
Abstract
Background
Adverse effects of COVID-19 vaccination on human menstrual cycle characteristics have been observed, but limited data are available on the relationship between COVID-19 vaccination status and birth rates.
Objectives
Therefore, we used nationwide data from the Czech Republic to examine rates of successful conceptions (SCs), that is, conceptions leading to live births 9 months later, for women who were either vaccinated or unvaccinated against COVID-19 before SC.
Methods
Summary monthly COVID-19 vaccination and birth data for women in the Czech Republic aged 18–39 years were retrieved for the period from January 2021 to December 2023. The numbers of SCs per month per 1000 women were calculated for preconception-vaccinated or unvaccinated women, respectively, as well as the number of SCs per month per 1000 women for all women aged 18–39 years.
Results
During the study period, there were approximately 1,300,000 women aged 18–39 years in the Czech Republic, and the proportion of COVID-19-vaccinated women increased from January 2021 until reaching a steady state of around 70% by the end of 2021. At least from June 2021, SCs per 1000 women were considerably lower for women who were vaccinated, compared to those that were unvaccinated, before SC. Furthermore, SC rates for the vaccinated group were much lower than expected based on their proportion of the total population.
Conclusions
In the Czech Republic, SC rates were substantially lower for women vaccinated against COVID-19 before SC than for those who were not vaccinated. These hypothesis-generating and preliminary results call for further studies of the potential influence of COVID-19 vaccination on human fecundability and fertility.
Introduction
Decreased birth rates have been reported in the Czech Republic and many other countries following the COVID-19 pandemic.1–3 Although studies have indicated that COVID-19 vaccination has no appreciable effect on human fertility and that COVID-19 vaccines are safe during pregnancy,4,5 adverse effects of COVID-19 vaccines on menstrual characteristics are well documented, suggesting that COVID-19 vaccination may influence fecundability, that is, the probability of achieving successful conception (SC) within a single menstrual cycle.6,7 The potential influence of COVID-19 vaccines on reproductive health was not assessed in randomized preauthorization trials. In addition, investigation of the potential influence of individual COVID-19 vaccines on human fecundability is encumbered by methodological challenges including, for example, temporal variation in vaccine-related factors (vaccine characteristics, accessibility, eligibility, hesitancy, policies, etc.), healthy vaccine and selection biases of available preconception cohorts (pregnancy planners, women undergoing in vitro fertilization, etc.), and inherent limitations of electronic health care data that are not designed to measure SCs (left-truncation bias, inability to capture early pregnancy loss without registered medical contact, etc.). 8 However, data that may add to evidence on the potential influence of COVID-19 vaccination on human fecundability are obviously of great importance to public health. The Czech Republic is one of the few countries where nationwide birth data for women who were vaccinated or unvaccinated for COVID-19 are available, and we therefore used these data to compare rates of SCs resulting in live births for these two groups.
Material and methods
Data for the number of live births by women in the Czech Republic aged 18–39 years (hereafter referred to as “women”) were retrieved from the Institute of Health Information and Statistics of the Czech Republic (IHIS). The data contained the number of births per month between January 2021 and December 2023 by women who were vaccinated, that is, had received at least one COVID-19 vaccine dose by the date of delivery, and by women who were unvaccinated, respectively. Furthermore, the numbers of births per month by women vaccinated by one or more doses during pregnancy were provided. A SC was defined as one that resulted in a live birth 9 months later. Accordingly, the obtained data enabled us to estimate the number of births per month by women who were vaccinated prior to SC. The lower bound for this estimate was computed as the number of women vaccinated by the date of delivery 9 months later, minus the number of women who received at least one dose of a COVID-19 vaccine during pregnancy, that is, the hypothetical situation where none of the women vaccinated during pregnancy had received any does before SC. The upper bound for this estimate was computed as the number of women vaccinated by the date of delivery, that is, the hypothetical situation where all the women vaccinated during pregnancy had received at least one vaccine dose before SC. The total number of women vaccinated against COVID-19 per month was also obtained from IHIS, and the total number of women in the population was obtained from the public database of the Czech Bureau of Statistics. Consequently, the numbers of SCs per month per 1000 women were calculated for women that were pre-SC-vaccinated and pre-SC-unvaccinated, respectively, as well as the number of SCs per month per 1000 women for all women aged 18–39 years in the Czech Republic. The study relied solely on secondary anonymized data and was, therefore, exempt from research ethics board review.
