
Abstract
Opioid receptors are distributed throughout the central and peripheral nervous systems and on many nonneuronal cells. Therefore, opioid administration induces effects beyond analgesia. In the enteric nervous system (ENS), stimulation of µ-opioid receptors triggers several inhibitory responses that can culminate in opioid-induced bowel dysfunction (OBD) and its most common side effect, opioid-induced constipation (OIC). OIC negatively affects patients’ quality of life (QOL), ability to work, and pain management. Although laxatives are a common first-line OIC therapy, most have limited efficacy and do not directly antagonize opioid effects on the ENS. Peripherally acting µ-opioid receptor antagonists (PAMORAs) with limited ability to cross the blood-brain barrier have been developed. The PAMORAs approved by the U S Food and Drug Administration for OIC are subcutaneous and oral methylnaltrexone, oral naloxegol, and oral naldemedine. Although questions of cost-effectiveness and relative efficacy versus laxatives remain, PAMORAs can mitigate OIC and improve patient QOL. PAMORAS may also have applications beyond OIC, including reducing the increased cardiac risk or potential tumorigenic effects of opioids. This review discusses the burden of OIC and OBD, reviews the mechanism of action of new OIC therapies, and highlights other potential opioid-related side effects mediated by peripheral opioid receptors in the context of new OIC therapies.
Introduction
Opioid agonists are commonly used for the treatment of moderate to severe chronic cancer and noncancer pain, owing to their analgesic actions, 1 mostly at µ-opioid receptors. Opioid receptor locations in the periphery include lung, spleen, kidney, heart, skeletal muscle, cartilage, synovium, periosteum, tendon, bone, liver, thymus, enteric neurons of the gastrointestinal (GI) system, pancreas, adrenal gland, and dorsal root ganglion (Table 1). 2 –5 The diverse central nervous system (CNS) and peripheral nervous system (PNS) locations of the µ-opioid receptors in particular contribute to the respective side effect profiles of opioid drugs. Due to the distribution of µ-opioid receptors in the enteric nervous system (ENS), a common and significant consequence of opioid therapy is opioid-induced bowel dysfunction (OBD), which is most often characterized by opioid-induced constipation (OIC), 6 –9 along with decreased appetite, increased reflux, nausea, and vomiting. 6,10 Studies in rats have shown that concentrations of systemically administered morphine are considerably higher in the GI tract than in the CNS, and GI concentrations correlate directly with inhibition of GI transit. 11 In addition, evidence from studies comparing the effects of central and systemic administration of morphine in rats suggests that CNS opioid receptors may have some influence on GI transit as well. 12 The interaction of opioids with µ-opioid receptors in the ENS of the GI tract induces multiple effects that lead to impaired GI motility, including slowing GI transit, promoting nonpropulsive motility and segmentation, and promoting contraction of the sphincters. 13,14 The increase in GI transit time, along with the opioid-induced stimulation of mucosal sensory receptors, results in enhanced fluid reabsorption, which further promotes constipation. 13,14
Locations and Inferred Functions of Opioid Receptor Subtypes.
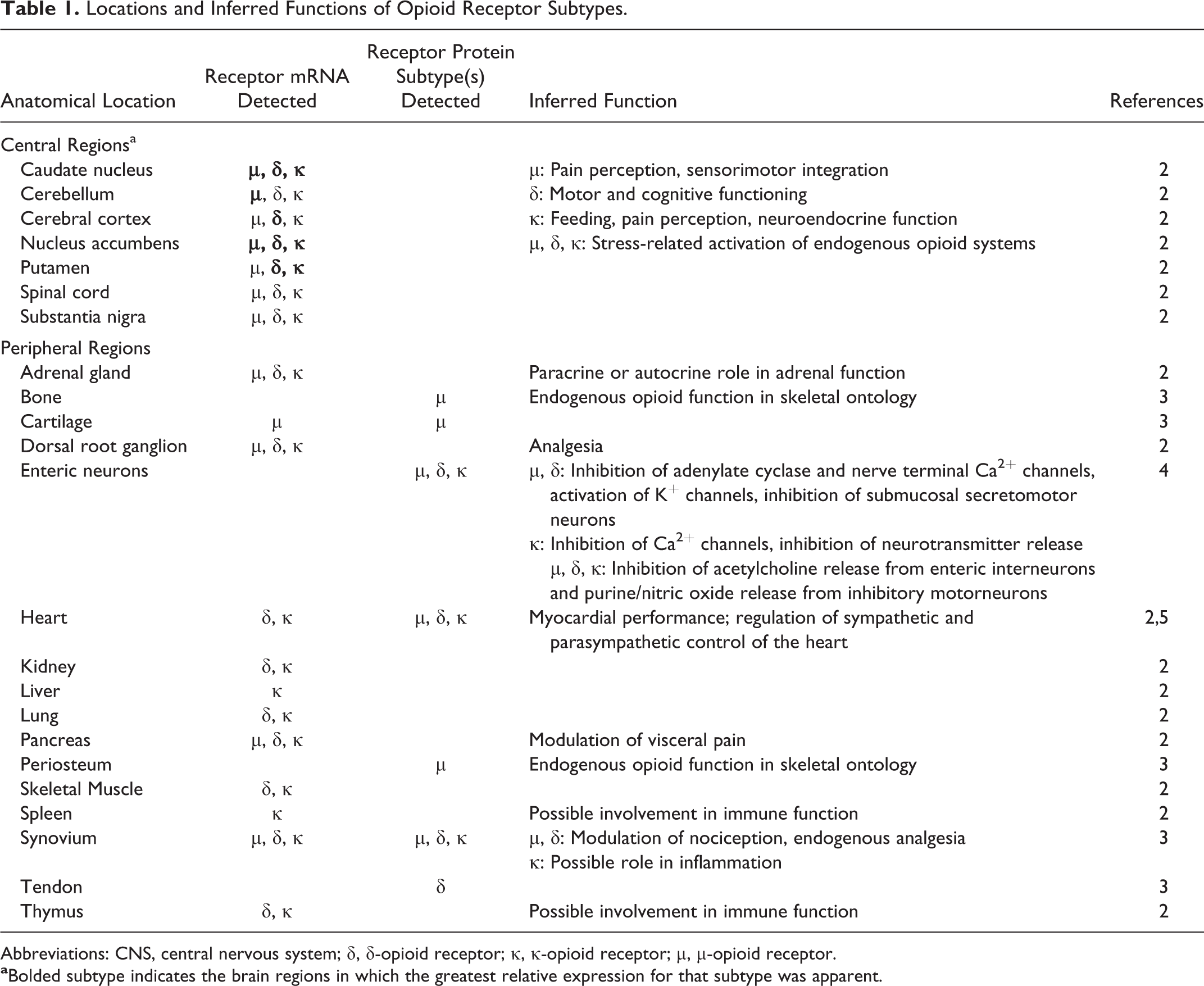
Abbreviations: CNS, central nervous system; δ, δ-opioid receptor; κ, κ-opioid receptor; µ, µ-opioid receptor.
