
Abstract
Objectives
This study examines whether the association between caregiving demands and mental health is non-linear and also, whether this non-linear association is contingent on the marital status of the caregiver.
Methods
We analyze the data from the Canadian Longitudinal Study on Aging, applying OLS regression and quadratic interaction terms.
Results
A lower level of demands is salubriously associated with symptoms of depression and life satisfaction, but this association becomes deleterious at higher levels of demands. Moreover, a connection to a marital partner extends the benefits of caregiving demands and stems the adverse consequences.
Discussion
This research shows that acts of caregiving may not themselves be detrimental. Instead, the degree and way in which caregiving relates to mental health may vary by both the extent of the demands of the caregiving role and familial relationships in which caregivers are embedded.
Keywords
Research evidence reveals a consensus that occupying a caregiving role has important implications for the mental health of caregivers
In this paper, we reconsider whether and how caregiving demands are related to the mental health of caregivers. We re-frame the association between caregiving demands and mental health in two ways. First, we integrate a “caregiving rewards” perspective (Lee, Bierman, & Penning, 2020Lee et al., 2020), which serves to underscore how a caregiver’s engagement in the tasks of care may also carry mental health benefits in addition to stresses. We suggest that the dual stresses and benefits associated with caregiving demands can best be illustrated by modeling a non-linear association between caregiving demands and mental health. Accordingly, the benefits are seen as predominating at low levels of demands whereas the stresses of caregiving predominate and create a deleterious association at high levels of demands. Prior research has generally not taken the possibility of this non-linearity into account. Second, we integrate sociological insights on stress and mental health encapsulated in a stress process perspective (Pearlin, 1999). In particular, insights regarding a marital partner as a primary source of social support and integration suggest that their presence may weaken the stressful aspects of caregiving demands and strengthen the positive aspects (Bierman, 2014), leading to different forms of this non-linear association among married and non-married caregivers.
To assess empirical support for these arguments, we analyze the first wave of a large national survey of adults aged 45 and over from the Canadian Longitudinal Study on Aging (CLSA). In examining both negative (symptoms of depression) and positive (life satisfaction) mental health outcomes, we find a similar non-linear association with caregiving demands: there are initial benefits of demands that become deleterious as demands increase. Moreover, for married as compared to non-married caregivers, the benefits of these demands extend across a greater number of demands, with weaker adverse associations.
This research contributes to the body of knowledge on caregiving and mental health by showing that acts of caregiving may not themselves be detrimental. Instead, the degree and way in which caregiving relates to mental health may vary in accordance with both the extent of the demands of the caregiving role and the type of familial relationships in which caregivers are embedded.
Background
Caregiving demands have typically been examined from a stress of caregiving perspective (Pearlin et al, 1990). A stress of caregiving perspective typically views caregiving as a “model of chronic stress” (Whittaker & Gallagher, 2019, p. 93), with multiple chronic stressors incumbent in this role (Swinkels et al., 2019). Care demands, stemming directly from the needs of the care recipient, serve as primary objective stressors that drive the stress process, including exposure to subsequent stressors and their outcomes (Pearlin et al., 1990). This process is known as “stress proliferation,” with the result that the potent negative effects of caregiving demands can extend in part from the subsequent stressors that are the consequence of these demands (Pearlin & Bierman, 2013). These consequent stressors can include interference, such as having less time for self or others, as well as additional strains, such as economic strains, and burnout from exhaustion (Lin et al., 2012). These secondary stressors are in turn likely to be more prevalent as a result of more extensive caregiving demands, with greater demands then presenting a more overwhelming role for the caregiver.
Yet, caregiving demands may paradoxically also elicit multiple benefits. As framed by a rewards of caregiving perspective (Lee et al., 2020), there are “rewards resulting from the caregiving relationship” (Walker, Powers, & Bisconti, 2016, p. 357). Critically, caregiving can provide caregivers with a sense of meaning and purpose (Noonan & Tennstedt, 1997), and may especially instill a sense that the caregiver “matters” to another (Tabler & Geist, 2021). Additionally, assisting in various demands can also bolster the caregiver’s sense of competence and mastery (Lloyd et al., 2016). This may also lead to a sense of being useful to others, which is a further positive influence for older adults (Gruenewald et al., 2007). Many of these attributes have been shown to have mental health benefits (Mirowsky & Ross, 2003; Taylor & Turner, 2001), and the positive aspects of caregiving have in turn been shown to be positively associated with mental health (Quinn & Toms, 2019). Along similar lines, the healthy caregiver hypothesis proposes that not only are those who are healthier more likely to become caregivers and remain in that role, but that the caregiving role also keeps caregivers healthier (Fredman et al., 2009). These effects can occur because providing recipients with care requires a higher level of physical and cognitive activity that preserve a caregiver’s well-being (Bertrand et al., 2012). Although supportive, the evidence to date is primarily from studies evaluating the cognitive and physical functioning (Bertrand et al., 2012), and mortality (Fredman et al., 2009) of caregivers.
We argue that both of these perspectives have relevance to an understanding of the association between caregiving demands and caregiver mental health. Essentially, the balance of these rewards and costs will vary depending on the degree of demands. Engagement with a limited set of tasks may result in better mental health outcomes than little or no caregiving because the positive aspects of caregiving will tend to be predominant when a low level of tasks is required of the caregiver. Conversely, as the level of tasks increases, greater role captivity and role overload will tend to occur. Both of these often will not only create stress but also negate some or all of the benefits of caregiving. Feeling overwhelmed and trapped in the caregiving role may well reduce a sense of efficacy and the degree of satisfaction the caregiver obtains from helping the care recipient. We also acknowledge that some research suggests that, under conditions of high caregiver demands, different types of caregiving experiences may occur, with some caregivers reporting high levels of stressors and other reporting high levels of both stressors and rewards (e.g., Pristavec, 2019; Sung et al., 2021). However, the pernicious and potent consequences of mounting stressor are likely to negate the mental health benefits of any potential caregiving rewards. The net will be a consequent non-linear association between caregiving demands and mental health, in which a positive association at a low number of demands turns negative at higher levels of demands.
The possibility of a non-linear association between caregiving demands and mental health is especially notable in light of previous research findings on this association. Although earlier research suggested that shifting into more burdensome demands is detrimentally associated with caregiver mental health (Burton et al., 2003), subsequent research has repeatedly documented a non-significant association between caregiving demands and mental health when caregiving demands assess the degree to which the caregiver needs to assist in activities of daily living (ADL) and/or instrumental activities of daily living (IADL) (Fekete et al., 2017; Pioli, 2010). However, a positive association at the low end of demands could counter the negative association found at higher levels of demands, with the result that there may be little evidence of an association if this non-linearity is not taken into account. Consequently, the current research gives greater attention to the complexities in this association through attention to non-linearity, and especially the potential benefits of the demands of care that are incumbent in the caregiving role.
