
Abstract
Objectives
We investigated whether functional social support—the degree to which one perceives support is available when needed—is associated with executive function, a key cognitive domain for everyday functioning and adaptation to change.
Methods
Analyses (n = 23,491) utilized cross-sectional data from the Comprehensive cohort of the Canadian Longitudinal Study on Aging (CLSA), a population-based study of community-dwelling adults aged 45–85 years. Executive function was assessed by neurocognitive battery. Perceived social support was measured using the 19-item Medical Outcomes Study-Social Support Survey. Logistic regression models were adjusted for sociodemographic, health, and social covariates.
Results
Positive social interactions as well as affectionate and emotional/informational functional social support were positively associated with executive function.
Discussion
Social support plays an important role in cognitive health. Diversifying social programming beyond tangible social support to target other subtypes of support may help preserve executive function in middle-aged and older adults.
Introduction
Cognitive function plays a key role in adaptation to change across the life span. Declines in major domains of cognitive function, such as executive function, can lead to reductions in independence in mid- to late-life through increasing risk of frailty (Hoogendijk et al., 2014), limitations to activities of daily living (Kim et al., 2014), institutionalization, and mortality (St John et al., 2002). Many modifiable risk factors for cognitive decline have been identified, including educational attainment (Fratiglioni et al., 2000; Iraniparast et al., 2022; Khondoker et al., 2017; Sims et al., 2011), income (Ramírez et al., 2007; Zhu et al., 2012), and physical health (Khondoker et al., 2017; Tilvis et al., 2004). However, opportunities to address many of these modifiable factors are limited by the need to intervene early in the lifespan and the complex societal structural barriers (e.g., economic status) involved. Identifying additional risk factors that can be altered in mid- to late-life to reduce the likelihood of cognitive decline is essential to supporting a globally aging population.
Social resources may provide a potential area of intervention for supporting cognitive health in mid- to late-life; however, little is understood about the processes through which social support influences cognition. Receiving emotional social support from others may reduce physiological arousal during periods of stress and thus prevent its downstream effects on the brain, a theory known as the stress-buffering hypothesis (Eisele et al., 2012; Sims et al., 2011). The act of developing and maintaining social relationships also uses various cognitive processes, encouraging their maintenance (Ellwardt et al., 2013), similar to what is observed in cognitive reserve (Eisele et al., 2012; Stern, 2002). In contrast to the stress-buffering hypothesis, a putative cognitive reserve mechanism would help to explain seemingly contradictory findings that positive social experiences as well as more negative social interactions (Hughes et al., 2008) and greater social strain in relationships (Ge et al., 2017) are all associated with higher global cognitive function.
Most research investigating the association between social support and cognitive function has focused on objective (structural) measures of support (e.g., marital status and size of social network) because this information is readily available in larger studies. However, considering only the objective quantity of support may not accurately reflect the actual levels of received or perceived social support or the potential benefit of social support interventions. Older adults often experience a trimming of their social networks over time as they focus on their most beneficial relationships and network members are lost; however, this reduction does not necessarily decrease the level of perceived social support they receive (Gurung et al., 2003).
Measures of perceived (functional) social support may explain changes in cognitive function even after accounting for structural measures of support. These measures capture access and quality of support by asking individuals whether they perceive sufficient support as being available when they need it (Sherbourne & Stewart, 1991). Higher ratings of functional social support are associated with higher scores on measures of cognitive function (Mogic et al., 2023) and lower risks of developing dementia (Khondoker et al., 2017; Sörman et al., 2015).
Whether an effect of functional social support on cognitive function is consistent across all subtypes of social support is less clear. Tangible and emotional/informational subtypes of support have been investigated in the greatest depth, often with conflicting results. Reductions in tangible support may negatively impact executive function (Dickinson et al., 2011), but increases may reflect greater need and signal a decline in cognitive health as those who report high tangible support may already be depending on these resources (Pillemer et al., 2019). In contrast, while high emotional support is not significantly associated with cognition in all studies (Eisele et al., 2012), it has generally been associated with better cognitive function in older adults (Ellwardt et al., 2013; Pillemer & Holtzer, 2016; Seeman et al., 2001; Sims et al., 2014; Stinchcombe & Hammond, 2022), whereas lower emotional social support has correspondingly been associated with worse cognitive function (Harling et al., 2020).
Assessing the types of functional social support that are associated with specific cognitive domains is essential for developing effective social support interventions to prevent cognitive decline in aging populations. Utilizing a large, population-based, community-dwelling sample of adults in mid- to late-life, this study investigated (1) whether functional social support was associated with executive function and (2) whether this association differed by subtype of functional social support.