A consensus definition for OIC is lacking. 15 Although not specific to OIC, the American College of Gastroenterology definition of constipation includes infrequent bowel movements and challenges with passing stool (eg, straining and/or incomplete evacuations). The Rome III criteria define functional constipation by the presence of multiple constipation symptoms, including less than 3 bowel movements per week and/or straining, lumpy or hard stools, a feeling of incomplete evacuation and/or anorectal blockage, or manual maneuvers during at least one-quarter of bowel movements. 13,16 There are several tools that can be used to assess the severity of symptoms of OIC and evaluate response to treatment, including the following: the Patient Assessment of Constipation, a 12-item questionnaire that evaluates 3 key areas of OIC (stool characteristics, rectal symptoms, and abdominal symptoms) 17 ; the Bowel Function Index (BFI), a 3-item questionnaire that evaluates the ease of bowel movements, feelings of incomplete evacuation, and patient-rated constipation 18 ; and the bowel function diary, which evaluates multiple constipation-related domains, including frequency and difficulty of bowel movements and medication use. 13,19
Due to the negative impact of OIC on pain relief, patient quality of life (QOL), and health-related outcomes, effective treatments of OIC are needed. Although evidence supporting the management of OIC with laxatives (stool softeners, osmotic agents, and stimulant laxatives) is limited, 10 several guidelines endorse laxatives as a first-line treatment of OIC. 20 –22 Additional prospective studies of laxatives versus alternative treatments, including new targeted therapies, may result in the revision of these guidelines for more effective management of OIC. The objectives of this article are to discuss the burden of illness of OIC and OBD, to provide an overview of the mechanism of action of new OIC therapies from basic science and clinical perspectives, and to highlight other potential opioid-related side effects mediated by peripheral opioid receptors and the potential effect of new OIC therapies on them.
Burden of Illness
OIC is highly prevalent among patients receiving opioids for cancer pain and chronic noncancer pain. Furthermore, unlike other opioid-related side effects, patients typically do not develop a tolerance to OIC over time with continued opioid use. 13 In a survey of more than 2000 patients receiving opioids for chronic noncancer pain, the prevalence of OIC was 57% overall and ranged from 17% to 67% depending on the particular opioid used (codeine, hydrocodone, propoxyphene, morphine, oxycodone, or tramadol). 9 In an analysis of 8 trials of patients with chronic noncancer pain receiving opioid treatment for up to 8 weeks, OIC was reported by 41% of patients. 7 That analysis determined that the number needed to harm was 3.4 (95% confidence interval, 2.9-4.0), meaning that for every 3 patients treated with opioids, 1 more would have constipation versus those treated with placebo. 7 A study of patients receiving opioids for cancer pain found that 62% had Knowles Eccersley Scott Symptom constipation scores from 9 to 39 points, indicating a problematic level of constipation. 6 In an online survey of patients with OIC, at least 80% of participants would like to improve the following aspects of constipation: the ability to have a pain-free bowel movement or to produce a soft (not loose or watery) stool, to worry less about performing a bowel movement, to experience no rectal straining due to constipation, to feel less bloated or to have less stomach pain, and to be more comfortable using opioid medication without fear of constipation. 23 The symptoms common to OBD and OIC that have been reported at a prevalence of ≥20% in patients with chronic pain are summarized in Table 2. 6,9,24,25
Common Symptoms of OBD and OIC Reported at ≥20% Frequency Among Patients Using Opioids for the Treatment of Chronic Pain.
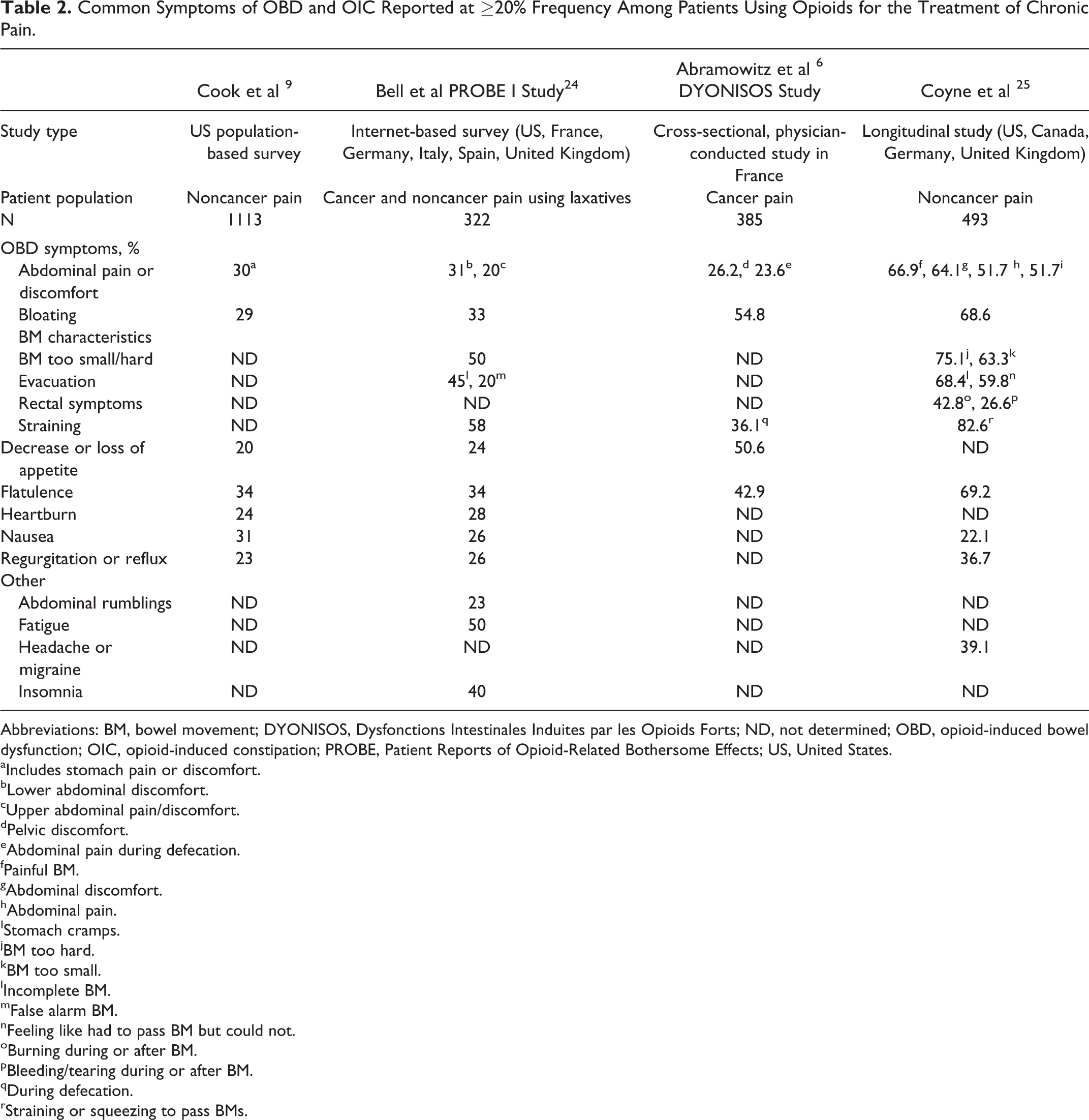
Abbreviations: BM, bowel movement; DYONISOS, Dysfonctions Intestinales Induites par les Opioids Forts; ND, not determined; OBD, opioid-induced bowel dysfunction; OIC, opioid-induced constipation; PROBE, Patient Reports of Opioid-Related Bothersome Effects; US, United States.
aIncludes stomach pain or discomfort.
bLower abdominal discomfort.
cUpper abdominal pain/discomfort.
dPelvic discomfort.
eAbdominal pain during defecation.
fPainful BM.
gAbdominal discomfort.
hAbdominal pain.
