
Abstract
Given the central importance of the peritoneal dialysis (PD) nurse in successfully training and supporting a patient with PD at home, as well as preventing complications as a result of the therapy, the International Society for Peritoneal Dialysis (ISPD) has provided guidance on the principles for training in two previous publications. Despite the lack of high certainty evidence in teaching PD, this ISPD 2025 Position Paper builds upon the two prior works to provide contemporary approaches to training a patient/care partner for PD to be performed at home, based upon an evolution in healthcare practices broadly and the cumulative evidence to support recommendations to date. A number of practice points have been provided. Suggestions are discussed on key areas in teaching PD which include: (a) Education, knowledge, skills and attributes for the PD nurse trainer; (b) Preparation for the training; (c) Methods of training/educational interventions; (d) Post training; and (e) Measures of outcomes. Areas for future research are suggested and include: best practices on educational interventions; knowledge and skills necessary for PD nurses; and how to best capture and measure the patient experience related to PD training.
This is a visual representation of the abstract.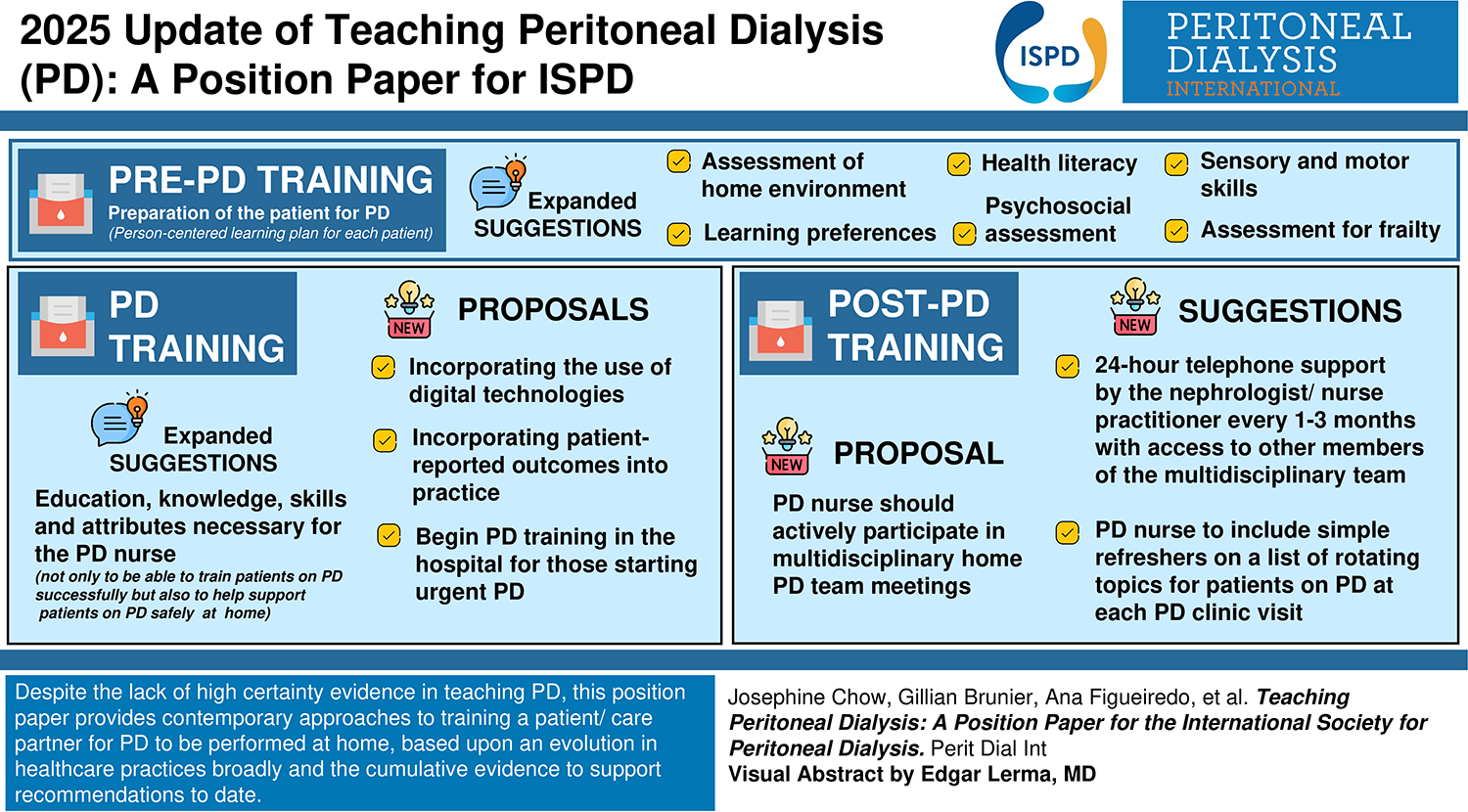
What's new with the 2025 update of the teaching PD: a position paper for the International Society for Peritoneal Dialysis?