Methods
Data Source and Study Population
Analyses utilized baseline data from the Comprehensive cohort of the Canadian Longitudinal Study on Aging (CLSA), a national, population-based, prospective panel study of community-dwelling Canadian adults between the ages of 45–85 years at recruitment (Raina et al., 2009). A detailed description of the CLSA recruitment and sampling process is provided elsewhere (CLSA, 2023). In brief, participants in the Comprehensive cohort were sampled from within 25–50 km of 1 of 11 data collection sites spread across seven provinces. Participants completed in-home surveys as well as interviews and physical examinations at their closest data collection site. The CLSA excluded full-time members of the Canadian Armed Forces; individuals living in the three Canadian territories, on federal First Nations reserves, or in institutions; and participants whom recruiting staff identified as having cognitive impairment. Additionally, we excluded participants who did not complete the assessment at their data collection site (n = 137) or who had missing data on any of our analytic variables (n = 6,469), thereby resulting in an analytic sample of 23,491.
Measures
Exposure
Functional social support was measured at baseline using the 19-item Medical Outcomes Study-Social Support Survey (MOS-SSS) (Sherbourne & Stewart, 1991). The MOS-SSS assesses overall social support as well as four subtypes of support: emotional/informational support (e.g., someone you can count on to listen to you when you need to talk), tangible support (e.g., someone to take you to the doctor if needed), affectionate support (e.g., someone who shows you love and affection), and positive social interactions (e.g., someone to get together with for relaxation). One item (i.e., someone to do things with to help you get your mind off things) is included in the calculation of the overall score of social support but is not included in any of the social support subtypes (RAND Health, 2018). Participants were asked to respond to the 19 questions on a scale from 1 (none of the time) to 5 (all of the time) based on how often the type of support described was available to them if needed. A higher score indicated greater perceived support. A combined score for each social support subtype was calculated using the average score from all items for that subtype, while the overall social support score was calculated by averaging the scores for all 19 items (RAND Health, 2018). As the social support scores were not normally distributed, low social support was dichotomized (yes vs. no [reference]) for overall support and each subtype using a cut-off of ≤3 out of 5 (reflecting support ‘none’, ‘a little’, or ‘some’ of the time).
Outcome
Executive function in the CLSA was assessed at baseline using five measures (Tuokko et al., 2017): the Animal Fluency Test (AFT) (Read, 1987), Mental Alternation Test (MAT) (Teng, 1995), Controlled Oral Word Association Test (COWAT) (Lezak et al., 2004), Time-Based Prospective Memory Test (TMT) (Loewenstein & Acevedo, 2001), and Victoria Stroop Neurological Screen Test (Stroop) (Bayard et al., 2009, 2011; Moroni & Bayard, 2009; Spreen & Strauss, 1998; Stroop, 1935; Troyer et al., 2006). Tests were modified for use in the CLSA. Specific details regarding how these instruments were modified, administered, and scored in the CLSA are available elsewhere (CLSA, 2019; Tuokko et al., 2017).
Scores on each of the five executive function tests were standardized within each test using z-scores, which were calculated separately for English and French speakers (Iacono et al., 2023). Persons who switched languages during test administration were excluded from analyses. An overall executive function score was calculated by combining the standardized z-scores on the AFT, MAT, COWAT, TMT, and Stroop. As performance on the Stroop is measured as the time to response, a higher score indicates worse cognitive function, and thus the standardized Stroop scores were reversed for inclusion in the overall executive function score (Demnitz et al., 2018).
Executive function was defined based on the distribution of combined z-scores and then dichotomized (low vs. not low). A cutpoint of at least 1.5 standard deviations (SDs) below the mean of the combined scores was used to define low executive function (Petersen et al., 1997; Sachdev et al., 2014). This cutpoint was derived from a weighted, cognitively healthy subsample (O’Connell et al., 2017) of CLSA participants and then applied to the analytic sample. The distribution of test scores by low executive function status is summarized in Supplemental Table S1.
Covariates
Sociodemographic, health, and social covariates were selected based on previous studies examining functional social support and cognitive function (Mogic et al., 2023). Sociodemographic variables were age group (45 to 54; 55 to 64; 65 to 74; ≥75 years), sex (male or female), education (less than high school; high school graduate; some post-secondary education; post-secondary degree/diploma), total annual household income (<$20,000; ≥ $20,000 to < $50,000; ≥ $50,000 to < $100,000; ≥ $100,000 to < $150,000; ≥ $150,000 CAD), province (Alberta; British Columbia; Manitoba; Newfoundland and Labrador; Nova Scotia; Ontario; Quebec), and residential setting (urban or rural).
Health covariates included self-reported clinical depression (“Has a doctor ever told you that you suffer from clinical depression?” [yes or no]) and self-rated health (poor; fair; good; very good; excellent). Additionally, 11 broad, self-reported medical conditions were combined into a dichotomous measure of chronic conditions (presence of any chronic disease vs. absence; see Table 3 for full list).
