
Abstract
Introduction
Adolescents and young adults (AYA) with cancer have been in the spotlight for the past several decades owing to their rising number and substantial ongoing needs after their treatment. According to National Cancer Institute (2023), about 85,980 AYA aged 15–39 are diagnosed with cancer each year in the United States, and their number is constantly growing. While their average survival rate is growing above 85% and the mortality rate is decreasing due to the advancement in medicine (National Cancer Institute, 2023), cancer makes them deal with complex, time-sensitive challenges that include an unfamiliar health care system, uncertainty and fear of death, and possible social alienation during their early development (Ferrari et al., 2010; Marshall et al., 2019; Sisk et al., 2019). Critically important life issues such as personal goals, school activities, peer relationships, and age-related developmental tasks often become secondary during treatment because of concerns about survival (Burgers et al., 2021). Despite their multidimensional suffering, this group has been marginalized in terms of age-appropriate care because neither pediatric nor adult health care settings are suitable for the provision of proper psychosocial services (Burgers et al., 2021). This qualitative study aims to obtain feedback on the planned nurse–patient dyadic storytelling. This will be an initial step in establishing a developmentally tailored, relationship-focused psychosocial intervention that caters to the unique needs of AYA with cancer.
Background
While traditional oncology care prioritizes survival and symptom elimination, AYA oncology care should focus on promoting the psychosocial capacity to deal with lifelong challenges and move toward the future. According to a thriving-based model of adjustment for young survivors of childhood cancer, the absence of psychological symptoms, such as depression or anxiety, does not necessarily imply optimal psychological functioning, and health care services should be able to build AYA strengths and capacities to deal with difficulties following cancer diagnosis (Scrignaro et al., 2016). Despite ongoing national research priorities, there are significant gaps in AYA-specific research and intervention development to promote their abilities to deal with cancer-related challenges. Without spotting and filling such gaps, these patients’ long-term quality of life may be compromised even though advances in medicine and technology mean that survival rates continue to increase.
Nurses taking care of those AYA are well positioned to provide individualized, holistic care in guiding individuals to develop or reclaim pathways toward complete well-being and a thriving future (National League for Nursing, 2014). In particular, oncology nurses spend a significant amount of quality time with patients at all cancer trajectories, from diagnosis to survivorship or end-of-life care, and are well-informed about their personalized, complex treatment (Charalambous et al., 2018). These nurses are well-trained and proficient in therapeutic communication skills that can build trusting relationships and eventually help AYA with cancer to feel understood and connected, reduce any feelings of vulnerability as they develop independence, and achieve better health outcomes (Essig et al., 2016; Jacobsen et al., 2015; Montgomery et al., 2017).
Storytelling is one of the supportive techniques nurses can apply to provide holistic care for AYA with cancer. Through storytelling, people have been communicating their messages containing their identity, life experience, perceived meaning of the events, wisdom or expertise, and even evoking a strong catharsis while sharing meaningful stories (Bowles, 1995). Storytelling has been the core of person-centered, relationship-focused nursing care, which can facilitate individuals’ recovery capacities by discovering and reconstructing the meanings of experiences (Fitzpatrick et al., 2019; Smith & Liehr, 2014). This creative and expressive strategy has been successfully utilized for young cancer patients to provide health education, information, legacy-making, and psychological care and led to positive impacts on their quality of life and psychosocial functioning, including coping, social integration, and connection, parent–child communication, and emotional comfort (Haase et al., 2020; Laing et al., 2017). Most storytelling intervention studies have been conducted and delivered by research teams, while the engagement of patients’ primary nurses who have created strong rapport has been limited.
Given the potentially powerful role of the nurse–patient relationship and storytelling in health care for AYA with cancer, we aim to apply a dyadic nurse–patient approach that guides both participants to co-create their stories, especially in the context of AYA oncology nursing. As one of the initial steps, this study explores the perspectives of AYA with cancer on a dyadic storytelling intervention with their primary nurses and answers the following question: “What are the perspectives of AYA with cancer on the idea of a dyadic storytelling intervention with their primary nurses?”
Theoretical Framework
The theoretical framework guiding this study is the Story Theory. Story Theory defines stories as a soothing narrative created through intentional, meaningful, and trusting dialogue with others, in which people find meaning by recounting their present life experiences and considering their past and future (Smith & Liehr, 2014). Through purposeful conversation, patients can identify their thoughts and feelings and the meaning of their experiences, truly embracing their stories from unique personal perspectives and beginning to change and resolve their perceived health challenges (Smith & Liehr, 2014).
Intervention Model Development
Our intervention development follows the Obesity-Related Behavioral Intervention Trials (ORBIT) framework, guiding behavioral intervention development and optimization through flexible, iterative, and systematic processes (Czajkowski et al., 2015). While the ORBIT framework was initially developed for obesity studies, this intervention development guideline can be applied across diverse contexts to create interventions that promote healthy behavior changes (Czajkowski et al., 2015). The current study corresponds to the design phase, which seeks to establish the basic intervention elements and determine the delivery mode (Czajkowski et al., 2015).
Our theory-driven prototype intervention model, Expressive Storytelling to Share AYA Stories (ESSAY), was developed based on the Expressive Writing Framework (Pennebaker & Evans, 2014) and multiple discussions with interdisciplinary palliative and pediatric/AYA oncology experts (n = 18). Experts included nurse researchers (n = 3), pediatric oncology nurses (n = 4), and pediatric oncologists (n = 4), as well as a palliative medicine specialist, an oncology recreational therapist, a child life specialist, a writing clinician, an oncology social worker, and developmental and clinical psychologists (n = 2). The prototype model was then successfully tested with a single nurse–AYA patient dyad (n = 2) and refined based on the participants’ feedback. For example, we partially employed the writing prompts of the Expressive Writing Framework while focusing more on the visual and spoken formats, following feedback from the participants of this single case study. The current study aimed to solicit thoughts from AYA participants regarding this change.