Marital/Partner Status as Moderator
A view of caregiving demands as a stressor also elicits a second important way in which the mental health consequences of demands may not be unitary across caregivers. A sociological perspective on stress and mental health encapsulated in a stress process perspective suggests that social statuses fundamentally structure the effects of stress exposure on mental health (Pearlin, 1999). Moreover, research in the sociology of mental health underscores that one of the most pivotal social statuses for mental health is that of marital status, with the married consistently reporting better mental health across a number of outcomes than the unmarried (Umberson et al., 2013). This pattern is also evident among caregivers specifically (van den Berg, Fiebig & Hall, 2014). Based on findings showing that marriage is protective of mental health, it has been argued that stress exposure in later life presents a form of “double-jeopardy” for the non-married, as stress in and of itself is a threat to mental health, but then the mental health threat posed by the stressor is stronger for the non-married (Bierman, 2014).
There are a number of reasons why the non-married may be more vulnerable to the negative mental health effects of chronic stress exposure in later life, and especially to the stresses posed by multiple caregiving demands. Although the social support function of marital status is commonly acknowledged (Umberson et al., 1996), from a sociological perspective, the presence of a marital partner plays a much more extensive role through its integratory function (Kyung-Sook, SangSoo, Sangjin, & Young-Jeon, 2018). A marital partner acts a main factor in health surveillance and influence on salubrious health behaviors (Umberson, 1987), as well as in staving off loneliness (Child & Lawton, 2019), which can further shape beneficial health behaviors (Kobayashi & Steptoe, 2018). Moreover, the presence of a marital relationship provides a sense that an individual matters to others (Bonhag & Froese, 2021), and the validation of basic worth to others can also reinforce mental health even in the presence of stressful experiences. The presence of a marital partner is also a key resource for a sense of control over life (Bierman, Fazio, & Milkie, 2006), and a stronger sense of control can help individuals to see multiple caregiving demands as less overwhelming (Mirowsky & Ross, 2003), as well as activate problem-focused coping efforts to address the demands of caregiving (Ben-Zur, 2002). Thus, even when multiple caregiving demands strain the functioning of the individual, the marital relationship provides a proximal arena of social care in which individuals are likely to be better protected from these deleterious effects (Bierman, 2009).
These arguments are supported by evidence showing that the presence of a marital partner can weaken the association between chronic stress and mental health (Caputo & Simon, 2013). We therefore suggest that the shape of the non-linear association between caregiving demands and mental health will be differentiated based on whether or not a caregiver has a marital partner. More specifically, we expect that a relationship with a marital partner will extend the mental health benefits of caregiving demands across a greater level of demands and weaken the adverse associations with mental health at a higher level of demands.
Methods
Data
This study draws on the Canadian Longitudinal Study on Aging (CLSA). The CLSA baseline sample includes 51,338 respondents aged 45–85 years and the survey combines data obtained from two sub-surveys—a tracking cohort survey and a comprehensive cohort survey. Tracking cohort respondents (N = 21,241) were randomly selected within age/sex strata for each province and were interviewed by telephone. They were recruited in three ways: (a) from a previous large-scale social survey, (b) through mail-outs from provincial health ministries, and (c) by means of random-digit dialing. Comprehensive cohort respondents (N=30,097) were also randomly selected based on age/sex strata, but all strata were between 25 and 50 km of one of 11 data collection sites across the country. Comprehensive cohort respondents received an in-home interview with questions similar to those administered to tracking cohort respondents. The surveys collected information between 2010 and 2015. The participation rate into the CLSA was about 45% with an overall response rate of 10% (Raina et al., 2019). Further information about the surveys can be found in Kirkland et al. (2015) and Raina et al. (2009). Because the measures used in this study were present in both the tracking and comprehensive components, the two subsamples are combined in all analyses. Multiple regression models control for survey cohort membership to account for differences that may reflect survey type.
Focal Measures
Mental Health Outcomes
Previous research using the CLSA demonstrates that stressful caregiving experiences may have distinct repercussions for negative and positive psychological states (Lee et al., 2020). In keeping with this research, we examined symptoms of depression as a negative mental health outcome and life satisfaction as a positive mental health outcome. Symptoms of depression were measured using a 10-item version of the Center for Epidemiologic Studies-Depression scale (CES-D) that has been validated for use with older adults (Andresen et al., 1994). The five-item Satisfaction with Life Scale (Diener et al., 1985), also validated for use with older adults (von Humboldt & Leal, 2017), was used to measure life satisfaction, with all responses coded so that higher values indicate more frequent symptoms of depression or greater life satisfaction, respectively.
Caregiving Demands
Caregiving demands were measured using a checklist of six common caregiving tasks that respondents reported having provided to family members, friends, or others inside and outside the household during the past 12 months: personal care such as assistance with eating/dressing/bathing/toileting; medical care such as help with taking medicine/nursing care; managing care such as making appointments; help with activities such as housework/home maintenance/outdoor work; transportation; and help with meal preparation or delivery. The number of tasks provided represented caregiving demands, with non-caregivers or individuals who did not endorse any of these items coded as 0.
Marital Status
Common-law marriage is increasingly prevalent among Canadian older adults (Mitchell, 2021). Canadian Longitudinal Study on Aging’ss measure of marital status included both married and common-law unions in one category. Consequently, marital status was coded in this study as 0 = non-married, 1 = married/living with a partner in a common-law relationship.
Control Measures
Study Descriptives.