Three additional social factors were assessed: marital status (single; married/common-law; widowed; divorced/separated), owning a household pet that provides companionship (yes or no), and loneliness. Loneliness was assessed using an item from the 10-item Center for Epidemiological Studies Short Depression Scale (CES-D-10) (Andresen et al., 1994), which asked participants how many days in a week they felt lonely: all of the time (5–7 days); occasionally (3–4 days); some of the time (1–2 days); or rarely or never (<1 day).
Analyses
We utilized Pearson chi-square tests and the CLSA’s trimmed weights to test for associations between categorical variables in descriptive analyses. We then employed multivariable logistic regression to assess the association between functional social support and executive function, controlling for the covariates described above. The regression analyses were weighted by the CLSA’s analytic weights. Information on the calculation of weights in the CLSA can be found in the CLSA’s sampling documentation (CLSA, 2023).
Regression analyses were run separately for overall social support and each subtype of support. We ran two regression models for each of the five forms of support: (1) a base model regressing executive function on the form of support in question that accounted for key sociodemographic variables and (2) an adjusted model containing all sociodemographic, health, and social covariates.
Model fit for all final models was assessed using the Mann-Whitney U statistic for the area under the receiver operating characteristic curve. All models had good fit: Area = 0.81, 95% Wald Confidence Limits = 0.80–0.81 (all models). We checked for multicollinearity with a variance inflation factor (VIF) threshold score >10 (Kleinbaum et al., 2014) and did not find any issues.
Ethics Approval
This research received ethics approval from the University of Waterloo’s Office of Research Ethics (file #41682).
Results
Distribution of Low Functional Social Support by Low Executive Function Status, Canadian Longitudinal Study on Aging, Weighted, n = 2,940,843. a
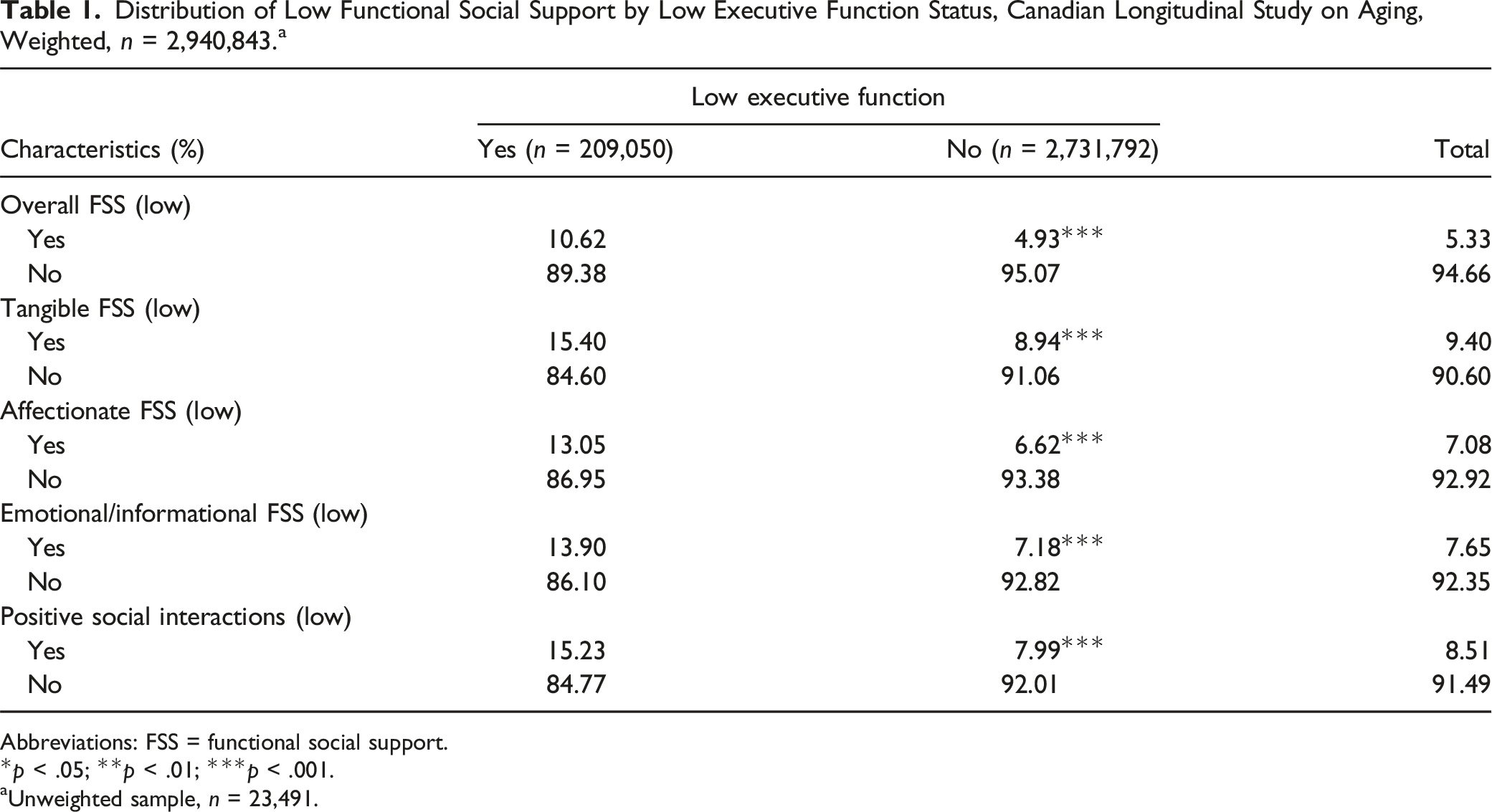
Abbreviations: FSS = functional social support.