ESSAY Intervention
ESSAY consists of five weekly online dyadic storytelling sessions between one AYA with cancer and one of their primary nurses. Once an AYA participant is recruited, they are asked to nominate three to five nurses they are willing to invite as their storytelling partners. The research team presents the list to the pediatric and AYA oncology department nurse managers and conducts an initial suitability screening based on the eligibility criteria (i.e. more than 1 year of oncology nursing experience, possession of adequate communication skills). The team then invites eligible nurses to participate, introduces the study, informs them that one of their patients has invited them as a storytelling partner, and obtains their written consent. To minimize the nurse burden, the study is conducted online during off-duty hours. Before the intervention, both AYA and nurse participants join an online orientation session independently. They are informed about the intervention procedure, potential benefits and challenges, and how to address any unexpected issues during the intervention. They have an opportunity to share their concerns or ask any questions about the intervention. During this process, nurses are informed that they will join this program as a storytelling partner, not as a nurse or a therapist. Then the AYA and nurse participants complete the 5-week sessions following instructions and topics (Table 1). They are asked to create their stories for each topic independently and then share the final stories with each other during the 1-hr online session. To provide a secure, private environment, the research team does not join the meeting but is available to provide any technical assistance or answer questions.
Intervention Overview
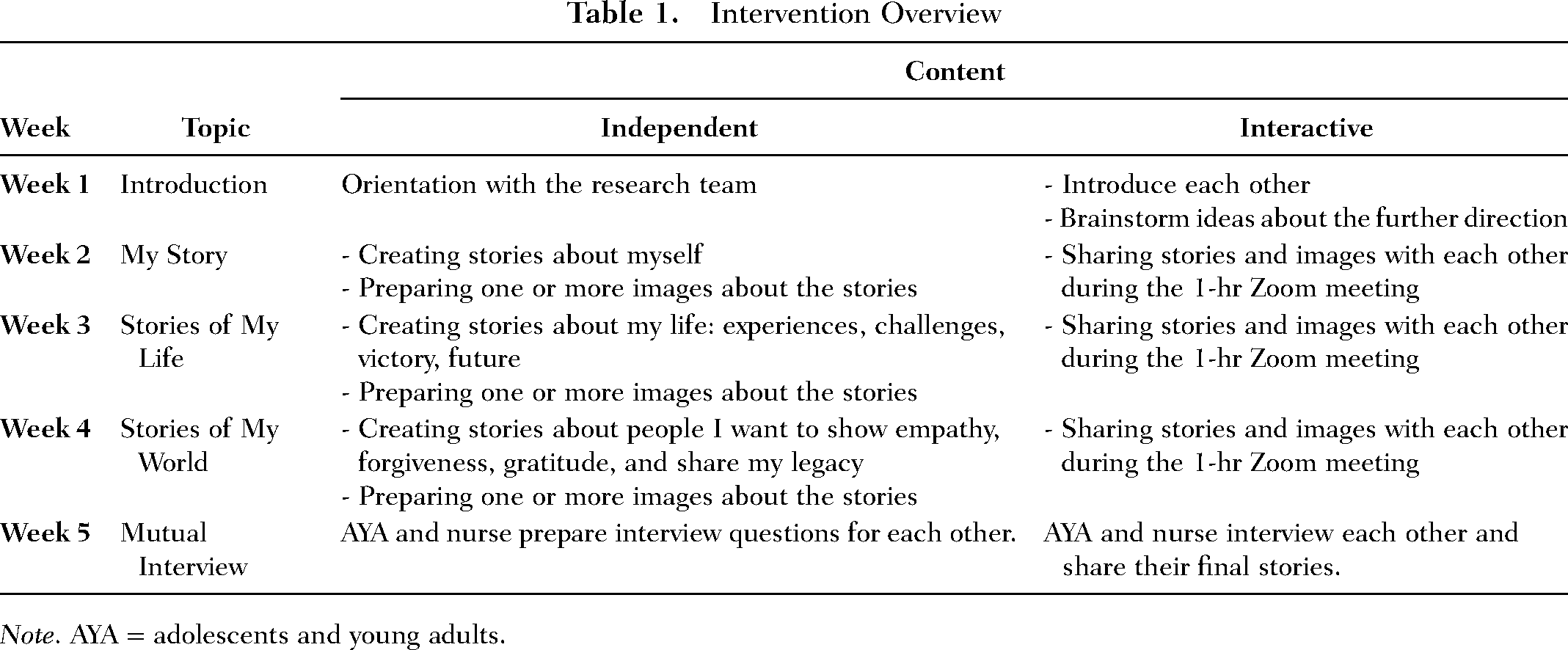
Note. AYA = adolescents and young adults.
Method
This qualitative study was conducted to introduce the ESSAY intervention model to AYA with cancer and obtain their feedback on this overall idea through a one-time online interview.
Settings and Participants
We recruited eligible AYA participants (a) aged 12–24, (b) diagnosed with any type of cancer during adolescence, (c) have moved into survivorship care within the last 5 years, (d) can write and speak in English, and (e) can access the internet using their own electronic devices. Participants were recruited through online research advertisements posted on (a) AYA cancer foundations (e.g. Stupid Cancer), (b) a listserv of the AYA cancer program at a university hospital, (c) social media platforms (e.g. Facebook), (d) snowballing, and (e) ResearchMatch, a national online recruitment registry that connects individuals who wish to participate in research to researchers (Harris et al., 2012).
Ethical Considerations
The institutional review board approval was obtained from Vanderbilt University (# 201808). Prospective participants who were interested in this study were requested to complete the screening survey, which was integrated into online research advertisements. To collect and manage the data securely, we used the Research Electronic Data Capture (REDCap) system. Upon being deemed eligible, the study personnel contacted prospective participants through their preferred mode of communication (e.g. text message, email, phone) to verify eligibility and schedule a Zoom appointment for the informed consent procedure and the interview. During the Zoom session, the study team went over the informed consent form with the participant, addressed any inquiries, and obtained their electronic signature. All participants were then provided with an electronic copy of their signed informed consent document.
Data Collection
Right after the informed consent procedure, we conducted a one-time, online qualitative interview with AYA cancer survivors to obtain feedback on our intervention model. Eligible participants who agreed to take part in this study were invited to an approximately 30-min individual online interview via Zoom. At the beginning of the interview, we introduced our prototype intervention model using PowerPoint slides. Then participants were asked to answer interview questions (Table 2) and share their feedback on the intervention model. Data collection continued until we achieved data saturation.
