
Abstract
Research reports that young people aged 10 to 24 years are reluctant to seek help for a mental health problem due to multiple factors and that intervention within this demographic is critical. The aim of this review was to critique the existing literature, using a systematic approach on how the type of helping relationship affects young people’s help-seeking behavior, engagement, and maintenance in mental health care. Searches of nine databases produced 22 relevant articles of original research with young people aged 10 to 24 years for inclusion in this review. A thematic analysis identified three themes: (a) context of trust and confidentiality, (b) supportive rapport, and (c) collaborative approach to treatment. Findings indicate that researchers, practitioners, and policy makers need to prioritize the role of the helping relationship and its core components of trust and confidentiality, supportive rapport, and collaborative treatment, as essential in the provision of meaningful mental health care for young people.
Background
Youth Mental Health and the Reluctance to Seek Help
The World Health Organization (WHO, 2018a) has estimated that up to 16% of people aged 10 to 19 years in the world today are experiencing a mental health problem. Despite the visible increase in health promotion campaigns and the availability of services within high-income countries in recent times, policy makers and practitioners are still facing problems with engaging and maintaining young people in mental health care (Gulliver et al., 2010; McGorry et al., 2013; WHO, 2018a). Mental health problems are the leading cause of disability in young people, and suicide is now the second leading cause of death among 15 to 29 year olds globally (WHO, 2018b). Having mental health problems in youth can result in lower quality of life as well as educational difficulties, and this impact can last into adulthood (WHO, 2018a). Considering that up to half of all mental health disorders will emerge between the 14 to 24-year age range, understanding what supports young people to seek help for a mental health problem, and stay engaged in mental health care, is important in the design and provision of timely, evidence-based, and meaningful interventions (Bramesfeld et al., 2006; Cornally & McCarthy, 2011; O’Neill et al., 2018; WHO, 2018a).
Why Young People Are Not Seeking Help
The most widely cited factors that impact a young person’s decision to seek help are stigma and a young person’s cultural influences (Goodwin et al., 2016; Gulliver et al., 2010; Nam et al., 2010; Rothì & Leavey, 2006) followed by low mental health literacy, negative attitudes or beliefs, previous negative experiences, and an overreliance on self-management strategies (Bilican, 2013; Chen et al., 2014; Cranford et al., 2009; Del Mauro & Williams, 2013; Dogra et al., 2011; Eisenberg et al., 2012; Hickie & McGorry, 2007; Jorm et al., 2008; Klineberg et al., 2011; Loureiro et al., 2013; Nada-Raja et al., 2003; Pheko et al., 2013; Rickwood et al., 2007; Rowe et al., 2014; Rughani et al., 2011; Ryan et al., 2014; Vanheusden et al., 2008; Wilson & Deane, 2012; Wilson et al., 2005). Young people’s developmental needs of emerging autonomy and self-reliance can also decrease help-seeking propensities (Chan, 2013; Gonzalez et al., 2005; Jackson Williams, 2014; Raviv et al., 2009; Wilson & Deane, 2012; Yoshioka et al., 2014). While research reports that young men and women are impacted differently by help-seeking, young people, regardless of gender, find help-seeking for a mental health problem difficult and generally prefer to turn to informal sources of support (Biddle et al., 2004; Bilican, 2013; Bradford & Rickwood, 2014; Burlaka et al., 2014; Draucker, 2005; Hernan et al., 2010; Jorm et al., 2007; Leavey et al., 2011; Lynch et al., 2018; MacLean et al., 2013; Nam et al., 2010; Rowe et al., 2014). Other findings report that a lack of services in rural areas, unsuitable services, and practitioners or unskilled community gatekeepers can prevent young people from accessing help (Birleson & Vance, 2008; Boyd et al., 2007; Burlaka et al., 2014; Cakar & Savi, 2014; Charman et al., 2010; Gilchrist & Sullivan, 2006; Hernan et al., 2010; Judd et al., 2006; Klineberg et al., 2011; Mackenzie et al., 2014; Mariu et al., 2012; Purcell et al., 2011; Raviv et al., 2009; Rickwood et al., 2005, 2007; Rughani et al., 2011; Ryan et al., 2014; Samouilhan & Seabi, 2010; Vanheusden et al., 2008).
Interpersonal factors, such as lack of trust, are often reported in the literature as help-seeking barriers, and a few studies have found that the human element is of central importance to young people in initiating and maintaining the use of mental health services (Jones et al. 2017; Medlow et al., 2010; Rickwood et al., 2007). What young people require from a helping relationship, the approach taken by the professional helper, and the quality of the rapport are imperative factors to consider when understanding young people’s help-seeking behaviors, how they engage with mental health services, and in helping maintain continued participation in mental health care.
Aims and Scope of Review
The aim of this review is to critique the existing literature on how the type of helping relationship affects young people’s help-seeking behavior, engagement, and maintenance in mental health care. As there are currently no reviews dedicated to this topic, this review will collate, synthesize, and critique literature that reports any aspect of the role that the helping relationship plays in engaging and maintaining young people in mental health care. This review will use the term “young people” to refer to all youths aged between 10 and 24 years of age (Sawyer et al., 2018; WHO, 2018a). The term “mental health problem” is used in this article to refer to the spectrum of personal distress and mental conditions that can affect an individual. The terms “helper” and “practitioner” refer to people in services whose primary role is to offer one-to-one therapeutic support for an individual’s mental health.
