
Abstract
A persistent problem in trade unions is the discrepancy/tension that exists between their progressive national equality-seeking agenda and the translation of equality principles into workplace activism and their application to members’ everyday working lives. Building on the notion of ‘feminising’ the union agenda, this article explores professional unions’ efforts towards ‘racialising’ the agenda, which is a neglected equality focus in extant literature. The study is located within nursing and midwifery in NHS workplaces where the existence of racism has long been recognised by all employment relations actors. It investigates how the national union anti-racism project is implemented by workplace union representatives. While it reveals recognition of the existence of workplace racism among union representatives, a degree of denial and discomfort also exists. This, combined with the absence of the empowering union strategies that might be expected, hinders the delivery of a racially inclusive union agenda on the front lines of healthcare.
Introduction
That unions need to ‘feminise’ in order to tackle the specific concerns of women workers related to gendered hierarchies and cultures, grading/pay structures and the organisation of work, has long been the subject of debate. Unions have made huge progress even if they are still open to criticism on this front (Cunnison and Stageman, 1995; Guillaume, 2022; Kirton, 2015; Munro, 2001). In a period when the Black Lives Matter movement has reinvigorated the public and policy conversation about workplace racism globally, this article extends the critical interrogation of the unions by exploring how far they have come in ‘racialising’ the agenda – developing an agenda that is responsive to race and racism. In so doing, it responds to an important and timely call for employment relations researchers to centre the narratives and voices of black and minority ethnic workers in order to arrive at richer understandings of worker interests (Lee and Tapia, 2021). When it comes to trade unions, it is important to avoid the assumption that they are necessarily inclusive and equal organisations and to view them as racialised structures (Lee and Tapia, 2021). Most importantly, while in the UK there are signs that the overall national union agenda is making progress on incorporating issues of race and racism (Kirton, 2019), it is less clear how this inclusive national agenda filters through to workplaces – to the front lines – where most of the member-facing union activity occurs.
We explore these issues through a study of the UK National Health Service (NHS), and nursing and midwifery specifically. This is an interesting context in which to study unions’ approaches to race and racism for three reasons. First, the NHS exhibits a markedly racialised hierarchy. It has depended on black and minority ethnic (BME) 1 and migrant labour since its inception in 1948 and today it is the largest employer of BME staff in the UK, with the overall number and proportion of BME staff across NHS trusts 2 increasing (WRES, 2018). While 26.5% of nurses and 13.7% of midwives are of BME background (NMC, 2019), BME nurses are over-represented at the lowest grade for qualified staff and under-represented across all higher pay bands, while only 3.4% of directors of nursing are from a BME background (WRES, 2018). 3 Thus, the ‘snowy white peaks’ metaphor coined by an influential report, which highlighted BME under-representation in NHS governance and leadership, has proved as enduring as it has powerful (Kline, 2014).
Second, the NHS has then struggled to become the inclusive environment it aspires to be. Despite comprehensive equality and diversity policies, very little progress has been made in the last 20 years on redressing the problem of race inequalities in the NHS generally, and nursing and midwifery specifically (see regular pieces in Nursing Standard and by The King’s Fund). 4 Research continues to reveal high levels of workplace racism that seems somewhat impervious to the plethora of initiatives (Aggergaard Larsen et al., 2005; Alexis et al., 2007; Deery et al., 2011; Likupe and Archibong, 2013). BME staff experience direct and indirect racism from multiple sources including managers, colleagues, patients and their families (Bernardotti et al., 2007; Deery et al., 2011). Further, racism is implicated in the greater representation of BME staff in formal disciplinary processes compared with white staff (WRES, 2018) and in the higher number of referrals of BME nurses and midwives for malpractice to the Nursing and Midwifery Council 5 (NMC, 2019).
Third, the NHS is a highly unionised environment. Hence, the unions are critical stakeholders in the employment relationship generally and potentially critical equality actors (Seifert and Wang, 2018). The disproportionate impact of the Covid-19 pandemic on BME healthcare workers has shone a spotlight on race and racism in the healthcare sector (see NHS Race and Health Observatory’s rapid review of evidence: Kapadia et al., 2022). The many media images of BME healthcare workers who lost their lives to Covid-19 are haunting and weigh heavily on the unions, therefore there is much at stake as regards their legitimacy as the voice of BME workers and their capacity to respond effectively as the main organisations representing the multiracial healthcare staff.
Against this context, we explore the extent to which the union agenda on the front lines has incorporated race/racism using findings from a case study of the main UK unions (which double as professional organisations) representing the female-dominated nursing and midwifery professions, RCN and RCM (the Royal College of Nursing and the Royal College of Midwives). In both unions, membership continues to grow, suggesting that they are valued sources of voice and support for staff, but there is little known about how the race equality agenda has been taken up by them, notably at the workplace level. Understanding the dynamics of workplace unionism can help to advance knowledge about the progress of the race equality project within the highly racially charged context of NHS healthcare.
The overarching research question the article addresses is how far have the unions RCN and RCM moved towards addressing race and racism on the front lines of healthcare? Specifically, what level of understanding of racism exists among nurse/midwife workplace representatives and to what extent do workplace representatives provide racially inclusive representation? The article next proceeds to discuss unions, race and racism including developing the theoretical framework that we term ‘racialising the union agenda’. The research methods section then describes the study and provides an outline of RCN and RCM. The findings section illuminates the challenges facing the two unions as regards accomplishing their national goal to do justice to BME members’ interests in the workplace.