Results
Estimates of the number of SCs for vaccinated and unvaccinated women are shown in Figure 1. During the study period (January 2021–March 2023), there were approximately 1,300,000 women aged 18–39 years in the Czech Republic, and the proportion of vaccinated women increased until reaching a steady state of around 70% of all women by the end of 2021 (Figure 1(a)). The Comirnaty (Pfizer-BioNTech) and Spikevax (Moderna) mRNA vaccines comprised 96% of all administered COVID-19 vaccine doses, with an 11:1 ratio in the use of these two vaccines. Blue-shaded areas in Figure 1(b) show intervals between upper and lower bounds for the estimates delineating the actual SC rates. The estimated intervals for SC rates varied substantially for vaccinated women at the beginning of the study period where few women had been vaccinated, that is, representing a very low absolute number of SCs. Notably, at least from June 2021, monthly numbers of SCs per 1000 women were considerably lower for women that were vaccinated before SC, compared to those that were not. SC rates for women vaccinated before SC were generally lower than expected based on their proportion of the total population of women (Figure 1(a) and (b)). In June 2021, an increase in the rate of SC was observed for women unvaccinated before SC, and this higher rate was maintained over the subsequent 6-month period. During 2022, rates of SCs stabilized in both women that were vaccinated and unvaccinated before SC, and the uncertainty in the estimates subsided. However, throughout 2022, SC rates remained about 1.5 times higher for women that were unvaccinated before SC compared with those that were vaccinated before SC (Figure 1(b)). (a) Histogram showing the percentage of women in the Czech Republic aged 18–39 years who were vaccinated with at least one dose of a COVID-19 vaccine by the end of the respective month (January-December = 1–12 on the abscissa). (b) Estimates of the number of successful conceptions (SCs) per 1000 women aged 18–39 years according to preconception COVID-19 vaccination status, and SC rates for all these