
Abstract
Keywords
As a result of a population aging, with a demographic shift toward a higher proportion of older persons and a lower proportion of working-age individuals, raising the retirement age, in order to compensate for the greater average life expectancy is a probable scenario in several countries (Christensen, Doblhammer, Rau, & Vaupel, 2009). As most individuals spend a significant part of their lives at work, a cause for concern, particularly when working longer, is the potential prolonged exposure to adverse working conditions that might affect health in later life.
Working conditions may contribute to the development of social inequalities in health; there is ample research showing the association between adverse working conditions and poor health (Ahola et al., 2012; Aittomäki, Lahelma, Rahkonen, Leino-Arjas, & Martikainen, 2007; Andel et al., 2012; Molarius et al., 2006). Furthermore, the distribution of adverse work conditions across the working population have been shown to be socially patterned, in that these conditions are more prevalent among persons with a lower educational attainment and among those with a lower occupation-based class (National Board of Health and Welfare, 2009). Persons with lower socioeconomic position more often have poorer health than those with a higher socioeconomic position (Åberg Yngve, 2005; Mackenbach, Kunst, Cavelaars, Groenhof, & Geurts, 1997; Marmot & Wilkinson, 2006; Marmot et al., 1991; National Board of Health and Welfare, 2009). For example, individuals who hold positions that involve lower qualifications are more likely to be exposed to adverse psychological and physical working conditions such as noise, chemicals, heavy lifting, static load, repetitive/monotonous tasks, and stress that in turn might exacerbate poor health (Siegrist & Theorell, 2006). Further, persons exposed to such conditions will be less able to work until, and after retirement age (National Board of Health and Welfare, 2009; Swedish Government Official Reports [SOU], 2002).
Some have posited that working conditions account at least partially for the association between socioeconomic position and physical health (Aittomäki et al., 2007; Mehlum, Kristensen, Kjuus, & Wergeland, 2008; Warren, Hoonakker, Carayon, & Brand, 2004). Others (Bauer, Huber, Jenny, Muller, & Hämmig, 2009; Rahkonen et al., 2012) have shown that working conditions explain socioeconomic differences in self-rated health. Moreover, socioeconomic position has been suggested to contribute to the differences in the relationship between psychological working conditions and cognition (e.g., Andel et al., 2011). A stressful and physically demanding job is, however, common amongst people of all socioeconomic positions, but unlike most other working conditions, studies suggest that it is more common among higher nonmanual workers in a managerial position (Niedhammer, Chastang, David, & Kelleher, 2008).
Research relating to socioeconomic health differences is typically based on various measures of socioeconomic position, including education, occupation-based social class, and income (Galobardes, Lynch, Davey Smith, 2007; Galobardes, Shaw, Lawlor, Lynch, & Davey Smith, 2006a, 2006b), with results potentially diverging as a function of how socioeconomic position was represented (Galobardes et al., 2007; Hallqvist, Lynch, Bartley, Lang, & Blane, 2004; Karp et al., 2004; Molarius et al., 2006). In the present study education and occupation-based social class are studied as origins of work-related inequalities in health.
Education is arguably the most encompassing measure of socioeconomic position as it bridges parent’s socioeconomic position to own adult socioeconomic position and tends to affect a range of life chances and living conditions through the life course (Fors, Lennartsson, & Lundberg, 2009; Galobardes et al., 2007; Monden, 2005). Moreover, level of education is a major determinant of an individual’s future occupation (Galobardes et al., 2007). Occupation-based social class, in turn, is a measure partly associated with occupational risks (Monden, 2005) that can have long-lasting effects that may extend beyond retirement (Karp et al., 2004). Studies so far have not attempted to examine socioeconomic position in relation to a comprehensive set of health factors in later life within one study, nor the combined influence of socioeconomic position and working conditions on health after retirement. Hence, the main objective of this study was to explore the role of working conditions in the association between socioeconomic position and health after retirement age using over 20 years follow-up using two measures of socioeconomic position (education and occupation-based social class) and six measures of health (self-rated health, psychological distress, musculoskeletal pain, circulatory problems, physical and cognitive impairment). By including self-reported as well as objective measures of health, we were able to obtain a uniquely comprehensive picture of these associations. In addition, we explored the contribution of both physical and psychological working conditions to any association between socioeconomic position and health.