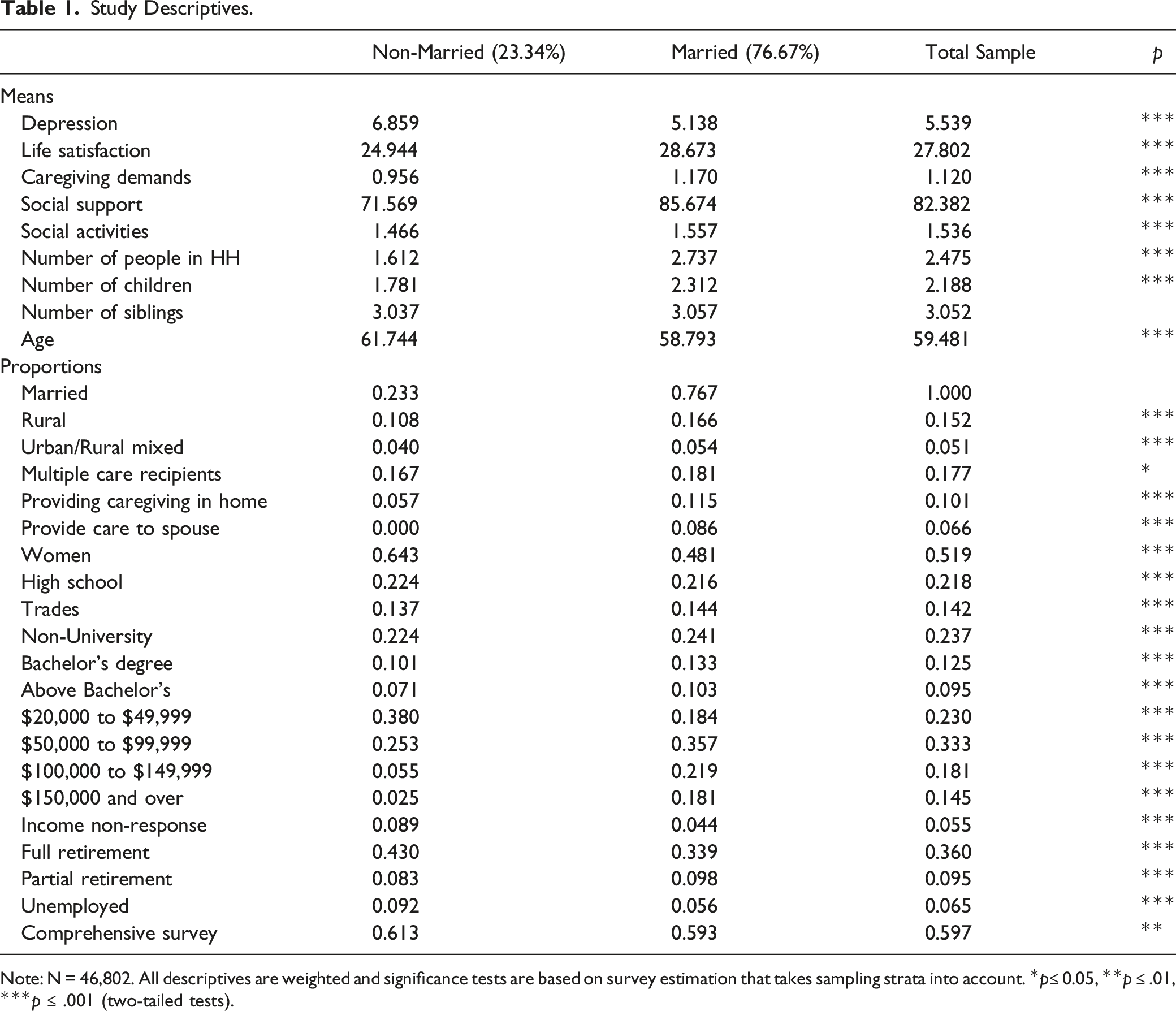
Note: N = 46,802. All descriptives are weighted and significance tests are based on survey estimation that takes sampling strata into account. *p≤ 0.05, **p ≤ .01, ***p ≤ .001 (two-tailed tests).
Plan of Analysis
Mental health outcomes are analyzed using ordinary least squares regression. Each outcome is examined using a set of four models. We first examine the association between caregiving demands and the outcome using a linear specification, and then in a second model add a squared term for demands, which serves to show if there is a non-linear association between demands and the outcome by estimating a quadratic association. Both models (Models 1 and 2) also include the control variables. Interpretation of a quadratic association is not straightforward because the slope for a predictor and outcome is constantly changing across levels of the predictor. To aid their interpretation, we employ figures to illustrate these associations, but we also estimate sets of “instantaneous rates of change.” The instantaneous rate of change shows how outcomes change as a predictor increases a very slight amount (McClendon, 2002), and can therefore generally be understood as the association between caregiving demands and mental health at a specific point in the predictor. We estimate the instantaneous rate of change across levels of caregiving demands, thereby specifying how the association between caregiving demands and mental health changes between low and high levels of demands.
We next test whether these associations differ by marital status with two additional models (Models 3 and 4). Model 3 tests an interaction between marital status and the linear term for caregiving demands, which serves to show whether care demands are associated with mental health differently between the married and non-married. Model 4 then adds an additional interaction between marital status and the squared term for caregiving demands, which shows whether the curvature in these associations differs significantly between the married and non-married. In ancillary analyses, we also tested these interactions in models that removed individuals who were providing care to a marital partner: the results were substantively the same as those presented here, suggesting that moderation by marital status is not due to the role of a marital partner as a care recipient.
All analyses are conducted using Stata 16.1. Analyses are weighted for nationally representative estimates using the CLSA sample weights version 1.2. Variance estimation takes sampling strata into account using Stata’s survey-setting and survey-estimation commands. We excluded respondents who became recently bereaved caregivers (i.e., those who provided care in the past 12 months, but care receiver is now deceased) because the measure of mental health outcomes is based on present status (i.e., in the past week). Deletion of recently bereaved caregivers reduced the sample size to 50,037, and listwise deletion further reduced it to 46,802 respondents. As missing responses reduced the sample by less than 8%, bias due to listwise deletion could be considered minimal.
Results
Caregiving Demands and Depression
Association Between Caregiving Demands and Symptoms of Depression.