Interview Questions
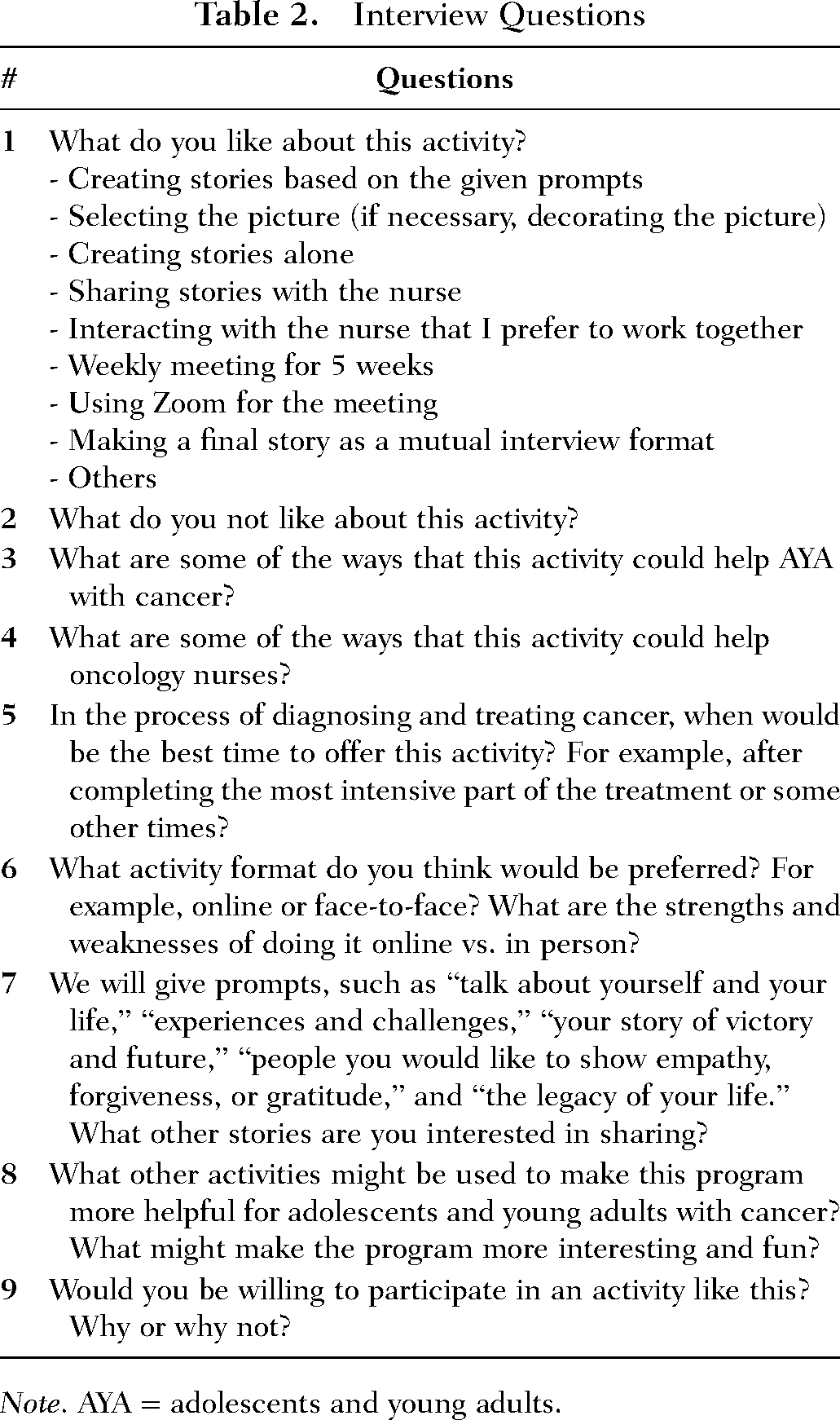
Note. AYA = adolescents and young adults.
Data Analysis
Each interview was audio recorded and transcribed. The transcribed interviews were entered into the Microsoft Excel program and analyzed by three trained coders of Vanderbilt University Center for Health Services Qualitative Research Core in collaboration with the principal investigator. A directed content analysis with a combined inductive and deductive approach was used as this study aims to validate the existing intervention model (Hsieh & Shannon, 2005). This content analysis began with immersion through repeated reading of the transcripts, clustering similar ideas/excerpts to inform preliminary categories, reviewing and revising coding schemes, and repeating this process until no new themes emerged and a consensus was reached (Saldana, 2015). To ensure rigor and trustworthiness, three coders cross-checked the coded data, regularly discussed the analysis at regular team meetings, and established reliability.
Results
A total of 13 AYA cancer survivors participated in the one-time, 30-min Zoom interview. The average age of participants was 21.77 (SD = 1.42) and average age at diagnosis was 18.38 (SD = 2.76). Most participants had no experience of cancer relapse (n = 12, 92.31%) and had an experience of chemotherapy (n = 12, 92.31%). Table 3 summarizes participants’ demographic and clinical information.