Pre PD training
Expanded suggestions for preparation of the patient for PD: assessment of the home environment; learning preferences, health literacy, psychosocial assessment, sensory and motor skills, and, for older adults, assessment for frailty, all to help ensure a person-centered learning plan for each patient.
PD training
Expanded suggestions for the education, knowledge, skills and attributes necessary for the PD nurse not only to be able to train patients on PD successfully but also to help support these patients on PD safely at home.
New suggestions for virtual training options to enhance flexibility and accessibility for patients.
New proposition for incorporating the use of digital technologies, including e-learning platforms and virtual simulations, creating a hybrid approach to PD training.
New proposition for incorporating patient-reported outcomes into practice, better to capture and measure the patient experience related to PD training.
New proposition for those patients starting PD urgently is to begin PD training in the hospital.
Post PD training
New suggestions for 24-h telephone support for patients and for the patient to be seen in the outpatient PD clinic by the nephrologist/nurse practitioner every one to three months with access to other members of the multidisciplinary team (MDT) where available.
New suggestions for the PD nurse to include simple refreshers on a list of rotating topics for patients on PD at each PD clinic visit – to aid in preventing peritonitis and managing potential complications.
New proposal that the PD nurse should actively participate in multidisciplinary home PD team meetings to review, discuss and update the patients’ plans of care.
Introduction
Peritoneal dialysis (PD) is a home-based therapy, performed by patients, their care partners, or health providers as with assisted PD. Thus, the success of PD as a kidney replacement therapy for kidney failure is dependent to a large part upon the patients’ or care partners’ or health providers’ abilities to consistently, reliably, and safely execute the technical procedure as well as to troubleshoot common problems that may arise at home. In a larger sense, patients accept a home-based dialysis therapy for kidney failure, such as PD, only when assured that the home program will provide adequate training and ongoing support to perform PD treatments at home and troubleshoot problems as they arise.
Given the central importance of training in successfully maintaining a patient with dialysis at home, the International Society for Peritoneal Dialysis (ISPD) has provided guidance on the principles for such training. The first such guidance was published by the Nursing Liaison Committee of the ISPD in 2006 and it addressed critical issues such as who should provide the training, the role of a physician, who should the learner be, what should be taught, where the training should occur, and how long it should last. 1 Notably, it underscored the importance of the trainer understanding the principles of adult learning when providing such training to the learner. In 2016, the Nursing Liaison Committee of the ISPD undertook a review of training practices around the world and expanded and updated the guidance. 2 The Working Group for this 2025 Position Paper had representation from North America, Latin America, Europe, Asia and Oceania. The Working Group had also consulted with three PD nurses from Africa. The practice points were formulated following consultation with patients and representatives from geographically diverse regions including Latin America, Africa and Asia. This 2025 update builds upon the two prior works to provide contemporary approaches to training for PD to be performed at home, based upon evolution in healthcare practices broadly and the cumulative evidence to support recommendations to date.