Method
Database Search Methodology
This narrative review employed a systematic approach to literature searching and retrieval, across nine databases, using the methodology proposed by Best et al. (2014). First, key concept groupings were established: (a) Young People (b) Help-Seeking Behavior and (c) Mental Health (d) Service Utilization. All studies included had to be relevant to all four groupings. Boolean logic was used in analytical searches to identify search parameters but as not all databases are standardized, this search procedure was adapted to suit each one. For databases without sophisticated search algorithms, the browsing method was employed. Searching cessation was informed by Kraft and Lee’s (1979) method as discussed in Best et al. (2014) which included (a) satiation, (b) disgust, and (c) utility. This procedure has been detailed in a PRISMA diagram (Figure 1).
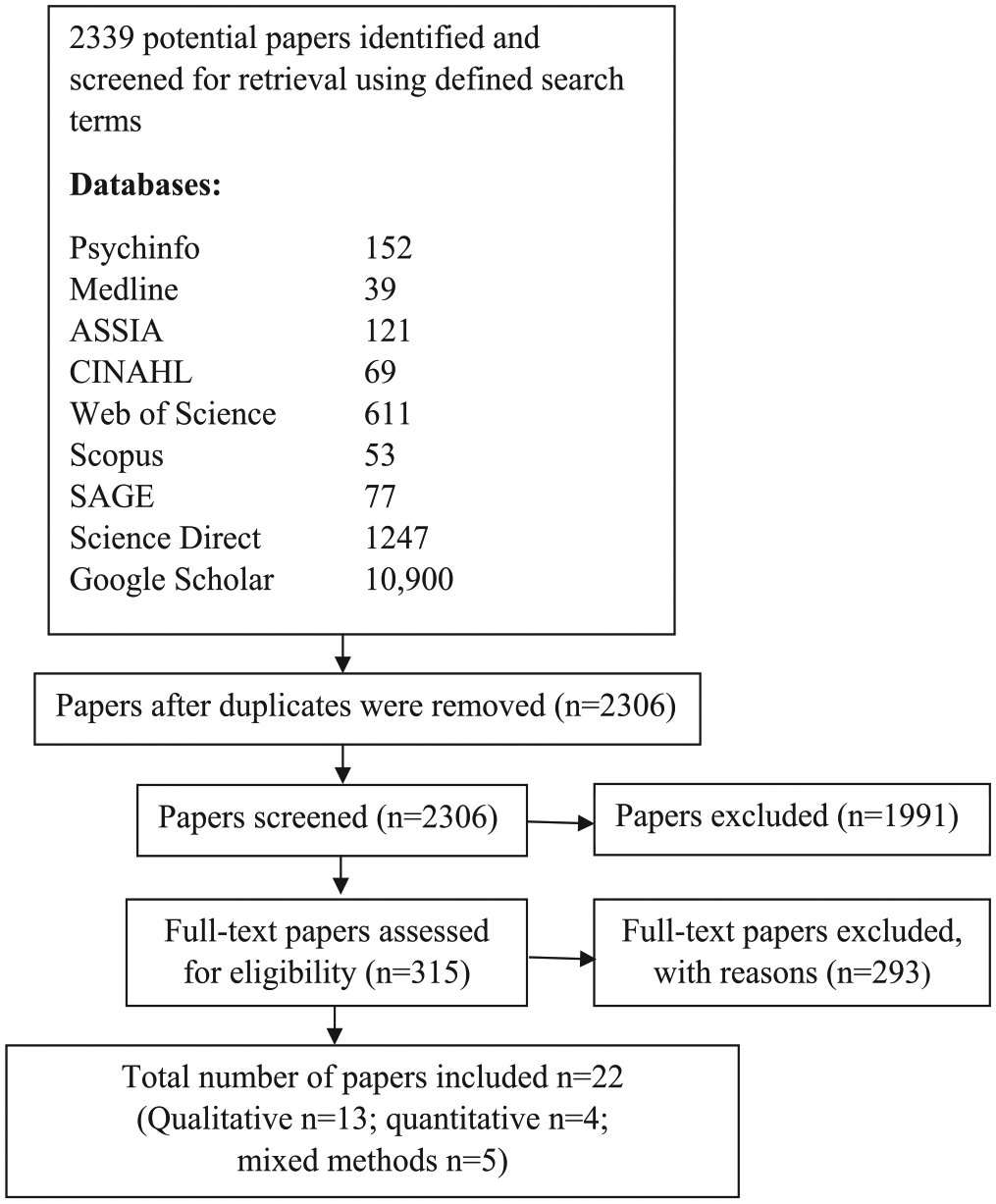
PRISMA diagram.