Demographic Characteristics (N = 13)
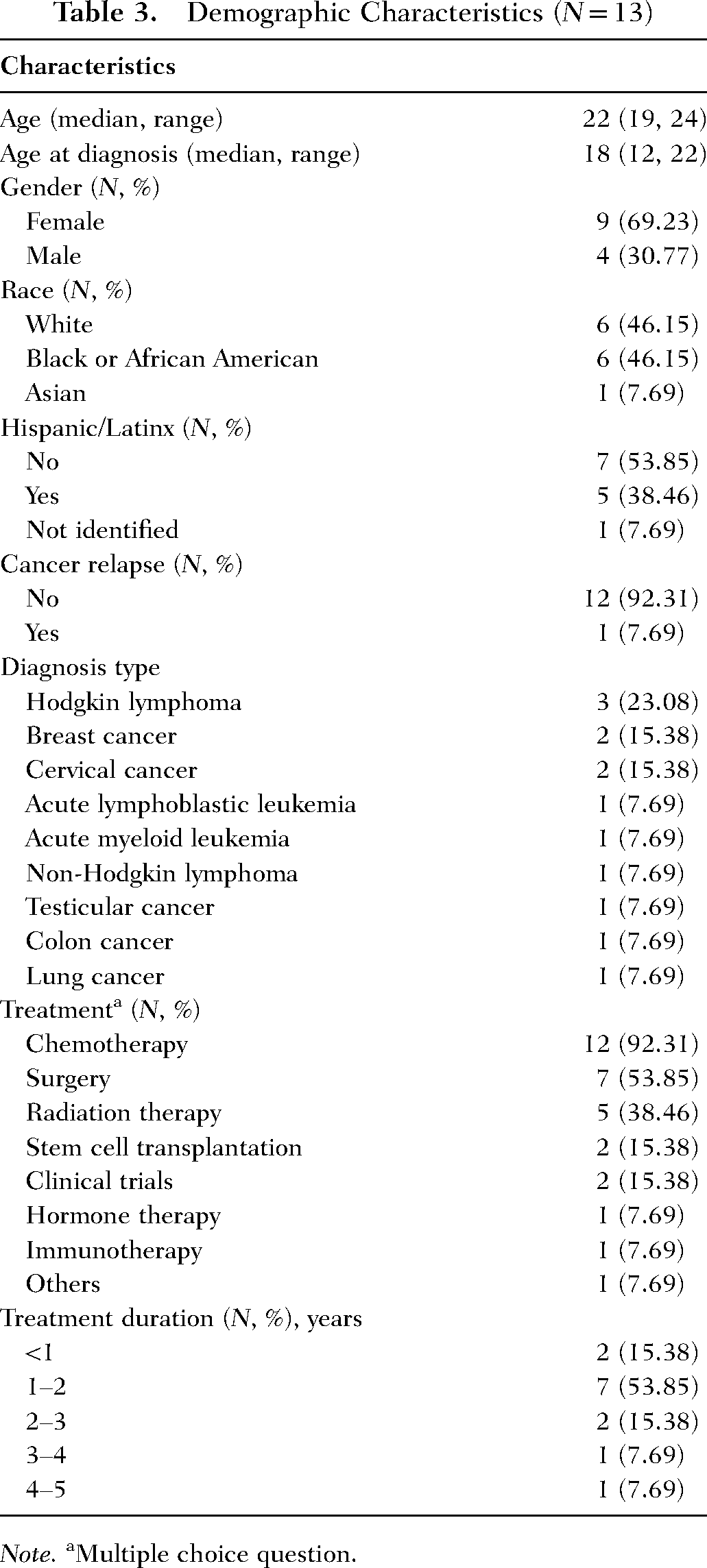
Note. aMultiple choice question.
Participants’ responses were categorized into two domains: Barriers and Facilitators (Table 4). Due to the limited space, detailed quotes for each subtheme were presented as Supplementary Materials (Appendix 1).
Barriers and Facilitators
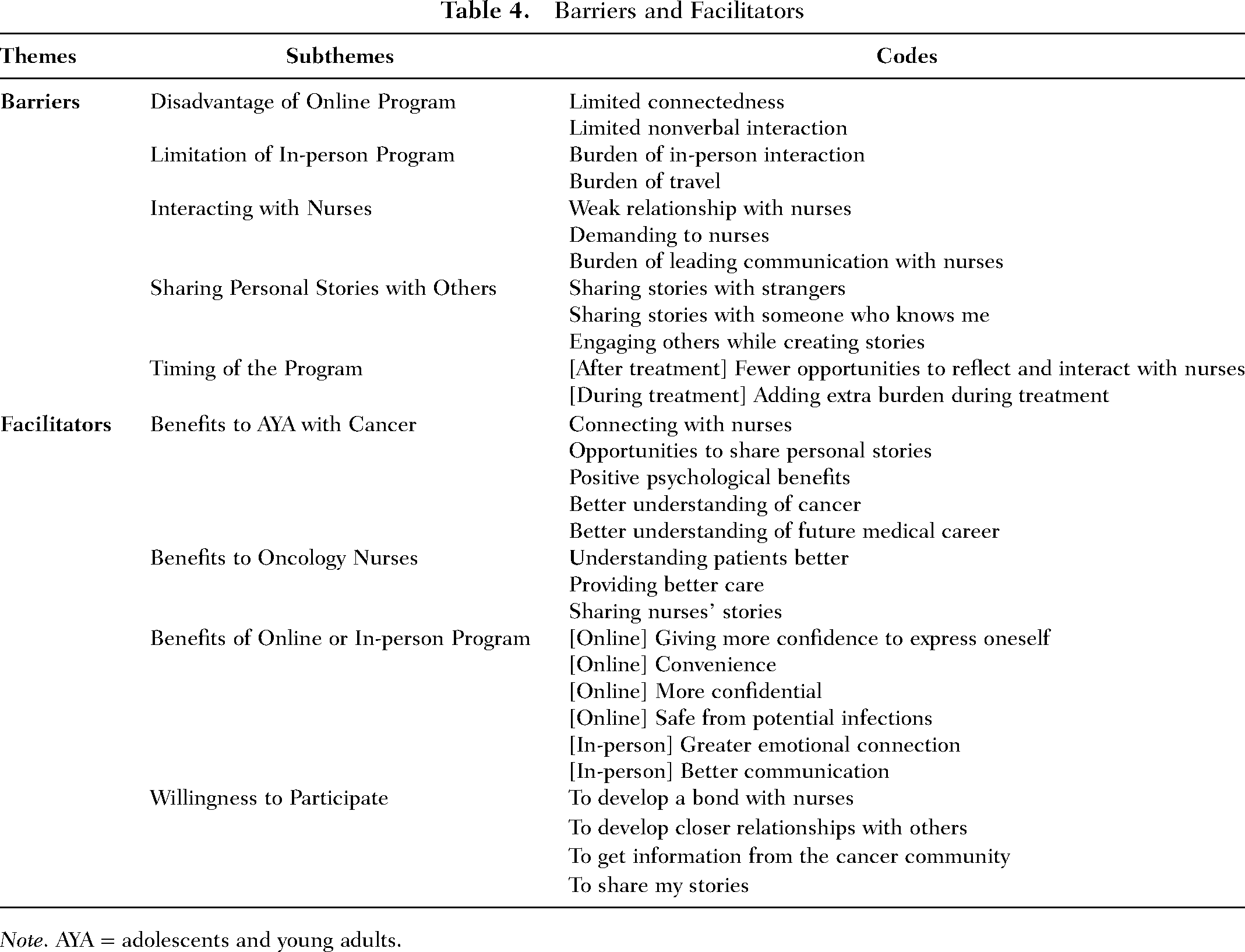
Note. AYA = adolescents and young adults.