Nevertheless, it is important to recognize that a major barrier to providing evidence-based guidance for training in performing home PD has been the paucity of research in this area. The authors of the 2006 guidance document for training patients identified only 46 publications from 1979 through 2005. 1 In the 5 years prior to the publication of the curriculum in 2016, only 17 articles had been published. 2 Further, a recently published systematic review identified 21 publications between 2013 and 2023, that included only three randomized controlled trials. 3 This limitation should be kept in mind when applying the recommendations in this document. This Position Paper provides expanded suggestions for preparation of the patient for PD such as learning preference, screening for health literacy, training based on adult learning principles, as well as follow-up post training such as regular simple quizzes for patients, home visits, and multi-disciplinary team meetings. Implementation of these suggestions should allow for adaptation of the approaches by different centers depending upon the organization of the health system and infrastructure, availability of resources and personnel, and cultural mores of the society. Yet, this document also provides some key principles that should be consistently followed, particularly by new and growing home programs.
Education, knowledge, skills and attributes for the PD nurse trainer
Our first suggestion is that the PD trainer should be a nurse, as indicated by multiple authors in both earlier and more recent publications.1,2,4–10 Second, we concur with Bernardini et al.,
1
that it is essentia
Our third suggestion is that we believe it is most beneficial and ideal if a PD nurse trainer has advanced education in nephrology nursing (Table 1). 12 Barriers to this can be cost for the nurse, lack of institutional support, and/or availability of such training in the region. 13 While a few of these advanced nephrology nursing courses listed in Table 1 are available to nurses residing in low- or middle-income countries, cost is still a concern, plus, for most courses, it is necessary to be able to understand English well. Ling 14 in a survey of 38 home PD units in Australia observed PD units with higher numbers of nurses who held a nephrology postgraduate qualification were associated with lower numbers of patients transferring to haemodialysis, although this finding was only weakly significant; King, 15 in the UK, found a specialist nephrology training course for nurses led to the nurses gaining ‘increased understanding to reasons and rationale for practice,’ as well as ‘enhanced assessment and decision-making skills’; while Béchade 16 in a national study in France found patients treated in a center with a nurse specialized in PD had a lower risk of peritonitis.