IStomach cramps.
jBM too hard.
kBM too small.
lIncomplete BM.
mFalse alarm BM.
nFeeling like had to pass BM but could not.
oBurning during or after BM.
pBleeding/tearing during or after BM.
qDuring defecation.
rStraining or squeezing to pass BMs.
OBD and OIC negatively affect patient QOL and activities of daily living. Almost all (93%) patients taking opioids for cancer pain who had constipation reported that their OBD symptoms affected their QOL, and 38% rated the effect as moderate to severe. 6 The difference in QOL between patients with and without constipation was significant, as measured by both the condition-specific Patient Assessment of Constipation–Quality of Life (PAC-QOL) and the generic Short Form-12 questionnaires. 6 In the Patient Reports of Opioid-related Bothersome Effects (PROBE) I study (a multinational Internet study to assess OBD), more than half of the patients who reported constipation, passing gas, and bloating noted that these symptoms had a moderate to great or great effect on their QOL. 24 Abdominal pain, bloating, passing gas, reflux, and heartburn were also reported to have a moderate to great or great effect on patient activities of daily living. 24 In a multicountry longitudinal study by Coyne and colleagues, patients with OIC had a lower QOL compared with others with chronic pain alone or other chronic conditions, 38% reported impairment in daily activities, and, of those who were employed, 9% missed work and 32% reported impairment while working due to OIC. 25
OIC may also interfere with pain management. Multiple studies have documented that patients may lower the dose of, switch, or stop taking their opioid medication to ameliorate their GI symptoms, which may in turn compromise pain control. 6,9,23 –25 However, constipation often occurs with opioid doses lower than those required for analgesia, so lowering the dose is generally not effective for managing OIC. 13 Although dose reduction to alleviate OIC is not typically feasible, switching opioids may reduce the symptoms of OIC in some patients. 13 Other nonpharmacologic methods of managing constipation, including increasing physical activity and fiber intake, have not been proven to be beneficial in patients with OIC but could offer some relief of symptoms. 13
Shortcomings of OIC Treatment With Laxatives
Although laxatives are often used as first-line therapy to treat OIC, they do not address the underlying pathophysiologic mechanism, because they do not oppose opioid actions at enteric opioid receptors. 8 Laxatives have not been well studied in randomized, controlled trials, 26 but published data from patient surveys suggest that most laxatives are not very effective for OIC. 6,8,9,24,25 In a survey by Bell et al of patients with chronic noncancer pain or cancer-related pain who were taking laxatives as well as opioids, 81% reported persistent constipation. 24 Abramowitz and colleagues showed that in patients receiving strong opioids for cancer pain, even though 84.7% were taking laxatives, 85.7% were considered by physicians to be constipated. 6 In a study by Rosti et al of patients receiving analgesics for chronic pain, the majority of which were strong opioids, 63.5% had OBD symptoms despite the fact that 89.5% of those who reported OBD symptoms were taking laxatives. 27 In a multicountry longitudinal study of patients with chronic noncancer pain taking opioids and experiencing OIC, the majority of whom were taking laxatives, Coyne and colleagues found that more than half reported dissatisfaction with their constipation treatment, and most who reported any benefit of their OIC treatment reported it provided little benefit. 25 Patient-reported achievement of the desired outcome at least half of the time with laxatives was 46% in 1 study, 8 and patient dissatisfaction with laxatives was reported by ∼25% of patients in another. 9 Because OIC is associated with a high burden of disease, cross-comparisons of the effectiveness of laxatives versus the newer, peripherally acting µ-opioid receptor antagonists (PAMORAs) in prospective placebo-controlled trials are needed.
Targeted Treatment of Opioid-Induced Constipation
PAMORAs were developed to address the need to block the GI actions of opioids in the periphery while not affecting their CNS actions, thereby directly targeting the mechanism of OIC. The first PAMORAs approved by the US Food and Drug Administration (FDA) were subcutaneous methylnaltrexone, which was initially approved for OIC in adult patients with advanced illness and later in adult patients with chronic noncancer pain, and alvimopan, which is indicated for accelerating the time to upper and lower GI recovery following surgeries that include partial bowel resection with primary anastomosis. 28 –30 Naloxegol was then approved in September 2014 for the treatment of OIC in adult patients with chronic noncancer pain. 31 Naldemedine was approved in March 2017 for the treatment of OIC in adult patients with chronic noncancer pain. 32
Mechanism of Action of PAMORAs
PAMORAs block opioids from binding to peripheral µ-opioid receptors, with the goal of restoring ENS function. Although PAMORAs may compete with opioids for µ-opioid receptor binding throughout the body, the desired therapeutic mechanism of action involves selective, competitive binding of the drug to enteric µ-opioid receptors (Figure 1). 33 The initial strategy in the drug development process was to investigate the use of the µ-opioid receptor antagonist naloxone for the treatment of OIC. 34,35 In a dose-ranging study, oral naloxone was given to patients with advanced cancer and OIC who were receiving morphine for pain control. 34 Naloxone at doses that were ≥20% of the morphine dose provided a clinically significant laxative effect in 9 of 12 patients, but 2 patients experienced generalized withdrawal reactions, 1 of whom also had a return of pain. 34 In a subsequent pilot study, administration of low-dose oral naloxone (2 or 4 mg) 3 times per day to patients with OIC increased the frequency of bowel movements from baseline in all patients; however, 3 of 6 patients experienced reversal of analgesia. 35 The mixed results in those trials led investigators to pursue this approach with modifications to keep agents from crossing the blood-brain barrier (BBB), which led to the development of PAMORAs.