Method
Data
We used the Swedish Level of Living Surveys (LNU) from 1968 and 1981 and the Swedish Longitudinal Study of Living Conditions of the Oldest Old (SWEOLD) from 1992, 2002, and 2004. LNU consists of a nationally representative sample of the Swedish population between the ages 15 and 75. SWEOLD, also representative on a national level, is a continuation of the LNU and consists of those participants from the LNU sample who reach age of at least 77 years at the time of SWEOLD data collection. Age of 69 years and above was used in the 2004 survey.
Face-to-face interviews were used for data collection in the 1992 and 2002 surveys. Telephone interviews were used for the 2004 survey. Proxy interviews (a family member or a caseworker who knew the individual well because such a proxy is familiar with the interviewee’s health) were conducted if direct interviews were impossible due to poor health or cognition.
For the purposes of this study, a longitudinal data set was constructed resulting in three waves. The first wave was a combination of the 1968 LNU survey and the 1992 SWEOLD survey, the second wave a combination of the 1981 LNU survey and the 2002 SWEOLD survey, and the third wave a combination of the 1981 LNU survey and the 2004 SWEOLD survey, resulting in follow-up times of 21 or more years.
Housewives, unemployed persons, students, or others without gainful employment were excluded because their working conditions could not be assessed.
Due to the selection process for the SWEOLD surveys, 226 people were interviewed both in 2002 and 2004, subsequent the 2004 responses were excluded, if interviewed in 2002. This resulted in a total sample of 1,131 respondents with valid information for at least one health outcome. Ages ranged from 46 to 64 at baseline and from 69 to 88 at follow-up (born between 1904 and 1935); 329 respondents were interviewed in 1968 and 1992; 284 respondents were interviewed in 1981 and 2002, and 518 respondents in the 1981 and 2004 period.
Measures of Health
Self-reported as well as objective measures of health were used.
Self-Reported Measures
Objective Measures
In 2004, the SWEOLD surveys were done solely by telephone; so tests of physical impairment were not performed. Data from SWEOLD refer only to 1992 and 2002.
Socioeconomic Position
Socioeconomic position was measured by education and occupation-based social class. Along with working conditions, these data were based on self-reports of the current situation at the time of baseline interviews in 1968 and 1981, when respondents were still in the workforce.
The
Measures of Working Conditions
Physical and psychological working conditions were measured using aggregated indices in which affirmative answers were coded as 1.
All independent variables—except for the measures of socioeconomic position (dichotomous)—were given a linear representation, that is, the likelihood (expressed as beta-coefficients) that a respondent reports poor health increase linearly with each additional unit in indices. If the analyses indicated that a linear representation regarding working conditions was inappropriate (by testing a linear effect in a dummy-coded variable) then for the physical working conditions, the original 0 to 2 categories were assigned to good, and 3 was assigned to poor. For the psychological working conditions, the original 0 to 2 categories were assigned to good, and 3 to 4 were assigned to poor. Specifically, the measure of physical working conditions did not follow a linear progression for psychological distress and musculoskeletal pain (in the models with social class for years 2002 and 2004), and the measure of psychological working conditions for physical impairment, and were therefore dichotomized.
Statistical Methods
Ordered logistic regression was used in the main analyses; covariates were age, sex, and survey year. Unlike binary logistic regressions, ordered logistic regression can analyze outcome variables of more than two categories if they can be ranked (e.g., where poor health outcomes can be expressed in several categories such as good, bad, or in-between). Unlike linear regression there is no assumption of equal step sizes with respect to the outcome. Coefficients from ordered logistic regression correspond to the result of a weighed value of a series of binary logistic regression and can be presented as an overall beta-coefficient. The coefficient gives the change when the independent variable changes by one unit, while all other variables are held constant. The beta-coefficient shows the effect of having a higher value in the dependent variable (e.g., reporting self-rated health as bad rather than in-between). For variables given dummy representation, the coefficient indicates the difference relative to the reference category (e.g., manual worker compared with nonmanual worker). For independent variables given linear representation, the coefficient indicates the change for each value of the variable.