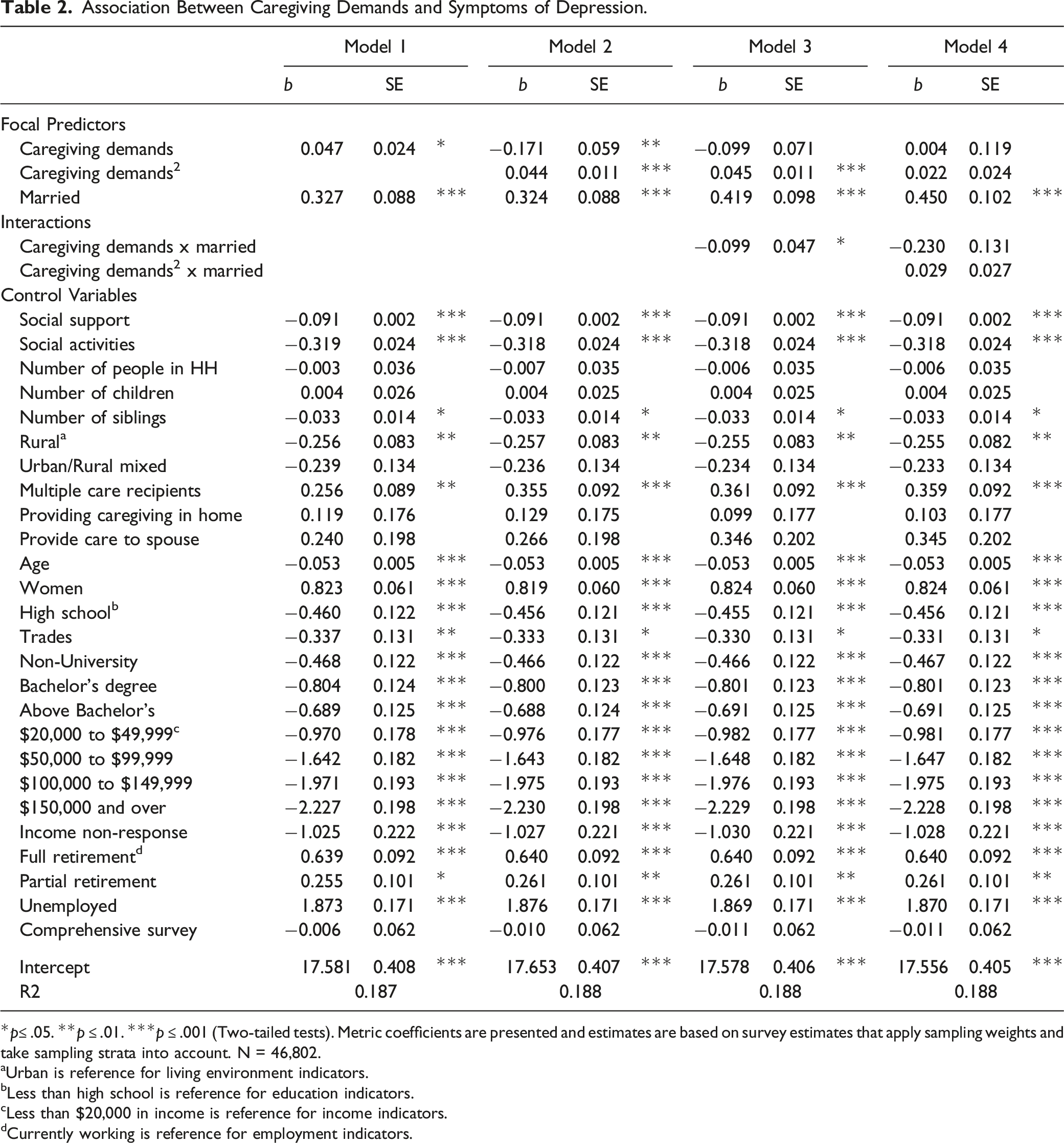
*p≤ .05. **p ≤ .01. ***p ≤ .001 (Two-tailed tests). Metric coefficients are presented and estimates are based on survey estimates that apply sampling weights and take sampling strata into account. N = 46,802.
aUrban is reference for living environment indicators.
bLess than high school is reference for education indicators.
cLess than $20,000 in income is reference for income indicators.
dCurrently working is reference for employment indicators.
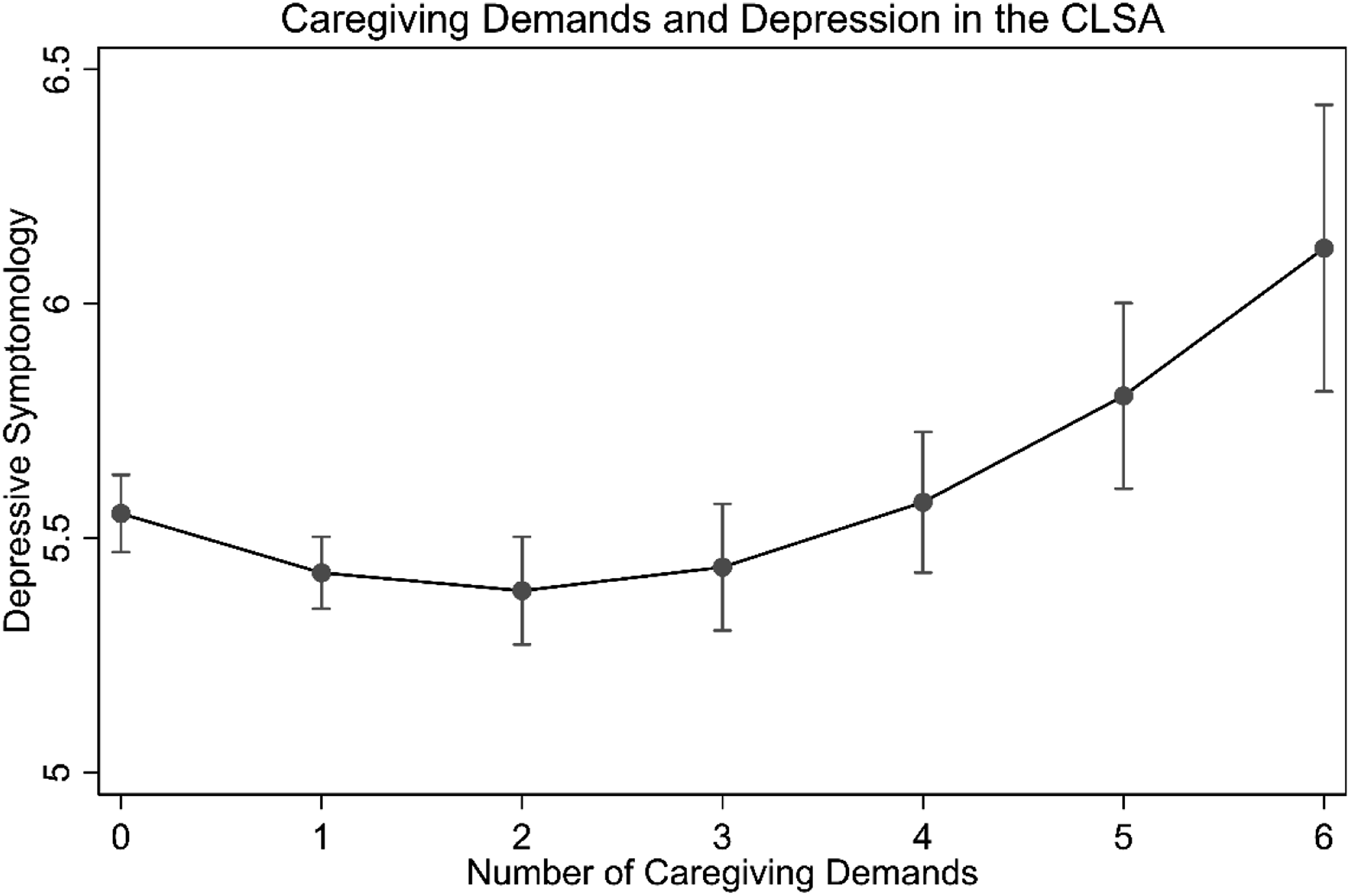
Caregiving Demands and Depression in the CLSA.