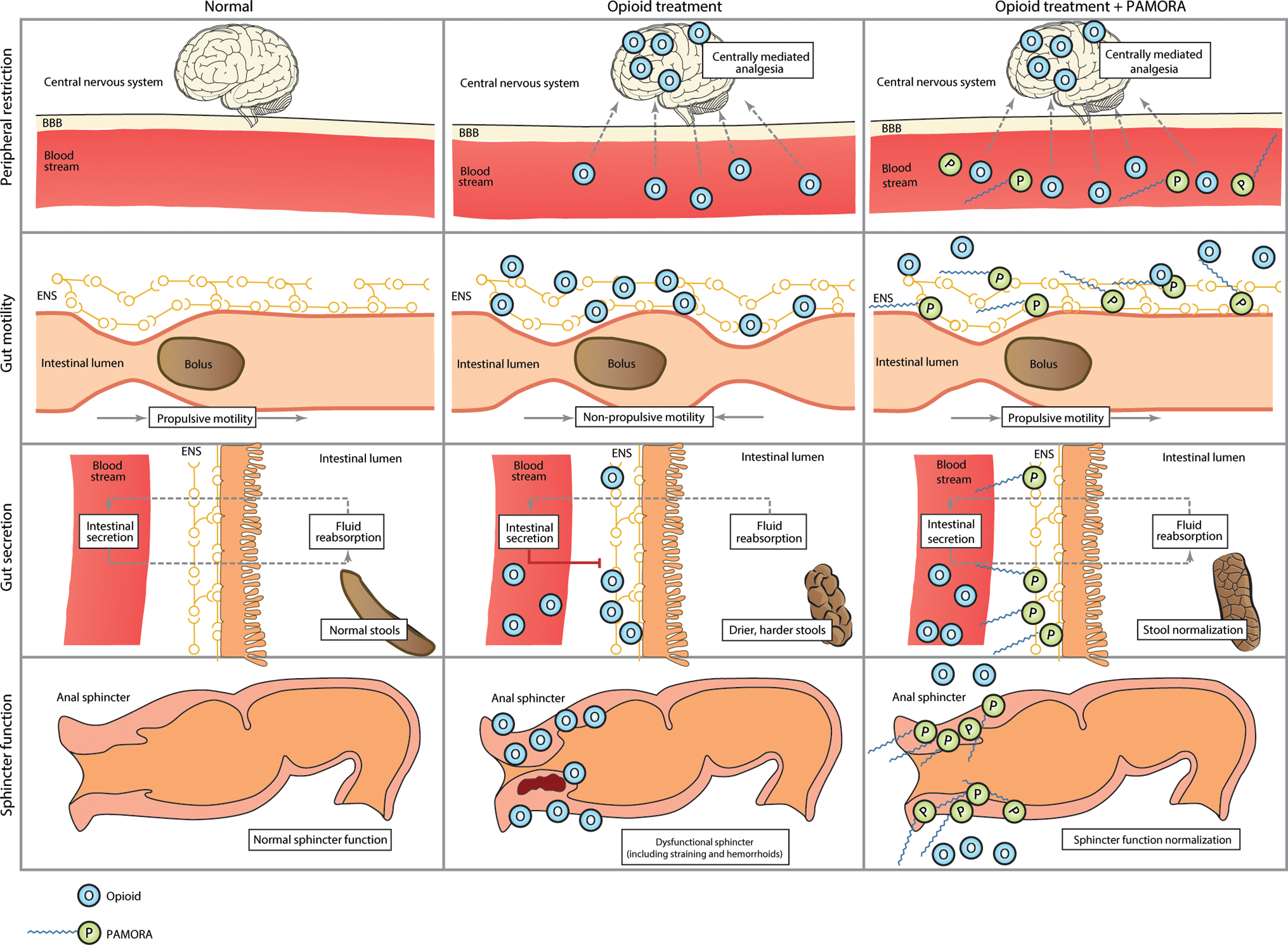
Mechanism of action of PAMORAs in the GI tract. 33 Normal GI activity is shown in the left column, the action of opioids in the GI tract is shown in the middle column, and the action of naloxegol in the GI tract is shown in the right column. The first row shows opioids crossing the blood-brain barrier from the blood stream, while naloxegol is restricted to the periphery and thus does not cross the blood-brain barrier or alter centrally mediated analgesia. The second row shows the interaction of opioids with µ-opioid receptors in the enteric nervous system, leading to nonpropulsive motility. Naloxegol has a higher affinity for these receptors and, by displacing opioids, can restore normal motility. The third row shows the impact of opioids on secretion of electrolytes and water into the intestinal lumen, leading to dry, hardened stools. Naloxegol counteracts the opioid-induced reduction in intestinal secretion, resulting in softer stools. The fourth row shows the impact of opioids on the sphincter and restoration of sphincter function through the action of naloxegol. GI indicates gastrointestinal; PAMORA, peripherally acting µ-opioid receptor antagonists. (Adapted with permission from Poulsen JL et al. 33 )
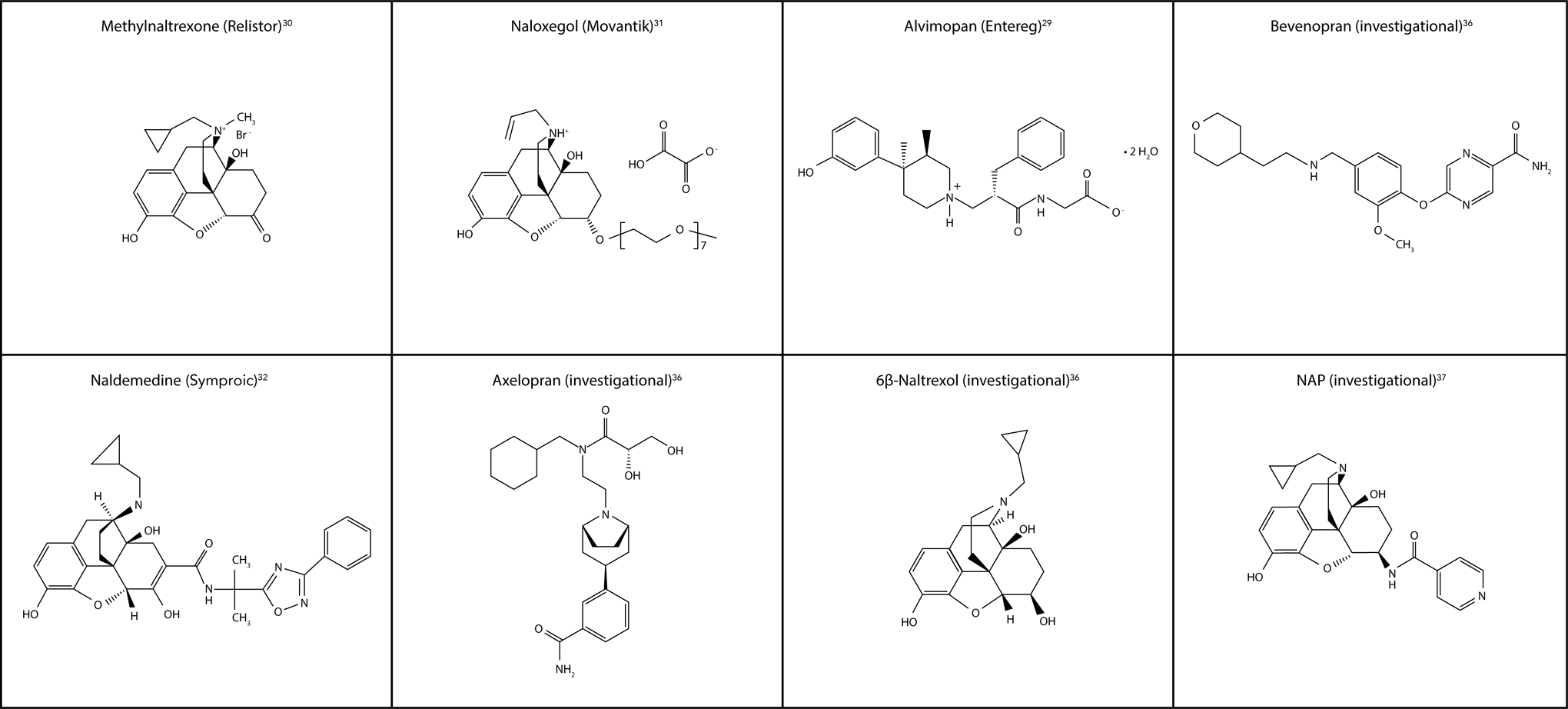
With PAMORAs, entry to the CNS is restricted as the result of various molecular properties or modifications that alter their ability to cross the BBB. Figure 2 shows the chemical structures of approved and investigational agents and the modifications that restrict them to the periphery. 29 –32,36,37 Methylnaltrexone is a quaternary amine with a positive charge on the nitrogen that increases its polarity and water solubility, reducing its ability to cross the BBB. 30 However, the quaternary amine structure has a significant effect on its µ-opioid receptor binding affinity, 38 such that higher doses are required, increasing the risk of possible side effects. Naloxegol is a pegylated form of naloxone 31 and is covalently conjugated with polyethylene glycol. This increases its molecular weight, making the amount of naloxegol that crosses the BBB negligible, while maintaining its µ-opioid receptor affinity. 31 The pegylation of naloxegol also results in it becoming a substrate for the P-glycoprotein (PGP) efflux transporter, 31 similar to therapeutic doses of the antidiarrheal opioid agent loperamide, which lacks CNS effects because it is subject to efflux by PGP. 39 PGP effectively pumps loperamide and naloxegol out of the CNS so that pharmacologically active concentrations are not reached. 31,39 Naldemedine is a derivative of naltrexone with an additional side chain that results in increased polar surface area and molecular weight; this side chain reduces the ability of naldemedine to cross the BBB. 32 Similar to naloxegol, naldemedine is a substrate of the PGP efflux transporter. 32
In theory, PAMORAs may be associated with therapeutic and/or withdrawal-like laxation, diarrhea, or other peripheral effects. No clinically significant opioid withdrawal has been observed in studies of PAMORAs approved for OIC. 40 –43 In addition to their therapeutic effect for reducing OIC, it is possible that blockade by PAMORAs may decrease the incidence of opioid-mediated adverse events (AEs) in other tissues, including cardiac tissue.