Results were adjusted for age, sex, and year of SWEOLD data collection in Model I. Models II and III were additionally adjusted for physical (Model II) and psychological (Model III) working conditions. Since covariation (measured in terms of Spearman’s rho) between physical and psychological working conditions was close to zero (0.042), highlighting the difference between the two constructs, adjusting for both measures of working conditions within one model was considered superfluous.
Models II and III also show a change in the beta-coefficient between Model I and Model II or III, expressed as the percentage value reflecting the extent to which physical or psychological working conditions account for the association between socioeconomic position and health. A negative value means that the association between socioeconomic position and health increases when working conditions is controlled for. We might infer from this that nothing of the association is explained and that socioeconomic differences in health would be greater if working conditions were the same.
The interaction between sex and socioeconomic position was not significant for any health outcome whereby the analyses were based on a combined sample of men and women. Similarly, there was no significant interaction between survey year and socioeconomic position except for the association between social class and musculoskeletal pain. Therefore, results are reported separately for 1992 and 2002/2004.
Results
As shown in Table 1, about 26% of the 1992 sample, 40% of the 2002 sample, and 57% of the 2004 sample reported more than mandatory education. This increase is partially attributable to the lower age threshold in 2004 (age 69). The difference between 1992 and 2002, in turn, is due to the actual changes in the proportion of individuals with higher education. Correspondingly, the proportion of manual workers decreased from 64% in 1992 to about 50% in 2002 and 2004. For all three periods, about 50% of the respondents reported they had not been subject to any of the negative aspects of physical working condition, while 5% to 7% reported that they had been subjected to all negative aspects. About 2% to 3% reported having been subjected to all four negative aspects of psychological working conditions. And the proportion of respondents who reported that they had been subjected to adverse physical working conditions noticeably declined over time, from 52% (100% to 48.3%) in 1992 to 42% in 2004. But the proportion of respondents who reported having been subjected to adverse psychological working conditions was greater and increased over time.
Descriptive Statistics (n = 1,131).
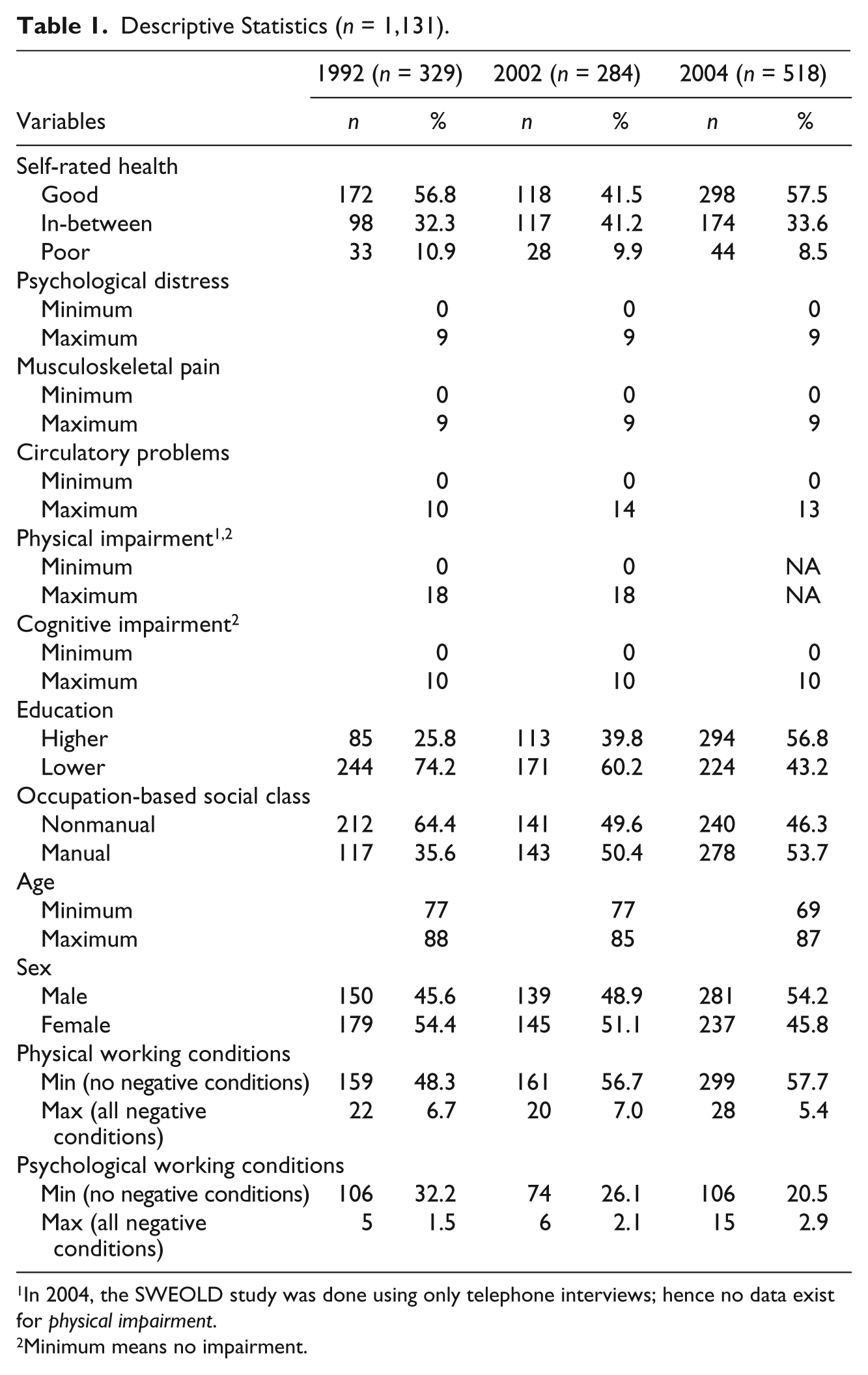
In 2004, the SWEOLD study was done using only telephone interviews; hence no data exist for physical impairment.
Minimum means no impairment.