It should also be noted that bivariate analyses (not reported here) reveal a negative association between marital status and depression, with married caregivers reporting lower levels of depression than those who were not married. However, this association is positive in the multiple regression models because these models include controls that account for the advantage of the married in depressive symptomology. As the focus of this research is on the association between caregiving demands and mental health, as well how this association differs between the married and non-married, and not differences in mental health between the married and non-married, we do not elaborate on the specific characteristics that explain the advantage of the married in depressive symptomology.
The next set of models test moderation by marital status. In Model 3, we interact marital status with the linear term for caregiving demands, and this interaction is significant. However, Model 4 includes an interaction between the squared term for demands and marital status, and this interaction is not significant. The significant interaction between the linear term for demands but not the squared term indicates that there is a difference between the married and non-married in the degree to which caregiving demands are associated with depressive symptomology, but the curvature in this association does not differ significantly between the married and non-married. Additionally, since the curvature of the association does not differ between the married and non-married, the linear interaction in Model 3 will be identical across values of caregiving demands. The primary difference of interest between the married and non-married is therefore shown in Model 3.
Based on Model 3, Figure 2 illustrates these patterns by plotting the predicted values for depression at different levels of demands separately for the married and non-married. As this figure shows, for the non-married, the association between caregiving demands and depressive symptomology is relatively flat until two demands, after which the number of demands is increasingly associated with greater levels of depression. This pattern is confirmed in tests of the instantaneous rates of change for the non-married, in which the association between demands and depression only becomes significant at three demands (3 demands: b = 0.172; 4 demands: b = 0.263; 5 demands: b = 0.354; 6 demands: b = 0.445; all p <0.001). Conversely, for the married, Figure 2 shows a negative slope at lower levels of demands. Supplementary analyses in fact indicated that instantaneous rates of change at no demands and one demand were significant and negative (b = −0.198 and −0.107, respectively; both p <0.01). The association at two demands was not significant (b = −0.017), with three demands and on showing significant and increasingly adversely associations with depression (3 demands: b = 0.074; 4 demands: b = 0.165; 5 demands: b = 0.255; 6 demands: b = 0.346; 3 demands p < 0.05, 4+ demands p < 0.001). For the non-married, then, we see evidence of the stress of caregiving, but no evidence of the rewards of caregiving. For the married, though, we see evidence of both the rewards and stress of caregiving. Caregiving Demands and Depression in the CLSA by Marital Status.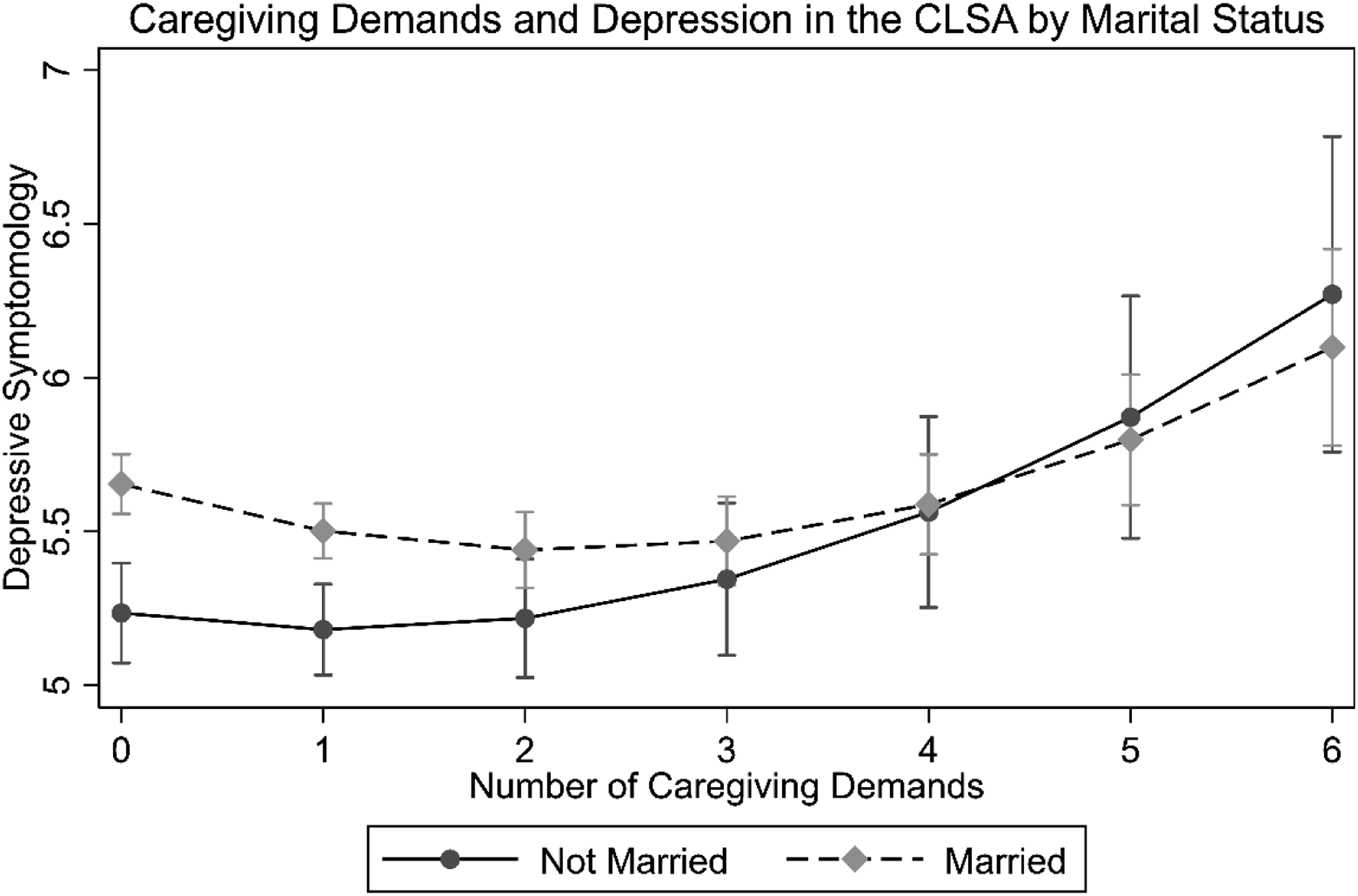
Caregiving Demands and Life Satisfaction
Association Between Caregiving Demands and Life Satisfaction.