Efficacy and Safety of FDA-Approved PAMORAs for OIC
Three of the 4 available PAMORAs are approved by the FDA for OIC, and their efficacy, safety, and dosing schedules are summarized here.
Methylnaltrexone
Subcutaneous methylnaltrexone (Relistor®; Salix Pharmaceuticals, Inc., Raleigh, North Carolina) is indicated for the treatment of OIC in patients receiving palliative care for advanced illness with insufficient response to laxatives (Table 3), and was approved for the treatment of OIC in patients with chronic noncancer pain in September 2014. In addition, oral methylnaltrexone was approved for the treatment of OIC in patients with chronic noncancer pain in July 2016. 30 Subcutaneous methylnaltrexone is administered as an every-other-day injection (0.15 mg/kg for patients <38 or >114 kg; 8 mg for patients ≥38 to <62 kg; 12 mg for patients ≥62 to 114 kg) in patients with advanced illness receiving palliative care and as a once-daily injection (12 mg) in patients with chronic noncancer pain. Oral methylnaltrexone is administered as a once-daily tablet (450 mg) in the morning. 30 In patients with moderate and severe renal impairment (creatinine clearance [CLcr] <60 mL/min) and those with moderate or severe hepatic impairment, the following reduced dosing is recommended: in patients with advanced illness, an every-other-day subcutaneous injection (0.075 mg/kg for patients <38 or >114 kg; 4 mg for patients ≥38 to <62 kg; 6 mg for patients ≥62 to 114 kg); and in patients with chronic noncancer pain, a subcutaneous injection of 6 mg once daily or a 150 mg oral tablet once daily. 30
Indications, Dosing, and Formulations for FDA-Approved PAMORAs for OIC.
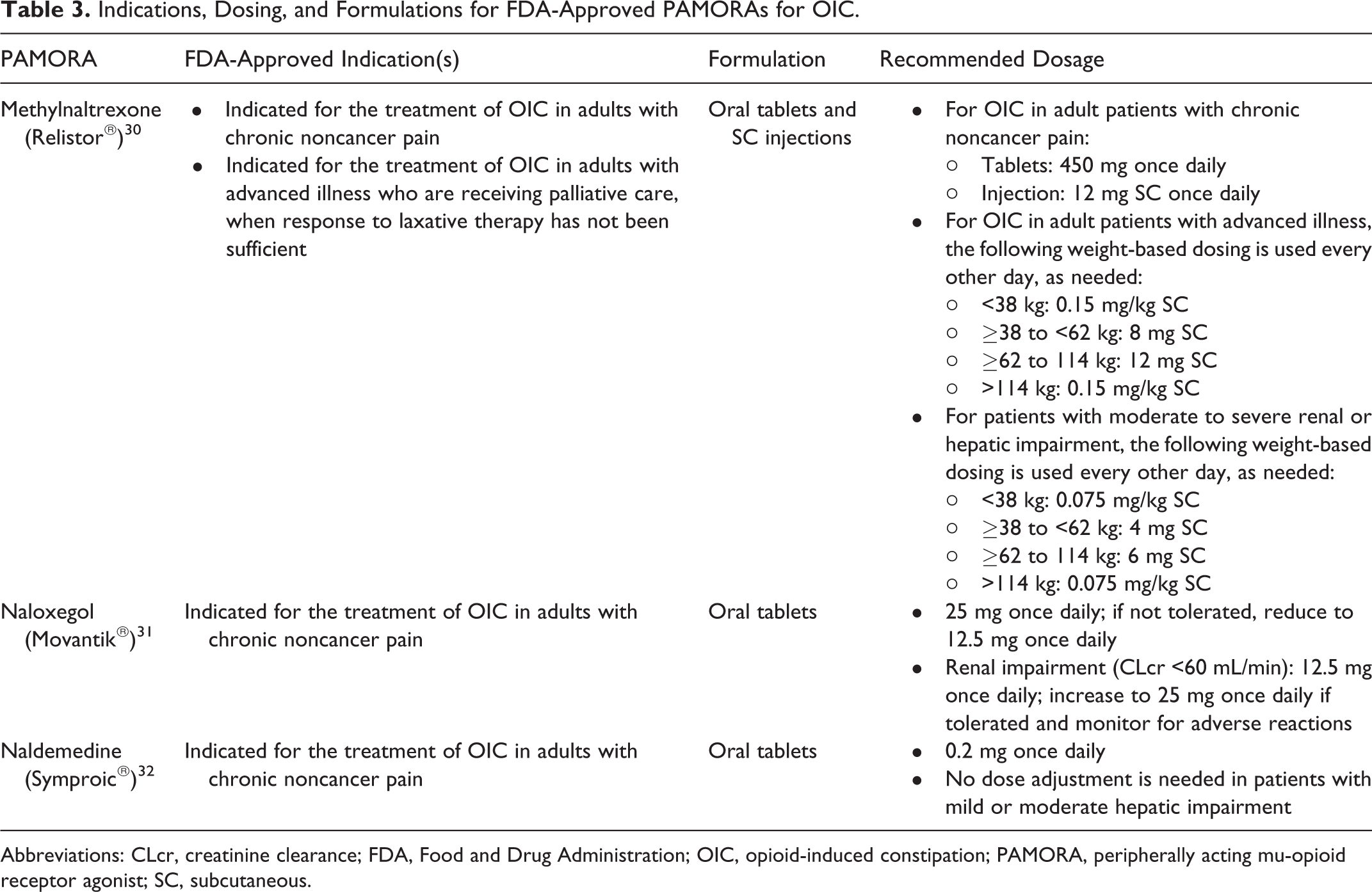
Abbreviations: CLcr, creatinine clearance; FDA, Food and Drug Administration; OIC, opioid-induced constipation; PAMORA, peripherally acting mu-opioid receptor agonist; SC, subcutaneous.