Unions, race and racism
To locate our study in a wider context, we begin the literature review by briefly considering the UK unions’ overall historical record on confronting race and tackling racism. We use ‘race’ analytically to refer to racial/ethnic identities/groups, while ‘racism’ is a social system of power, regulation and control that oppresses racial minorities (Solomos, 2003). Our premise is that unions need to recognise the existence of both race (and what it means for BME workers’ lived experiences) and racism (and how it structures BME people’s lives). Yet it is clear from extant research that as ideologically class-based organisations operating within a hostile capitalistic context, unions have struggled to acknowledge and understand let alone champion other social cleavages beyond class, including gender but particularly race (Cunnison and Stageman, 1995; Munro, 2001; Pearson et al., 2010; Virdee, 2000). Thus, any discussion about the necessity for unions to develop an agenda that adequately addresses race and racism extends beyond any specific setting.
Unions’ ambivalent attitudes towards race began with the arrival of post-war migrants in the 1950s/60s from the Indian sub-continent and Caribbean; that ambivalence existed despite relatively higher rates of union joining and membership among those migrant workers (Phizacklea and Miles, 1992). Recruited to work in areas such as transport and healthcare, BME migrants engendered widespread hostility from grassroots to the highest levels of the union movement fuelled by colonial racist stereotypes and amid concern about protecting the jobs of white British workers supposedly put at risk by the influx of cheaper (im)migrant labour (Martinez-Lucio and Perrett, 2009; Wrench, 2000). Hence, the action taken by unions to defend the economic interests of their members developed in protectionist, racially exclusive ways that were entangled with racism and which proved difficult to shake off in the decades that followed (Phizacklea and Miles, 1992; Virdee, 2000). In fact, Phizacklea and Miles (1992: 44) go so far as to claim that the union movement is implicated ‘in the process of confining a large proportion of Asian and Caribbean labour to the low-paid, low-skill section of the economy in much the same way that women have been so confined’.
Phizacklea and Miles (1992) offer a rare and detailed historical account of the British trade unions and racism, which uncovers a complex picture of workplace-level neglect of BME workers’ interests and collusion with employers in discriminatory policies/actions/behaviour, alongside declared principled opposition to racism and fascism at national level from the 1970s onwards. Moving forward, Munro’s (2001) study of unionised hospital ancillary workers identifies very little awareness about race and racism among shop stewards and considerable reluctance to discuss the issues. Even into the 2000s, Bernardotti et al. (2007) find that UK trade unionists in the healthcare sector typically regarded tackling racism as concerned with challenging the racist ideology of far-right political parties at a campaign level rather than dealing with everyday racist incidents at the workplace. Representatives saw the latter as irrational individual acts/experiences rather than symptomatic of a systemic problem requiring a coordinated and sustained union response. Meanwhile, recent evidence finds that, in general, union representatives are now viewed by many members as an important source of support in helping BME workers to ‘speak out’ and challenge racism at work as well as cope with it (Ashe and Nazroo, 2016), which suggests that some change in a positive direction has occurred on the ground and not just in policy and rhetoric.
Theoretical framework: Racialising the union agenda
Debates around unions and race have not to date specifically addressed the question of ‘racialising the agenda’, therefore we begin by referring to the idea of ‘feminising the union agenda’, which has been explicit or implied in much of the research on women and trade unions over the last three decades. Cunnison and Stageman (1995) are among many scholars who argue that gender has not been recognised as part of the agenda and that women’s voices have not been heard. They called for a feminising of the union agenda, which they define thus:
Women and men share common interests stemming from common needs for money, security of employment and tolerable conditions of work. But women also have distinctive needs and priorities. Feminizing the trade union agenda means extending it to include these needs and priorities (1995: 220).
Cunnison and Stageman (1995: 131) proceeded to identify four sets of feminisation policies that unions had adopted to enhance women’s representation, voice, influence and power: (i) policies of attraction (attempt to bring new members into the union by cultivating a woman-friendly image); (ii) policies of encouragement (putting women’s issues on the policy agenda, creating women’s structures); (iii) educational policies (to increase women’s knowledge, skills and confidence to participate); (iv) policies of empowerment (e.g. proportionality, reserved seats, self-organisation and networking to assure women positions of influence and power).
Based on the same logic as feminising the union agenda, the project to racialise the agenda would follow a similar path involving going beyond publicly championing anti-racism and race equality to develop policies and practices designed to confront the culture and practices that have led unions to neglect race and racism in their actual work. On the policy front, the unions began to respond to these questions in a more progressive and strategic manner from the 1970s onwards after the Race Relations Act in 1976. The Trades Union Congress (TUC) published the first Black Workers’ Charter in 1981, and in 1989 its first negotiators’ checklist for black women (Cunnison and Stageman, 1995). Many unions created national anti-racist policies providing race awareness training materials and BME workers’ conferences, groups and committees (Cunnison and Stageman, 1995; Wrench, 2000). Despite the plethora of initiatives, Kirton and Greene (2002) highlight the lesser progress on tackling racism compared with gender inequalities, which they attribute to race being politically less unifying, which often places it on the margins of the workplace agenda.