*p < .05; **p < .01; ***p < .001.
aUnweighted sample, n = 23,491.
Distribution of Sociodemographic Covariates by Low Executive Function, Canadian Longitudinal Study on Aging, Weighted, n = 2,940,843. a
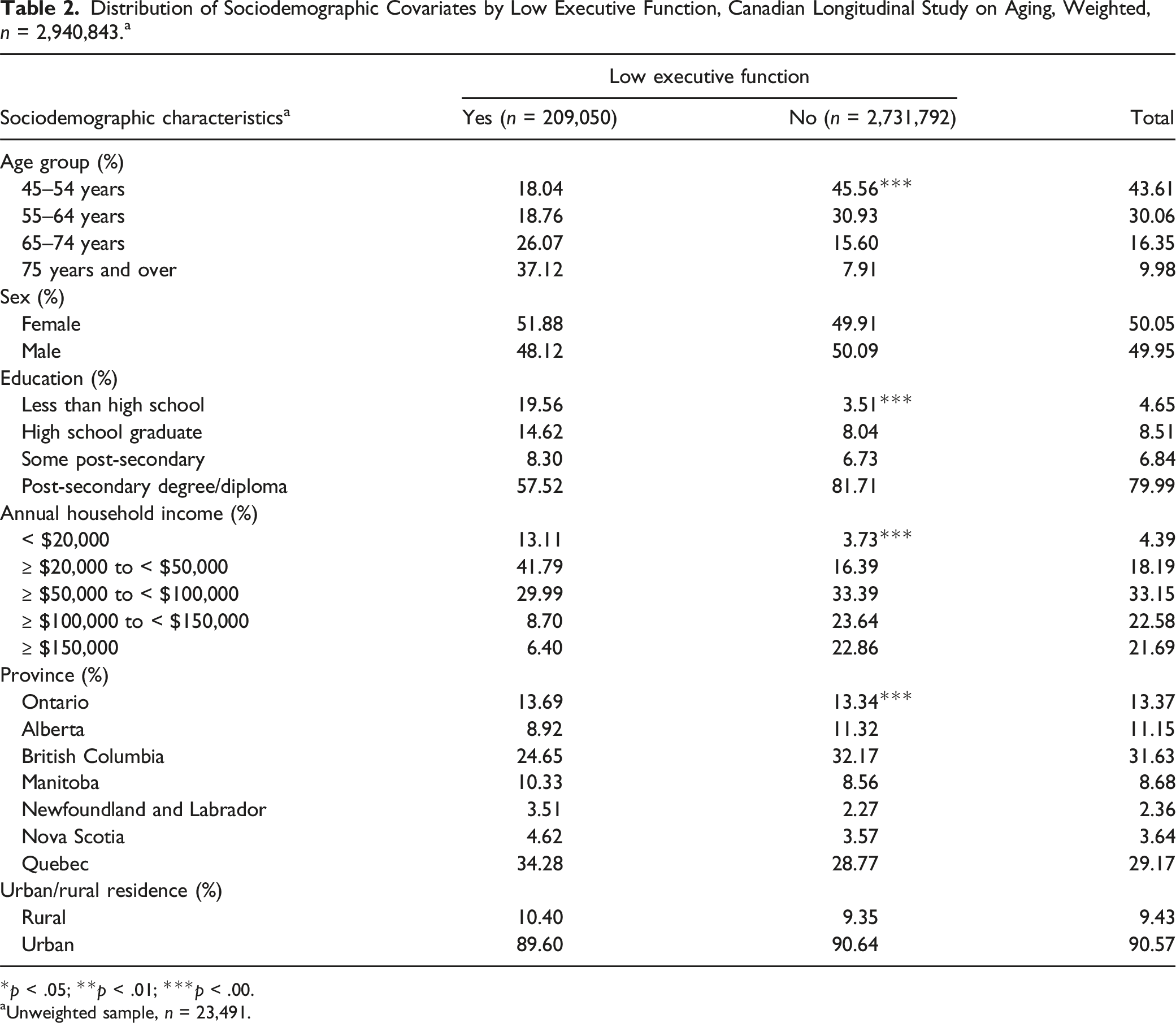
*p < .05; **p < .01; ***p < .00.
aUnweighted sample, n = 23,491.