Selection Criteria
All studies selected for this review had to contain direct reporting from young people on the role that the helping relationship plays in engaging and maintaining them in mental health care. Studies had to include male and female participants aged between 10 and 24 years of age and had to be published in a peer-reviewed journal between 1996 and 2018. Database searching was restricted to the English language. Reviews or research using university students were excluded.
Study Selection
In total, after duplicates were removed, 2,306 studies were retrieved. Abstracts were reviewed, and 315 relevant studies were selected. Finally, 22 studies were identified as meeting the selection criteria. Only one study investigated the helping relationship specifically (Ungar et al., 2018). The remaining 21 studies covered broader topics and so each paper was read in-depth to search for relevant data for inclusion in this review.
Coding and Analysis of Studies
Each study was recorded on a preformulated coding sheet and described the key study characteristics. After the final studies were identified, the process of analysis involved reading and searching for data in reference to relationship qualities, dynamics, behaviors, characteristics, qualities, or traits of the helper. Relevant data were subsequently thematically analyzed, coded, and refined into key themes using the methodology of Braun and Clarke (2006).
Study Characteristics
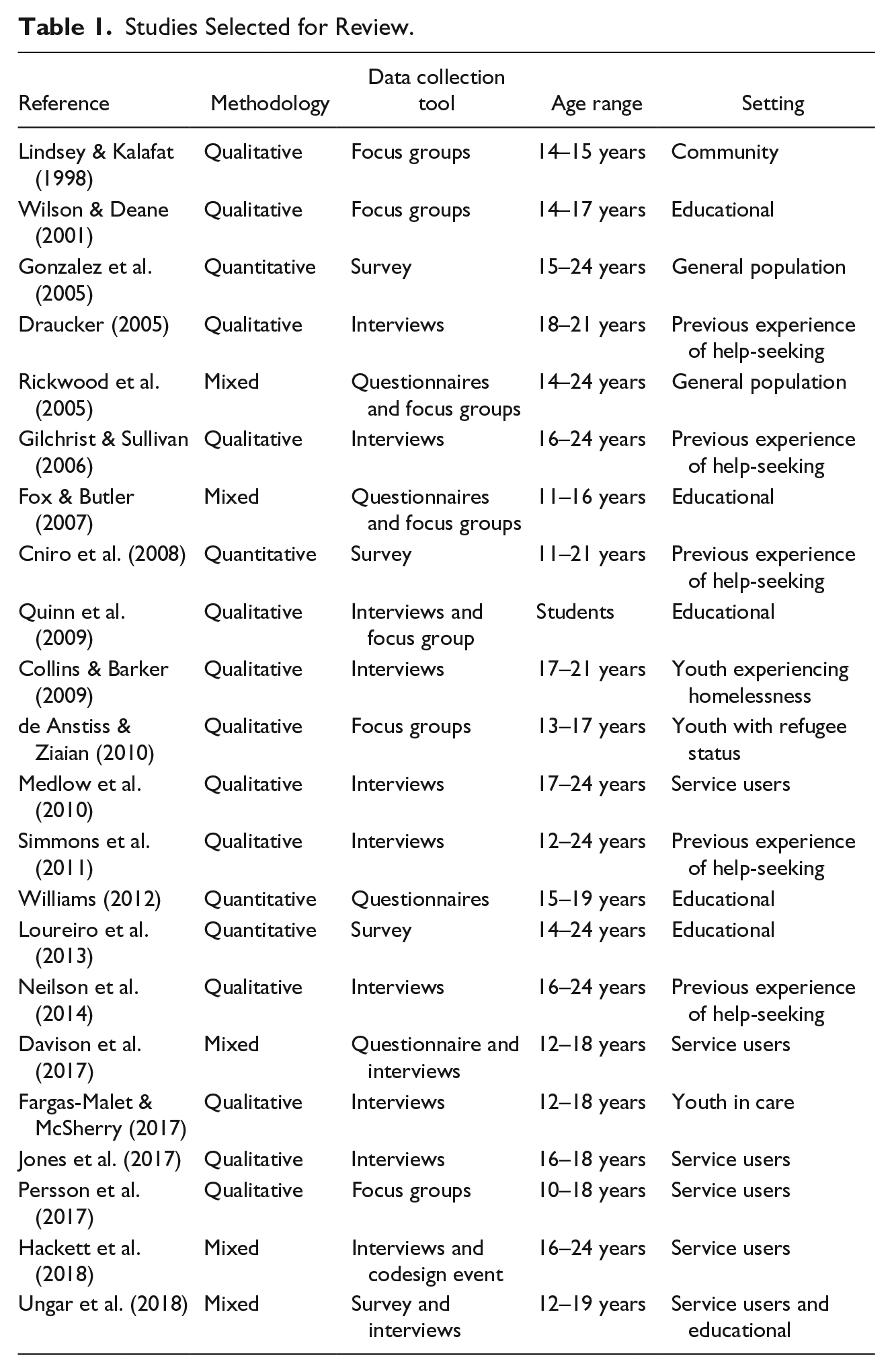
This section provides a summary of the location, year, methodologies, sample size, participant information, and study setting. An overview of the key characteristics of each study selected for this review is available in Table 1. Following this, the findings of the thematic analysis will be presented.
