
Abstract
Although young people in Sweden report good health, there is an increase in self-reported symptoms. However, there is uncertainty regarding what these symptoms signify. Using interviews with 15-year-olds, this research examines what the symptoms asked for in the Health Behavior in School-Aged Children survey represent. The analyses takes inspiration from a performative understanding of surveys. It demonstrates that while problems such as feeling low and nervousness are reported as poor mental health, some participants refer them to deep-seated problems and others to everyday challenges. The results points to the necessity of reporting from symptom scales with caution to avoid the pathologisation of everyday problems.
Keywords
Introduction
Swedish young people are feeling worse and worse. About half of the country’s 15-year-olds experience frequent psychosomatic problems (Dagens Nyheter, 2018).
The mental health problems of children between the ages of 10 and 17 has increased by more than 100% in 10 years (Socialstyrelsen, 2017).
The first statement above was published in one of the biggest national newspapers in Sweden, Dagens Nyheter, in a supplement on young people’s mental health, and the second (translated by authors) was published online in a research report by Socialstyrelsen, a Swedish state agency that manages health care. Over the past few decades, similar statements have been common worldwide in media articles and research reports, suggesting a drastic decline in young people’s mental health (cf. Morrow and Mayall, 2009). The idea of a crisis is now firmly rooted in society and has been accepted by the public, politicians, officials and practitioners who deal with young people’s health. Survey studies on young people’s mental health, however, paint a much more complex picture. For example, the latest report from the cross-national survey Health Behavior in School-Aged Children (HBSC) identifies two seemingly contradictory trends among young people in Sweden. Although young people report very good health and quality of life in almost all areas, especially compared to young people in other countries, there has been an increase in their self-reported psychological and somatic symptoms since 1986, especially among girls (Folkhälsomyndigheten, 2018). Among 15-year-olds, 66% of girls and 85% of boys report high or very high levels of well-being, while 62% of girls and 35% of boys report at least two symptoms per week (Folkhälsomyndigheten, 2018). In other words, HBSC shows an increase in self-reported symptoms, whereas levels of well-being are stable. Likewise, the global prevalence of anxiety disorders and major depressive disorders remained largely stable between 1990 and 2010 (Baxter et al., 2014). While the increase of self-reported symptoms has been reported widely, the fact that young people also report high levels of well-being has tended to be underreported in the media. There is a duality in the state of young people’s mental health that is rarely reported.
Due to the complexity of the issue, conclusions in literature reviews have become cautious about identifying trends in young people’s mental health (e.g. Petersen et al., 2010:13; Potrebny et al., 2017). In a systematic review of 21 published primary studies on self-reported psychosomatic health complaints, one study (Potrebny et al., 2017) concludes that there was a minor increase of adolescents’ self-reports in Northern Europe. However, they emphasise that the identified changes may reflect a shift in how young people perceive and report health complaints (Potrebny et al., 2017). The Royal Swedish Academy of Sciences concluded in a systematic review, following a State of the Science Conference (SSC) about the mental health trends of children and young people between 1945 and 2010, that it is ‘not possible to verify or disprove the general perception of a sharply rising frequency of mental disorders among Swedish children and adolescents’ (Petersen et al., 2010: 13). There remains considerable uncertainty regarding what the reported symptoms of young people mean (e.g. What kind of problems cause feeling nervous or stomach ache?). The panel at the SSC asked whether the questions used in surveys were relevant to young people in terms of both how they feel and how they view their situation (SSC, 2010). To come to terms with the uncertainty regarding what the reported symptoms of young people mean, the panel emphasised the importance of including children’s and young people’s perspectives in mental health research (SSC, 2010). If we return to young people themselves and ask what the symptoms represent in their lives, we can contribute to the picture that quantitative studies have given us and ultimately acquire a deeper understanding of the measured symptoms.
The media reports that emphasise a crisis in young people’s mental health often refer to symptom scales. These include the HBSC symptom checklist (HBSC-SCL), which is ‘a brief screening instrument that asks about the frequency of occurrence of symptoms, such as headache, stomach-ache, irritability/bad temper, feeling nervous, etc.’ (Erhart et al., 2009: 163). If at least two of the symptoms are reported more than once a week, it is classified as poor mental health. The framing of young people’s reported problems as symptoms of poor mental health is underpinned by the processes of indexing and categorising young people’s health reports (Kvist Lindholm and Wickström, 2020). In this article, we wish to leave the established categorisations of self-reported symptoms and examine what they represent in young people’s lives (i.e. what causes them), from the perspective of young people themselves, taking the HBSC screening instrument as an example. Our use of the HBSC-SCL as an example is highly relevant, as it is commonly referred to in research reports and the media, and similar symptom checklists are used worldwide (e.g. Baxter et al., 2014). We report on our research, which comprised of interviews with forty-one 15-year-old teenagers in two schools. This article is part of a larger research project on young people’s perspectives on mental health. In this article, we focus on one question measuring self-rated health by using eight symptoms and examine what these symptoms represent in young people’s everyday lives. We begin by providing an overview of HBSC. We then discuss the theoretical lenses that guided our exploration of measurement in the HBSC health survey and develop the specific aim for this article. Before presenting the results of our research, we also provide an account of the methods used for this research and how the fieldwork was accomplished.