Distribution of Health and Social Covariates by Low Executive Function, Canadian Longitudinal Study on Aging, Weighted, n = 2,940,843. a
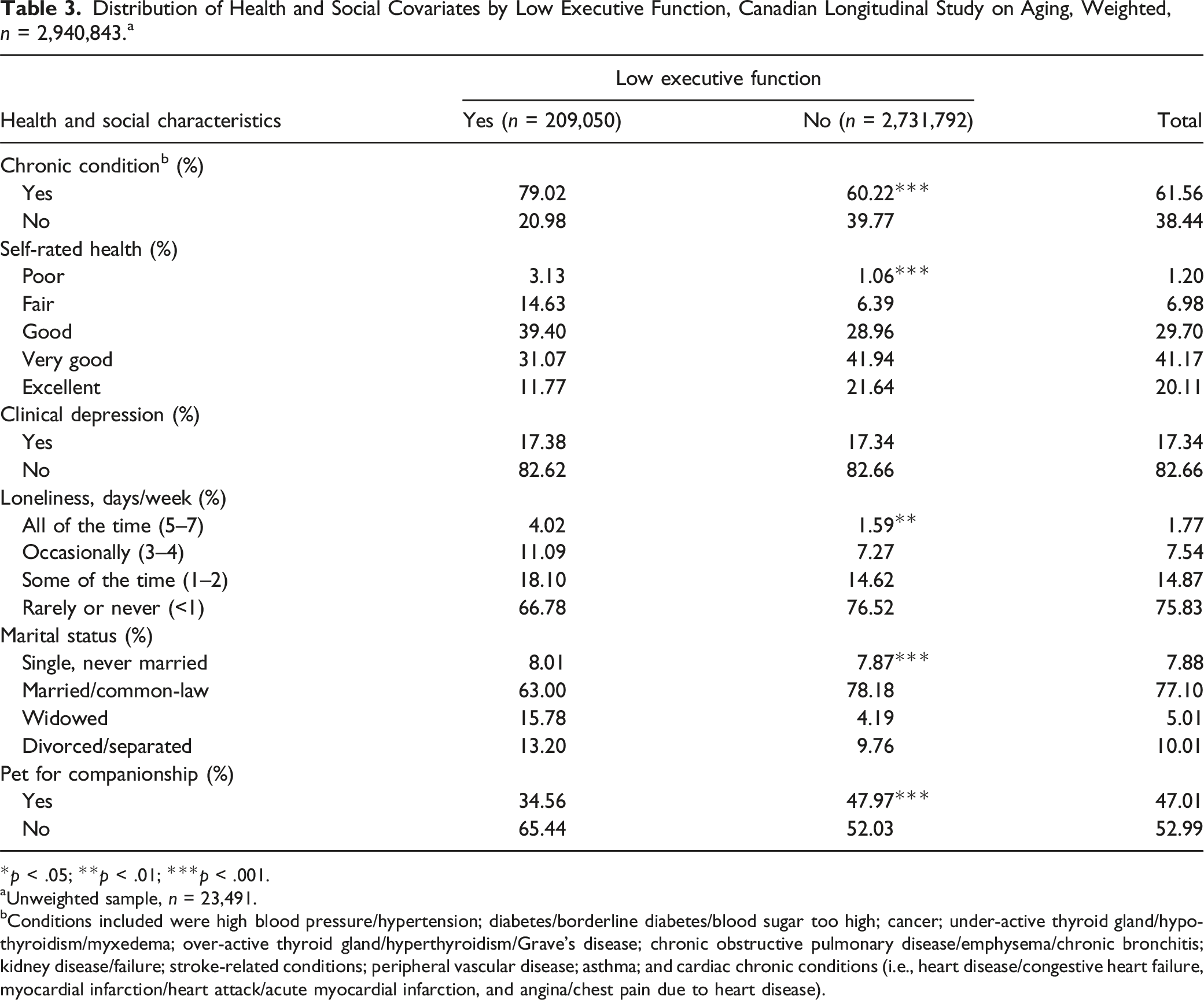
*p < .05; **p < .01; ***p < .001.
aUnweighted sample, n = 23,491.
bConditions included were high blood pressure/hypertension; diabetes/borderline diabetes/blood sugar too high; cancer; under-active thyroid gland/hypothyroidism/myxedema; over-active thyroid gland/hyperthyroidism/Grave’s disease; chronic obstructive pulmonary disease/emphysema/chronic bronchitis; kidney disease/failure; stroke-related conditions; peripheral vascular disease; asthma; and cardiac chronic conditions (i.e., heart disease/congestive heart failure, myocardial infarction/heart attack/acute myocardial infarction, and angina/chest pain due to heart disease).
