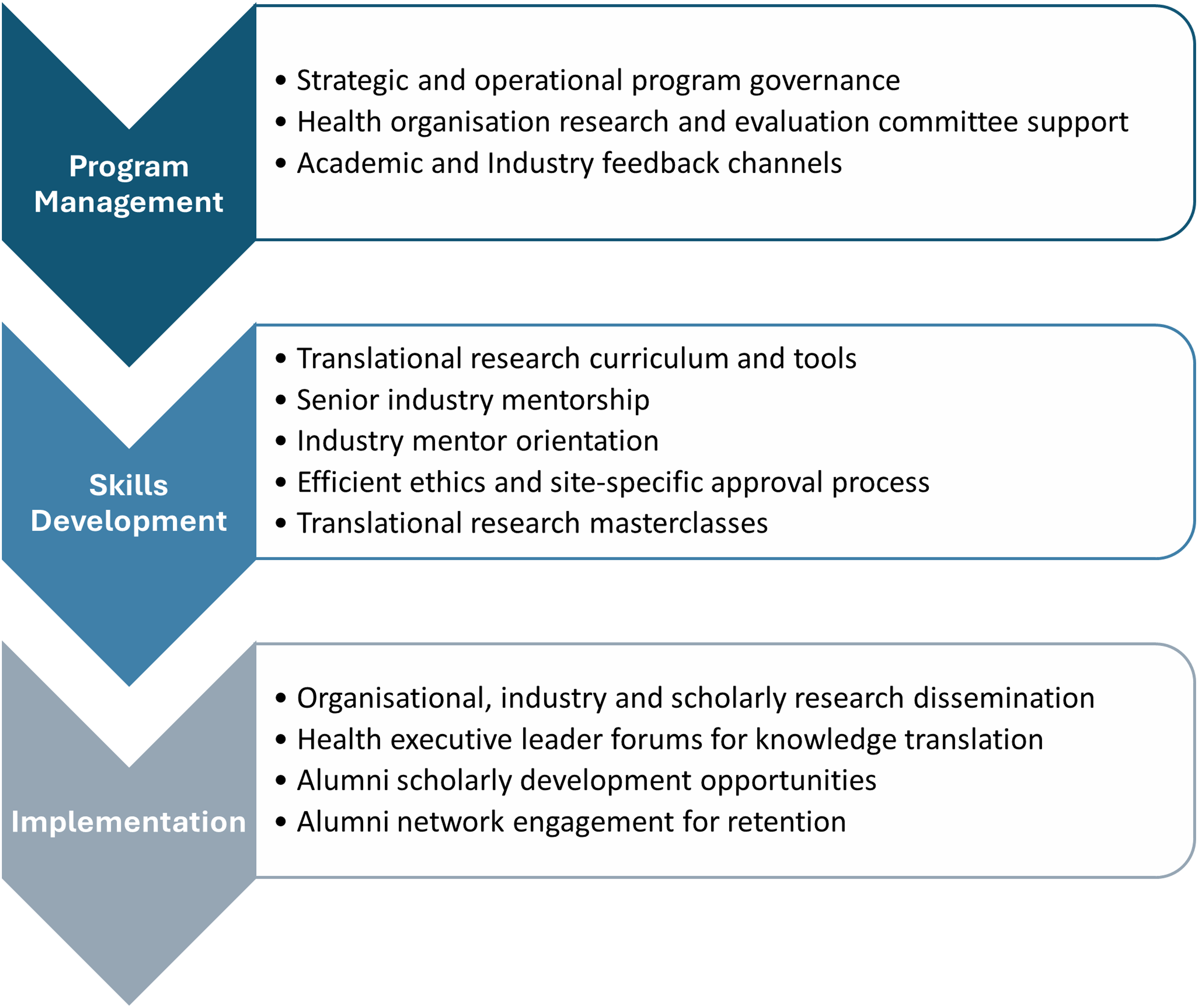
In the second phase of the modified Delphi process, each panel member was invited to construct 1 or more of the essential elements by developing a short explanation of its significance and specifying practical advice regarding its implementation. This development was informed from both the formal knowledge and experiential expertise of members. In phase 3, the written elements were collated into a single document which was forwarded to members for their review, amendments and feedback. All panel members reviewed the item and provided feedback and amendments. This contributed to a final consensus. All feedback and amendments were incorporated into the final revision of the THSIP model and its 12 elements. The final phase invited panel members to complete a final review of the model and the explanation of its individual elements.