The HBSC-SCL
The HBSC cross-national survey was founded in 1982 and adopted by the World Health Organization’s (WHO) Regional Office for Europe in 1983. The survey is distributed every 4 years to young people aged 11, 13 and 15 in 48 countries and regions in Europe and North America. It seeks to develop knowledge over time about young people’s well-being, behaviour and social contexts (WHO, 2019). Sweden has participated in the survey since 1985. In 2017, the questionnaire was sent to 150 randomly selected school classes that consisted of students in the appropriate age groups. The large-scale questionnaire contains 79 questions and many sub-questions covering physical and mental health, drug use, social relations, school, social media and so on. In this article, we report from the parts of our interviews that focused on the symptom checklist. This question is presented in Figure 1 (Inchley et al., 2018).
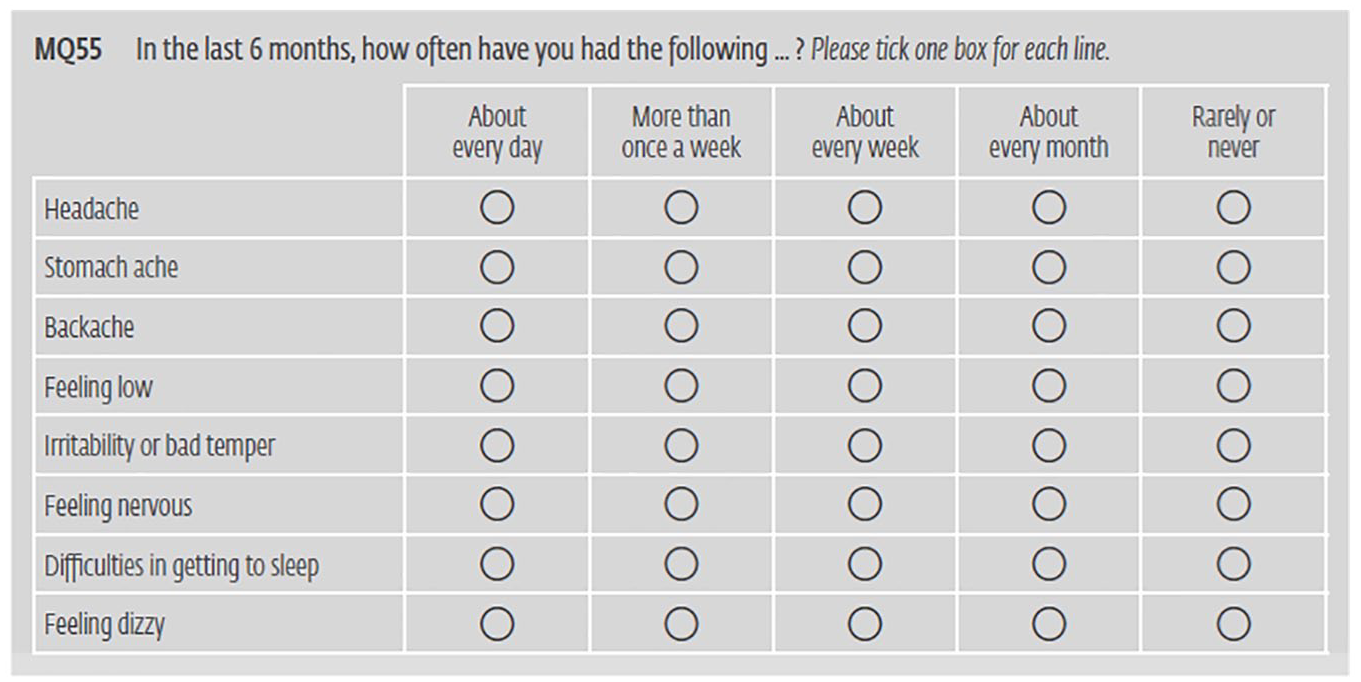
Question 37 of the HBSC survey in relation to the frequency of symptoms (English version).