Studies Selected for Review.
Location and year
The studies in this review were published between 1998 and 2018. The most frequent locations were Australia (n = 6) (de Anstiss & Ziaian, 2010; Gilchrist & Sullivan, 2006; Medlow et al., 2010; Rickwood et al., 2005; Simmons et al., 2011; Wilson & Deane, 2001), the United Kingdom (n = 6) (Collins & Barker, 2009; Davison et al., 2017; Fargas-Malet & McSherry, 2017; Fox & Butler, 2007; Jones et al., 2017; Quinn et al., 2009), and the United States of America (n = 4) (Cniro et al., 2005; Draucker, 2005; Gonzalez et al., 2005; Lindsey & Kalafat, 1998). The remaining studies included three from Canada (Hackett et al., 2018; Neilson et al., 2014; Ungar et al., 2018), one from Sweden (Persson et al., 2017), and one from Portugal (Loureiro et al., 2013). One study had a mixed location; research was conducted with young people in Jamaica (Williams, 2012), but findings were reported and published through a university in the United States of America.
Methodologies
The studies in this review were predominantly qualitative (n = 13) (Collins & Barker, 2009; de Anstiss & Ziaian, 2010; Draucker, 2005; Fargas-Malet & McSherry, 2017; Gilchrist & Sullivan, 2006; Jones et al., 2017; Lindsey & Kalafat, 1998; Medlow et al., 2010; Neilson et al., 2014; Persson et al., 2017; Quinn et al., 2009; Simmons et al., 2011; Wilson & Deane, 2001), with four studies using quantitative methodologies (Cniro et al., 2005; Gonzalez et al., 2005; Loureiro et al., 2013; Williams, 2012) and five using mixed methodologies (Davison et al., 2017; Fox & Butler, 2007; Hackett et al., 2018; Rickwood et al., 2005; Ungar et al., 2018). The qualitative research used either focus groups (n = 4) or interviews (n = 9), with one study using interviews and a codesign event. The quantitative research comprised of surveys (n = 3) and questionnaires (n = 1). The mixed methodology research used focus groups or interviews with questionnaires or surveys (n = 6).
Participants
Most studies provided clear information regarding sample size and participant demographics. All studies included male and female participants aged 10 to 24 years of age. Studies that reported gender breakdown numbers were generally representative but tended to have more female participants, with only three studies having equal representation. Only one study reported a disparate variance in gender, where out of 23 participants there was only a single male participant.
Study setting and research populations
This review included studies from a mix of settings and young people from different backgrounds including community, education, previous experiences of help-seeking, service users, in state care, experiencing homelessness, refugee status, and general population. These are detailed in Table 1.
Sample size
Across the 22 studies, sample sizes ranged from 7 to 5,877 participants. Qualitative studies had between 7 and 85 participants, and quantitative studies ranged from 34 to 5,877 participants. A few studies included other participants, such as parents or professionals; however, data on young people were presented clearly and these data were extracted and then analyzed to be included in this review.
Findings
This review has identified three key themes in relation to the type of helping relationship that young people have reported as necessary to engage with and maintain their participation in mental health care. These themes—(a) context of trust and confidentiality, (b) supportive rapport, and (c) collaborative approach to treatment—are nested within each other and describe the essential and connected features in the type of helping relationship that young people need when seeking support for their mental health (Figure 2).
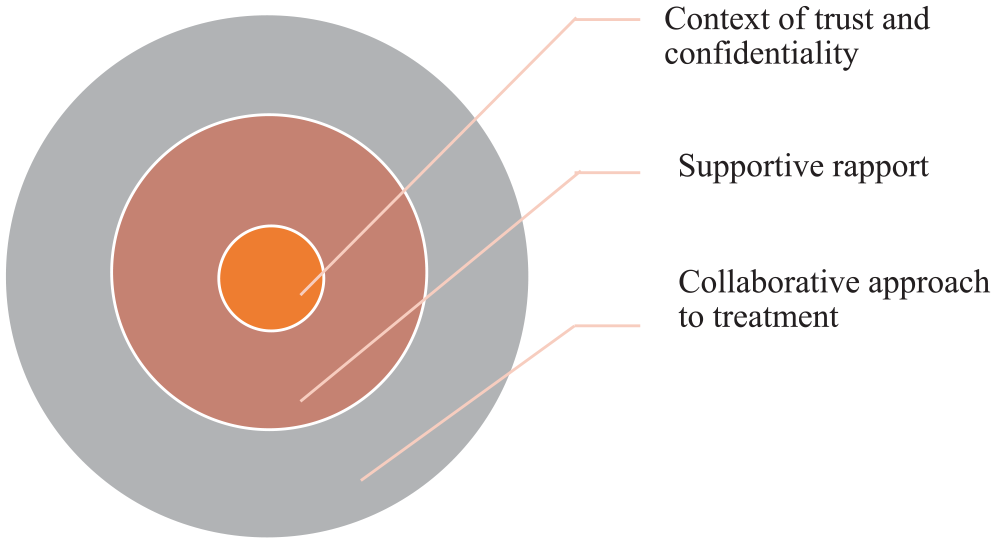
The core components of the helping relationship in youth mental health care.