Translational health service improvement program model
The 12 elements of the THSIP model are arranged into three key areas including: 1. Program management, 2. Skills development and 3. Implementation. Combined, the elements can enable immediate service improvement through organisational evidence uptake structures and broader systemic improvements through evidence dissemination.
Program management elements
Element 1: Establish a strategic and operational program governance structure between the university and the health organisation
Strategic and operational governance systems enable the integration of university research training in a health organisation’s service environment.. Strategic governance between the health organisation and the university ensures that the translational research program is meeting the strategic goals of both organisations. Correspondingly, operational governance is necessary for its co-delivery. Together, this provides clarity for both organisations about their roles and responsibilities for program management, skills development, and research implementation. This clarity helps to foster effective working relationships between departments, units, and teams in both organisations for those activities.
Strategic governance can be managed through quarterly meetings between the health organisation’s executive staff and the university’s professorial staff. Key review items at this level include: (1) partnership arrangements, (2) program alignment to strategic organisational goals, (3) resourcing, and (4) health organisational support for evidence uptake.
Operational governance may occur between university course convenors and several health organisational teams including: the Chief Executive’s Office, Education and Organisational Development Service, Research Ethics Office, Research and Evaluation Committee(s) and industry mentors. Meetings are to occur as required to coordinate the program against academic calendar timelines and to support the health organisation’s schedule for evidence uptake. Regular and effective communication between operational and strategic structures is essential.
Element 2: Integrate student translational projects into a health organisation research and evaluation committee for industry learning, student support, and organisational oversight
Health organisational research and evaluation committees (REC) which report to broader steering committees are helpful forums with which to connect students and staff. The REC supports students to develop research projects aligned to the health organisation’s strategic and operational goals, ensuring their research remains anchored to those needs throughout the project’s completion. The Committee’s engagement with the students and their projects helps to convey the value to students and serves as a key motivating factor driving research accountability and completion.
Holding the Committee meeting monthly offers a useful cadence to report student progress. It allows for a sufficient period with which to progress the project against key milestones, whilst also a timely check should there be any challenges. University representation on the REC enables updates on student progress to industry representatives. Then on a quarterly basis students present their research updates, on topics such as: scoping review results, methods, results, and translational recommendations. This provides opportunities for health organisational staff to learn from the study’s findings, provide feedback about how to keep the project anchored to the organisation’s needs, and support the student with any operational impacts. Minutes and outcomes from the research meeting are passed to the broader steering committee for review and action.
Element 3: Create academic and industry communication channels to feedback information for translational program improvement
Continuous academic and industry communication is required for whole of program evaluation and improvement. Regular review points are necessary. Health industry communication channels are required to advise of research training amendments against any complex changes in policy and practice in the health service environment(s). They also function to enhance the systems, processes, and supports needed for research evidence uptake in the organisation. Correspondingly, academic communication channels are required to review the translational research curriculum, its tools, and training supports against student and industry feedback. Together, they serve to enhance the applied research training and evidence uptake processes for service improvements in the health organisation. It is important to ensure the focus for any change decisions are made with quintuple aim outcomes in mind.
Industry feedback is obtained through student and industry mentor meetings, health organisation REC meetings, and senior executive leaders who support the research uptake processes. Academic feedback occurs through regular course convenor check-ins with students and industry mentors about areas working well and areas requiring improvement. Other sources include overall student progress and assessment results, student experience surveys, course engagement metrics and supervision observations. Together, these channels report through to the strategic and operational program governance structures. They cater for real-time improvement to the program’s delivery, against a complex changing health environment.
Skills development elements
Element 4: Scaffold a translational health research curriculum, inclusive of tools to align student projects towards the health organisations strategic and operational goals
Scaffolding is about creating a structured curriculum so that key THSIP stakeholders are in alignment with respect to the research objectives and outcomes. Operating in different contexts, health organisational and university stakeholders must collaborate effectively to support students in their research journey. Their collaboration must address not only the health organisation’s strategic and operational goals for improving health services, but also the university’s curriculum, learning outcomes, and governance processes. If the THSIP curriculum is well-scaffolded, it can enhance the knowledge translation skills of students, and all stakeholders involved in health services improvement.