Various studies have revealed a discrepancy between the publicly declared national race equality agenda and what happens in workplaces (Cunnison and Stageman, 1995; McBride, 2001; Munro, 2001). Local bargaining and representation in particular remain centred on issues that affect most workers (which essentially means white) and often without accommodation of specificities affecting a minority or minorities (Martinez-Lucio and Perrett, 2009; Munro, 2001). Thus, while, just as with gender, national race equality structures (e.g. committees, conferences, self-organised groups) have been seen as critical empowering resources, their anti-racist work does not necessarily permeate the everyday practices of local unions who are the ones actually representing workers and their concerns (Kirton and Greene, 2002; Martinez-Lucio and Perrett, 2009; McBride, 2001). Munro (2001), in her work in hospital settings for example, detected little awareness of race discrimination issues among shop stewards and a continuing neglect of the workplace interests of BME workers.
Jefferys and Ouali’s (2007) study is among the few that focus singularly on how workplace unions address race and racism, and they identify four main types of response: protectionist (protecting the power of the dominant racial group); denial (of the presence of racism); assimilationist (belief that BME workers should subscribe to the existing union agenda); and equal opportunities (implementation of policies and practices to promote race equality). In their study, denial responses were the most prevalent among workplace unions, followed by assimilation. While protectionism is arguably the most pernicious response, the most popular responses of denial and assimilation also impede racialising of the agenda: denial conceals the problem, while assimilation persuades BME people to accept the priorities of the dominant group. Jefferys and Ouali (2007) conclude that union representatives mediate workplace racism through contradictory, yet simultaneous responses: exclusionary (where they cover up the presence of racism) and inclusionary (where they welcome BME workers and try to involve them in the union). How these tensions can be resolved is a moot point.
However, there can be no doubt that participation of BME workers is a key element in shaping awareness and understanding of racism and strategies for combating it (Jefferys, 2007; Kirton and Greene, 2002), but it is unlikely to be sufficient considering that the vast majority of union representatives are white. Thus, white representatives are necessarily part of the solution in tandem with unions providing structures and mechanisms for BME voices. Despite the now taken-for-granted national-level commitment to tackling racism, the persistent under-representation of BME people among workplace representatives combined with white representatives’ insufficient understanding and awareness about race and racism, means that all the signs point to workplace unions having only limited capacity to address BME members’ concerns on the ground (Jefferys, 2007; Kirton and Greene, 2002).
Looking specifically at professional unions as studied here, while they may not have the overt class-based identity that has arguably hindered special attention to gender and race in some of the examples above, there is still a tendency within such unions to privilege economic and industrial issues alongside professional to an extent that limits the scope of the agenda in actual workplaces (Kirton, 2015, 2021). Bernardotti et al. (2007), for example, find that nurses’ concept of professionalism led to the excusing of patient racism by reference to patients’ age, frailty or mental health. This ambivalence surrounding how or even whether healthcare unions should tackle this prevalent source of workplace racism highlights a deeper tension between concerns to promote professional workers’ rights as workers and self-concepts of professional ethos centred on almost sacrificial duty to patients. This dilemma for professionals is one that resonates for many unions given that professional unionism now dominates (e.g. Kirton, 2015).
As regards the implications of the above discussion for the political project of racialising the union agenda in nursing and midwifery with the practical goal of challenging workplace racism, theory and practice are complicated by the dual union and professional association role played by the two main unions studied here (RCM and RCN). As suggested earlier, unions and their members may knowingly tolerate forms of racism or perhaps racism from certain sources (e.g. from patients and their families) out of regard for the greater good of their profession and professional values. As professionals, they recognise that they bear some responsibility for the service and its quality and pursue goals beyond their own working conditions. Therefore, arguably the ‘racialising the agenda’ project of professional unions necessarily needs to be built carefully upon the occupational identity of members as well as appeal to employers and the state in order to build unions’ ‘legitimacy power’ as constructive organisations that contribute to the overall goals of this particular domain (Ackers, 2015: 103). This will necessarily involve consideration of service aspects as well as workers’ rights and conditions, thus complicating the project and extending it beyond a conventional ‘them and us’ approach.