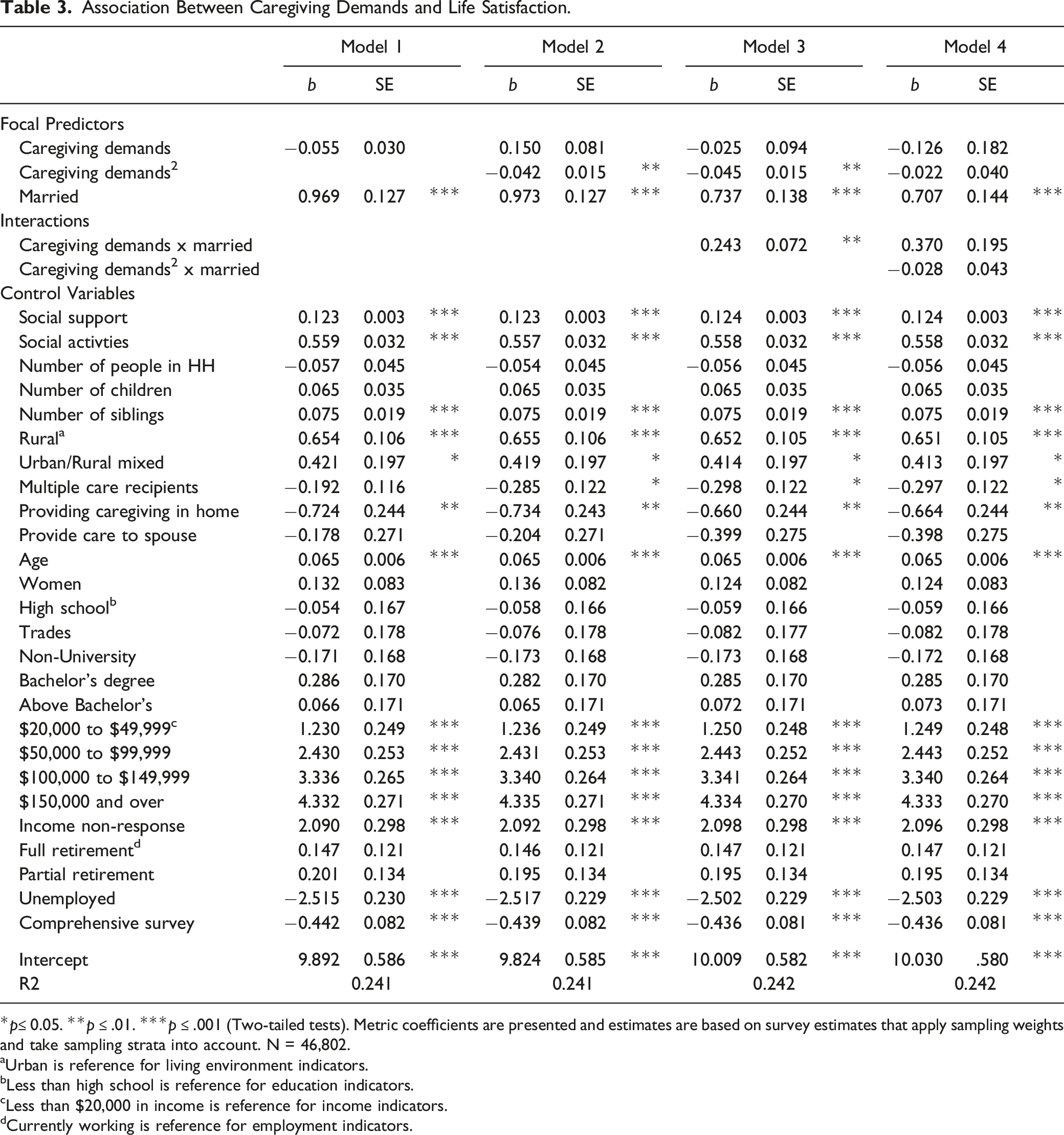
*p≤ 0.05. **p ≤ .01. ***p ≤ .001 (Two-tailed tests). Metric coefficients are presented and estimates are based on survey estimates that apply sampling weights and take sampling strata into account. N = 46,802.
aUrban is reference for living environment indicators.
bLess than high school is reference for education indicators.
cLess than $20,000 in income is reference for income indicators.
dCurrently working is reference for employment indicators.
Figure 3 uses Model 2 to plot the predicted values of life satisfaction at different levels of demands. This figure shows non-significant associations up to two caregiving demands (0 demands: b = 0.150; 1 demands: b = 0.067; 2 demands: −0.016). However, starting at three caregiving demands, we see gradually increasing declines in life satisfaction as the number of demands increases (3 demands: b = −0.100; 4 demands: b = −0.183; 5 demands: b = −0.266; 6 demands: b = −0.350; all p <0.01). These analyses therefore show that, without taking differences by marital status into account, there is little evidence of the rewards of caregiving for life satisfaction, and evidence of the stress of caregiving is observed only at higher levels of care demands. Caregiving Demands and Life Satisfaction in the CLSA.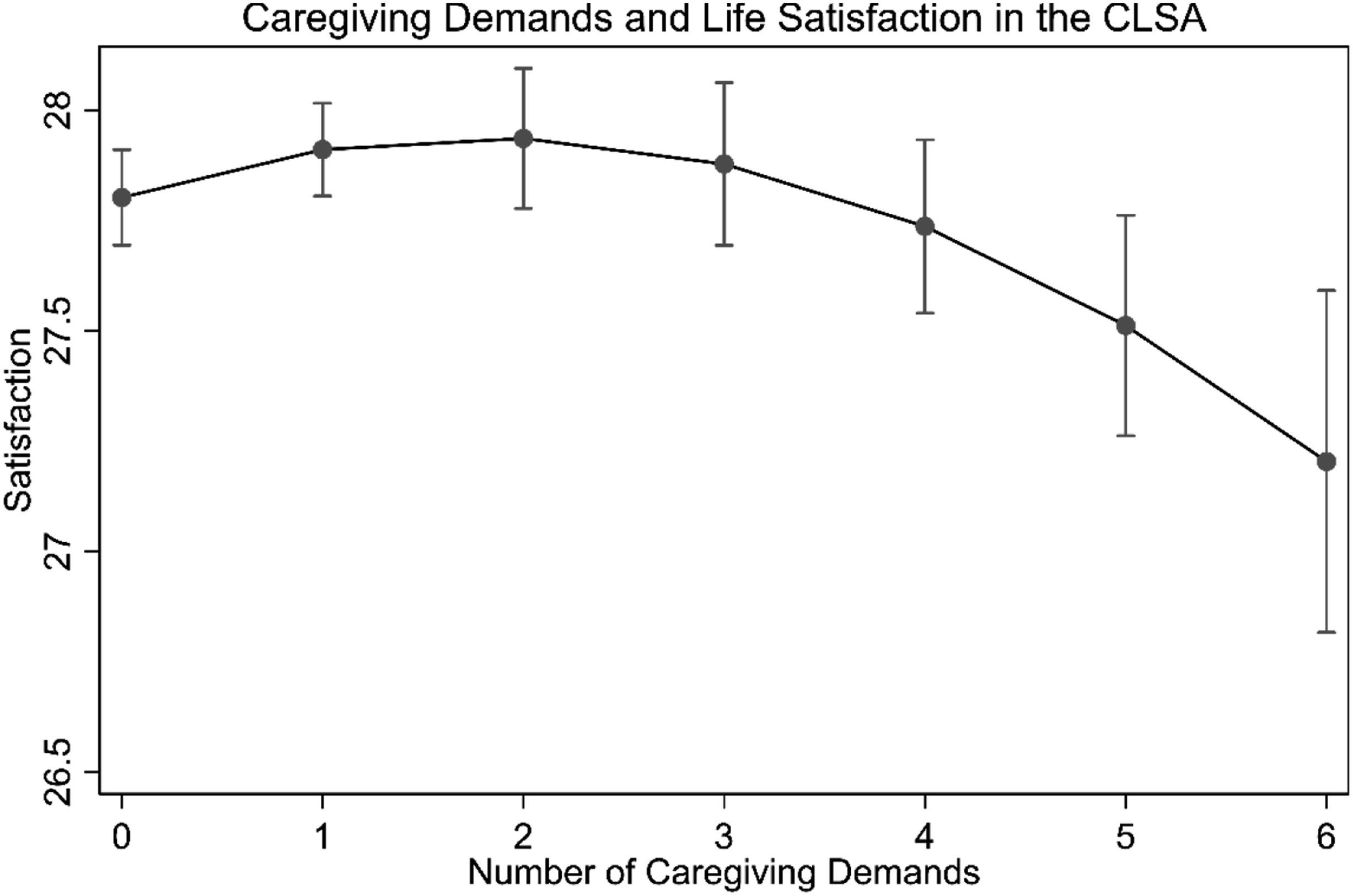
Additionally, while not of focal interest to the paper, it should also be noted that the married show an advantage in life satisfaction even when all controls are included in the models. In bivariate analyses (not reported here), the married also had significantly higher level of life satisfaction. The study covariates do not appear to provide the same explanatory power for the overall difference between the married and non-married in life satisfaction as these covariates do for the difference between the married and non-married in depressive symptomology.