Scaffolding, which needs to be initiated about 4 months before the study period, is led by the university’s course convenors. Initially, the convenors understand the health organisation’s goals and proposed research objectives. They then align these with the university’s strategic themes and curriculum. This could lead to updating the research course learning outcomes with the university committee’s approval. Finally, the convenor translates the agreed research objectives into curriculum topics like research scoping for knowledge translation and formulates assessments to test students on these topics. Throughout the study period the convenor also collaborates with academic and industry mentors who guide the students with the assessments.
Element 5: Identify senior industry mentor(s) in the health service who can provide contextual guidance about the project, its feasibility, and its implementation
Senior industry mentors understand health service governance structures, work structure, and professional roles, which are context attributes key for successful knowledge translation Engaging senior industry mentors is vital for knowledge translation after project completion as they can influence the implementation and sustainability of the research project. As senior leaders in the student’s field, they have specialised experience to provide tailored mentorship relevant to the research topic. Mentors can relate at a job level to the student which can increase the student’s confidence navigating the service environment for improvement.
Each mentor requires relevant field experience and be in a senior leadership role in the organisation, where they can facilitate engagement with organisational stakeholders. Mentors assist students in engaging and liaising with other senior and key stakeholders within the organisation. This needs to occur early in the research planning phase of project timeline. It enables students to build rapport with the mentor, and their organisational networks for ongoing contextual guidance and advice regarding the project. It can also increase service buy-in, which is an important factor for translating any service improvements surfacing from the research and ensuring their sustainability.
Element 6: Develop an industry mentor orientation session which introduces the program, candidate assessments, and industry support expectations
Alignment of expectations of all parties is a prerequisite for successful translational projects. To address a disintegration between knowledge producers and users, an interactive relationship between the university and health organisations is required. The academic and health organisations need to orientate each other to the translational research program. The industry mentor role and expectations need to be clarified to allow an understanding of both the program structure and how industry staff and academics collaborate to support students. When the program parameters are not clearly defined the potential scope of projects may be beyond what is feasible for the student, who generally also has significant other commitments including full-time employment. Mentors need to understand the nature of the program to ensure that they support the academic objectives and assist to focus on the project rather than detract from it.
Two online orientation sessions with industry mentors working in the health system and the academic institution are scheduled at mutually convenient times, considering that the health practitioners’ primary role is generally providing patient care. Course convenors provide mentors with an overview of: (1) the learning outcomes, (2) program structure, (3) assessments, (4) data collection requirements and the (5) roles of the industry and academic mentors. Opportunities for experienced industry mentors to share their experience and insights of working with students should be facilitated.
Element 7: Develop supportive ethical research training and application review structure
A research ethics review process is required to assess the project against ethical guidelines and policies. Alternatively, site governance review is necessary to ensure that the health service has the resources and expertise with which to participate. Efficient review times by the Ethics Committee are paramount for students undertaking translational projects as lengthy delays can impact available time to collect and analyse data and disseminate findings against academic calendars. A secondary benefit of ethical and site-specific review is the development of a detailed step-by-step roadmap for the study’s completion including any contingency processes for foreseeable risks. This detail removes uncertainty for students and provides a clear plan for study completion.
To aid an efficient review process by health organisation Human Research Ethics Committees, projects are developed as low to minimal risk, respond directly to ethical guidelines such as the 2023 National Statement on Ethical Conduct in Human Research, and comply with formatting requests from the health organisation’s research ethics office. Course convenors could collaborate with the ethics office to stagger student ethics application submission dates. This ensures the review committee is not overloaded and can review submissions in an efficient manner.
Element 8: Champion translational research masterclasses connecting students with experienced change management and research implementation practitioners
Translational research education is a key component to support the knowledge and skills of students in both change management and in implementing research findings into practice.
Success in the implementation of translational research in healthcare settings is variable This is partly influenced by the complexity of the healthcare environment, that is continually changing and adapting. Understanding organisational change and the mechanisms that influence successful implementation including human factors and organisational factors, assists researchers to consider how research findings can be applied in complex healthcare settings.