Selected nephrology nursing specialty education programs.
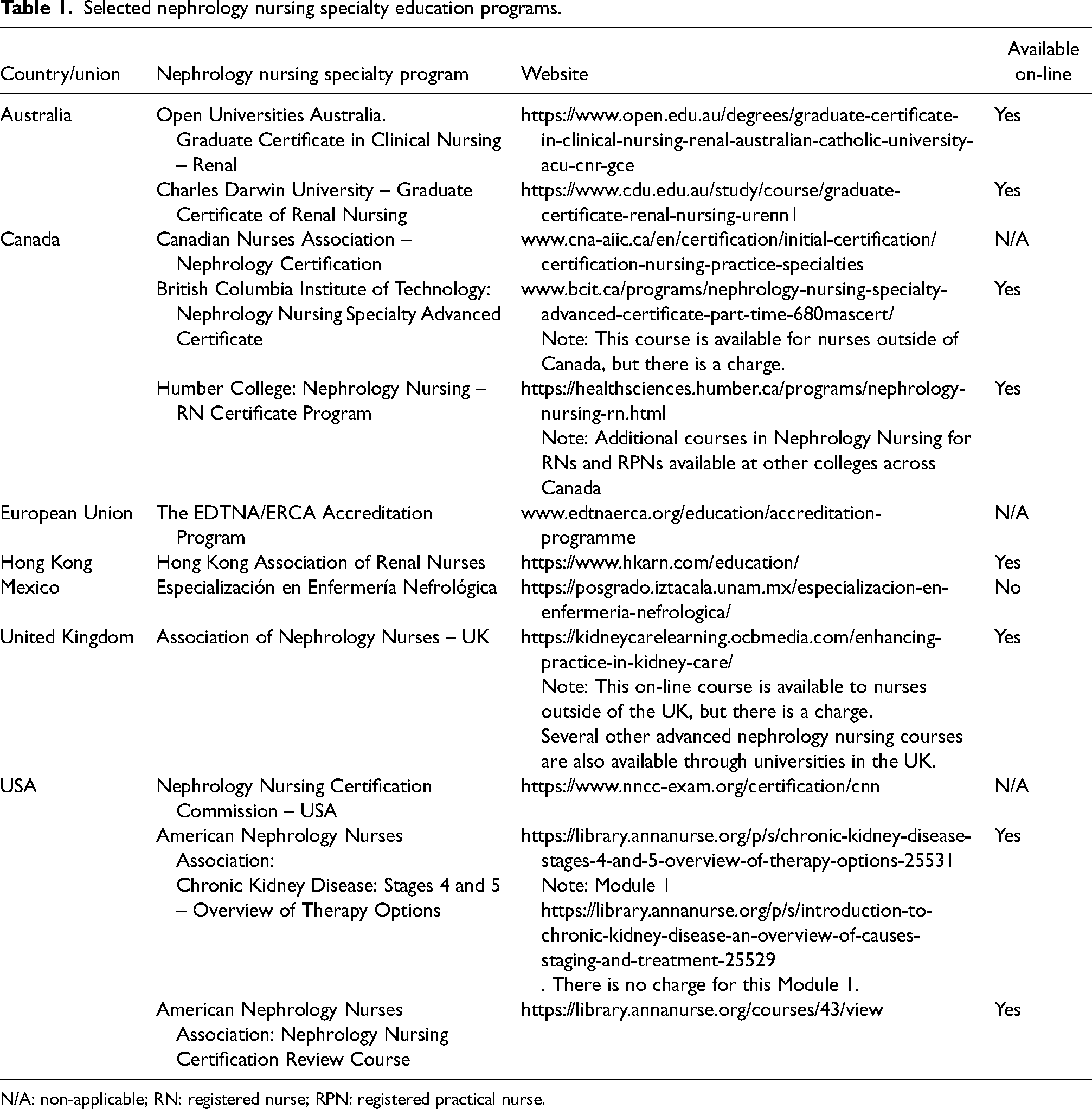
N/A: non-applicable; RN: registered nurse; RPN: registered practical nurse.
Training a patient for PD can be a formidable task; skills to perform a procedure do not necessarily translate into ability to teach, and learning how best to teach cannot be learned passively through experience.1,17 Thus, our fourth suggestion is that education in the principles of adult learning should be considered for all PD nurse trainers, also advocated by other authors.1,2,18,19 Fifth, we concur with Chow et al. 17 that PD nurses should have regular opportunities to update their knowledge; however, from a recent Peritoneal Dialysis Outcomes and Practice Patterns Study (PDOPPS) survey of home PD units, in 6 out of 7 of these countries surveyed, less than 60% of home PD nurse trainers reported that they received continuing education, 20 unquestionably an area that should be improved and where opportunities such as ISPD webinars could play a role.
Our sixth suggestion is that we believe there are some other very relevant attributes, such as empathetic understanding, that a PD nurse trainer should have. From interviews with PD nurse trainers in three qualitative/descriptive studies, nurses emphasized the importance of alleviating patients’ fears and building a collaborative relationship with patients. 21 They also highlighted the need for flexibility and customized training 22 and valued including family members or care partners in the process. 18
For our seventh suggestion, we endorse that the newly hired PD nurse trainer complete a 6- to 8-week orientation with assignment to a senior PD training nurse mentor who would familiarize the new nurse with all the home PD procedures and coach the new nurse through all aspects of the first training of a patient for home PD. 1 This mentorship relationship, we anticipate, would continue on through the new PD nurse trainer's first year of practice. For nurses where mentorship is not available, especially for those in low- or middle-income countries, ISPD does offer a scholarship program for a nurse or doctor/nurse team to visit for up to 3 months an established PD center with experience in training new PD specialists (www://ispd.org/ispd-fellows/).