Objective 1: Overall Social Support and Executive Function
Summary of the Association Between Low Functional Social Support (Overall and Subtypes) and Low Executive Function, Canadian Longitudinal Study on Aging, Weighted, n = 2,940,843. a
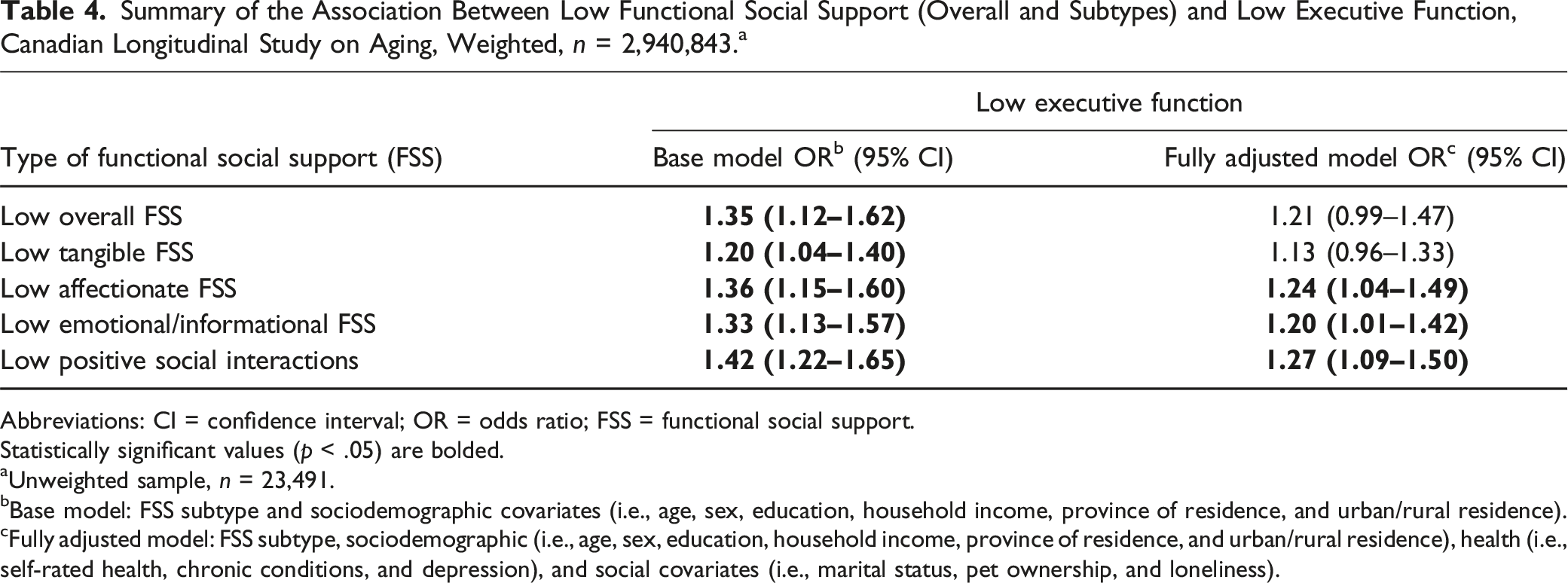
Abbreviations: CI = confidence interval; OR = odds ratio; FSS = functional social support.
Statistically significant values (p < .05) are bolded.
aUnweighted sample, n = 23,491.
bBase model: FSS subtype and sociodemographic covariates (i.e., age, sex, education, household income, province of residence, and urban/rural residence).
cFully adjusted model: FSS subtype, sociodemographic (i.e., age, sex, education, household income, province of residence, and urban/rural residence), health (i.e., self-rated health, chronic conditions, and depression), and social covariates (i.e., marital status, pet ownership, and loneliness).