The checklist is meant to cover four psychological symptoms (i.e. feeling low, irritability or bad temper, feeling nervous, difficulties in getting to sleep) and four somatic symptoms (i.e. headaches, stomach aches, backaches, feeling dizzy) and measures trait of psychosomatic complaints (Inchley et al., 2018: 71). The reason for including somatic symptoms is that different forms of pain may be expressions of psychological encumbrance or psychosocial stress (Folkhälsomyndigheten, 2018). The measurements of the instances of these symptoms are presented on a scale from rare to frequent (i.e. about every day, more than once a week, about every week, about every month, rarely or never). In Sweden, incidents of at least two psychological or somatic symptoms, or a combination of these, more than once a week during a period of 6 months are registered as psychosomatic symptoms. Haugland and Wold (2001) conducted a study to determine the validity of an extended version of the HBSC-SCL by interviewing 15- to 16-year-olds. Their findings indicate that most items on the checklist were adequately valid, but that some represented positive or neutral feelings. This means that not only problems, but also situations that young people perceive as positive or neutral such as being in love, are measured as psychological or somatic symptoms. The Public Health Agency of Sweden explicates that even if the symptoms could be typical reactions to various aspects of normal life, they still imply risks: ‘People who suffer from, for example, anxiety, feeling low and sleep disorders have a considerably greater risk of being struck with psychological problems later on’ (Folkhälsomyndigheten, 2014: 23). In our discussion, we will return to this notion of risk and consider what it might mean for our understanding of and reporting on young people’s mental health.
Theoretical approach
In this section, we refer to three theoretical fields that inform our research: studies of knowledge practices in the social sciences, sociological literature on medicalisation, and interdisciplinary childhood studies. Social science studies of knowledge practices begin with the assumption that surveys do not only represent people’s attitudes, views and experiences but also enact these elements into being (Law, 2009). According to Law (2009), surveys do more than describe or capture reality. They are not just neutral tools; rather, they themselves are part of knowledge production practices. Taking the example of reports on young people’s mental health, they do not only describe reality in terms of health, well-being and indicators of poor mental health. They also partake in creating reality when representing young people’s experiences in terms of psychosomatic symptoms and poor mental health. Various methods of creating reality are performative in the sense that ‘realities are not real outside the chains of practices that perform them’ (Law, 2009: 242). If we transfer Law’s theories to representations of poor mental health in reports, the focus is on psychosomatic symptoms due to a large network of practices. Without the symptom checklists, young people filling in questionnaires, tables of symptoms developing over time and research reports and news in the media, these psychosomatic symptoms would not be at the centre of our interest when considering young people’s well-being. The focus on ‘symptoms’ is created within a network of measuring and representing practices (Law, 2009). However, when research reports and media articles take the symptom checklist as the core focus, they create a deficit model approach to the study of children’s lives and mental health (Morrow and Mayall, 2009). The other side of the dual picture referred to above is effaced, and young people’s mental health is enacted as a phenomenon that is defined by the incidence of psychosomatic symptoms.
The performative understanding of methods allows us to question whether we can contribute to the extant knowledge of this subject by using other methods. In this article, we explore a contextual understanding of young people’s experiences. It is not that symptom checklists are wrong; rather, they create a discourse on young people’s mental health only in the context of its own categorisation of what characterises poor mental health. This may misdirect efforts to counteract poor mental health, as has been demonstrated in previous research (Kvist Lindholm, 2015; Kvist Lindholm and Zetterqvist Nelson, 2015; Wickström, 2012, 2018; Watson et al., 2012). When survey reports focus on symptom frequencies, young people’s self-reported symptoms are treated as indicators of normal or divergent mental health. In this matter, social science researchers have argued that public health surveillance governed by biomedical diagnostic systems has led to the medicalisation of childhood, where well-being has become frozen within nosological categories (Watson et al., 2012).
In the sociology literature, the concept of medicalisation is used to describe aspects of bodies and lives that have previously been deemed ‘normal’. These aspects have typically been outside the jurisdiction of medicine and are now considered medical problems (Clarke et al., 2003). The concept does not refer to misguided professional efforts but to political economic shifts such as a focus on risk and efforts to rationalise surveillance (Clarke et al., 2003). Processes of medicalisation are often preceded by various types of pathologisation. To distinguish between the two concepts, pathologisation involves institutions labelling certain conditions as pathological, while medicalisation concerns the interventions that become justified because of this labelling (Scholl, 2017). The benefit of medicalisation is that deviants are less condemned and social stigma may decrease (Conrad, 2007). The negative effect of medicalisation is that complex social problems are individualised, as the burdens of problems are placed on individuals, not on institutions and practices (Conrad, 2007).