women, respectively. The blue-shaded areas in Figure 1(b) show the intervals between the lower and upper bounds for estimates of actual SC rates for women vaccinated (dark blue) and unvaccinated (light blue) before SC. The large initial divergence between the lower and upper bounds for estimated SC rates for vaccinated women was due to the small sample size, as indicated in Figure 1(a).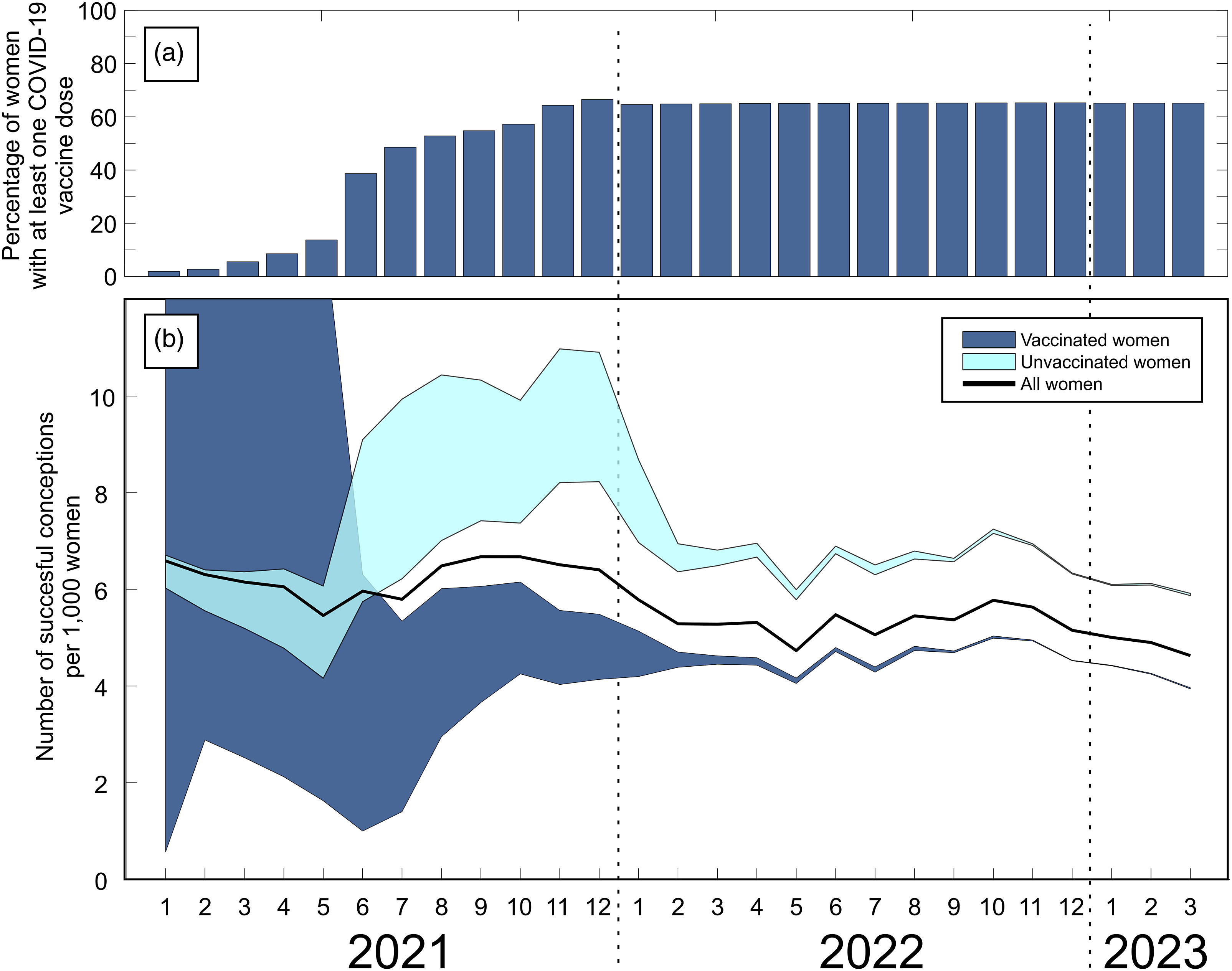
Discussion
In this study, we used simple descriptive statistics and data visualization to analyze summary COVID-19 vaccination and birth data for all women in the Czech Republic aged 18–39 years and found that at least from June 2021 to December 2022, monthly numbers of SCs per 1000 women were markedly lower for women vaccinated before SC compared to those that were unvaccinated before SC. Furthermore, the contribution of women vaccinated before SC to the total monthly rate of SCs was substantially lower than expected according to the proportion of vaccinated women in the total population of women.
A sharp fall in birth rates has been reported in many countries following the COVID-19 pandemic and has been associated with economic instability, social inequality, and the stringency of pandemic-related social restrictions.1–3 An association between declining birth rates and onset of COVID-19 vaccinations has also been suggested and thought to indicate that women postponed conception until after vaccination.2,3 Indeed, concern about COVID-19 vaccine safety has been a major reported reason for remaining unvaccinated, and reproductive adults appear particularly anxious about potential adverse effects of COVID-19 vaccination on fertility.9,10 In this regard, although the overall safety of COVID-19 vaccination during pregnancy has been well documented, 5 vaccination may be associated with menstrual pain and changes in menstrual flow and cycle length, and direct effects of the Comirnaty vaccine (Pfizer-BioNTech) on the ovarian follicle were reported recently.6,7 However, to date very little data on a relationship between birth rates and COVID-19 vaccination status have been reported.