Context of Trust and Confidentiality
The first theme, trust and confidentiality, was the most frequently reported finding in the selected research. As young people often enter services with fears that a helper will disclose personal information or content from private discussions to others, the provision of an ethically bound confidential service can create a context for trust to develop (Draucker, 2005; Fargas-Malet and McSherry, 2017; Fox & Butler, 2007; Gilchrist & Sullivan, 2006; Gonzalez et al., 2005; Jones et al., 2017; Loureiro et al., 2013; Lindsey & Kalafat, 1998; Medlow et al., 2010; Persson et al., 2017; Quinn et al., 2009; Rickwood et al., 2005; Wilson & Deane, 2001). Findings imply that the relationship between trust and confidentiality is axiomatic; trusting relationships for young people are built on confidentiality and so it is only as confidentiality is proven protected over time that trust can establish (Fox & Butler, 2007; Gilchrist & Sullivan, 2006; Gonzalez et al., 2005; Jones et al., 2017; Lindsey & Kalafat, 1998; Williams, 2012; Wilson & Deane, 2001). Trust and confidentiality may be of a higher priority for young people who experience homelessness, refugee status, or issues related to sexuality (Cniro et al., 2005; Collins & Barker, 2009; de Anstiss & Ziaian, 2010). As this theme of trust and confidentiality is the most frequently reported finding in this review, it can be understood as playing a central role in youth mental health care and in the building of a supportive rapport.
Supportive Rapport
The second theme describes how interpersonal factors merge to create a positive and supportive rapport between a young person and their helper. Supportive rapports, provided in conjunction with meaningful care, are built on good interpersonal skills from a helper who is understanding, caring, open, attentive, nonjudgmental, genuine, relatable, available, and who ensures young people feel comfortable and welcomed (Cniro et al., 2005; Collins & Barker, 2009; Draucker, 2005; Fargas-Malet & McSherry, 2017; Hackett et al., 2018; Jones et al., 2017; Lindsey & Kalafat, 1998; Medlow et al., 2010; Neilson et al., 2014; Quinn et al., 2009; Ungar et al., 2018; Wilson & Deane, 2001). Asking for help can be difficult, and when young people do ask for support it is crucial that they are provided with care in a timely manner from an empathetic helper (Lindsey & Kalafat, 1998; Medlow et al., 2010; Quinn et al., 2009; Wilson & Deane, 2001). Two studies report that young people want to see professionals who like working with young people and are passionate about their job (Draucker, 2005; Lindsey & Kalafat, 1998). Young people can need different types of professional boundaries depending on their risk or resilience profiles (Ungar et al., 2018). Importantly, young people want the time and opportunity to build positive rapports and establish stable relationships as these are crucial to ongoing engagement and maintaining participation in mental health care (Davison et al., 2017; Jones et al., 2017; Persson et al., 2017). This supportive rapport, built on trust and confidentiality, provides a young person with the necessary context to engage in collaborative care.
Collaborative Approach to Treatment
The third theme identified in this review concerns findings regarding the ability of the helper to discuss, inform, and offer an individualized and collaborative treatment plan to young people. Young people want to be involved in decisions about their care and have a choice of which intervention they would like to try; if they are excluded from this decision-making process, then there is a greater chance they will disengage from treatment (Davison et al., 2017; Draucker, 2005; Gilchrist & Sullivan, 2006; Neilson et al., 2014; Persson et al., 2017; Quinn et al., 2009; Simmons et al., 2011; Wilson & Deane, 2001). In particular, young people reported wanting a helper that was knowledgeable about mental health, providing them with information and high-quality guidance (Draucker, 2005; Gilchrist & Sullivan, 2006; Neilson et al., 2014; Quinn et al., 2009; Simmons et al., 2011; Williams, 2012; Wilson & Deane, 2001). Helpers also need to be knowledgeable and skilled regarding the lived reality of a young person’s experiences; for example, if a young person identifies as lesbian, gay, or bisexual, then helpers need to be knowledgeable about how specific sexuality issues can impact an individual’s mental health (Cniro et al., 2005). Similarly, if a young person has refugee status then the helper needs to be skilled at working cross-culturally (de Anstiss & Ziaian, 2010). Finally, young people value consistency in their mental health care (Davison et al., 2017; Hackett et al., 2018) and need developmentally appropriate interventions (Jones et al., 2017; Persson et al., 2017). The offering of a collaborative treatment plan to young people, based on a supportive rapport, can increase engagement and maintain participation in mental health care.