Objective 2: Subtypes of Social Support and Executive Function
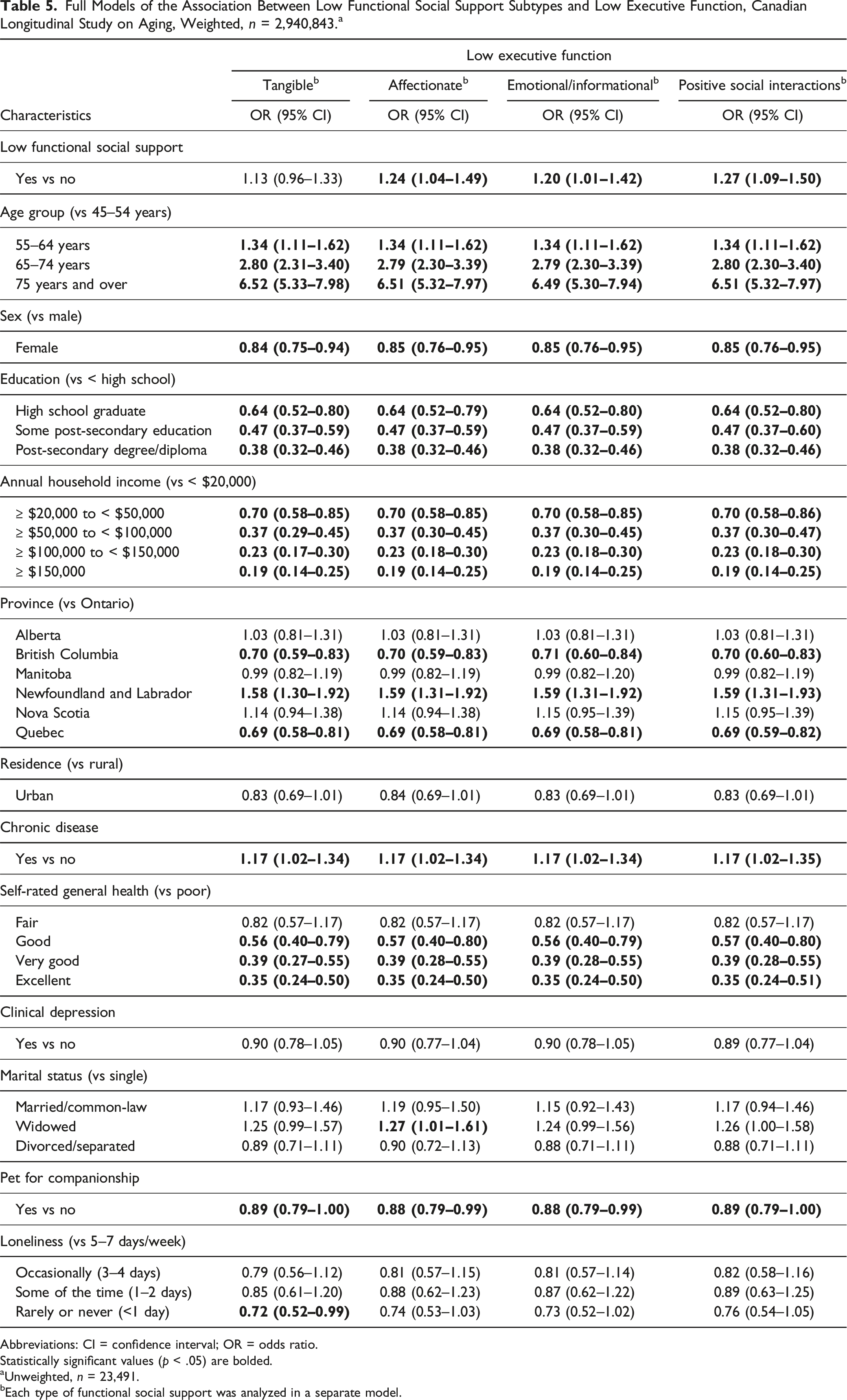
Of the three subtypes of functional social support that remained significantly associated with low executive function in the fully adjusted models, individuals reporting low affectionate support (e.g., having someone who shows you love and affection) had 24% greater odds of having low executive function compared to those with higher levels of support (OR = 1.24, 95% CI = 1.04–1.49). This was similar in magnitude to individuals with low emotional/informational support (e.g., having someone to confide in or talk to about yourself or your problems) and low positive social interactions (e.g., someone to have a good time with), who had 20% (OR = 1.20, 95% CI = 1.01–1.42) and 27% (OR = 1.27, 95% CI = 1.09–1.50) greater odds of having low executive function, respectively.
Full Models of the Association Between Low Functional Social Support Subtypes and Low Executive Function, Canadian Longitudinal Study on Aging, Weighted, n = 2,940,843. a
Abbreviations: CI = confidence interval; OR = odds ratio.
Statistically significant values (p < .05) are bolded.
aUnweighted, n = 23,491.
bEach type of functional social support was analyzed in a separate model.
Discussion
This study investigated whether functional social support was associated with executive function in a community-dwelling sample of middle-aged and older adults. All subtypes of functional social support were positively associated with executive function. After controlling for sociodemographic, health, and social covariates, three subtypes—affectionate support, emotional/informational support, and positive social interactions—remained significantly associated with executive function.