Barriers
There were 23 entries coded as barriers, and each statement received one or more additional codes. Several barriers were coded when participants talked about having the program online or in person while there was no consensus on the preferred methods. Some participants noting that relying on remote technology took away from the value of the program by limiting connectedness: “…without COVID or if COVID becomes no longer dangerous, I would probably prefer face to face … I think that connection would be a lot more deeper if it is in person.” Another participant thought that online intervention might make it harder for some patients to follow up on their participation: “…people can’t do a follow-up in some ways because it is online, so there could be some issues related to that challenges.” The loss of facial expressions and other nonverbal cues was seen as a problem associated with online implementation: …when you are interacting with someone face-to-face, you don’t hide what you are feeling, because you know … facial expression and movement, they make a big part of … how someone think while talking, so I feel like when [doing it] face-to-face, you can see all things.
On the other hand, a few participants felt less comfortable with the idea of face-to-face interactions compared to using Zoom. One participant stated that creating stories with another person present would be more uncomfortable and burdensome than working alone: “I really don’t feel comfortable meeting nurses that I know face-to-face … this is maybe not easy for some people…” Having to travel for face-to-face interactions was seen as another barrier. One participant said “…travel, that could another big issue. So, if I can do it in the hospital during the stay [face-to-face], it could be nice.”
In addition to the mode of communication, interaction with the nurses was viewed by some as difficult or uncomfortable. There was an opinion that this intervention would mainly benefit nurses, and the advantages for the patients may depend on the existing relationships with the nurse. If an AYA patient has a weak relationship with their nurses, then sharing stories with someone they have a stronger relationship with could be more beneficial: “I think it could be positive depending on the relationships between the person and their nurse. …I think it could still help the cancer patients if they had or have a strong relationship with their nurse.”
One participant saw participation in this program as generally beneficial to the oncology nurses but was worried that exposure to multiple patients’ physical and emotional challenges might be overwhelming: It could be a lot for the nurses like, taking on both their physical and emotional needs… I just think, if there is one nurse has to interact with a lot of kids and it's kind of like, it could be emotionally overwhelming…
Another participant was concerned about the final session which they saw as involving more self-guided communication with the nurses. This AYA said, …I think sharing stories and creating stories based on given prompts, that something allows me and helps me to get through my journey, but the [mutual] interview would be … If I need to be more independent and act like Oprah Winfrey, that would be a burden.
Participant discomfort with sharing stories and information with others they know or do not know was another potential barrier. One participant was willing to share stories with nurses they knew but would feel uncomfortable sharing with someone they did not know: If that is a nurse that I didn’t have a relationship, I wouldn’t want to really share much, and I wouldn’t really be like comfortable with that. But if it's one that I’ve had a relationship, I think that wouldn’t be an issue.
Meanwhile, some participants thought it might be uncomfortable to share pictures and stories with nurses they know and suggested it might be easier to tell the stories if they remain anonymous. They had concerns about sharing sensitive information with someone they already knew: …someone may want to talk about their stories to someone who doesn’t know them, so their identity remains unknown, no one knows that I’m talking about my story.… If the nurses know you, you may not want to share your pictures [through video camera], but if nurses don’t know you, you don’t need to care. You can just express yourself freely.
The other participant also mentioned, “…someone will feel uncomfortable to tell some of their stories to someone who knows them because then it can affect someone's thoughts [and perspectives] on you.” The other participant reported feeling more uncomfortable when someone is engaged in the story-making process and listening to their story: “I like creating stories alone because not every people feel comfortable about talking face-to-face or when someone else is listening to them.”
Finally, the timing of the problem was discussed as a potential barrier. One participant said that involvement in the program after treatment may not be ideal because they cannot fully reflect on their experience and communicate with nurses: …during the treatment [will be better to offer this activity] because that’s the time when you are actually really working with nurses, and that’s when you want to feel like [you want to be] known by nurses and you want to know them.… And the storytelling part could be helpful like, maybe even towards the end of the treatment so that you have processed more.
However, other participants thought that doing the program during chemotherapy would be less than optimal. They stated that they would like to wait until after treatments have finished in order to participate: I think if you’d asked me if I want to participate while I’m in the treatment, I would say no. And if you’d asked me after my treatment, I would say yes. Mainly just because when I think back that time, I just felt.. It was very overwhelming, so I would have more to offer after my treatment, after the experience, cause I’m sort of trying to piece it all together.
Facilitators
Facilitators are elements of the program or other processes that make it easier, more satisfying, and more beneficial for patients to participate in the storytelling program. Facilitators were also coded when participants discussed the advantages or benefits of participating in the program or some element of the program. The facilitator code was used on 121 different responses when coding participants’ answers to the nine open-ended questions. Each of these responses included an average of 3.8 other codes to describe their content. In the following paragraphs, we will identify the main facilitator themes and offer some representative quotes.
Benefits to AYA With Cancer
There were five themes identified as benefits to AYA for participation in the program: (a) connecting with the nurses, (b) opportunities to share personal stories, (c) positive psychological benefits, (d) better understanding of cancer, and (e) better understanding of the future medical career.