Finally, in light of the global nursing shortage, including that of nephrology nurses, it is imperative to concentrate on retaining home PD nurses.20–22 This can be achieved by fostering a positive work environment within home PD units, ensuring sufficient nurse-to-patient staffing ratios, and providing opportunities for continuing professional education for nurses.23,26,27 Whether improvements in remote monitoring and telehealth would help lighten the workload for home PD nurses has yet to be shown.28,29
The challenges of recruitment and retention and the evolution of different unregistered roles have been seen worldwide, with examples of non-registered practitioners with varying titles in haemodialysis settings in many countries,27–29 Similarly, these roles are used within PD, especially for assisted home PD ‒ making the option of home PD available for older and more frail patients.33,34 These different models can help to provide additional support for tasks that do not need a registered nurse at a lower cost. However, caution is needed as these assistants still need to be trained and supervised by the registered PD nurse and the specialist skills of the PD nurse are still required for problem solving and answering questions from the assistants. 28
Home PD nurses are a critical part of home PD therapy and strategies need to be developed not only to promote recruitment of new nurses but also to retain them in the home PD setting, while the effectiveness and safety of use of other licensed health care nurses and non-health care assistants in a home PD unit need further study.
Practice points
The PD nurse should:
Be a registered nurse Have prior nursing experience on a medical/surgical ward Ideally have advanced education/certification in Nephrology Nursing Have education in the principles of Adult Learning Have regular opportunities for continuing education Have relevant attributes such as empathetic understanding and the ability to be flexible in the teaching process Have a 6- to 8-week orientation with a senior PD nurse mentor, with mentorship to continue for the first training of a patient on PD and through the first year of practice.
Preparation for the training
Definition
Any training, assessment or education given to a patient and/or care partner before commencement of PD training.
Preparation and assessment before commencement of PD training is an important step in successfully establishing a patient and care partner on PD therapy. There are differences between assessments designed to assess for suitability and assessments designed to personalize the PD training. The evidence for what, how and when these should take place is limited.
Assessing for suitability
Once a patient has opted for PD as their modality choice, many PD units will conduct a home visit to assess the environment and undertake further assessments. The suitability of an individual's home is in many cases based on local practices. For example, in some countries, basic supplies, such as water and adequate clean space, may be limited so adaptations and innovative ways to overcome these have been used. Basic requirements are a clean, dry and adequately lit environment to perform PD, access to hand washing and space for supplies. An Australian study to evaluate the effect of a pre-dialysis assessment was conducted in 155 incident patients receiving PD in a single centre. 35 This study used the Jo-Pre-training Assessment Tool (J-PAT) tool consisting of 38 assessment items in six domains: physical stability, nutritional status, communication ability, ability to maintain self-care, psychological suitability and social support, originally designed to assess patients’ suitability for home PD. 36 Outcomes measured were peritonitis, length of time on PD, transfer to haemodialysis (HD) and death. There was no difference in peritonitis risk in those who underwent pre-dialysis assessment but as the tool was designed as an assessment of suitability, they reported a time lag before commencement of PD and recommended a repeat of the assessment before commencement. 35
Pre-PD education and assessments