The significant associations of emotional/informational support and positive social interactions with executive function are consistent with previous research showing a positive association between broadly conceptualized emotional support (Ellwardt et al., 2013; Seeman et al., 2001) and friendship (Hughes et al., 2008) on cognitive function. Further, previous research utilizing the MOS-SSS in older adults also identified emotional/informational support and positive social interactions as being significantly associated with cognitive domains other than executive function: visuospatial, language, attention, and memory domains of cognitive function (Pillemer & Holtzer, 2016). These findings support the stress-buffering hypothesis, with the subtypes of social support that are significantly associated with cognition representing positive emotional connections (i.e., emotional/informational support and positive social interactions). Access to these social resources may reduce stressful experiences and lessen detrimental physiological reactions during times of adversity, with the effects theoretically building across the lifespan. Low tangible support and overall social support were positively associated with low executive function, although these associations became nonsignificant after the inclusion of health and social covariates. In terms of overall support, Pillemer and Holtzer (2016) also found that higher levels of overall social support were significantly associated with better general cognitive function in cross-sectional analyses.
Study design and differing operationalizations of social support and cognition may help explain variations across studies in the published literature. For example, our final models—in which the association of overall and tangible functional social support with executive function became nonsignificant—controlled for social covariates (i.e., marital status, loneliness, and pet companionship) that were not included in most other analyses (Pillemer & Holtzer, 2016), which may help to explain why we found nonsignificant results. To address highly skewed data on social support and cognitive function, this study dichotomized social support and executive function, compared to other studies that used continuous scores of social support or cognition (Pillemer & Holtzer, 2016). Supported by previous literature, a cut-off of 1.5 SDs below the mean was selected versus a stricter definition of low cognitive function (e.g., 2 SDs below the mean) so that we would include those with early, milder cognitive decline (Petersen et al., 1997; Sachdev et al., 2014). An additional potential explanation for inconsistent results is variation in cognitive outcomes. Pillemer and Holtzer (2016), for example, assessed cognitive function in the visuospatial, language, attention, and memory domains in contrast to our focus on executive function, which may suggest that the association between social support and cognitive function differs across cognitive domains. Executive function, a key domain of cognitive function, was selected for this study given its key role in attention, planning, adapting to change, completing goals, and problem solving (Alvarez & Emory, 2006; Diamond, 2013).
This study contributes to the social support literature by supplementing past research completed on smaller and more highly selected samples. We conducted a robust set of analyses on a large, community-based sample of middle-aged and older adults to investigate the association between subtypes of functional social support and an aggregate measure of executive function, while accounting for a broad range of potential sociodemographic, health, and social covariates. However, at the time of analyses, only cross-sectional, baseline data were available from the CLSA, and we cannot infer temporality.
Generalizability of results may also be limited by selection bias. Participants in the CLSA’s Comprehensive cohort were actively recruited from within 25–50 km of 11 data collection sites and are more likely to be white, heterosexual, better educated, and wealthier than the general Canadian population. The high level of social support reported by this group may not reflect the average experience of older adults living in the community. In addition, the CLSA was limited to generally cognitively healthy adults, which minimized the number and severity of cases of low executive function. This combination of recruitment and volunteer biases likely produced a bias to the null in the described findings, reducing the magnitude of our odds ratios and making the association between functional social support and executive function appear smaller than what would be found in the target population.
The findings of this study indicate the potential benefits of social interventions for supporting executive function in mid- to late-life. Many of the current social programs available to the public focus on tangible forms of support, such as meal support, which, while serving a necessary purpose, may be insufficient for supporting cognitive function. Given the importance of positive social interactions and emotional connection, increasing social programs focusing on these forms of support in addition to tangible resources may be an additional way to support the cognitive health of middle-aged and older adults in the community. These programs could be aimed at increasing both access to shared spaces and community programming that fosters friendship building and opportunities for group enjoyment. Future research aimed at investigating the association between social support and cognitive function could build upon this study by further considering the impact of identified social factors (e.g., gender, marital status, and loneliness), the intersections of functional and structural support, and the longitudinal impacts of social support on cognitive health over time.
Conclusion
A better understanding of the relationship between social support and cognitive function is essential for guiding public health policies and future research directed at helping adults maintain their independence and adapt to change. The results of this study demonstrate that, despite many of our current programs focusing on tangible support, other subtypes of functional social support are also associated with low executive function. Future programs aimed at supporting cognitive health in adults in mid- to late-life may be further bolstered by focusing on increasing opportunities for positive social interactions, emotional/informational support, and affectionate support and identifying the forms of social support most appropriate for different subsets of the population.
Supplemental Material
Supplemental Material - Functional Social Support Subtypes Are Associated With Executive Function in Middle-Aged and Older Adults: Findings From the Baseline Comprehensive Cohort of the Canadian Longitudinal Study on Aging
Supplemental Material for Functional Social Support Subtypes Are Associated With Executive Function in Middle-Aged and Older Adults: Findings From the Baseline Comprehensive Cohort of the Canadian Longitudinal Study on Aging by Emily C. Rutter, Mark Oremus, Colleen J. Maxwell, and Suzanne L. Tyas in Journal of Aging and Health.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Velux Stiftung Project [No. 1190].
Ethical Statement
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.