Table 2 displays results from the main analyses, presented as beta-coefficients. All three models contain the same observations per each outcome. Overall, the results show that low socioeconomic position was associated with poor health across the outcomes, but for the association between occupation-based social class and musculoskeletal pain in 2002 and 2004. That is, those with a low socioeconomic position reported slightly more health problems than those with a high socioeconomic position. The results also demonstrate strong direct associations, after adjusting for socioeconomic position, between psychological working conditions and poor self-rated health, psychological distress and musculoskeletal pain, and to cognitive impairment though a weaker association for the latter (Model III). Adjusting for socioeconomic position, the results show direct associations between physical working conditions and musculoskeletal pain in 2002 and in 2004; psychological distress, and physical impairment.
The Influence of Working Conditions on the Association Between Socioeconomic Position and Health After Retirement Age—Adjusted for Sex and Age. Presented as Beta-Coefficients (ß).

Notes:
Reference category.
Linear representation unless stated otherwise.
Formula: 1-(β Model II or β Model III) / β Model I)).
Work conditions are dichotomized.
Practically no differences between manuals and nonmanuals were observed, hence no change in ß not presented
Results from 1992 only, as differentiated from 2002 and 2004.
Results from 2002 and 2004 in combination as differentiated from 1992.
Negative correlation between occupation-based social class and musculoskeletal pain, thus no change in beta presented.
p < .11. † p < .10. *p < .05. **p < .01. ***p < .001.
Model I: Shows the association between socioeconomic position and health, adjusted for sex, and age.
Model II: As model I, additionally adjusted for physical working conditions.
Model III: As model I, additionally adjusted for psychological working conditions.
Generally, the influence of working conditions on the association between socioeconomic position and poor health in old age was quite small. The strongest working-condition influence was on the association between socioeconomic position and physical impairment and musculoskeletal pain. When adjusting for physical working conditions (Model II), the association between education and physical impairment decreased from 0.27 in Model I to 0.18 in Model II. The association between occupation-based social class and physical impairment decreased from to 0.27 to 0.16. The corresponding change in the beta-coefficient was 33.3% (education) and 38.5% (occupation-based social class). Similar patterns were discerned regarding musculoskeletal pain, where the association to education decreased 20.0%, when adjusting for physical working conditions. In turn, the difference between former manual workers and nonmanual workers decreased 44.4% in 1992. But the impact from physical working conditions on the association between occupation-based social class and musculoskeletal pain was only observable in 1992.