Exploring the well-being of young people from their point of view is a distinctive field of research within interdisciplinary childhood studies (e.g. James, 2007; Wickström and Zetterqvist Nelson, 2018; Watson et al., 2012). Their perspectives contribute to knowledge that contextualises their experiences. In our previous research concerning the realisation of psycho-educational programmes in schools, we were struck by the discrepancies between what are considered to be the needs of young people from the viewpoint of the programmes and from the viewpoints of young people themselves (Kvist Lindholm, 2015; Kvist Lindholm and Zetterqvist Nelson, 2015; Wickström, 2012, 2018). We found that the categorisation of mental health in terms of psychosomatic symptoms has certain repercussions on young people, as psycho-educational programmes are distributed to schools, who then implement techniques designed as treatment, but practised as prevention (Kvist Lindholm, 2015; Kvist Lindholm and Zetterqvist Nelson, 2015; Wickström, 2012, 2018). Reports of a decline in mental health have spurred an invasion of psycho-educational programmes, and young people’s mental health has been dealt with on contract, regardless of them experiencing problems or not (Watson et al., 2012). The focus of the programmes is on young people’s individual thoughts and emotions, while young people highlight mental health as a complex social and relational matter (Wickström, 2018). Studying the realisation of the programmes revealed that generalised programmes link poorly with young people’s lived experiences, and that it is therefore important to enact contextualised versions of young people’s well-being through examining young people’s perspectives.
Research based on young people’s perspectives is scarce, not only regarding their experience of filling in health surveys and symptom checklists, but also regarding their lived experience of these symptoms’ underlying causes. We seek to address this research gap. In this article, our aim is to examine what the psychological and somatic symptoms in the HBSC-SCL represent in young people’s lives (i.e. what causes the symptoms), from the perspective of young people themselves. To that end, we will discuss any discrepancies between young people’s perspectives gained from the interviews regarding their symptoms and the representation of these same symptoms in media articles and research reports. We will also address the probable consequences of these discrepancies.
Methods and ethics
In order to recruit 15-year-olds, we contacted 50 principals of senior-level schools to locate the schools that were selected to participate in HBSC 2017–2018. Out of four identified schools, one principal agreed to let us approach the selected class in the inner-city school. However, several of the other principals got interested in our interview study and asked if we could include them in our research despite them not being part of the HBSC survey. We agreed and chose two classes in a provincial school. The three classes contained a mix of sociodemographic backgrounds. Ethical approval was granted by the Regional Ethics Board (No. 2017/171-31). The teachers informed the parents and the students that two researchers would visit the class. During the information meetings, we introduced ourselves and our research project. The young people received written information about the study and our interest in exploring young people’s views on questions asked in the HBSC survey and what the symptoms reported by them represent in their daily lives. They also received written information to bring to their parents. If they were interested in participating in the study, they were asked to sign the consent form. Students below the age of 15 were asked to acquire consent from their parents as well. We informed the participants about the possibility of withdrawing at any point, and seven of the participants made use of this option. In total, 32 girls and 9 boys took part in the interviews. The consent given to participate was not considered a single process before the fieldwork started but as an ongoing consideration during the research process. We were observant of any reactions of being uncomfortable or in a bad way and saw to pause an interview or refer a participant to professional support.
To build trust through the practice of repeat interviews and to allow detailed descriptions of the participants’ perspectives, 41 individual and 10 group interviews took place (cf. Hammersley and Atkinson, 2007). The individual interviews provided participants with the possibility of expressing opinions that they might not have been comfortable sharing in a group. In the group interviews, the participants could agree/disagree and position themselves in relation to the questions discussed. Towards the end of the individual interviews, we asked for suggestions on how to create groups in which everyone felt comfortable sharing their thoughts. Some had very specific requests, while others were open to several possibilities, which made the process easy. Based on their suggestions, we created nine same-sex groups and one mixed-gender group consisting of two to five people each. Three of the 41 students could not partake in the group interviews because of illness.
Both the individual and group interviews were semi-structured and lasted between 45 and 90 minutes, depending on how comprehensive the participants’ answers were. During the individual interviews, we sat side-by-side with the participants and allowed them to recall the questionnaire by quickly looking through a copy of it. For those who had not seen it before, they could look through it carefully. In this article, we will report the data that we acquired from interviews about what the eight symptoms listed in question 37 represented in the participants’ everyday lives. We asked them about each symptom and how they experienced it. Moreover, follow-up questions served as an important strategy to examine their perspectives further (e.g. in what situations they experienced a specific symptom). In order to get a background understanding of the students’ particular situations and problems, we also paid attention to the narratives that they constructed about their lives in other parts of the interview. Thus, our analysis is based on the participants’ narratives that developed during the interviews.