Research methods
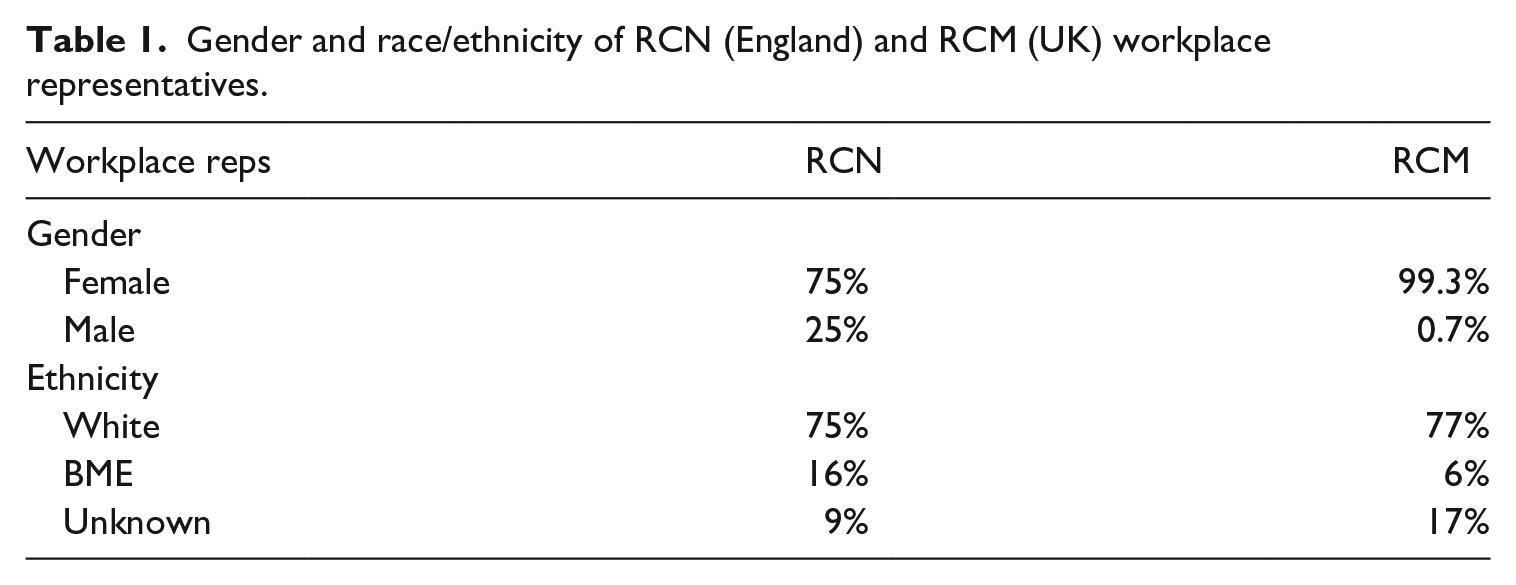
The study is located within the two main nursing and midwifery unions, RCN and RCM. RCN was founded in 1916 as a professional association and registered in 1976 as a union, although it remains non-TUC affiliated. RCN represents around 435,000 nurses, nursing students, midwives and healthcare assistants. RCM was founded in 1881, registered in 1976 as a union and affiliated to the TUC in 2015. It represents around 48,000 midwives, student midwives and maternity support workers. Both unions have national and regional officers supporting the activities of local union branches as well as workplace representatives. Additionally, RCM has a team of organisers. RCN currently has around 1300 workplace representatives (learning representatives, health and safety representatives, stewards) in England, while RCM has around 745 nationally. The majority of representatives are white (Table 1).
Gender and race/ethnicity of RCN (England) and RCM (UK) workplace representatives.
The research was carried out in collaboration with the two unions following initial discussions with senior officers. The collaboration encompassed co-production of the research design, including data collection strategy and fieldwork instruments (interview and focus group guides). The unions also arranged access to key national officers, union education and equality staff as well as to selected senior workplace representatives; from the latter, we snowballed to other representatives to increase the size of the sample. For the focus groups, we had access to union training courses and time dedicated to our discussion.
A total of 110 workplace representatives (split more or less evenly between RCN and RCM; 33% BME and 92% female) participated either in a one-to-one interview (34) or in a focus group (76). The rep interviews/focus groups were utilised to gather ‘on-the-ground’ experiences, which were critical regarding fulfilling the main research objective. Focus groups were a practical means of gathering the views of a larger sample of representatives and they also provided an opportunity to witness representatives discussing issues among themselves, which in particular allowed us to gauge the level of comfort around talking about race in a group setting. In addition, 12 national/regional union officers and four union staff members with portfolios in education, equality and legal participated in interviews. This group of interviewees provided insight into the unions’ national thinking on and approaches to the race equality agenda, as well as garnered broad experiences of dealing with apposite issues within their remits.
Interviews and focus groups used guides containing themes, headline questions and prompts, which afforded a large degree of thematic consistency across the interviews/group discussions, but also some flexibility depending on participants’ union roles. The interviews had broad themes covering work context and conditions of nursing and midwifery; local and national union contexts, structures and activities. We also asked all participants about workplace racism and union approaches to tackling it. Focus group discussions concentrated on the local workplace context and representatives’ on-the-ground experiences. Unsurprisingly, BME interviewees talked for longer about race/racism and spoke very openly about incidents they had personally experienced/witnessed or that BME friends/colleagues had confided. Several confided that they were grateful to have the opportunity to contribute to research incorporating this important but under-researched topic.
Interviews were of 60–90 minutes’ duration and focus group discussions 60–120 minutes; all were digitally recorded and transcribed verbatim before being imported into the qualitative research software NVivo11 for thematic coding. Interviews and focus groups were conducted confidentially; therefore, we have made every effort to ensure participants’ anonymity by using generic role descriptors for example. We show selected bio-demographic details of workplace representatives beside quotations in order to add biographical context to the narratives (gender, race/ethnicity, age), but these details do not expose any individuals. Although the research was carried out in collaboration with the unions, we did not report the names of those who participated and only the researchers had access to sound-files and transcripts.
Research findings
As discussed earlier, the available evidence paints a troubling picture of race/ethnic inequality of treatment, opportunity and outcome in the NHS, which suggests a challenging context in which the unions seek to address the specific concerns of BME nursing and midwifery staff. This findings section first briefly outlines race and racism and the national agenda in RCN and RCM; the focus then shifts to the workplace level looking at racism recognition, awareness and denial among union representatives, and providing racially inclusive representation at the workplace.