Research students require access to translational research masterclasses that include experts in change management and in the application of research into practice. This would include theory and practical examples of change management and research implementation, preferably in a similar setting to where the translation research will be applied. The masterclasses could be face to face or virtual session that allow time for group discussion of issues, and application of learning to specific research areas. Translational research masterclasses can be implemented either prior to students defining a research area, or after the definition of a research question. The benefits of education prior include an increased understanding the process of research, and change management required to support the implementation of the research, which can facilitate the development of the research question.
Implementation elements
Element 9: Encourage students to disseminate their research at appropriate organisational, industry, and scholarly forums
Encouraging students to disseminate their translational research findings supports their abilities and opportunities to continue to engage in research. Dissemination of student research at organisational, industry and scholarly forums enhances the awareness of the research findings and provides opportunity for innovation to be adopted and embedded into clinical (or routine) practice, particularly at national and international levels. Furthermore, dissemination allows the student to network with health professionals and academics for further analysis of their findings. Students also receive feedback to support embedding new knowledge. Dissemination opportunities support the development of industry relationships that support the student’s skill development in the research and academic space. Dissemination supports students to contribute to policy and practice at broader systemic levels.
Dissemination of findings following completion of the translational research occurs via three key formats - posters, presentation, and papers. Presentations and posters can be disseminated at (but not limited to) structured professional forums, industry research advisory bodies, case reviews or scholarly forums such as professional conferences. Publication is also a key way for findings to be disseminated more broadly. Academic or industry mentors should work with the student to aid the project’s successful dissemination at national and international levels.
Element 10: Provide symposia for students to present their findings to the health organisation’s senior executives and decision makers
Facilitating the student’s ability to present through symposia to senior executives and decision makers lifts the status of the project for the student. Knowing from the beginning of the program that this is an expectation and outcome of their project can further validate their efforts and provides an audience for them to show case before decision makers and influencers. It creates an environment for real change, not just an academic project. Research project’s designed and conducted by staff captures insight into real questions, resulting in evidence that can inform change, and buy-in which assists with sustainability.
The key to success is based on two simple steps: 1. Ensure time is scheduled in the senior executives’ diaries, 2. Create a template identifying key content that needs to be presented. Creating a template will support the student in deciphering the main messages from their project for this target audience. This needs to be included as part of the expectations and outcomes of the project conveyed at the beginning of the program. Identifying an executive sponsor specific to the project will also provide the student with another avenue where ideas are presented and discussed. A secondary benefit is that formalising this relationship creates accountability of the executive sponsor.
Element 11: Identify scholarly career development opportunities post completion of the program to enable alumni skill development
Identifying scholarly career development opportunities for alumni is important to cement translational research skills and foster their extension in the workplace. This can equip health professionals with capabilities to: develop evidence informed solutions to complex problems, effectively communicate in the workplace, and train, assess and mentor junior colleagues. These capabilities can aid the career advancement of health staff within their organisation. However, it also opens possibilities for staff to pursue a higher degree in research including a Doctor of Philosophy or a Master of Philosophy.
Course convenors can support this capability development in several ways including: (1) encouraging alumni to deliver a guest lecture about their translational research project, (2) inviting alumni to collaborate on more methodological complex research, (3) encouraging alumni to become academic or industry mentors for future student projects in the program, (4) creating academic employment opportunities for alumni to assess future student assignments, and (5) supporting alumni to write a research proposal for entry into a doctoral program and find appropriate supervision.
Early in the program, convenors need to draw attention to future scholarly opportunities. This action enables students to have adequate time to think about the career development possibilities post completion.
Element 12: Develop an organisational alumni network to foster staff engagement and retention, and cultivate a community of current and former staff
The alumni networks can help the organisation build a community with current and former staff. It can serve a similar function in a professional environment, allowing staff to stay engaged with the organisation and interact with other former staff. They all have something in common regardless of how long they have worked for the organisation. With the right program, the recruitment teams can engage, nurture and convert past staff that might be interested in returning to the organisation. It paves the way for talent acquisition and talent management to re-hire and re-engage quality staff who are already familiar with the organisation.
Implementation includes: (1) Defining the goals and objectives of the alumni network, (2) Creating a forum where current and former staff can stay connected with the organisation, (3) make signing up for the alumni network simple, (4) schedule events and activities to foster a sense of community, (5) Consistently communicate to ensure everyone is receiving the most up-to-date organisational information, effectively keeping the lines of communication open with the organisational alumni.