The efficacy and safety of subcutaneous methylnaltrexone was investigated in 2 randomized, double-blind, placebo-controlled, phase 3 clinical trials in patients with advanced illness receiving palliative care and OIC, and 1 randomized, double-blind, placebo-controlled, phase 3 trial in patients with noncancer pain and OIC. 41,44,45 In 1 trial, 154 patients with advanced illness receiving palliative care were given a single dose of methylnaltrexone 0.15 or 0.30 mg/kg or placebo. 41 The primary end point was laxation within 4 hours of drug administration. 41 Patients could then enter a 28-day open-label phase to receive methylnaltrexone as needed (starting dose, 0.15 mg/kg) as often as every 24 hours, followed by the option to continue in a 3-month extension. 41 The primary end point was achieved by 62%, 58%, and 14% of patients who received a single dose of methylnaltrexone 0.15 mg/kg, methylnaltrexone 0.30 mg/kg, and placebo, respectively (P < .0001 for both doses vs placebo). The median time to rescue-free laxation (spontaneous bowel movement [SBM] without interventions such as laxatives) was 1.10, 0.8, and >24 hours in these respective groups (P < .0001 for both doses vs placebo). 41 Almost all patients (97%) continued to the open-label phase, and 54% of those who had previously received placebo achieved laxation within 4 hours of administration of the first open-label dose of methylnaltrexone. 41 The most common AEs that occurred more frequently with methylnaltrexone than placebo were abdominal pain and flatulence. 41 No patient had a significant change in baseline pain score or experienced opioid withdrawal. 41 In this population of patients with advanced illness, the response to methylnaltrexone may have been lower due to the contribution of other nonopioid-related mechanisms to constipation, including reduced fiber intake or immobility. 41 Furthermore, the rate of AEs in the palliative care population was fairly high, and determining the relationship of these AEs to the administered study agent or to the advanced illness was challenging. 41 Nevertheless, this randomized, placebo-controlled study showed that methylnaltrexone was effective for rapidly inducing laxation in this palliative care population and was well tolerated. 41
In the other trial, 134 patients with advanced illness receiving palliative care were given subcutaneous methylnaltrexone (0.15 mg/kg) or placebo every other day for 2 weeks, after which they could opt to continue in a 3-month, open-label extension trial to receive drug as needed up to every 24 hours. 44 The coprimary end points were rescue-free laxation within 4 hours after the first dose and within 4 hours after 2 or more of the first 4 doses. 44 Rescue-free laxation within 4 hours after the first dose was achieved by 48% and 15% of patients who received methylnaltrexone and placebo, respectively, and rescue-free laxation within 4 hours after 2 or more of the first 4 doses was achieved by 52% and 8% of patients in these respective groups (P < .001 vs placebo for both comparisons). 44 The median time to rescue-free laxation was 6.3 hours with methylnaltrexone and >48 hours with placebo (P < .001 vs placebo). 44 The most common AEs that occurred more often with methylnaltrexone than placebo were abdominal pain and flatulence. 44 Minimal changes from baseline pain score occurred over time, and no patient experienced withdrawal. 44 The population included in this study was patients with advanced illness who were constipated at baseline despite laxative treatment (median, 2 classes of laxatives). 44 These patients could have responded to a change in their baseline laxative treatment and, thus, did not represent a population that had failed optimal laxative therapy. Furthermore, approximately half of the patients included in this study did not respond to the first dose of methylnaltrexone. 44 As in the former study, this population could have had other contributing factors to their constipation, which would have reduced the response to methylnaltrexone. 44 This randomized, placebo-controlled study showed that methylnaltrexone was associated with rapid laxation in these patients, with no effects on analgesia or evidence of opioid withdrawal. 44
In a trial of 460 patients with noncancer pain and OIC, subcutaneous methylnaltrexone 12 mg or placebo was given once daily or every other day for 4 weeks. 45 The coprimary end points were rescue-free laxation within 4 hours after the first dose and active injections per patient resulting in rescue-free laxation within 4 hours. 45 Rescue-free laxation within 4 hours after the first dose was achieved by 33%, 35%, and 10% of patients who received methylnaltrexone every day, methylnaltrexone every other day, and placebo, respectively, and the percentage of active injections resulting in rescue-free laxation within 4 hours was 29%, 30%, and 9% of patients in these respective groups (P < .001 vs placebo for all comparisons). 45 The median time to laxation was significantly shorter with both schedules of methylnaltrexone versus placebo (P < .001). 45 The most common AEs that occurred more often with methylnaltrexone than placebo were abdominal pain, diarrhea, nausea, and hyperhidrosis. 45 No clinically significant change from baseline in pain intensity or clinically meaningful evidence of withdrawal was found. 45 Evaluation of the benefits of subcutaneous methylnaltrexone on QOL with the PAC-QOL at baseline and end of study showed a mean improvement of 33% with daily methylnaltrexone, 27% with every-other-day methylnaltrexone, and 18% with placebo (P < .001, daily vs placebo; P = 0.014, every other day vs placebo). 45 The double-blind treatment period in this study was only 4 weeks, which is relatively limited considering the long-term management needed for OIC in patients with chronic, noncancer pain. 45 In addition, no upward titration of opioid analgesics was anticipated in this trial; in a clinical setting, patients could require an increase in their opioid dose to manage worsening pain. 45 Results of this randomized, placebo-controlled study indicate that methylnaltrexone was effective and well tolerated for addressing OIC in patients with chronic noncancer pain. 45
The efficacy and safety of oral methylnaltrexone were demonstrated in a randomized, double-blind, placebo-controlled study of 401 patients with chronic noncancer pain and OIC. Patients received oral methylnaltrexone 450 mg (n = 200) or placebo (n = 201) once daily for 4 weeks, after which treatment was given on an as-needed basis (no more than once daily) for an additional 8 weeks. Treatment response was defined as ≥3 SBMs per week, with an increase of at least 1 SBM per week over baseline for ≥3 of the first 4 weeks. The response rate was 52% with oral methylnaltrexone and 38% with placebo. Abdominal pain and diarrhea were the most common AEs with oral methylnaltrexone. 19 In this study and the above-described studies in patients with advanced illness or chronic noncancer pain and OIC, 41,44,45 methylnaltrexone was not compared directly with other first-line treatments such as laxatives.