Race and racism and the national agenda in RCN and RCM
Similar to other unions, at national level both unions have a broad equality agenda encompassing all the legally protected identity characteristics. The agenda also reflects RCN/RCM’s dual role as unions (concerned with workers’ terms and conditions) and professional bodies (concerned with service delivery):
Equality, inclusion, diversity and human rights provide a foundation for a modern and forward looking profession where nurses, healthcare support workers, and students, regardless of the sector that they work in or their field of practice, can continue to transform their working environments and the care they deliver to patients. (RCN: https://www.rcn.org.uk/professional-development/publications/pub-006212) Equality and Diversity is important for providing high-quality care for women and their families. To be able to provide a truly inclusive service and an NHS which treats all service users with respect, dignity and compassion, the NHS workforce needs to be treated in the same way. (RCM: https://www.rcm.org.uk/supporting/equality-diversity/)
In addition to its overall equality strategy, RCM has recently developed a specific anti-racism strategy to tackle internal race equality and diversity, which it sees as intricately connected to its capacity to deliver a racially inclusive agenda:
First and foremost, we must look at ourselves as an organisation. From the limited data we have available we estimate about 15% of the midwifery and MSW
6
workforce is BAME. The RCM remains an overwhelmingly white organisation and we must tackle that and ensure our organisation becomes more truly representative of our membership (RCM, 2020).
As regards structural support for equalities work, again as per most unions, RCN and RCM both have a staff member responsible for the equalities brief who co-ordinates, supports and initiates national campaigns and other national-level equalities work (e.g. analyses and disseminates relevant research/data). These staff members are acutely aware of the pressing need for both unions to enhance their work on race and racism. Unlike many other UK unions neither union has a national equalities committee nor a nationally led BME network/group, which according to previous research might facilitate involvement of traditionally under-represented groups and enable their voices to be heard (Kirton, 2015; Parker and Douglas, 2010). RCM recently canvassed the views of members about establishing a BME network but found minimal support/demand and therefore did not go ahead. RCN supports a grassroots group ‘Equality 4 Black Nurses’ established in 2020 specifically to help nurses lodge grievances about racially discriminatory treatment. Thus, neither of the unions has the policies of empowerment that would be the strongest hallmark of ‘racialising the agenda’.
However, both unions firmly acknowledge the importance of building the knowledge and skills of officers and representatives vis-a-vis tackling race issues through training and other initiatives. RCN holds an annual equality and inclusion conference for workplace representatives, which we attended on two occasions witnessing the prominence of the theme of race/racism and the passion with which BME participants spoke on the issues. RCN also has a podcast series called ‘Nursing whilst Black’, which features the stories and reflections of members, and it has a ‘Cultural Ambassador Programme’ comprising BME nurse volunteers who are trained to participate in teams that investigate racism in NHS workplaces. RCM’s programme of action includes training for staff and activists on race awareness and ensuring race is considered explicitly in all work programmes and projects, including branch and workplace activity (RCM, 2020). Thus, both unions have adopted policies of attraction, encouragement (vis-a-vis BME members) and educational policies towards ‘racialising the agenda’.
In summary, both unions’ approaches towards racialising the agenda depart somewhat from those of other unions that have depended on structural resources, particularly at national level (e.g. committees, self-organised groups, reserved seats) (Kirton and Greene, 2002). RCN and RCM focus more on attempting to engender representatives’ awareness of racism and to build their competencies to tackle it in the workplace. While arguably the approach is not radical (Kirton and Greene, 2002), the workplace is, as previously stated, where many union services, including representation, are delivered and where activities such as local bargaining and campaigns occur. Therefore, the potential of the RCN/RCM approach is worthy of detailed evaluation.
Workplace racism recognition, awareness and denial among union representatives
We begin this section by discussing representatives’ perspectives on the existential question frequently raised in interviews and focus groups of whether RCN and RCM are the ‘right’ unions for BME staff. BME participants spoke about the image of RCM/RCN as the unions for white, middle-class nurses/midwives, frequently using the phrase ‘twinset and pearls’, with its implied ‘whiteness’ and middle-class connotations. Meanwhile, some white participants thought it was a question of union style, expressing the view that BME nurses/midwives favour the putatively more militant approach of large, general public services union UNISON that also recruits nurses and midwives:
A lot of them [BME nurses] tend to go towards UNISON because somebody is screaming, yelling and banging tables and they get what they want nine times out of ten. I don’t think they’re particularly happy with the RCN because we are a little bit more professional in the way that we work. (Interviewee: RCN steward, female, white)
The ‘othering’ of BME nurses and midwives barely concealed in the notion that they necessarily prefer a militant style that is alien to professional unions is to some extent a culturally essentialist trope that in itself reveals some white representatives’ lack of awareness or denial of race as well as failure to appreciate the shared professional identity that for many transcends racial/ethnic difference extending to BME staff too:
I don’t think it gets you anywhere if you go in shouting. This is what I say with the BME group – they thought that as BME staff we were going to moan, we were going to shout, we were going to demand. We showed them that this is not what we’re about. We’re about equality, we’re about inclusion, we’re asking for fairness, we’re not asking for anything different . . . we’re all nurses . . . (Interviewee: RCN steward, female, BME)
Rather than union style or image being the issue at hand, some BME representatives claimed BME staff wanted to see more done practically to tackle workplace racism. According to some, UNISON (with its highly racially and occupationally diverse membership) had been bolder and more effective than RCN/RCM where ‘whiteness’ was not merely a superficial image, but embedded in the culture of the organisations. Many BME representatives believed the organisational culture was slowing down the anti-racism project. Such participants wanted to see a proactive campaigning and bargaining agenda:
I think that by the mere fact that it was the first time that we posed a motion [on tackling workplace racism] to the TUC in 2016, that says a lot, doesn’t it? . . . We should have been involved a long time beforehand. (Interviewee: RCM steward, female, BME)
Nevertheless, participants reported that BME staff often remained loyal to RCN/RCM because of the dual function as professional bodies – being the ‘voice of the profession’ and not ‘just’ unions. Some BME participants had stepped up as workplace representatives precisely to demonstrate that RCN/RCM were the ‘right’ unions for BME staff.