Findings Limitations
The selection criteria used for this review has been informed by the aims of the research and by academic publishing guidelines, which might have had a significant impact on the studies selected. Academic journal publishing guidelines often recommend the exclusion of research that includes university students due to issues concerning generalizability and representativeness (Hanel & Vione, 2016). While age ranges vary in youth research, many journals set the age limit of 10 to 24 years (Sawyer et al., 2018; WHO, 2018b). The inclusion of research in this review that provides direct reporting from young people resulted in 86% of research from high-income countries. However, the exclusion of university students and age limit (studies including participants up to 25 years of age) for this review resulted in the exclusion of nine studies, creating almost complete exclusion of studies from countries often referred to as being in the Global South (Odeh, 2010). Apart from one study (Williams, 2012), all the studies in this review were from higher income (95%), Western (100%), and English-speaking countries (90%). This meant that three studies—Burlaka et al. (2014) from the Ukraine, Bilican (2013) from Turkey, and Mbuthia et al. (2018) from Kenya, which met the study criteria, direct reporting from young people—did not meet academic publishing criteria, the exclusion of university students and age limits. Including these three studies might have provided a deeper dimension of analysis regarding cultural differences and similarities, alternative perspectives, and new insights, to the understanding of trust, confidentiality, support, care, and collaboration. This current review therefore provides a limited cross-cultural analysis of the topic.
Discussion
This review has identified three key themes regarding the type of helping relationship that young people need to increase their help-seeking, engagement, and maintenance within mental health care. Much research reports findings, such as trust and empathy, in an extracted form, as individual influences, described as barriers or facilitators. This removes the context and dynamic between a practitioner and client in a help-seeking relationship and provides a shallow understanding of how these factors interact. How the key themes interact together as part of a pattern of supportive behavior will now be discussed in a reintegrated and contextualized form.
The Type of Helping Relationship
When a young person decides to seek professional help for a personal problem, they are looking for a supportive relationship where they can feel safe, comfortable, understood, respected, and guided to solve their problems (Draucker, 2005). Before this can happen, a young person must overcome pragmatic and administrative barriers that are common in mental health services and find a helper to trust, a practitioner. Personally, they may have to navigate self-stigma and grief regarding the loss of self-management while disclosing sensitive and personal information to numerous people in exchange for the promise of help (Chan, 2013; Rickwood et al., 2005). This process can be both intimidating and complicated and is often why young people prefer established relationships for help with personal problems (Gilchrist & Sullivan, 2006; Loureiro et al., 2013; Rickwood et al., 2007). At the beginning of treatment, the helper is unknown and unpredictable and so discussing personal problems with them can cause young people discomfort (de Anstiss & Ziaian, 2010; Gilchrist & Sullivan, 2006; Gonzalez et al., 2005; Loureiro et al., 2013; Quinn et al., 2009; Rickwood et al., 2007). Rapport is an intangible interpersonal quality, described by Jones et al. (2017) as something that is “felt” and a young person needs time to gauge a practitioner’s behaviors to assess if they can provide the type of supportive rapport they need (Draucker, 2005; Jones et al. 2017). The literature presents clear findings demonstrating how foundationally important it is in practice, before treatment can begin, that time is made available for establishing a good working rapport.
Trust and Confidentiality
Although research consistently reports that trust and confidentiality are core concerns for young people, some studies, typically quantitative, portray “trust” and “confidentiality” as external entities, without reference to between whom this trust exists and how it is built, maintained or broken within the context of a helping relationship. A practitioner may view themselves as trustworthy, engaging, or approachable, but this does not mean that a young person does; practitioners need to establish professional boundaries regarding confidentiality at the first meeting so that a young person can make a reasonable presumption about how the helper will respond to personal disclosures, and this provides the foundation for trust (Gilchrist & Sullivan, 2006; Loureiro et al., 2013; Rickwood et al., 2007; Williams, 2012). As young people lack privacy and control in their lives in general, hypervigilance over confidentiality breaches may not be an unrealistic concern for them and what a young person deems a breach of confidentiality and what a practitioner does can differ. Confidentiality has a dialectical dynamic, and dimensions of trust appear to be connected to the depth and duration of the relationship with the helper and their proven ability to maintain confidentiality over time (Draucker, 2005; Fox & Butler, 2007; Gilchrist & Sullivan, 2006; Gonzalez et al., 2005; Jones et al., 2017; Lindsey & Kalafat, 1998; Rowe et al., 2014; Williams, 2012; Wilson & Deane, 2001).
Young People’s Development and Life Circumstances
A major consideration when rapport building, and in the application of individualized treatment, is a young person’s development and life circumstances. Looking at developmental differences across the 10 to 24 age range, five research studies in this review explored middle and later adolescence and five investigated emerging adulthood, 18 to 24 years. There were no studies investigating early adolescence alone, but the age range of 10 to 24 was included in the remaining 12 studies and findings were reported together (see Table 1). Although the findings show that young people, across these age ranges, report similar needs in the type of helping relationship, the literature does not adequately address or discuss how these needs can differ throughout the age range of youth. Some studies do report developmental needs, but these tend to be for younger adolescents and there is not enough insight on the needs of emerging adults.
While all young people prefer informal environments and rapport styles, younger adolescents may need activities or games for rapport development (Davison et al., 2017). If an adolescent’s distress stems from their homelife, seeking help can be further complicated by the need for caregiver consent (Draucker, 2005; Fox & Butler, 2007). Adolescents can have fears about their caregivers finding out the contents of their disclosures in case it would exacerbate their problems, specifically around stigmatized behaviors such as self-harm, substance abuse, or suicide ideation (Fox & Butler, 2007; Michelmore & Hindley, 2012; Wilson et al., 2005). Importantly, as caregivers often initiate help-seeking on younger adolescents behalf, practitioners need to find out if a young person’s participation is voluntary and to what level of involvement, if any, they want from caregivers within their treatment decisions, being upfront from the beginning with examples of when they have to break confidentiality and also what that process would look like (Persson et al., 2017; Rickwood et al., 2005; Simmons et al., 2011; Wilson & Deane, 2001).