Naloxegol
Naloxegol (Movantik®; AstraZeneca Pharmaceuticals LP, Wilmington, Delaware) is an orally administered PAMORA that was approved in September 2014 for the treatment of OIC in patients with chronic noncancer pain (Table 3). Naloxegol is administered orally as a once-daily tablet at a recommended dose of 25 mg. 31 In patients with moderate, severe, or end-stage renal disease (CLcr <60 mL/min), a dose of 12.5 mg once daily is recommended as the starting dose; the dose can be increased to 25 mg once daily if well tolerated. 31
The efficacy and safety of naloxegol were evaluated in 2 identically designed, pivotal, randomized, double-blind, placebo-controlled, phase 3 clinical trials in outpatients with noncancer pain and OIC. 40 Patients were given naloxegol 25 mg, naloxegol 12.5 mg, or placebo once daily for 12 weeks. 40 The primary end point was response rate, with response defined as ≥3 SBMs per week and an increase of ≥1 SBM over baseline for ≥9 of the 12 weeks of treatment and ≥3 of the last 4 weeks of treatment. 40 In the first study (N = 652), the response rates were 44.4%, 40.8%, and 29.4% with naloxegol 25 mg, naloxegol 12.5 mg, and placebo, respectively (P < .001 for naloxegol 25 mg vs placebo; P = .02 for naloxegol 12.5 mg vs placebo). 40 In the second study (N = 700), corresponding response rates were 39.7%, 34.9%, and 29.3% (P = .02 for naloxegol 25 mg vs placebo; P = .20 for naloxegol 12.5 mg vs placebo). 40 In the first study, the median time to the first SBM was 6 hours with naloxegol 25 mg and 36 hours with placebo; in the second study, values were 12 and 37 hours, respectively (P < .001 for both comparisons). 40 The AEs that occurred more commonly with naloxegol than placebo were abdominal pain, diarrhea, nausea, and flatulence. 40 No clinically significant changes from baseline in pain score were reported, and symptoms of potential withdrawal syndrome were infrequent (1 patient in each treatment group in the first study [0.5% incidence per group]; 1 patient in the naloxegol 12.5-mg group who ran out of opioid medication in the second study [0.4% incidence]; and 4 patients in the naloxegol 25-mg group in the second study [1.7% incidence]). 40 The long-term safety and tolerability of naloxegol 25 mg were evaluated in a 52-week, randomized, open-label, parallel-group, phase 3 clinical trial (N = 844) in outpatients with noncancer pain and OIC, and results indicated that treatment was generally safe and well tolerated. 46
The pivotal phase 3 studies also examined the benefits of naloxegol treatment on a number of symptoms commonly described by patients. 40 Compared with placebo, the first study reported that 25 mg naloxegol produced significant improvements in severity of straining per week (5-point scale; P < .01), stool consistency per week (Bristol stool scale; P < .05), percentage of days per week with a complete SBM, and number of SBMs per week (both end points, P < .001); 12.5 mg naloxegol significantly improved the number of SBMs per week (P < .05). 40 In the second study, both naloxegol doses produced significant improvements in all 4 measures versus placebo: severity of straining per week, stool consistency per week, percentage of days per week with a complete SBM (all end points: 12.5 mg, P < .01; 25 mg, P < .001), and number of SBMs per week (12.5 mg, P < .05; 25 mg, P < .001). 40 Although the improvements from baseline in SBMs were comparable for both studies, response rates with naloxegol compared with placebo were numerically lower in the second study than in the first, and a significant difference in the response rate between naloxegol 12.5 mg, and placebo was only observed in the first study. 40 The reasons for the differences in response between these 2 identically designed studies were not clear. 40 Furthermore, similar to the studies of methylnaltrexone, naloxegol was not directly compared with first-line treatments, including laxatives, in these studies. Nevertheless, this study showed that naloxegol was associated with a strong treatment response, with no reduction in opioid-induced analgesia. 40
Naldemedine
Naldemedine (Symproic®; Shionogi Inc., Florham Park, New Jersey) is an orally administered PAMORA that was approved in March 2017 for the treatment of OIC in patients with chronic noncancer pain (Table 3). 32 Naldemedine is administered orally as a once-daily tablet at a recommended dose of 0.2 mg, with or without food. 32 No dose adjustment is required for patients with mild to moderate hepatic impairment, while the use of naldemedine is not recommended in patients with severe hepatic impairment. 32
The efficacy and safety of naldemedine were evaluated in 2 identically designed, pivotal, double-blind, randomized, placebo-controlled, phase 3 studies in adult outpatients with noncancer pain and OIC. 43 Patients were randomized to treatment with oral naldemedine 0.2 mg or placebo once daily for 12 weeks. 43 Similar to the 12-week studies of naloxegol, the primary end point was response rate, with response defined as ≥3 SBMs per week and an increase of ≥1 SBM over baseline for ≥9 of the 12 weeks of treatment and ≥3 of the last 4 weeks of treatment. 43 In the first study (N = 547), the response rate was 47.6% with naldemedine 0.2 mg and 34.6% with placebo (P = .002); in the second study (N = 553), the response rates were 33.6% and 18.9%, respectively (P < .0001). 43 The most common AEs reported with naldemedine in these 2 studies were abdominal pain and diarrhea. 43 The incidence of symptoms of potential opioid withdrawal were uncommon across these 2 studies (1% each in the naldemedine 0.2 mg and placebo groups). 32 Long-term tolerability was comparable in a double-blind, placebo-controlled, 52-week, phase 3 study (N = 1240) in patients with chronic noncancer pain and OIC. 32
Similar to naloxegol, the impact of naldemedine on symptoms of OIC was evaluated in the pivotal phase 3 studies. In the first study, the mean change from baseline in the number of SBMs per week at the last 2 weeks of the 12-week treatment period was 3.4 with naldemedine 0.2 mg and 2.1 with placebo; in the second study, the mean change from baseline in the number of SBMs per week at the last 2 weeks of the 12-week treatment period was 3.6 and 2.2, respectively (P < .0001 for naldemedine vs placebo for both studies). 43 The mean change from baseline in the number of complete SBMs per week at the last 2 weeks of the 12-week treatment period was 2.6 with naldemedine 0.2 mg and 1.6 with placebo in the first study and 2.8 and 1.6, respectively, in the second study (P < .0001 for naldemedine vs placebo for both studies). 43 The mean change from baseline to the last 2 weeks of treatment in the number of SBMs without straining per week was 1.5 with naldemedine and 0.7 with placebo in the first study (P = .0003 for naldemedine vs placebo) and 1.9 and 1.1, respectively, in the second study (P = .0011 for naldemedine vs placebo). 43
Some of the response rates quoted in the above studies of PAMORAs (∼40%) approximate the patient survey results with laxatives discussed previously. Thus, studies need to be performed that directly compare the performance of laxatives versus PAMORAs, to determine whether the use of PAMORAs is justified or whether PAMORAs should replace laxatives as first-line treatments. An additional consideration is cost: laxatives in general are relatively inexpensive, while the cost of PAMORAs is more variable. The cost of methylnaltrexone is similar whether dosed orally (recommended dose, 450 mg [3 tablets] per day [wholesale acquisition cost ∼US$53 for 1 450-mg daily dose]) or subcutaneously (recommended dose, 8 mg every other day for patients ≥38-<62 kg [∼US$107 for 1 dose] and 12 mg every other day for patients ≥62–114 kg [∼US$112 for 1 dose]), while the cost of naloxegol (recommended dose, 12.5-25 mg [1 tablet] per day) is ∼US$11 for 1 12.5- to 25-mg daily dose (cost information for naldemedine was not yet available at the time this article was written). 47 These factors require study, and the relatively modest performance of PAMORAs as discussed above suggests that new and more efficacious PAMORAs need to be developed.
PAMORAs in Development
Oral axelopran (formerly TD-1211), which has been shown in preclinical models to reverse loperamide inhibition in the GI tract and not induce withdrawal in morphine-dependent animals or impair analgesia, 48 is currently in phase 2 clinical development.