We employed a thematic analysis to organise our data (Braun and Clarke, 2006) and sort the participants’ perspectives on the eight symptoms and what they represented into different patterns or themes. Initially, we sorted their narratives according to the content of the interviews. We used Microsoft Excel to generate a content list that was close to the participants’ referred problems (e.g. fever, conflicts at home, presentations in school) and the incidences referring to them. We then combined the initial codes into broader units of analysis (Braun and Clarke, 2006), such as bodily experiences, relationships, school issues and difficult life events. Two to 3 months after the interviews, we returned to the schools to get feedback on our preliminary analysis. The participants’ comments confirmed some aspects of the analysis and led us to re-evaluate others. To give an example, we divided the problems into those that were ‘everyday’ and those that were more long-lasting serious problems. One student commented that the difference was not about duration but degree of affect, and other students agreed with this comment. The feedback became crucial for identifying the main themes. It was important to us that our themes include all possible aspects of the problems that the participants had identified and connected to their symptoms. In order to make sure our themes were comprehensive, we reread the interview transcripts individually, discussed the content again and refined the themes. As a note, all of the names used in the article are anonymised, and all of the quotes have been translated from Swedish into English by the authors.
Results
The main finding of the larger research project is that the determining factors of young people’s mental health concern friends, family and school. No matter what type of problems the participants referred to, they all shared the view that relationships and school play a crucial role in their well-being and form the basis of a meaningful life. This means that relationships and school also cause problems. In our analysis of the underlying causes of the symptoms, from the perspective of young people themselves, we found two main themes – namely, everyday problems and deep-seated problems, and three sub-themes of each theme, as seen in Figure 2.

The thematic map of the underlying causes of the participants’ symptoms.
There is, of course, a sliding scale: everyday problems can become complicated issues and deep-seated problems can diminish. Most of the participants, however, described their own and other’s experiences as feeling good (i.e. feeling good but having everyday problems) or not feeling good (i.e. being in a complicated and serious situation), as demonstrated in the excerpt below.
Sara: If I think about myself compared to others, then I don’t think I have many problems, even if I think that it is hard work in school. One is stressed before a test, or one has a headache because there is a lot to do in school. [. . .] But perhaps I don’t have as many headaches as someone who experiences serious depression, or that I am not feeling good [. . .] I perhaps have it now and then, because I have a lot to do, but then it passes.
Sara made a distinction between those who do not feel well and those who are under a lot of pressure but still feel well (e.g. herself). Based on our analysis of the interviews, we divide the results into everyday problems and deep-seated problems. The excerpts below are chosen as illustrative examples. We also expand the information in relation to different cases by summarising the narratives that evolved during the interviews. By going beyond the description of the data, we make arguments related to our aim.
Everyday problems
In relation to the question of what caused the eight symptoms, a considerable number of the participants expressed that they were fine, but still reported experiencing common everyday problems. In the analysis, we identified three salient sub-themes that are related to everyday problems: the body, school and relationships.
Symptoms related to the body
When talking about the body, we refer to the mindful body to emphasise a holistic view of bodily experiences in which body and mind are united (Scheper-Hughes & Lock, 1987). Many of the participants’ experiences of the eight symptoms were caused by menstruation or illness. Lisa explained about having a headache:
What does having a headache mean?
For me, a headache is when you have a fever.
Other common explanations in relation to the eight symptoms was related to bad posture, exercising or bad eating habits:
Feeling dizzy then: What does it mean?
It is when I have been eating badly and then exercised, for example. Then I usually feel dizzy.
The participants’ experiences of the eight symptoms were also caused by social media. Nick recounted his difficulties in getting to sleep:
After 11, it is almost always the phone that stops me from falling asleep. You are on the phone instead of going to sleep.
And what do you do on the phone?
Text people or check YouTube.
So it disturbs your sleep?
I guarantee that. It would be odd if it did not.
Social media, interacting with people and online entertainment made it difficult for Nick to fall asleep. Others mentioned that school activities interfered with their body. Rachel explains, You know, we have had concerts and rehearsals; we have had those all week. Then you get a backache, because you stand up a lot.
The bodily reactions that the participants referred the eight symptoms to were reactions to human activities or illness, experiences that were part of their lives. The participants considered themselves to be feeling well, even as they managed these issues. The reactions were ordinary responses to managing the body during exercise or in times of illness, and the mismanagement of the body due to social media or ergonomics. Therefore, seen from the perspectives of the participants, the symptoms represent ordinary and recurrent bodily experiences that are not related to poor mental health.
School
The eight symptoms also referred to the physical environment of the school as well as to school-related activities. The sound in school created dizziness or headaches for some participants. For others, heat or crowded rooms created dizziness. The most salient aspect, however, concerned the young people’s experiences of presenting a project or receiving feedback on a test.
Feeling nervous then?
I usually become like that when we have presentations in front of the class. [. . .] You have searched for facts, you have written down text, and you are supposed to stand up and give an account for both the teacher and the class. Then you become like this: ‘Will they judge me now?’ Then I usually become very nervous.
Conducting a presentation in front of their classmates resulted in many of the participants feeling nervous. Considering that presentations are standing element in school activities, the issue of feeling nervous was a symptom that arose from time to time. Another symptom arose in relation to succeeding in school:
Feeling low?