The analyses revealed that the influence of psychological working conditions consistently explained little, if any, of the association between socioeconomic position and health in general. Rather, the results indicated that the association between socioeconomic position and health in old age would be stronger if psychological working conditions would be similar for those with lower socioeconomic position versus higher socioeconomic position. This is because respondents with a higher socioeconomic position had worse psychological working conditions than respondents with a lower socioeconomic position.
Discussion
With a follow-up period of over 20 years, this study explored to what extent working conditions during working years contributed to the association between socioeconomic position and health after retirement age in Sweden. To this end, the influence of physical as well as psychological working conditions and two measures of socioeconomic position and six measures of health were assessed.
The results indicated that physical working conditions account for substantial portions of the association of socioeconomic position with physical impairment and musculoskeletal pain in old age. This suggests that any influence of socioeconomic position on these outcomes may at least partially be due to more adverse physical working conditions in low socioeconomic position.
These results match well with previous research based on the employed population. For example, those with lower education often have jobs that expose them to physical factors that can contribute to load-induced injury, such as heavy physical labor, monotonous, nonergonomic movement patterns, and noise (National Board of Health and Welfare, 2009; Siegrist & Theorell, 2006; Swedish Work Environment Authority, 2010).
In contrast, psychological working conditions consistently explained very little of socioeconomic health inequalities among the old. Rather, the reverse relationship was observed, whereby respondents with a high socioeconomic position during their working years were more likely to have been exposed to harmful psychological working conditions. While this result is aligned with previous research, which reported that stressful, psychologically demanding jobs are more common among persons with a higher socioeconomic position (National Board of Health and Welfare, 2009; Niedhammer et al., 2008), other studies reported that persons in lower socioeconomic positions are particularly susceptible to stress-related problems due to work situations that combine high demands, low degrees of autonomy, and insufficient support (National Board of Health and Welfare, 2009; Siegrist & Marmot, 2004). Unlike persons in high socioeconomic positions, these persons have no control over their work situations (National Board of Health and Welfare, 2009; Siegrist & Marmot, 2004).
Given the limited influence of psychological working conditions, the present study may have disregarded dimensions of working conditions, poor health or both, which are more likely to influence the association between socioeconomic position and health in old age. A reduction in the relative number of industrial workers in Sweden did not occur until the late 1970s (Brante, Andersen, & Korsnes, 2001). This might indicate that respondents to the 1968 and 1981 surveys were more frequently employed in some form of industry that commonly involved heavy labor, nonergonomic working positions, and loud noise. With this in mind, the present study’s results might reflect working conditions of that time. For respondents with lower socioeconomic positions, heavy physical labor often characterized working conditions that led to load-induced disorders such as musculoskeletal pain and physical impairment.
However, a considerable proportion of the workforce is still exposed to the adverse effects from physical work conditions in Sweden (Swedish Work Environment Authority, 2010). Physical load, which affects muscles and joints, is the single most common cause of work-related problems such as musculoskeletal damage. Construction workers, loggers, and farmers still run a serious risk of such disorders (Swedish Work Environment Authority, 2010). Moreover, because manufacturing has declined in importance over the past few decades (due to automation and international outsourcing) and because the service and care sectors have expanded, female workers (e.g., health care assistants, nursing auxiliaries, and till operators) have become increasingly susceptible to these load-induced disorders (Swedish Work Environment Authority, 2010).
Even though the results only show influence of physical work conditions on the association between socioeconomic position and two out of the six measures of health, one cannot dismiss the notion that an individual either has to their disposal health-promotive resources or is subject to health-damaging exposures during his or her working life depending on socioeconomic position. Hence, there can be no doubt that working conditions impinge on health in old age when accounting for the results showing direct associations between working conditions and health among the old, in general, and between the psychological working conditions and health in particular.
Whereas earlier studies were based on persons still active in the workforce, this study, with its extensive follow-up period (more than two decades separates the survey of socioeconomic position and working conditions on the one hand, and health outcomes on the other), provides unique insight into how former working conditions affected the association between socioeconomic position and states of health in old age.
In applying a comprehensive approach by including several self-reported and objective measures of health, this study sheds new light on the exposure to adverse physical working conditions as one reason for socioeconomic differences in physical impairment and musculoskeletal pain in later life.