When discussing race and the workplace union’s approach, similar to earlier research in a healthcare setting (Munro, 2001), we noticed discomfort among many white workplace representatives. This manifested in lowering of voices (almost whispering even though interviews were in private) and hesitation in speaking about the issues. We also heard stories that suggested racialised tension in workplaces (e.g. the claim that BME nurses/midwives stick together in their specific ethnic groups self-segregating from others). However, most white representatives as well as BME of both unions acknowledged the existence of systemic race discrimination in healthcare and recognised the way it produces racialised power hierarchies that are hugely consequential for BME staff and their careers:
We’re dealing with lots of equality issues [for BME staff]. You’ve got people who don’t always get the same opportunities to go on courses and so that makes it very difficult. Some people are pushed forward and promoted very quickly and . . . some people never get acknowledgement. (Interviewee: RCN steward, female, white)
Most representatives also named racism as explaining why BME nurses and midwives are disproportionately represented in disciplinary and capability proceedings. Indeed, many representatives had direct experience from their own union casework:
Somebody was suspended, didn’t need to be suspended for what they had done. She was black. The person who lost the appeal I spoke about, she was black. So, the people who have lost or have been sacked have been black. Nobody has been white. (Focus group member: RCM steward, female, white)
At the same time as strong acknowledgement of racism among many research participants, there was also a contrary tendency towards a degree of denial among some white representatives as identified in other studies (Bernardotti et al., 2007; Jefferys, 2007; Munro, 2001). A focus group discussion illustrated a wider finding where a BME midwife quoted damning statistics from the WRES reports, which attracted supportive nods from other BME participants. However, her claims about endemic workplace racism met the following interjection:
. . . I have an issue with that because I think that although statistics seem to demonstrate that [BME midwives are over-represented in disciplinary cases], I wouldn’t necessarily say that is the case . . . it depends on what your workforce picture looks like. If 100% of that trust’s midwives are black, then 100% of those disciplined will be black. (Focus group member: RCM steward, female, white)
Intentionally or not, these somewhat defensive remarks conjured up a scenario that rarely exists (100% black midwifery workforce) in order to ‘prove’ that structural racism does not exist, which attracted support (via nods, etc.) of some white participants, thus diminishing the claims of BME participants. We can also read denial in the belief expressed by a small number of white representatives in other interviews and focus groups that some white nurse/midwife managers (who comprise the majority of managers) are not racist but rather they fear accusations of racism if they say or do the ‘wrong thing’ around BME staff. Hence, they allegedly escalate minor performance/conduct issues (e.g. punctuality or complaints about manner of speaking to staff/patients) to avoid interpersonal racial conflict. In addition, BME representatives reported that it was not always any easier for the often lone BME manager to stand up against racism for fear of being discredited in their managerial role.
While we did not detect universal denial among workplace representatives in either union, the greatest level was around what might be called ‘everyday racism’ – the kind of discrimination manifested in the form of subtle acts rather than major events (Deitch et al., 2003). The following quotation, where the representative speaks about how African (born and trained) nurses do not really fit in, illustrates how essentialist stereotypes serve to deny racism and again conceal racialised power hierarchies where supposed white behavioural norms are implicitly superior:
We struggled with their English and their understanding of our standards and procedures. I had a long conversation with one of the girls. Although she was a registered nurse in her own country, when she came here, she found it very difficult. She comes from a very sort of dictatorial background and sometimes when she talks to people, she’s a little bit abrupt. I think as a culture we’re quite sensitive to the way people talk to us. So, the way she was delivering something was normal to her, wasn’t normal to us. (Interviewee: RCN steward, female, white)
Thus, in the ‘othering’ narrative above, culture, language and accent, rather than any racism, account for the way some BME workers are perceived. A lack of understanding, even if not denial, of everyday workplace racism is also illustrated in the following quotation where a white representative interprets the absence of BME staff complaints about race discrimination as an achievement for the union:
I have to say I have never ever, since 2015, since I became a representative, had a member come to me yet over a discrimination issue. I think that actually that is a marvellous achievement. (Focus group member: RCM steward, female, white)
In contrast, all the BME participants (and some white) explained absence of complaints as BME staff being reluctant to voice their concerns because they felt like ‘easy targets’ or they lacked confidence that they would be heard. This echoes previous research suggesting that BME staff view the organisational ‘voice climate’ more negatively (Behtoui et al., 2017). The widely spoken about ‘blame culture’ in healthcare workplaces meant that those bringing race complaints would be cast as the ‘problem’ rather than as ‘victims’, which encouraged BME staff to ‘keep their heads down’:
. . . the person being bullied is often very vulnerable, very anxious and very frightened and is already scared of this person, is worried about the repercussions. So, it’s getting the confidence of that person to have the courage to say this was done to me. I can take this forward [as a representative] but obviously you will be asked questions, you might have to make a statement and they often don’t want to do that so that’s where it ends. (RCM representative, female, BME)
Again, this reinforces that silence can indicate resignation to the way things are, rather than satisfaction (Behtoui et al., 2017). In summary, on the one hand, while our research suggests strong acknowledgement of structural racism among RCN and RCM representatives, which offers some promise of greater incorporation of race issues within the workplace agenda insofar as campaigning and bargaining go, on the other hand, a degree of discomfort, denial and lack of understanding of everyday racism poses challenges around developing an agenda to address lived experiences through broader representational processes. As one national officer said:
I would love to see more black reps in London, but what I would love to see more are reps that are actually able to speak to and understand difference. That is the skill that they need . . .