One is tired or not feeling well because – it is not necessarily something big really but – something might have happened in school or you did not do well in a test or something like that.
Many symptoms represent everyday problems related to performance in school. These comprise ordinary experiences related to the participants’ daily occupation that often involves presentations and tests. The symptoms therefore represent the results of the participants’ aspirations and efforts to manage their schoolwork; the participants did not express these problems as mental health issues.
Relationships
The third sub-theme that this group of participants referred the eight symptoms to was relationships:
Irritability or bad temper?
It is kind of like being a little angry.
What might have happened?
One is perhaps tired and then becomes irritated. Somebody is annoying. Or one might have quarrelled with ones’ mum in the morning about something.
Anna, and many others, emphasised interactions and relationships as the main reasons for feeling irritated or bad-tempered. John’s account of his difficulties in getting to sleep exemplifies the meaning of social relationships in young people’s lives:
Difficulties getting to sleep: What does it stand for, for you?
One can have problems falling asleep. One thinks too much, perhaps.
When your thoughts start to spin, what do you think about?
Mostly about myself and things I have done. I think like this, ‘Why did I do this?’ ‘Why did I say this?’ and lots of other things. No big things. One said ‘Hello’ perhaps, and then one regrets it because one thinks it was silly.
John wished to fit in with others and behave in a way that was considered appropriate, and this appropriateness was something he thought about at night. The eight symptoms in this sub-theme concerned relationships, thoughts about social behaviour and how to get on well with people. Anna, John and the other participants struggled with these questions on a daily basis, but nonetheless reported that they were doing well. Quarrelling with somebody, agonising over interactions and determining one’s position in a specific group of young people were part of their everyday lives but did not mean that they were experiencing poor mental health. A related problematic aspect of the HBSC-SCL is the duration of the period in which the participants are asked to report on their symptoms. The cut-off point is two problems more than once a week for 6 months. However, the participants stated that it was difficult to look back over 6 months and that their markings were related to how the situation was currently or to what happened during the break preceding the lesson where the questionnaire was distributed.
To conclude, the first theme of everyday problems was associated with issues that were mere consequences of being human and having a social life. The participants talked about a body to manage, schoolwork to handle and relationships to manoeuvre. Although these common problems occasionally proved difficult to navigate and resulted in symptoms such as feeling low, problems sleeping, headaches or nervousness, they also created meaning in the participants’ lives. The interviews demonstrated that the three factors (i.e. the body, school and relations) represented everyday problems that invoked a lot of effort but were actually invaluable to the participants’ well-being.
Deep-seated problems
In the second theme, the participants related the same eight symptoms to deep-seated problems. The problems are diverse and complicated and derive from the participants’ local social contexts. The three identified sub-themes concern exposure to difficult life events, serious school problems and a lack of social affinity.
Exposure to difficult life events
A common trope in this sub-theme was related to the social sphere at home. In the following extract, Elsa explains what feeling low means to her: Very bad things have happened. One is not happy, but one is not very, very sad, so one is crying. One is kind of empty.
Without specifying, Elsa made us understand that she had been in a situation that was problematic for her. Towards the end of the interview, it was obvious that she had been drawn into a serious conflict between her parents and was accused by one of them of withholding information about the other’s infidelity, and she was blamed for not trying to bring about reconciliation. Other participants spoke about difficult life events related to illness and death in the family. These life events created chaotic situations that had an extensive impact on their mental health.
Joanna spoke about multiple symptoms, such as feeling low, irritability and bad temper, that constantly troubled her. She also described an incident of abuse: A close friend of Joanna’s family had contacted her on the Facebook Messenger application and threatened to rape her, describing in detail how he would realise his plan. Joanna reported the man, and a series of meetings with the police and social services began. The narratives in this sub-theme represent young people who reported having problems because of their social situations. These situations can create feelings of powerlessness, as Emily explains: I want to get help, I want to feel better, but I don’t know how I would feel better, kind of. These are things that I have no possibility to influence, like when people have died and conflict and such in the family. I cannot just go in and solve those issues.
The quote from Emily represents the desire for change and help. Being unable to influence a situation is a salient aspect of the first sub-theme.
Serious school problems
The second sub-theme of the main theme of deep-seated problems concerns managing school, either in the form of failure or success. Greta related several of the eight symptoms to school, including difficulties concentrating and understanding. To sit an exam made her nervous, so she did not even try. Her failure in school also interfered with her social life: I speak to my friends and relatives, and then suddenly they bring up school, and I feel rather low. They have good grades and then it is me. I feel like – I am not worth anything.
Greta explained how her failures in school made her feel worthless in relation to her friends and relatives. Another group of young people spoke about being successful in school but always feeling under immense pressure to perform.