Other agents in earlier phases of investigation are 6β-naltrexol and 6β-naltrexamine. 6β-naltrexol, the main metabolite of naltrexone, inhibits receptor activation but does not suppress basal signaling, making it a neutral opioid receptor antagonist. When administered intravenously, 6β-naltrexol (AIKO Biotechnology, Portland, Maine) antagonized morphine-mediated GI slowing of orocecal transit time in healthy volunteers 49 and antagonized hydrocodone-induced inhibition of GI transit in mice. 50 Another neutral opioid receptor antagonist, a 6β-N-heterocyclic substituted naltrexamine derivative, is a substrate of PGP and increased intestinal motility in mice following subcutaneous administration. 37 Both molecules appear to be neutral antagonists under a variety of testing conditions (unpublished data), which may enable the use of higher doses to further increase the reversal of opioid constipating effects without precipitating significant withdrawal in an opioid-dependent gut. This hypothesis must be verified clinically.
General considerations or strategies for future drug discovery involve optimizing the receptor selectivity and affinity of candidate compounds as well as the route of administration. Given the findings that µ-opioid receptors demonstrate functional selectivity/biased agonism, 51 functionally selective antagonism with PAMORAs or functionally selective agonists that are biased against β-arrestin-2 52 may be considered as a potential means to target OIC.
Other Potential Uses of PAMORAs
The potential therapeutic activity of PAMORAs in the GI tract extends beyond the treatment of OIC. Alvimopan is a substrate for the PGP efflux transport protein, 29 which limits its entry into the CNS. It also has a higher affinity for the µ-opioid receptor than methylnaltrexone. 53 Alvimopan is an FDA-approved oral PAMORA indicated to accelerate the time to upper and lower GI recovery following surgeries that include partial bowel resection with primary anastomosis. 29 Its use is restricted to the hospital setting, and it is intended only for short-term use (12 mg given 30 minutes to 5 hours before surgery and 12 mg twice daily starting the day after surgery and continued until discharge, for a maximum of 7 days). 29 In a 12-month study of alvimopan for OIC in patients with chronic noncancer pain, a higher incidence of myocardial infarction (MI) was reported with alvimopan than with placebo, which led to the inclusion of a black box warning related to the increased risk of MI with long-term exposure in the prescribing information for alvimopan. 29 This potential cardiovascular risk has not been reported with other FDA-approved PAMORAs. 30,31 It is not approved by the FDA for OIC. The primary end point in all of the alvimopan registration studies was time to achieve resolution of postoperative ileus, which was a composite of upper and lower GI recovery. 29
Additional nonanalgesic effects of opioids may occur via opioid receptors in other peripheral tissues. Opioid receptor subtypes have been detected in myocardial cells and individual nerve fibers of the heart, 5 and therefore binding of opioid agonists to cardiovascular opioid receptors may cause significant effects. In a comparison of patients using opioids for noncancer pain with those not using opioids, users had a 1.3-fold higher risk of MI versus nonusers, and any cumulative use of 11 to 50 opioid prescriptions conferred a 1.4-fold increased risk of MI versus nonusers. 54 Data from another study indicated that patients using opioids chronically for noncancer pain had a 2.7-fold higher rate of MI and a 2.4-fold higher rate of a combination of MI or coronary revascularization (whichever occurred first) than an untreated, general population of matched individuals. 55 A 1.8-fold elevated risk of cardiovascular events, including MI, stroke, heart failure, revascularization, and out-of-hospital cardiac death, was identified in patients taking opioids versus nonsteroidal anti-inflammatory drugs for osteoarthritis or rheumatoid arthritis. 56 A study of opioid-dependent men found a dose-response relationship between lifetime opioid exposure and central cardiovascular age and arterial stiffness, with an acceleration in vascular age of >10% versus controls. 57 Stimulation of µ-opioid receptors may depress sinoatrial and atrioventricular node function, leading to bradycardia and reduced heart rate variability. 58 Methadone prolongs the QT interval and may induce torsade de pointes in individuals with cardiovascular risk factors. 58 While these retrospective studies have limitations, the collective data should still inform evolving hypotheses. Future preclinical and clinical trials should explore the potential cardioprotective effects of PAMORAs, 59 which are certainly of interest, given the widespread use of chronic opioid agonists.
Activity of opioid receptors may also have implications in patients with cancer, as recent data suggest that PAMORAs could decrease the potential effects of opioid drugs on cancer cell proliferation and metastasis. In human lung cancer cells in vitro, blockade of peripheral µ-opioid receptors dose dependently inhibited cell proliferation and migration stimulated by epidermal growth factor. 60 In addition, stimulation of human lung cancer cells by morphine, fentanyl, or a synthetic opioid peptide induced proliferation, migration, and epithelial mesenchymal transition. 60 These findings suggest a role for the µ-opioid receptor in these processes. Retrospective evaluations of opioid use and survival in patients with advanced cancer found that a higher opioid requirement was associated with significantly shorter overall survival in patients with stage IIIB or IV non–small-cell lung cancer 61 and significantly shorter progression-free and overall survival in patients with stage IV prostate cancer. 62 These associations were independent of other prognostic factors. 61,62 A recent retrospective post hoc analysis of pooled data from 2 placebo-controlled clinical trials of subcutaneous methylnaltrexone found that treatment with methylnaltrexone was associated with significantly longer median overall survival compared to placebo in patients with advanced cancer and OIC. 63 Although data from prospective studies are not yet available, further attention to the relationship of opioid exposure with survival and the potential of PAMORAs to slow disease progression is warranted in the future.
Summary and Conclusions
Optimal use of opioids for analgesia is often compromised by OIC, which is mediated primarily by µ-opioid receptors in the GI tract. OIC exacts a considerable burden on patients in terms of impaired QOL and activities of daily living. Early attempts to treat OIC with naloxone led to the development of PAMORAs. Three currently approved PAMORAs have shown efficacy in treating OIC in patients with chronic pain, and new PAMORAs currently in development are likely to provide more treatment options in this patient population. Consensus guidelines from the American Academy of Pain Medicine recommend the use of prescription therapy for OIC, including PAMORAs, for patients with a BFI score of ≥30 (out of a possible score of 100) and an inadequate response to first-line treatments (eg, dietary changes, over-the-counter laxatives). 15 Future research should address whether PAMORAs are more efficacious than laxatives and other first-line treatments, and whether PAMORAs have actions in addition to preventing exogenous opioids from binding to µ-opioid receptors, such as blocking endogenous tone or acting as inverse agonists. Future research should also address whether PAMORAs can reduce the increased cardiac risk or potential tumorigenic effects of opioids.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: E.B. is a cofounder of Biousian Biosystems Inc. and Aiko Biotechnology. E.B. holds founding shares of Biousian Biosystems Inc. and Aiko Biotechnology. E.B. holds several issued patents around opioid agonists and antagonists. J.M.S. is a cofounder and equity partner of Teleport Pharmaceuticals, LLC. J.M.S. has received contract funding from Stealth Peptides and Depomed, Inc. as a fee for service. E.B. has conducted contracted work through the University of New England for several biotechnology and pharmaceutical companies.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Sponsored by AstraZeneca Pharmaceuticals LP. Editorial support was provided by Stephanie Leinbach, PhD, Diane DeHaven-Hudkins, PhD, and Erica S. Wehner, RPh, Complete Healthcare Communications, LLC (Chadds Ford, PA) and was funded by AstraZeneca Pharmaceuticals LP.