To our knowledge, the relationship between COVID-19 vaccination status and rates of SCs has not been examined previously on a population level. However, a prospective cohort study of pregnancy planners (n = 2126 women) in the US and Canada indicated that preconception COVID-19 vaccination did not influence the probability of SC, albeit that study only included women who were trying to conceive and was also limited by use of self-reported vaccination status. 11 Contrary to these findings, our current real-world population data from the Czech Republic indicated that COVID-19 vaccination was associated with a substantial and sustained decrease in SC rate compared to non-vaccinated women.
While the strength of our study is its nationwide unselected sample of fertile women, the observed association between decreased SC rates and COVID-19 vaccination is, of course, not proof of a causal relationship between vaccination and fecundability. For example, it is possible that more women who wished to become pregnant, that is, achieve SC, chose not to be vaccinated, and/or that more women who did not plan to become pregnant opted for vaccination. Indeed, such self-selection bias is compatible with the increase in SCs of the women unvaccinated before SC in the second half of 2021 (Figure 1(b)). However, to defer vaccination was against sanctioned national public recommendations in the Czech Republic at the time, and if this type of self-selection bias had been the predominant underlying factor for the observed reduction in SC rates in vaccinated women, the total fertility rate for the entire population would have remained relatively constant throughout the study period. In contrast, the total fertility rate in the Czech Republic decreased from 1.83 births per 1000 women in 2021, to 1.62 in 2022, and 1.45 in 2023, 12 and, therefore, self-selection bias does not seem to fully explain the observed association between vaccination status and SC rates. Notably, we and others have previously found a batch-dependent safety signal for the Comirnaty vaccine (Pfizer-BioNTech) in the Czech Republic, Denmark, Sweden, and the US, and the possibility of a disproportionate influence of early batches of this vaccine on SC rates remains to be investigated.13–16
The current study should be interpreted in view of other limitations that include, for example, unmeasured confounders such as the age distribution of the 18- to 39-year-old women, socioeconomic and lifestyle factors, comorbidities and sexual health, effects of individual COVID-19 vaccine products or vaccine boosters, concurrent COVID-19 infection, preconception fertility, contraception use, pregnancy loss, stillbirths, and paternal health and vaccination status. Unfortunately, we were not granted access to this information. Also, the estimated SC rates for vaccinated women were uncertain, mainly in the early phase of the vaccination campaign. In addition, the Czech Republic population is almost exclusively Caucasian, and results may not apply to other ethnicities.
Conclusion
We conclude that at least from June 2021, SC rates in the Czech Republic for women vaccinated against COVID-19 before SC were substantially lower than for those who were unvaccinated before SC. These hypothesis-generating and preliminary results call for further studies of the influence of COVID-19 vaccination on human fecundability and fertility.
Supplemental Material
Supplemental Material - Rates of successful conceptions according to COVID-19 vaccination status: Data from the Czech Republic
Supplemental Material for Rates of successful conceptions according to COVID-19 vaccination status: Data from the Czech Republic by Vibeke Manniche, Tomáš Fürst, Max Schmeling, Jonathan D Gilthorpe and Peter Riis Hansen in International Journal of Risk & Safety in Medicine.
Footnotes
Author contributions
Conceptualization: TF and VM; methodology: TF and VM; investigation: TF, VM, and PRH; data curation: TF and MS; formal analysis: TF, VM, MS, JDG, and PRH; writing-original draft: VM, TF, JDG, and PRH; writing-review and editing: VM, TF, MS, JDG, and PRH; project administration: VM; and funding acquisition: VM.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Donation-based crowdfunding (Danish Ministry of Justice, Department of Civil Affairs, journal number 23-700-06725). The funding source did not have any role in the writing of the manuscript or the decision to submit it for publication.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.