Discussion
The THSIP model offers practical guidance about how to foster interdisciplinary collaboration between health staff and academics for translational health service improvement research. This extends the existing knowledge base (Bowes et al., 2023; Myers et al., 2020) by challenging the traditional QI curriculum for medical, clinical, and health degrees through a translational research pathway. This pathway offers students enhanced skill development, allowing for them to make not only immediate service improvements in their health organisation, but also contribute to broader systemic improvements at the national and international levels through broader research dissemination (Eljiz et al., 2023).
The THSIP extends existing research by offering methodological insight into the infrastructure that can support postgraduate students with applied research. Together the program management, skills development, and implementation components address some of the challenges students face including knowledge acquisition for translation, brokering relationship and dynamics, scoping industry aligned projects, and navigating course timeframes.
Together, the program management elements provide the academic and industry governance infrastructure to scope industry aligned projects within academic timeframes. They also enable feedback mechanisms for ongoing program improvement. On the other hand, the translational research curriculum, tools, and masterclasses help students to navigate the research journey. Finally, guidance offered from both industry and academic mentors enable students to safely navigate the cultures and dynamics of academia and the health organisation.
Translational research training by drawing on efficient ethics and site-specific approval processes, also extends student awareness of the ethical principles and requirements of involving human participants in research. The values of justice, beneficence, non-maleficence, respect and research merit (National Health and Medical Research Council and Australian Research Council and Universities Australia, 2023) are not only needed in research but are also fundamental to the actual delivery of health services with consumers, patients and carers (Varkey, 2021). Practice applying these values in a formally supervised low risk research setting can foster greater student awareness and understanding of them. This can enhance student confidence in their capacity to also apply them to their clinical and non-clinical health practice.
Finally, the THSIP model demonstrates how health staff and academics can collaborate to provide supportive research education and training at the service delivery site. Engagement between health professionals and academics is required across all three areas of the THSIP to make the training effective. This necessitates the need to build trustful, interdisciplinary, boundary spanning relationships and to be prepared to challenge the traditional siloed ways of working in professions, disciplines, health organisations, and universities. This paper’s methodology and its THSIP model demonstrate how this collaboration can be possible.
Further evaluation of the THSIP model against the quintuple aim goals is necessary however to ensure that it is not only fostering exceptional education outcomes but also enabling evidence-informed service and population health improvements for the local community. The THSIP model was developed in an Australian metropolitan context. Therefore, further research is also needed to test the model’s feasibility in rural and remote areas, and in other country contexts. This will lead to further understanding of its applicability to different higher education contexts and healthcare systems.
The modified Delphi design used in this project adopted a transparent approach and allowed for the panel to see the opinions and feedback from each member in phases 2-4. A strength of this process allowed members, who are directly responsible for the THSIPs implementation, to collaboratively crystalise and refine the model for its ongoing application. This provides explicit clarity about the program’s elements and the roles and responsibilities of each partner in the industry-university collaboration. It also offers a model which has also been practically tested for its implementation feasibility. A key limitation of the modified Delphi approach, however, is that the results are biased to the views of members directly responsible for the program’s strategic and operational management. A second limitation of a transparent Delphi panel process is that the results from rounds 2-4 may have been influenced by underlying social dynamics including social preferences for group cohesion and agreement (Barrett and Heale, 2020). These two limitations point to a need for the independent evaluation of the THSIP model and this forms the next phase of the project. This can be achieved through an evaluative design aligned to the third THSIP element where academic and industry feedback can be used for independent review of the model, and its ongoing refinement.
Conclusion
There is an opportunity to reconstruct QI training through a translational health service improvement pathway using the THSIP model. This requires close interdisciplinary collaboration between health staff and academics to create the governance, training, infrastructure, and support necessary for student skill attainment, and service and systemic improvements. Reimagining a research pathway can equip students to make longer-term contributions to their service and profession for enhanced, safe, high-quality care delivery. However, further research is required to evaluate the THSIP’s contribution to value-based healthcare delivery. Additional research is also necessary to understand its transferability across different health systems and contexts.
Footnotes
Ethical considerations
Ethics approval was not required as this paper reports the conceptual development of a translational health service improvement program model, informed from existing evidence and from each author’s experiential knowledge regarding the model’s implementation.
Funding
The authors received no financial support for the research and authorship of this article. The article has been published Open Access under the Open Access Agreements Negotiated by CAUL.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.