The research is clear around young people who are experiencing severe distress, such as suicidal ideation or those at psychiatric in-patient services, and how practitioners may need to be more explicit in their demonstration of respect and understanding in supporting recovery (Hackett et al., 2018; Neilson et al., 2014). Young people experiencing homelessness or who are in state care have often had their trust broken previously by adults, and building trust with a practitioner could need more time (Collins & Barker, 2009; Fargas-Malet & McSherry, 2017). When working with youth with refugee status, practitioners need to be skilled at cross-cultural work, as a lack of understanding about the refugee process and differing conceptualizations of mental health can re-traumatize youth or cause more problems (de Anstiss & Ziaian, 2010).
Collaboration
The factors that will influence a young person’s engagement and maintenance in mental health care will not always be evident to practitioners upon first meeting (Simmons et al., 2011; Ungar et al., 2018). To alleviate young people’s caution to engage in interventions, practitioners have to first demonstrate that they take their distress seriously and that they have the interpersonal skills needed to help that young person solve their problem (Draucker, 2005; Fargas-Malet & McSherry, 2017; Lindsey & Kalafat, 1998; Neilson et al., 2014; Persson et al., 2017; Wilson & Deane, 2001). Young people primarily want to be listened to and to have their opinions, thoughts, and feelings treated as important; therefore allowing them enough time to feel comfortable and begin expressing themselves is important (Davison et al., 2017; Persson et al., 2017; Wilson & Deane, 2001). Young people can have differing needs regarding relationship boundaries, and Ungar et al. (2018) suggest that young people with higher levels of risk exposure often prefer looser boundaries and need the helping relationship to feel “real” while young people with higher levels of resilience can respond better to more structure, expectations, and boundaries. Jones et al. (2017) has found that trust in the process of mental health care appears to develop as therapeutic gains emerge. In this way, relationship building can be understood as an ongoing process that runs parallel to collaborative treatment.
Collaborative care is thoroughly discussed in the literature as having features of individuation, choice, and balance; practitioners have to be flexible, knowledgeable, and creative ensuring that the young person is central to a care plan and that their personal characteristics, values, and preferences are included alongside developmentally appropriate and evidence-based treatment options (Davison et al., 2017; Draucker, 2005; Gilchrist & Sullivan, 2006; Hackett et al., 2018; Jones et al., 2017; Neilson et al., 2014; Persson et al., 2017; Quinn et al., 2009; Simmons et al., 2011; Ungar et al., 2018; Williams, 2012; Wilson & Deane, 2001). Considering young people, especially under the age of 18 years, can have large aspects of their lives controlled, practitioners can actively compensate for this by ensuring they are involved in all aspects of decisions about their care and in explaining a choice of interventions in age-appropriate language. Working in this open and transparent style with young people greatly contributes to trust development (Jones et al., 2017). This can ensure that young people make informed decisions, feel secure enough to ask questions, and have space to try out an intervention without pressure. In fact, being involved in the decision-making process using a collaborative approach may in itself be therapeutic for young people as it promotes autonomy which is developmentally important for young people and may compensate for the loss of autonomy that help-seeking can cause (Chan, 2013; Simmons et al., 2011). Simmons et al. (2011) suggests that in situations where young people were very unwell, being involved in some capacity over some smaller aspects of their treatment could compensate for being excluded from larger decisions. Ultimately, if practitioners fail to include young people in decision-making, young people will often withhold information, be selective about disclosing personal information, or exit treatment earlier (Davison et al., 2017; Draucker, 2005; Simmons et al. 2011).
The Role of Services
In traditional systems, some research suggests that the time practitioners can spend with youth clients is decreasing and that practitioners may be compromising treatment or bending rules to try and balance a young person’s needs within time-restrictive service policies (Hackett et al., 2018). Policies that dictate the “minimal adequate treatment” length are often informed from research with older adults; young people often need more flexibility in appointments, consent, location, frequency, and time as well as access to accurate information and advocacy support (Davison et al., 2017; Harris et al., 2015). Hackett et al. (2018) found that young people rated practitioners who bent rules more positively in their mental health care. This raises questions about restrictive policies such as how much policy is evidence based? Who does the policy serve? and are these policies harming young people’s mental health? Adapting adult models to be more “youth friendly” will probably not suffice; it’s important that service providers recognize adolescents as a distinct cultural group with individual needs based on a spectrum of developmental needs (Rickwood et al., 2019; Sawyer et al., 2018). The task is not impossible; there are youth-designed services such as Headspace in Australia which are implementing evidence-based practice with some success over traditional models (Rickwood et al., 2019).