MDT pre-dialysis care is an area of practice deemed important to help support shared decision-making to enable and increase the uptake of people choosing a home dialysis therapy. How it is delivered and by whom are not clearly defined. Some studies of MDT pre-dialysis care have reported improvement in self-management strategies, which, whilst not PD specific, have focused on chronic kidney disease (CKD) progression, dialysis start and mortality as end points.37,38 The same authors reviewed the impact of the same MDT pre-dialysis program on PD outcomes in a 5-year prospective study comparing groups who received MDT pre-dialysis care (MPE) vs standard care (non-MPE). 39 Outcomes included episodes of peritonitis and outcomes after peritonitis (hospitalization, technique failure, HD transfer, switching of modality into haemodialysis or death). After 5-years follow-up (mean follow-up duration: 29.4 months; 30.1 months in MPE group vs. 28.5 months in non-MPE group), the MPE patients had significantly lower peritonitis rates (0.29 ± 0.72 vs. 0.64 ± 1.5 episodes/person-year or median [IQR]: 0 [0.29] vs. 0.11 [0.69] episodes/person-year, p < 0.001) than non-MPE patients. The MPE group had lower peritonitis-related death rates compared to the non-MPE group (3.6% versus 8.7%, p = 0.04). However, the frequency of hospitalization and the percentage of HD transfer did not differ significantly between the two groups. 39 Recommendations have been made to support shared decision-making in PD and placing more emphasis on ‘person-centred care’. 40 A mixed methods study from Denmark that evaluated an intervention of shared decision-making demonstrated over 80% of participants felt they had experienced shared decision-making; including making a high-quality decision, with higher knowledge scores in those who chose a home dialysis option. 41
In a study that was PD-specific, the authors described a pre-PD program in which patients and care partners underwent education (PD catheter insertion, regimens) and assessments (home dialysis support, dexterity, mobility, vison, hearing and psychosocial support) with additional learning resources provided. 42 An evaluation of 94 patients who underwent the program was conducted. Outcomes for this study reported on the results of the assessments; 30 (32%) had no issues, poor eyesight was the main issue in 34 (36%), and two or three issues (including hearing impairment, mobility, dexterity and support) were identified in 30 (32%) patients. Whilst the observed numbers were small, the benefits of the assessments on understanding different needs of patients were highlighted. Patients and care partners expressed a greater level of satisfaction and were welcoming of the support during this pre-PD program. 42 An instrument to assess self-management capability of patients receiving PD recommended to be used pre-training has also been developed. 43 This tool includes cognitive, sensory and motor capabilities but as yet has not been validated at scale, and therefore requires further evaluation.
In large observational studies of the associations between training practices and PD infection outcomes, commencement of education ahead of PD training or PD catheter insertion were reported to be associated with purported benefits.44,45 The Brazilian study described simulation training ahead of PD catheter placement as a novel technique to enhance patients’ and care partners’ learning of PD technique 45 ; showing better results in terms of peritonitis rates when compared to patient training only after catheter insertion.
General principles of adult learning can be applied in the PD setting. As previously reported, assessing learning styles is a useful start in planning the PD training around the individuals’ preferences. 2 One such tool is the visual, aural, read/write, and kinesthetic (VARK- https://vark-learn.com) questionnaire, which assesses preferences based on visual, aural (hearing), read/write and kinesthetic (motor) domains. The use of written support and starting PD learning with hands-on training alone were associated with a higher risk of peritonitis-free survival (HR 1.59 and HR 1.94, respectively). Conversely, incorporating audio support and combining hands-on training with theoretical learning were linked to a lower risk of subsequent peritonitis episodes after the first (HR 0.55 and HR 0.57, respectively).,11,46 A study with home dialysis patients with diverse learning styles, found that with visual learners experiencing fewer adverse events within the first six months following training. This highlights the importance of tailoring home dialysis training to individual learning styles.47,48 Despite the lack of more studies in PD, these results can be extrapolated to PD training since the patients share similar characteristics.
Factors affecting uptake of PD are well documented including culture, language, education and economics, 49 as well as a global recognition of low PD uptake in low-income settings. 50 There is also inequity in higher middle-income countries in certain ethnic groups. Whilst many factors will contribute to this, language maybe an issue. For preparation of PD, language needs to be considered as it can be a barrier to learning 51 ; therefore, appropriate access to translated information, interpretation services and culturally specific educational material is important.