I have had lots of headaches. Stress in school. Stomach aches are also stress-related. I am very stressed in school. [. . .] I must get my exercise done; I must get my homework done. [. . .] Headaches and stomach aches essentially happen every day. (Alba)
Greta and Alba represent the participants who told that they experienced several of the eight symptoms because of deep-seated problems regarding their schoolwork. These problems also created feelings of worthlessness or insufficiency.
A lack of social affinity
The third sub-theme in relation to the participants’ perspectives on symptoms caused by deep-seated problems involved difficulties with socialising and finding meaning in life.
Feeling low: Can you relate to that?
Yes, it runs in the family. I was a bit depressed before. [. . .]
Depression, you say: What does that mean to you?
One has lost the will to live, and one just sits there and cannot go on any longer. I usually become like that when I don’t get any variation. [. . .] One wakes up, goes to school and then one sits there [Laughs].
Michael described a problematic situation where he found school activities monotonous, a situation that sometimes resulted in feelings of meaninglessness. Michael and other participants in similar situations recounted the daily struggle to find meaning and ultimately connected their symptoms to a lack of social affinity.
To conclude, the second theme of deep-seated problems includes various disparate problems. The narratives that the participants shared regarding the symptoms and causes revealed difficult circumstances, such as exposure to serious problems at home, in school or in relation to social integration. The participants explained that these issues influenced their lives to a large extent and that they sometimes found it difficult to function.
Discussion
When research reports and media articles focus on self-reported symptoms, young people are problematically framed as a homogeneous group increasingly suffering from poor mental health (Morrow and Mayall, 2009). Explorations of young people’s perspectives, specifically in relation to their symptoms, question the theory that these symptoms are representative of poor mental health alone. Above all, the analysis contributes to the knowledge of young people’s mental health by elucidating and diversifying the causes of the symptoms reported. The fact that we found two different themes demonstrates the importance of nuance in reports. If our sample had been bigger, we would most likely have found an even greater variation. Therefore, our results demonstrate that what is measured in symptom scales represents a variety of problems with varying levels of severity. Although Haugland and Wold (2001) did not categorise their interview answers according to the level of severity, our study is consistent with their conclusion that some symptoms are not perceived as complaints but are instead related to neutral or positive experiences and result of lifestyle. The participants in their study, just like the participants in ours, indicated that several symptoms represented workload at school, spatial and physical conditions, and negative experiences with family, peers or school (Haugland and Wold, 2001). Young people’s experiences of symptoms are complex and diversified, and cannot be attributed to poor mental health alone.
The question on why there is an increase in self-reported symptoms over time, however, remains. Even though this was not initially in focus for our study, the young people draw attention to several aspects that had changed over time and could be considered as one of several plausible explanations for the measured increase. One interesting aspect of our participants was their desire to talk to somebody about their problems. This willingness to talk about their problems may be one reason for the measured increase in reported symptoms over time. Other reasons for the escalation in reported symptoms could be due to the increased openness of discussions surrounding mental health; this was seen in the participants’ ability to talk about their deep-seated problems. Compared to 1985 when Sweden joined the HBSC, our interviews demonstrate that young people today are used to evaluating and discussing health issues with friends and on the Internet. Moreover, the fact that social relations have been expanded from physical venues to digital arenas may contribute to increased pressure, as may the increase of achievement tests in school. Finally, the way the participants used concepts, such as anxiety, depression and feeling low, shows that the value of words have been devaluated, as they are used daily (Kvist Lindholm and Wickström, 2020). This contrasts with the extent of their use in 1985; this questions the possibility of discussing the prevalence of poor mental health over time without taking into account the changes to young people’s lives and society over time (Kvist Lindholm and Wickström, 2020).
Another important discussion is what is considered poor mental health and what is deemed reactions to the conditions of life. Because of its relation to definitions of normal and abnormal, the choice of cut-off points in screening scales is a compromise between ignoring abnormal cases or misjudging normal ones (Tseng, 2017). The Public Health Agency of Sweden legitimises the inclusion of problems that may be part of normal life in their calculations, because the problems can constitute a risk of future problems in relation to poor mental health (Folkhälsomyndigheten, 2014). Referring to the risk of psychological problems changes the measurement to a question of probability in relation to future problems (Gillespie, 2012). It means that the cut-off point (i.e. at least two symptoms more than once a week during a period of 6 months) is not only legitimised by what the reported symptoms might represent at the moment of filling out the questionnaire, but also by what these symptoms might denote in the future. In the reports from the HBSC-SCL, however, the symptoms are reported as present mental health problems and as representations of an actual increase in poor mental health (Folkhälsomyndigheten, 2018). Gillespie (2012) argues that reducing reported problems to a probability and framing them as a risk is problematic, as it may mean that more and more aspects of young people’s everyday lives are pathologised (Gillespie, 2012). Studying the surveillance of children’s health in Taiwan, Tseng (2017) identifies the deployment of a ‘riskised regime’, through which a higher prevalence of mental health problems is claimed. The inclusion of risk when choosing the cut-off point in symptom scales can make the high prevalence of symptoms quite unsurprising.