Providing racially inclusive representation
In this context of both recognition and denial and limited awareness of (everyday) workplace racism, to what extent are workplace representatives providing racially inclusive representation? To begin with, there was some acknowledgement, particularly among national officers, that although the small number of BME workplace representatives (Table 1) is unsurprising (broadly reflecting the membership/workforces), it hinders overall levels of understanding of workplace racism and how to tackle BME members’ concerns on the ground (Bernardotti et al., 2007; Kirton and Greene, 2002). BME representatives believed that BME staff valued having a representative ‘who looks like them’ that they could turn to for help, support and understanding:
Mainly the cases I get are disciplinary cases against black nurses, a lot of African nurses . . . some of it is sickness related, but I could see where the sickness was attributable to the stress and the strain they were under . . . they get so down about it and haven’t got anybody really to talk to. Some of them are so happy when they see another black face come to represent them because they think, ‘I’m not on my own, someone understands’. (Interviewee: RCN steward, female, BME)
Yet, BME representatives felt that BME nurses and midwives were discouraged from stepping forward for union roles because they believed they would struggle to get themselves heard in the union or seen by management as legitimate union representatives, a twofold obstacle:
I try to encourage people to become a rep, it’s very difficult. Because they will say you’re alright because you can talk, you’ve got the support. But I say all you’ve got to do is just knock on the door . . . That’s what I’ve done really, I’ve gone to HR with a lot of disciplinary cases, and I say can we just sit and look at this, does this have to be a disciplinary, could we not get the manager and sit and talk and ask what is going on or why this went on? . . . it’s just something as a black person, I’ve got to put my head above the parapet. (Interviewee: RCM steward, female, BME)
While there were hurdles to overcome to recruit more BME representatives, some white representatives (as well as BME) made a point of actively reaching out to BME staff:
I have noticed just recently I’ve had a big increase in BAME nurses coming over from UNISON to the RCN and I think that’s just being out and about and listening to them. (Interviewee: RCN steward, female, white)
In addition, many white participants declared a strong sense of responsibility to stand up against and call out racism, even from patients:
We had a couple of patients that said, ‘I’m not having that black so-and-so . . .’, and I go up to them and say look, this is not private healthcare, I appreciate you have your views but this nurse is trained, knowledgeable and experienced to look after your baby. If you do not wish to have said nurse look after your baby then I suggest you go and seek private healthcare but I’m not allowing you to refuse that nurse to look after your baby . . . that is not acceptable. (Interviewee: RCN steward, female, white)
As well as being alert to individual incidents of racism, some white representatives also sought to bring collective claims to management:
Tomorrow we have a meeting with one of the divisions to go through disciplinaries . . . is it happening to a particular group or a particular ward? . . . So that we can actually parachute somebody in there to try and sort it. (Focus group member: RCM steward, female, white)
Also in this vein, several participants had worked in partnership with local management to co-create leadership development opportunities for BME staff, Black History month events or local BME staff networks. Some participants had also initiated local union campaigns that consciously incorporated workplace racism within broader aims to improve the working environment:
This area is not very diverse in general . . . and we had a problem with staff at [one hospital] and they put in a [collective] grievance, we [RCM] supported them putting in a grievance about their opportunities within [the hospital]. They felt like there wasn’t a lot of development opportunities for BME staff and they felt like people were treating them in a discriminatory way. (Interviewee: RCM steward, female, white)
In summary, while a starting point towards racialising the workplace agenda that some participants had adopted was to seek to increase the active participation of BME members, some workplace representatives were certainly aware that the anti-racism political project also needs to involve everyone – namely, white representatives as well as BME.
Conclusion
The UK union movement undoubtedly has a chequered history as regards its approach to race and racism (Phizacklea and Miles, 1992; Virdee, 2000), but significant efforts to racialise the union agenda have been made, through policies similar to those used towards feminising the agenda, whether it be recruitment strategies for BME workers or encouragement policies via putting BME workers’ issues on the policy agenda and the provision of resources at national level (Kirton and Greene, 2002). Extant research on unions’ efforts to address race and racism tends to focus on these national (race) equality initiatives rather than on the way workplace representatives take them up locally, which only a small number of studies have addressed (e.g. Jefferys, 2007; Jefferys and Ouali, 2007; Munro, 2001; Seifert and Wang, 2018). This article extends existing knowledge about the implementation of the race agenda through a case study of workplace representatives in two feminised professional unions – RCN and RCM – in the healthcare context where a high proportion of staff is BME and where race and racism are on the public policy agenda.