These analyses do not consider the marital context of these associations, though, and this question is examined in the next set of models. Model 3 shows that an interaction between the linear term for caregiving demands and marital status is significant, but Model 4 shows that the inclusion of an additional interaction between the quadratic term for demands and marital status is not significant. Again, then, we observe that the degree to which the number of demands is associated with the outcome differs significantly between the married and non-married, but the degree of curvature in this association does not.
Figure 4 displays the predicted levels of life satisfaction based on Model 3. This model shows a clearer negative slope for the non-married. Ancillary analyses showed that, for the non-married, the instantaneous rates of change were significant at two demands, with this association growing stronger as demands increased, in a demonstration of the increasing stress of demands (2 demands: b = −0.203; 3 demands: b = −0.293; 4 demands: b = −0.382; 5 demands: b = −0.471; 6 demands: b = −0.560; 2 demands p <0.01, 3+ demands p <0.001). Conversely, for the married, there is evidence of a positive association with life satisfaction at lower levels of demands, and then a negative association at higher levels of demands, reflecting the rewards of caregiving at lower levels of caregiving demands and stress of caregiving at higher levels of demands. However, estimation of the instantaneous rates of change showed an important qualification: the association between the number of demands and life satisfaction was significantly associated with less life satisfaction only at a relatively high threshold of four care demands (0 demands: b = 0.217 , p < 0.01; 1 demand: b = 0.128, p < 0.05; 2 demands: b = 0.039, not significant; 3 demands: b = −0.050, not significant; 4 demands: b = −0.139, p < 0.05; 5 demands: b = −0.228, p < 0.01; 6 demands: b = −0.317, p < 0.01). Thus, in addition to providing rewards for life satisfaction specifically for the married, the married were protected from the adverse association between caregiving demands and life satisfaction until a much higher threshold than were the non-married. Caregiving Demands and Life Satisfaction in the CLSA by Marital Status.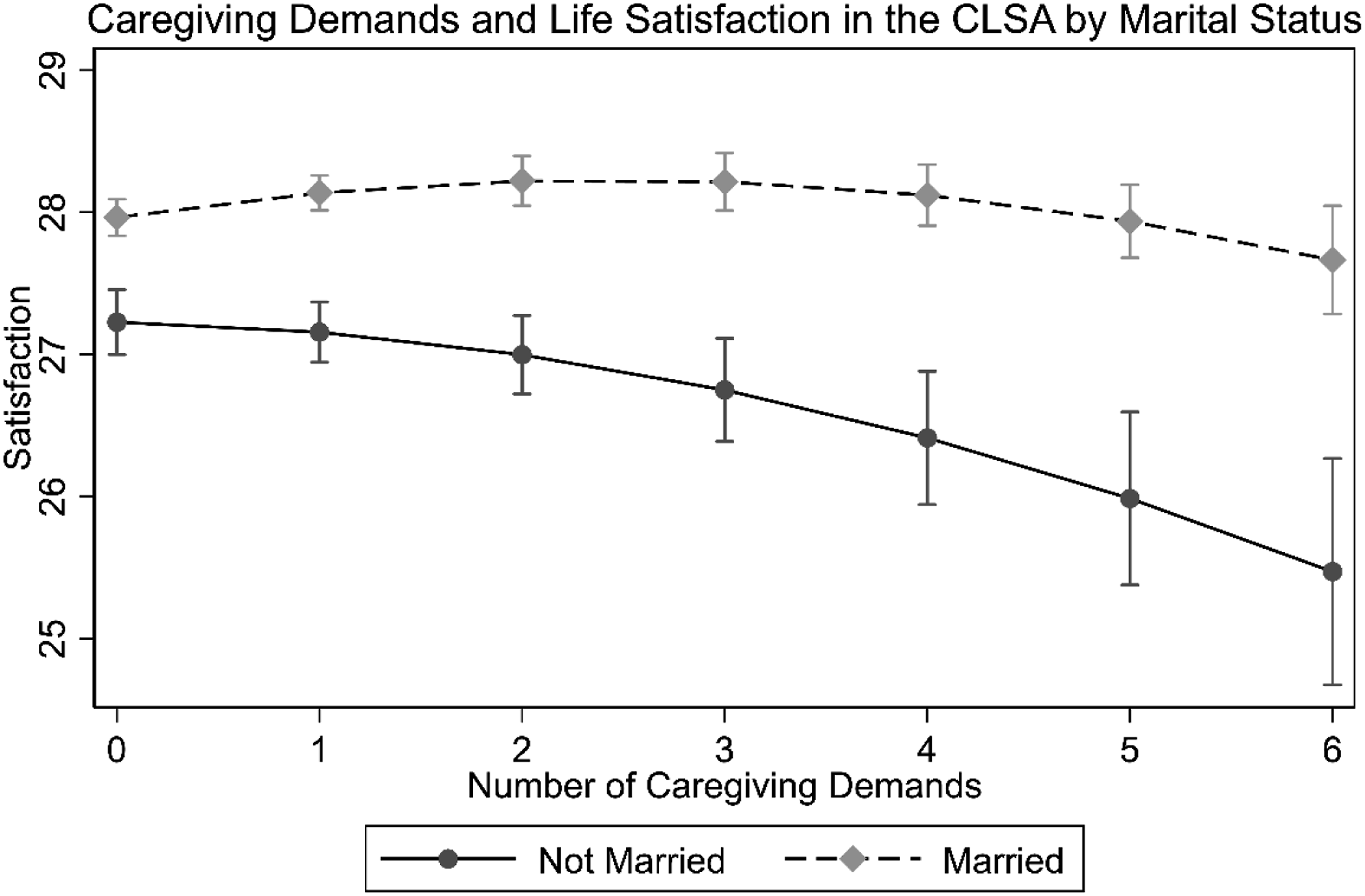
Discussion
Caregiving is often framed in research as a stressful experience (Whittaker & Gallagher, 2019), but some researchers have noted that caregiving can result in a variety of personal rewards (Lloyd et al., 2016; Walker et al., 2016). The results of our research challenge the belief that caregiving must be detrimental to mental health and demonstrate that a greater consideration of the ways that the demands of the caregiving role can be beneficial is warranted. Our findings show that caregiving demands are associated with better mental health at lower levels of demands, and we see that this association is detrimental only at higher levels of demands. Moreover, a connection to a marital partner facilitates the benefits of caregiving demands and can also stem their adverse effects, showing that the assumption of the negativity of caregiving must further be qualified based on the caregiver’s marital relationships.