Research From Global South
There is a lack of research from the Global South, which have direct reporting from young people, on preferences in a supportive rapport that young people prefer when mental health help-seeking. There is a possibility that research has been conducted and reported in another language other than English which the authors could not access. Nonetheless, existing research shows that professional mental-health help-seeking rates in these regions are low and this may be due to stigma, low mental health literacy, and differing conceptualizations of mental health (Al-Krenawi et al., 2009; Burlaka et al., 2014; Dogra et al., 2011; Mbuthia et al., 2018; Pheko et al., 2013). A significant factor to consider is that this review explored the type of helping relationship in mental health care that young people want, and this is ultimately based on a Western conceptualization of mental health, which presupposes that young people view mental health problems as issues that require professional intervention (Mbuthia et al., 2018; Pheko et al., 2013). There are differing conceptualizations of mental health throughout the globe; for example, in some countries such as the Ukraine, Nigeria, Kenya, and Botswana, young people use traditional healers or religion for their personal problems (Burlaka et al., 2014; Dogra et al., 2011; Mbuthia et al., 2018; Pheko et al., 2013). In Arabic cultures, speaking about problems outside of the family is taboo because collective needs are expected to be prioritized over individual needs (Al-Krenawi et al. 2009; Bilican, 2013). This may explain why the systematic search retrieved few studies on this topic outside of Western countries. Finally, it is important to note that it is often with university students that researchers begin to explore under-researched or taboo topics and while there is established research to justify the exclusion of university students in academic and scientific publishing, it must be considered how this decision impacts on the inclusion of perspectives from the Global South.
Limitations
This review has a few limitations. First, there was only one study available that investigated the impact of the helping relationship, young people, and mental health (Ungar at al., 2018) thus highlighting the need for research in this area. Due to this limited research, the remaining data in this review were obtained from studies which examined much broader topics within young people’s help-seeking behavior. The lack of specificity and various methodologies may have affected the quality of this review. The second limitation is that this review examined English language–only research which means there may be research on this topic available in other languages. The third limitation is that research with young people up to 25 years of age was excluded and may contain data that could increase understanding on the topic. The final limitation, and the most significant, is that this review has no data on adolescents from the Global South, meaning insights from this review are restricted to the Global North.
Implications and Recommendations for Further Research, Practice, and Policy
Practice and Policy
Practitioners working with young people need to allow extra time for the development of a trusting rapport, be explicit about the limits of confidentiality, protect disclosures unless professionally obliged not to, and work collaboratively on a treatment plan in a developmentally appropriate way. The amount of time a young person requires to develop a trusting rapport with a practitioner will vary, and this process needs to be supported by service policy. Management and employers need to recruit appropriate staff and ensure that existing staff have up-to-date training from the evidence-base on how to work with young people (Jones et al., 2017; Ungar et al., 2018).
Despite the mammoth task of youth mental health reform, there is an opportunity for all providers and policy makers to improve service provision and support practitioners to provide meaningful care. This can be done by evaluating current practice through service-user feedback and in the establishment of evidence-based policies. A properly designed mental health service for young people can also contribute to a more effective and efficient service delivery, which could have the potential to eliminate other service issues (Davison et al., 2017; Fargas-Malet & McSherry, 2017; Hackett et al., 2018; Jones et al., 2017; Rickwood et al., 2019).
Policy makers and practitioners should not underestimate the role that the type of relationship plays in young peoples’ mental health care, with extra attention paid to those who may be experiencing compounded life stressors such as young people experiencing homelessness, suicidal ideation, refugee status, or are in state care. Research has demonstrated that these young people are at a substantial risk for mental health problems, may have lower resilience, be experiencing trauma, and have had their trust broken previously by adults. Responding to these young people with suitable mental health interventions is crucial (Collins & Barker, 2009; de Anstiss & Ziaian, 2010; Fargas-Malet & McSherry, 2017; Hackett et al., 2018; Ungar et al., 2018).
Research
This review has identified the lack of culturally specific research into the impact that the type of helping relationship has on young people’s help-seeking behavior, engagement, and maintenance in mental health care. This topic needs to be examined further to increase understanding as it is emerging as one of great importance in the provision of meaningful interventions (Ungar et al., 2018). It is crucial in future research that young people are not treated as a homogeneous group and that developmental needs within the 10 to 24 years age range are addressed in study designs. It is also important to critically engage with the evidence base that informs agreed-upon age ranges for guiding adolescent research as this may have unintended consequences on the exclusion of important research. Critically, there is a need for research with young people in the Global South to ensure that interventions are appropriate to the needs of all adolescents globally (Blum & Boyden, 2018).
Conclusion
This article has identified that the type of helping relationship has a significant impact upon young people and their help-seeking behavior, engagement, and maintenance in mental health care. Understanding the type of helping relationship as a central determinant in youth mental health care provides a different perspective on the problem of youth reluctance to seek help. By focusing on rapport development, trust, confidentiality, and collaborative care, practitioners can provide appropriate and responsive support that young people need and want. In the interest of improving mental health outcomes for young people, practitioners, policy makers, and researchers must prioritize the role of the helping relationship above all other factors in the provision of youth mental health care.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.