Connecting With the Nurses
Participants saw multiple benefits from being able to share their stories. Several participants mentioned the connection or bond with nurses as a benefit of program participation. One participant reflected on how hard it was to be treated in the adult cancer center at age 20 and how beneficial it would be to connect with the nurses: I was 20, and I just learned that I couldn’t go to the children’s hospital [because of my age], so I was treated at an adult hospital, and it’s really different. …What I was really wanted was like [having] that consistency of nurses … and to feel like you are being treated by someone who really cares about you and specifically about your health.
Some participants described the benefit as building a bridge between patients and nurses in order to create closeness and connection. The opportunity to share one's story about having cancer with someone who knows what it is was viewed by several as a benefit of the program. One of them said “Sharing stories with the nurses, it flattens the bridge between the patients and the nurses, so they will be closer and consequently creating the connection between them.”
Opportunities to Share Personal Stories
Sharing stories with someone they know or do not know could be a beneficial way to understand feelings about cancer: “… [I like] sharing my story to you because I think it would help to bring awareness to feelings or stories, everything AYA patients with cancer has to go through.” Participants saw telling stories as potentially healing by changing motivation and belief, and giving them a chance to express their feelings, especially feeling they have been reluctant to talk about. For example, one participant stated, “I think it will help AYA to express how it feels and shares what they’ve been holding in, or something like that.”
Another participant emphasized sharing as an expression of creativity: I think that it allows the patient to have a creative outlook. And it allows the patients to tell everyone around … exactly what they went through in a creative way and in a very formal way, and in a positive way and in a negative way … it allows the patient’s voice to be heard.
One of the participants reflected on how cancer is life-changing and how this kind of program can offer a chance to share thoughts and feelings about that: When you are diagnosed with cancer, your whole life changes. During the journey and even after recovering from the treatment, it’s hard to express your feelings and share thoughts, so I think this is a great opportunity for them to do it with.
Positive Psychological Benefits
There were several psychological benefits as a result of participation in the program that were identified as facilitators for involvement in the program. Participants talked about building strength to cope with cancer, acceptance of having cancer, and hope: “And it can also give them the courage and strengthen them.” The other participant also shared the experience by saying During this activity, AYA will embrace the fact that they are dealing with cancer and accept that they are now a new person [and] it’s really okay to having cancer. [Through this activity, they can] deal with the fact that they have cancer.
Another person said, “I think sharing their stories will bring hope, it's really a great way to highlight everyone's life.” One AYA said this program will build confidence to share their story with other people: “…it's helpful like crafting their stories that they can feel confident in their stories later on, like telling other people, helping other AYA craft their stories…”
Better Understanding of Cancer
Gaining a better understanding of cancer and its treatment was viewed as a benefit of program participation. One participant described having questions about cancer and cancer treatment answered: I think, especially for young adults facing such issues, engaging them into the interaction through the weekly meetings will be really helpful because most of their questions, concerns, other things about sickness, and maybe some issues like treatment can be answered.
Better Understanding of Future Medical Career
Participants reported that the intervention improved their understanding not only of cancer and its treatment, but also future career paths. One young adult described how listening to nurses’ stories can lead to a better understanding of ways to have a career in health care: In high school, I actually knew I wanted to work in medicine, but I didn’t know exactly what I wanted to do but, when I was being treated at [place], I formed a lot of relationships with all the nurses and all the PAs and … that’s what really inspired me to become a PA and eventually go on to PA school, working in oncology and BMT transplant.… Just listening to nurses’ stories and listening to what they have to say and all their own experienced is really inspiring, you know.
Benefits to Oncology Nurses
Participants were asked how oncology nurses might benefit from participating in the program, and their responses represent three subthemes: (a) understand patients better, (b) provide better care, and (c) share nurses’ stories. Some participants described nurses having a better general understanding of patient needs. As an example, one person said, “I think it will help them feel like they can understand their patients more, and then understand their needs more, and then they can feel more helpful in a way.”
Others were more specific and stated that nurses would be better able to understand patients’ psychological and emotional needs. Therefore, nurses could provide better care and may become more effective at making patients feel comfortable. One of the participants reported as follows: There are other issues like psychological issues, and people get affected [by those things]. It’s not on the health record but they can get affected psychologically, so nurses can definitely get understand their patients better, and they will know other better ways to handle their patients, to make them feel comfortable.
Another participant thought that nurses would learn more about how to interact with different kinds of people by participating in the storytelling project: I think nurses can learn a lot from the patients. If they are one on one, there’s so many things that people normally not so openly talk and share with others. If they are together, the nurses can really learn a lot which could actually improve the services provided.
Participants recognized that nurses also have their own stories to tell. One participant said this program may allow nurses to get benefits by sharing their traumatic stories with their patients: I’m sure an oncology nurse has a lot of stories to tell. I’m sure they definitely been through a lot of difficult situations and have their own traumas, especially working in oncology … so it’s important that they also have to have some outlet … let their voice be heard, and their stories be heard.
Benefits of Online and In-Person Programs
Participants stated their preferences for doing the program online versus in person. As each participant had different preferences, no consensus was reached. Some participants preferred online, and others favored in-person. Reasons for selecting the online format included: (a) giving more confidence to express oneself, (b) convenience, (c) more confidential, and (d) safer from potential infections. The in-person format was thought to be more beneficial for some participants because it allows (a) greater emotional connection and (b) better communication.
Some participants said that online programs could provide a sense of distance while they are talking with others and make it easier to express themselves: “In case of online, maybe sometimes, someone who are more shy and stand-offish? it might be good because just having some distance.” Another person stated “I think the benefit of doing it online is actually, so many people can’t express themselves face-to-face mostly, maybe because of fear of judgment or something.”
One AYA said the online intervention is more convenient and less burdensome: Doing it face-to-face, it may cause some people not to attend because it requires a lot of commitment. Doing online, it is more comfortable and convenient because you don’t need to move, you can just sit down at the time you can meet via Zoom, so it’s easier to do.
Another participant said the online meeting is better for keeping confidentiality: “… when you offer it online, there is some type of confidentiality more than face to face. [Participants] still can get some bond in online, but still they can get some confidentiality.”
We conducted this interview during the COVID-19 pandemic; thus, several AYA responded that the online intervention could be considered an excellent way to protect them from infection: “You know, before with pandemic, I really preferred face-to-face, but since the pandemic, because cancer patients are generally immunocompromised, so I think I prefer online now.”