It is notable that RCN and RCM are attempting to incorporate race and racism into the union agenda albeit in the absence of the empowering policies (race or BME member committees, conferences, self-organised groups) that previous literature on feminising has seen as key to successful equality projects (Briskin, 2008; Kirton, 2015; Kirton and Greene, 2002). RCN and RCM national-level strategies can be characterised as declarative with their implementation dependent upon engendering greater awareness of race and racism among key actors on the front lines (i.e. workplace representatives). On the optimistic side, it is important to acknowledge that with race inequalities and racism in the NHS having had a high profile in recent years, unlike findings of research in other contexts or earlier studies (Jefferys, 2007; Munro, 2001), it was apparent from our study that this prominent organisational discourse had permeated the consciousness of the predominantly white nursing and midwifery workplace representatives, particularly those working in the larger cities in England with higher concentrations of BME staff and patients. Nevertheless, that a level of denial of workplace racism exists among RCN and RCM representatives attests to the educational and empowerment challenges of achieving a racialised agenda in practice.
The first research question concerned the level of understanding of race and racism among nurse/midwife workplace representatives. We operationalised this as meaning representatives’ practical and positive engagement with, and responses to, workplace racism as experienced by members; that is, their capacity and willingness to hear BME members and to challenge the status quo. It is important that the situated knowledge that BME representatives bring to the table from their marginalised subject positions meets opportunities to contribute to the union agenda in order to break the racialised silences that seemed to pervade workplace unions. In the professional workplace context, self-evidently, it is not a question of BME nurses and midwives having an entirely different set of interests. Clearly, BME staff share many of the interests of their white colleagues as regards their working conditions and professional concerns, and their powerful shared occupational identity might paradoxically contribute to a reluctance to confront the social and racial divisions that run through the professional group. In light of the evidence of racism and race-related issues (Bernardotti et al., 2007) in the sector, bringing the project of racialising the union agenda to the forefront implies tackling the specific concerns of BME nurses and midwives around barriers to career opportunities, under-representation in more senior grades, over-representation in disciplinary, performance and conduct processes, but also racialised bullying and harassment, which often takes the form of subtle forms of micro-aggressions between colleagues, or with patients, which are very difficult to appreciate and address by (white) union representatives who do not personally experience such daily indignities.
The first research question was linked to the need to deepen understanding among white union representatives who must necessarily take some responsibility for racialising the agenda. Clearly, the conversation needs to be had and embedded in the union education provision. It is often difficult to blame what we cannot or will not name and despite the existence of compelling evidence, some white union representatives are still not convinced of the systemic and institutional nature of race discrimination (cf Jefferys and Ouali, 2007). Several factors contribute to this blind spot: the diversity of the workforce, at least in large cities, creating the impression that there is no race discrimination in the NHS, but also historical racial stratification that creates embedded, and often hidden, hierarchies of power and privilege; the informal and routine nature of micro forms of racism in daily interactions among colleagues, management and patients. Further, out of commitment to the profession, there is often a degree of acquiescence among staff to a bullying culture that invisibilises gender, class and race inequalities, while constituting them (Crenshaw, 1991). Finally, the existence of formal equality and diversity policies at the NHS level and within unions serves to create the impression that the problem is being dealt with institutionally. RCN has approached the issue with a very broad framing around inclusion, which does not quite name the problem for what it is from the perspective of BME nurses (i.e. racism). RCM’s frank acknowledgement that the organisation needs to do more on race and racism is only recent and is yet to translate into concrete actions and tangible outcomes.
The second research question concerned the extent to which workplace representatives provide racially inclusive representation. Most participants, particularly those in racially diverse areas, recognised that more BME workplace representatives are needed for the purposes of expanded interest identification as well as empathetic and knowledgeable individual representation. Yet BME participants saw members’ reluctance to speak out and assert interests as emanating from a palpable fear of repercussions, or of being perceived as a ‘troublemaker’, which does not encourage active union participation. As previous work on the feminisation of the trade union agenda has shown (Cunnison and Stageman, 1995; Munro, 2001), one of the challenges is the establishment of educational policies and empowering spaces where union representatives from minority groups can develop their awareness and knowledge of the problems they face and build their confidence (Greene and Kirton, 2002). Racialising the union agenda on the front lines can only be achieved by the active engagement of workplace representatives empowered to de-individualise experiences and incidents of race discrimination, politicising them and transforming them into collective demands (Chun et al., 2013). Moreover, it is also important for white allies, who will likely always constitute the majority of representatives, not merely ‘to help’ individual victims but ‘to speak up against systems of oppression’ such as race (Briskin, 2008).
Thus, in conclusion, we argue that a national anti-racism agenda will not be sufficient. The Black Lives Matter movement should be instructive for unions insofar as it is emblematic of the hunger of marginalised groups for collective empowerment, meaning that unions, among other institutions, will need to include BME people in the co-creation of a progressive agenda and practices towards a more inclusive future. Future research addressing these issues in different union and workplace contexts would help to push that agenda forward by bringing a neglected debate into the public and intellectual domains.
Footnotes
Acknowledgements
We thank the RCM and RCN for their collaboration and all the nurses and midwives who participated. Finally, thanks to the anonymous reviewers for their constructive and encouraging feedback.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We are grateful to have received a British Academy/Leverhulme small grant to carry out this research.