The primary finding of a non-linear association between caregiving demands and mental health leads to the question of how this association can be explained. We suggest that, for most caregivers, there are both rewards and costs to providing care. What changes is the balance of these costs and rewards. The sense of satisfaction and self-efficacy derived from helping with various tasks likely diminishes as the number of tasks becomes more burdensome. Conversely, as the number of care tasks increases, feelings of captivity and overload may act as stressors that tax mental health and further deplete the remaining rewards of caregiving. As a means of better understanding how the non-linear association between caregiving demands and mental health occurs, then, it is important that future research directly examine both additional stressors and positive rewards as sequalae of caregiving demands.
Our research also emphasizes that the mental health consequences of caregiving demands must be considered in the context of the broader network of social relationships in which caregivers are embedded. Much sociological research emphasizes that a marital partner provides a vital social connection that enhances social integration and support (Umberson et al., 2013). The presence of this partner likely helps to enhance the rewards of caregiving and stave off the experience of additional stressors, leading to our finding of more extensive mental health benefits and weaker negative effects. It is noteworthy that this is the case regardless of whether the partner is the recipient of caregiving as we controlled for this in the analyses, indicating that the protective effects of having a marital partner are not simply due to the care provided as a part of the marital relationship. This finding is also in concert with additional findings showing that marital status modifies the mental health effects of potential stressors (e.g., Bierman, 2009; Caputo & Simon, 2013). We suggest that research on stress in later life should more commonly consider how marital status provides a crucial network context for these stressors. Moreover, for research on caregivers, greater attention should be paid to additional social relationships that may modify the mental health consequences of caregiving demands, such as relationships with siblings and offspring. The greater web of a caregiver’s social relationships may well shape and constrain the adverse effects of a higher number of demands.
Several limitations to this study should be acknowledged. First, this study was cross-sectional in design, and additional longitudinal research could better help establish causal ordering in the association between demands and mental health. Second, some have suggested that the mental health benefits of marital status will vary by gender (Umberson et al., 2013). However, in ancillary analyses, we found that the moderating effects of marital status did not differ by gender. Third, marital quality was not examined in this research. It is also important in future research to consider whether the moderating effects of a marital partner are observed more clearly in higher-quality marriages, or if the presence of a marital partner is sufficient because attachment to a marital partner serves as a source of social integration, over and above the social support function of a marital partner. Fourth, due to their unavailability in the dataset, many other covariates relevant to caregiving contexts and care recipients’ characteristics could not be included in the analyses. Lastly, it should be noted that the sample of the currently study was restricted to those aged 45–85 years and thus, the generalizability of the results to younger/older adults is unclear.
These and other limitations can be addressed in future studies. The use of instruments or scales to assess both the positive and negative experiences of caregiving can validate the current findings. Moreover, a longitudinal study examining how positive aspects of caregiving change over time as well as how relationships between care demands and both aspects of caregiving change over time and influence mental health is warranted. Findings from our study also have several practical implications for policy and practice. Knowing that there is a threshold in caregiving demands when taking care of a loved one transitions from a positive experience into one with negative implications for mental health and well-being, we need to come up with some strategies that make it possible for caregivers to maintain optimal levels of care demands. This could be done either by sharing the care demands with other caregivers or by utilizing formal care services. Also, caregivers without marital partners who might be more vulnerable in terms of experiencing negative outcomes might benefit from added social support and social integration.
In closing, to the best of our knowledge, this study is the first to reveal a non-linear relationship between caregiving demands and mental health outcomes. Our findings imply that mental health benefits of caregiving may be bolstered by maintaining the optimal number of caregiving tasks. This optimal amount can be achieved by sharing the tasks with someone else or using formal care services. This study also suggests that stress-reduction interventions should target caregivers with higher caregiving demands, and especially caregivers with a high level of demands who do not have a marital partner.
Supplemental Material
Supplemental Material - Mental Health Benefits and Detriments of Caregiving Demands: A Nonlinear Association in the Canadian Longitudinal Study on Aging
Supplemental Material for Mental Health Benefits and Detriments of Caregiving Demands: A Nonlinear Association in the Canadian Longitudinal Study on Aging by Alex Bierman, Yeonjung Lee and Margaret J. Penning in Journal of Aging and Health
Footnotes
Acknowledgments
This research was made possible using the data/biospecimens collected by the Canadian Longitudinal Study on Aging (CLSA). Funding for the CLSA is provided by the Government of Canada through the Canadian Institutes of Health Research under grant reference: LSA 94473 and the Canada Foundation for Innovation, as well as the following provinces, Newfoundland, Nova Scotia, Quebec, Ontario, Manitoba, Alberta, and British Columbia. This research has been conducted using the CLSA Baseline Tracking Dataset version 3.4, Baseline Comprehensive Dataset version 4.0, under Application Number 180606. The CLSA is led by Drs. Parminder Raina, Christina Wolfson, and Susan Kirkland.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a Social Sciences and Humanities Research Council of Canada (SSHRC) grant (#430-2018-00437) to Y. Lee.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.