On the other hand, in-person, face-to-face interactions were thought to allow a greater emotional connection and better communication, especially nonverbally: “And doing it in person, there could be more connections that you can create with the patients. Also, emotions can be evoked.” Another person also said, “Also, I feel like um … the face-to-face is much better because you get to see, actually see the people visually and physically, you get to work with them physically, and it creates connection.”
Willingness to Participate
Several participants talked about how one or more elements of the program make them more willing to participate, which can be another facilitator. Reasons for participation included deeper relationships, social support, information about cancer, and the opportunity to talk about having cancer with someone else. One participant spoke about how the program can allow the development of a greater bond with one of the nurses: I’m comfortable to having this conversation with nurses because I remember that talking to them in a personal level, one on one, that was great. … [When we are in the hospital for the treatment] we get to one nurse today and the following day you don’t have that nurse, but you have a different nurse. This program [can help] you get to know this, one particular nurse for this period of time, you get to bond, she gets to know you, or he gets to know you better, and that’s just great.
Another participant talked about how participation in the program led to closer relationships with nurses, oncologists, and even people outside of health care. Feeling less alone and more connected to others was also viewed as a facilitator for participation in the program: I think if I have learned about this activity at my local cancer clinic, I would’ve been one of the first person who just sign for it [(laughing)]. I think because, it would make me feel less alone and more connected with other people in my age and with my nurses, and it would promote more trusting relationships with my health care team.
More generally, some participants saw social support and a chance to get questions about cancer answered as a benefit of participation. Knowing that they are not alone was also stated as a benefit of participation in the program. They stated, I really want to-, you know, activities like this can bring people together, and people with different thoughts and different ideas can come together and get to learn more. And you get to know that you are not the only one suffering from this, there are other people who are also suffering from this, and the other people are there [to support you], help to fight for their life.
Rather than focusing on relationships, one AYA participated because of an opportunity to talk about the experience of having cancer since there were limited opportunities to talk about this outside of the program: I feel something like this would be interested because, first of all, not so many of us get opportunities to talk with someone or a group of people about how we’ve been feeling, the journey, everything that we’ve been going through. Not so many of us get that opportunities. And this activity will provide that opportunity to many of us.
Discussion
This study was the first step to developing an innovative nurse–patient dyadic storytelling intervention by identifying perceptions of AYA with cancer. Participants’ feedback was mostly positive, and the current intervention program was evaluated as a promising way of promoting positive outcomes among AYA with cancer. Participants expressed their appreciation of the storytelling activity. However, their perceptions of the dyadic storytelling with their primary nurses varied. Most AYA had a good relationship with their nurses; however, they showed mixed responses toward creating and sharing their stories with their primary nurses. Some AYA welcomed the opportunity to share their experience with those they trust, but others shared their concerns about disclosing personal details. In addition, some participants valued the online intervention format because of its convenience and safety, as this interview was conducted under the impact of the COVID-19 pandemic. Others still highlighted the value of in-person interactions.
Their mixed responses may indicate that the intervention requires a flexible, individualized format to fulfill their needs and acknowledge their different preferences. While most participants showed positive reactions to the proposed intervention model, AYA might have each different preferred mode of intervention. Several participants suggested allowing participants to choose their intervention format (e.g. online, in-person), timing (e.g. after the treatment, during the treatment), and partners (e.g. creating stories alone, working with nurses, working with other cancer survivors). Previous studies also showed mixed responses on their preferred intervention delivery methods (Touyz et al., 2019). In a study exploring the preferred types of intervention for young adult cancer survivors, their participants wanted interventions convenient and providing social support (Rabin et al., 2013). Although this population is well known to have high digital technology preference (Abrol et al., 2017), some of our participants emphasized the importance of face-to-face interactions, which are critical to an in-depth understanding of others’ experiences and building meaningful connections. Their preferences for storytelling partners also varied. While our intervention model is tailored to nurse–patient dyads, several participants said they preferred to share their stories with other cancer patients or do it alone. Their mixed responses show that future research should focus on individually tailored, flexible intervention development. To optimize and customize the intervention based on each preference, we may consider multiple factorial experiments and pilot tests of various intervention versions in the future.
The nurse–patient dyadic storytelling intervention model is innovative due to its dyadic nature, especially through collaborations with primary nurses. Dyadic psychosocial interventions using digital mediums were reported to provide positive impacts on individuals with diverse health conditions, including cancer (Luo et al., 2020; Shaffer et al., 2020). While dyadic approaches have been primarily used for patients and their caregivers, our intervention program aims to find a positive interaction between patients and their health care providers, specifically with their primary nurses. Cancer patients at this age often struggle between desired independence, which is a common developmental need, and the inevitable reliance on their parents during treatment (Cameron et al., 2019). Having a meaningful interaction with reliable people other than their parents and family may expand their self-identity and provide more independence as well as social support (Hedstrom et al., 2004; Hotchkiss et al., 2022). Oncology nurses often foster strong relationships with this young population and their families (Conte, 2014), which can be an excellent psychosocial asset for the patients (Hedstrom et al., 2004). Despite the provisional benefits and few existing models explaining the interdependence between the clinician–patient dyad (Turcotte et al., 2019), dyadic relationships and interdependence between a patient and a health care provider is still an understudied area compared to the dyadic health studies between a patient and their family members such as married couples or parent–child dyads.