The baseline surveys, when the studied populations was in working ages, where conducted in 1968 and 1981. In Sweden the situation for the labor force regarding work place safety and regulations of the work conditions were comparable to that in most of the developed countries (Blau & Kahn, 1996; Smulders, Kompier, & Paoli, 1996). This makes it likely that our findings about work conditions would be similar to other developed countries.
As with any research, results from this study should be interpreted with caution on three points. First, a comparison of older individuals with varying socioeconomic position can be a somewhat hazardous enterprise. Selective survival (Markides & Machalek, 1984), that is the systematic difference between survivors and nonsurvivors, might have affected the present study in that the analyses only apply to survivors. Many factors are related to the probability of living into old age (e.g., good health, healthy lifestyles, and a higher socioeconomic position). Such selection might have affected the association between socioeconomic position and poor health among the old in this study by underestimating it. Thus, selective survival is not a phenomenon that is specific to this study; it is a phenomenon that affects all studies of the life and health of older persons. It has been shown that the health gap persists into old age despite selective survival (Fors et al., 2008; Karp et al. 2004).
Second, while LNU and SWEOLD were nationally representative surveys with low nonresponse rates, it is plausible that the actual health of the old is worse than reported in the health data used in this study, because it was not possible to conduct interviews with the most frail (selective nonresponse). In population studies, nonresponses are often related to poor health and results from surveys of the old are thus particularly susceptible. Including information from proxy interviews, when such were available, partially compensated for this loss. But we cannot eliminate the possibility of less reliable data when including proxy interviews. But findings from a review of self and proxy responses studies suggests that proxy responses are of no worse quality than direct responses (Moore, 1988). Rather, by ignoring proxy interviews, the nonresponse rate would increase and make respondents appear healthier than the group they are meant to represent. In addition, this would exclude many of the oldest old (Kelfve, Thorslund, & Lennartsson, 2013).
Third, by measuring socioeconomic position from only one point during the period of occupational activity, one cannot fully eliminate the possibility of social mobility that in turn might alter results in one direction or another. But the effect of social mobility may be minimal considering the age span in the present study’s population (ages 46–64 at baseline). Finally, due to the nature of the analyses, socioeconomic position was measured dividing education and occupation-based social class into just two categories (lower and higher education and manual and nonmanual workers). Such a crude categorization may have resulted in loss of significant information. Socioeconomic position is not a matter of poor health for the disadvantaged and good health for everyone else. Rather, the society is based on a multilayered socioeconomic hierarchy that follows a social health gradient, whereby health declines the lower down the hierarchy one goes (Marmot et al., 1991). Consequently further research, based on more comprehensive information on socioeconomic position, may reveal more significant health differences among the old.
Conclusion
The influence of working environment on health is substantial and may grow in the younger generations in parallel with the growth of total time spend working, owing to a raised retirement age (Statistics Sweden, 2012b). Sickness-related reduced work capacity is strongly associated with the nature of the work a person has or has had, which is reflected in socioeconomic differences that exist between groups of individuals. The results of this study show that individuals with lower socioeconomic position during their years in the workforce develop problems with musculoskeletal pain and physical functional impairment in later life—partially due to physical working conditions. The presence of heavy physical load, high demands, and cutbacks are cited among the reasons for not staying at work until retirement age (SOU, 2002). Since musculoskeletal pain and physical impairment increase with age (Ahacic & Kåreholt, 2010), we can expect the presence of a higher proportion of older workers to lead to an increase in the number of people with such complaints. If changes in working life are reflected in greater disparities in working conditions, then socioeconomic differences associated with poor health between occupational groups might also increase.
Investing in measures that promote healthier working conditions to create conditions that resemble those for occupational groups with a low incidence of sickness absenteeism and debilitating physical and psychological impairment is particularly urgent. Going forward, such investments might have positive effects on health and medical care costs. They might narrow the socioeconomic difference gap, and hopefully encourage the working-age population to stay active in the workforce until, and after age 65.
Footnotes
Acknowledgements
The authors gratefully acknowledge financial support from Marianne och Marcus Wallenbergs Stiftelse: grant MMW 2011.0036, the members of the social gerontological sector of the Aging Research Center (ARC), Stockholm, for valuable comments on earlier manuscripts of the text. The Karolinska Institute Ethics Committee approved the project.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research for the article was funded by the Marianne and Marcus Wallenberg foundation, No: MMW 2011.0036.