Going beyond the HBSC-SCL, which was used as an illustrative example, and drawing on Law’s (2009) theories of what surveys perform and ‘what versions of the real they are helping to enact’ (p. 244), we can see that there are risks involved in reporting on young people’s mental health by mainly drawing from symptom checklists. First, there is a risk that the reports create a reality that does not match young people’s lived experiences. Everyday problems and deep-seated problems become blanketed by a specific cultural model (i.e. individual medical symptoms used to understand young people’s well-being). Everyday experiences of young people, who argue that they feel well, are reported alongside problematic circumstances and experiences. This conflation means that emotional, physical and relational reactions to everyday life are at risk of being reported as signifiers of poor mental health. Emotional reactions to young people’s everyday problems may be considered erroneous, and human conditions turned into treatable disorders (Conrad, 2007). If the everyday managing of the most valuable elements of young people’s lives (body, friends, family and school) become reduced to individual symptoms of poor mental health, their bodily reactions, ambitions and relational issues are pathologised. Reporting young people’s emotional reactions as pathological may in turn lead to a process referred to as self-pathologisation and become a problematic aspect of young people’s self-understanding (Scholl, 2017). Young people may begin to view everyday problems caused by living, working and interacting as health problems in need of cures.
When symptoms caused by all sorts of problems are reported as indicators of poor mental health, the more serious problems are at risk of being overlooked. A common factor in this regard is related to social problems. When the psychological and somatic reactions to the problems the young people with deep-seated problems described are marked on a checklist, the social causes of the problems may become hidden (Conrad, 2007). Reactions to conflicts at home; incidents of assault, death and disease; problems in school; and a lack of affinity are similarly reported as individual mental health problems. The use of an individual medical lens for emotional distress may lead to a displaced focus that moves from the influence and impact of difficult circumstances to individual deficiency (Graham, 2015). Young people’s reactions to the situations described seem expected and plausible: They are reasonable reactions to unreasonable situations. Viewing them as medical problems may conceal the real impact of institutions and social, economic and cultural contexts (Morrow and Mayall, 2009). Young people’s psychosomatic symptoms become foregrounded while the educational system, the pressure of schooling and problematic life situations risk being pushed to the sidelines. Moreover, young people living under difficult circumstances may come to view themselves as the problem, as if being irritated and nervous and feeling low are health problems that they should rid themselves of.
Second, we see a risk of medicalisation if reports re-contextualise young people’s lived experiences into crisis of mental health. The reports and media representations have repercussions for young people’s lives. A majority discourse has developed that young people are not feeling well; a discourse that politicians, officials and professionals has taken as the starting point when they plan for interventions in school (Graham, 2015; Watson et al., 2012). Since the turn of the millennium, manual-based psycho-educational programmes have been implemented broadly in schools in Sweden and elsewhere in the minority world in order to counteract the assumed deficits in the psychological and emotional skills of young people (Graham, 2015; Kvist Lindholm, 2015; Watson et al., 2012; Wickström, 2018). The interventions begin with a general understanding that most young people have similar problems to do with their thoughts, emotions and attitudes and target groups of school children, irrespective of their mental health (Kvist Lindholm, 2015; Kvist Lindholm and Zetterqvist Nelson, 2015; Wickström, 2012, 2018). Psycho-educational techniques based on values, norms and methods defined in a context of surveillance medicine and treatment technologies have been implemented as prevention (Watson et al., 2012). The broader social, relational and cultural contexts that young people highlight as the foundation of their well-being risk being downplayed and social causes being depoliticised. Efforts to counteract poor mental health must start with a careful identification of needs in the local context. For example, the young people in these classes pointed out various needs that can be addressed within the context of the school: improvement within the physical environment, increased support for conflict resolution, and reorganisation of activities in order to minimise pressure. Considering the results presented here, we believe that dealing with young people’s everyday problems daily and securing access to professional services for those who have deep-seated problems constitute the prevention of mental health problems among young people. To avoid the generalisation of young people’s problems, we suggest a cautious interpretation (cf. Gariepy et al., 2016) when reporting from symptom scales and a meticulous identification of young people’s experiences in their social and cultural context.
Footnotes
Acknowledgements
We would like to thank the young people who shared their thoughts with us in this research project. We also thank the anonymous reviewers for their valuable comments.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this paper.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this paper: This work was supported by the Swedish Research Council for Health, Working Life and Welfare (Reg. No. 2016-00129) and the Swedish Research Council (Reg. No. 2016-00784).