Our intervention could be more advantageous compared to one-sided storytelling programs because it can provide mutual benefits to both AYA and nurses. Nurses caring for young cancer patients often have to deal with high emotional and moral stress, work-related loss and grief, self-doubt, and ethical dilemmas (Conte, 2014; Hecktman, 2012). Some participants reported nurses could gain from this program as they can get better knowledge and understanding of their patients. The experience of meaningful recognition and an empathetic connection with patients can reduce nurses’ moral distress and enhance their professional quality of life (Cherven et al., 2020; Kelly et al., 2015). Narrative nursing is a patient-centered, relationship-focused approach; through stories, nurses can learn to recognize the unique value of their own experiences and to understand the lives and perspectives of patients, their families, and colleagues (Artioli et al., 2016; Fitzpatrick et al., 2019). The unique nurse–patient relationship and its mutual benefits can be explained by the Synergy Model, highlighting that a nurse's competencies are rooted in a patient's needs (Curley, 1998; Curley, 2007). When their characteristics match, synergy arises and leads to optimal outcomes for both patient and nurse (Curley, 1998; Curley, 2007). When Coats et al. (2020) developed and tested an intervention incorporating patient narratives into their electronic health record, patients’ primary nurses exhibited high levels of satisfaction and reported that reading these stories enhanced their connections and communication with patients. However, a nurse–patient dyadic approach has rarely been applied to intervention research for AYA with cancer, which indicates the need for future research. Furthermore, only a few dyadic intervention research reported the outcomes of the individuals with supporting roles (Shaffer et al., 2020). To understand nurses’ perspectives, further research should be conducted with oncology nurses and explore their perceived benefits of this intervention.
Despite the probable advantages and the AYA participants’ willingness to join, we should consider potential challenges. Logistics of this intervention can bring unintentional risks to AYA with cancer and nurses, including privacy and confidentiality problems, psychosocial and emotional burdens on each side, institutional and systemic issues (e.g. incentives or payments to participated nurses, on-duty or off-duty participation), or potential legal problems. While this intervention may bring advantages to oncology nurses, developing a deeper relationship with their patients can intensify their grief and work-related loss (Conte, 2014). Institutional efforts should follow to minimize nurses’ burden and protect their privacy while they engage in such holistic care. We will continue to establish appropriate support and protection strategies for both participant groups in our future studies.
Limitations
Although our age criteria of eligible participants were 12–24 years, all recruited participants were young adults. We used private cancer foundations, a hospital AYA oncology program, social media (e.g. Facebook), and ResearchMatch for recruitment. Adolescents may have limited access to such advertisements. And minor participants interested in this study had to ask their parents to contact us and provide consent first, which became another barrier to participation. We will consider adolescent-tailored recruitment strategies for our subsequent study.
Because all participants were recruited from online platforms, we could not access their medical records and had to rely on their self-reported information. This limitation may allow some study applicants to misrepresent their information, a common drawback of online recruitment strategies (Glazer et al., 2021). During the study, we found that the demographic and clinical information differed in the answers provided by two participants to the eligibility screening survey. One interview participant constantly provided irrelevant answers to our cancer-related questions. After a thorough discussion, we excluded the interview from the data after reporting to the Institutional Review Board because we could not guarantee that this participant was an actual cancer survivor. Such events showed the possibility of eligibility fraud by study applicants, which can create bias in the findings and damage the integrity of the entire study and data quality (Glazer et al., 2021). We will consider applying additional screening strategies for our next online recruitment, including a secondary screening and using identity verification or fraud reduction tools (Glazer et al., 2021).
Our future study should also investigate nurses’ feedback on the dyadic storytelling intervention while the current study focused on the feedback from AYA with cancer only. Even though this intervention could bring benefits to nurses, there could be several drawbacks from nurses’ perspectives such as time limitation, additional workload, and emotional burden. In addition, there is no guarantee that their willingness to participate presented in this study would lead to actual intervention participation. Thus, further postintervention evaluations should be conducted to identify its feasibility, acceptability, recruitment and retention rates, and additional barriers or facilitators. Finally, this study was performed under the impact of the COVID-19 pandemic. Therefore, the global health crisis could impact participants’ perceptions of online and in-person programs. For example, some participants said they prefer an online program because it is safe. Their preferences could be different if they were not under the potential infection risk.
Implications for Holistic Nursing Research, Education, and Practice
Our study shows several holistic implications for future nursing research, practice, and education. Importantly, future research can further explore dyadic intervention approaches, which have been mostly implemented on a family basis. While the family-focused care model is ideal for pediatric oncology patients, AYA with cancer tend to have different needs compared to younger children, characterized by the various levels of maturity and independence (Ferrari et al., 2010). Our study suggests that dyadic approaches can be considered between AYA cancer patients and oncology care providers outside their immediate family. Oncology nurses develop and maintain uniquely solid bonds and close relationships with their patients and their families because those nurses meet young patients often and for a prolonged period (Conte, 2014). Our findings may indicate that those nurses can play a wide range of integrative roles in the oncology clinical settings. Eventually, our current and future studies will suggest a nurse's potential for holistic care while interacting with AYA with cancer in various settings.
Our study also indicates that AYA with cancer has a vital need to create and share their unique stories. Nurses should be ready to engage and provide such opportunities through holistic care. However, the current nursing curriculum tends to focus on knowledge (i.e. cognitive domain) and skill development (i.e. psychomotor domain) rather than affective domains, which provide formal opportunities to develop students’ attitudes, values, and motivations toward holistic, person-centered nursing care (Day et al., 2017; Miller, 2010). Hence, students often have limited ability in communicating and creating meaningful relationships with individuals that have complex health issues. The current study findings emphasize the core values of nursing, such as caring and presence, which are familiar to all nurses but often lack priority in the busy clinical field. Nursing educators can consider integrating narrative nursing into the core curriculum to cultivate holistic capacities in nurses.
Conclusion
Our study showed that AYA with cancer are interested in storytelling activities to share their experience and perceive dyadic storytelling with nurses can bring potential psychosocial benefits. However, the study showed that it was difficult to reach a consensus as they have diverse opinions and preferences. Therefore, future research will focus on optimizing and customizing the intervention tailored to the needs of AYA with cancer.
Supplemental Material
sj-docx-1-jhn-10.1177_08980101231189392 - Supplemental material for Perspectives From Adolescent and Young Adult Cancer Survivors for a Planned Nurse–Patient Dyadic Storytelling Intervention
Supplemental material, sj-docx-1-jhn-10.1177_08980101231189392 for Perspectives From Adolescent and Young Adult Cancer Survivors for a Planned Nurse–Patient Dyadic Storytelling Intervention by Eunji Cho and Terrah Foster Akard in Journal of Holistic Nursing
Footnotes
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.