A scoping review to assess learning styles and factors affecting learning analyzed 45 articles and found that health literacy was the most commonly reported factor affecting learning, followed by anxiety, illness condition, cognitive deficits, comorbidity, older age and lack of suitable communication by healthcare professionals. 46 This review recommended that education should be tailored to more characteristics of learning than learning styles. 46 The association of low health literacy with PD outcomes has been described as important, yet adequate assessments remain unclear and poorly defined in PD.52,53 It is not within the scope of this Position Paper to present evidence on self-management, health behaviours and methods to improve health literacy, but suffice to say it is deemed important as it is associated with outcomes, such as peritonitis, and therefore an important consideration in assessments before commencing PD.2,54
It is important to recognize the growing older population with increasing multi-morbidity and frailty, which are associated with adverse outcomes such as hospitalization and higher mortality. 55 Cognitive impairment in PD patients is a particularly important consideration and quoted at 28.7% prevalence 56 ; highlighting the importance of recognition and screening ahead of training so that modifications can be made. Being older has been associated with modifications in the relationship between training requirements and PD outcomes and therefore should be considered as part of the pre-assessment process. This would also align with the ISPD guideline on goal-directed care, particularly for older people living with frailty. 57
Preparation for PD should include a number of assessments to ensure patients and families are adequately prepared and enable a person-centred training plan to be developed with patients and families together. This will allow the nurse trainer to adapt to the patient's and family's needs, taking into account suitability for different PD modalities and levels of support required including assisted PD, 1:1 training, group training and training in the home. It will also provide an opportunity to establish the needs of patients and families for social workers, psychologists or other members of the MDT who can assist in widening the support required.
Practice points
Home Assessment – The purpose of the home assessment can include assessing the environment and provides an opportunity to meet the patient and care partner to build therapeutic relationships.
Learning Style, Characteristics and Preferences – A detailed assessment should include learning preferences using a validated tool such as VARK. Detailed interaction with the patient and family members to better understand goals and preferences.
Assessment of health literacy to establish the specific tailored teaching materials and support required for each patient. This should include language specific information.
Psychosocial assessment should incorporate patient reported outcome measures that include depression, anxiety and cognition, plus social circumstances and support requirements. This will include others who may be involved in some or all aspects of the PD care, e.g., care partner or family member.
Sensory and motor assessments should include vison, hearing, dexterity and mobility.
For older adults, assessment of frailty is suggested and will include some of the above but also other older person impairments such as continence, falls, cognitive impairment and polypharmacy and may include advance care planning if appropriate.
Methods of training/educational interventions
The training process for PD is a crucial component of ensuring that patients and their care partners can perform the procedure safely and effectively at home. This comprehensive training encompasses a range of elements, including duration and schedule, staff ratio, materials used, home visits, virtual training, and the integration of technology.
Duration/schedule
The training for PD generally spans from several days to a few weeks, depending on the patient's learning pace and the complexity of the individual case. A typical training program might last from 5 to 10 days, with sessions scheduled daily or every other day, with the duration of 1–3 h per session. Most studies are retrospective observational cohort designs, and there are no randomized controlled trials (RCTs) assessing the effectiveness of training duration. The BrazPD study suggested that 15 h or more training duration was associated with lower peritonitis rates when compared to less than 15 h (0.26 per year at risk versus 0.32 per year at risk, p = 0.01). 45 A small retrospective study, consistent with the findings of BrazPD, reported that patients required a median of 10 training sessions (IQR 8–13), with each session lasting 2–3 h, resulting in a total training time of approximately 20–30 h. 58 However, patients who required more than 26 h of training, typically older and with more comorbidities, were found to have a higher risk of peritonitis. Another observational study reported that older patients took longer to be trained (18.1 ± 7.9 vs. 12.7 ± 4.3 h, p = 0.004) and had a higher risk of peritonitis than younger patients although no difference was found in training time between patients who did and did not experience peritonitis. 59 Similarly, a prospective study using an initial structure training initiative (iSTI) for adult caregivers of pediatric patients reported lower peritonitis rates in the STI group compared with controls (0.29 vs. 0.69 episodes per year, p = 0.001). In this study, the median training duration was 19.5 h (18–20) with a median score on objective structured assessment (OSA) of 97%. If the OSA performance was below 95%, the care partner received re-training (iSTI) for a further 10 h. 60
A survey from the International Pediatric Peritoneal Dialysis Network found that shorter (< 20 h) training duration and lower number of training tools (both p < 0.02) were associated with higher peritonitis rates, after adjustment for proportion of treated infants and income of country of residence. 61 On the other hand, the study from Gadola et al., found lower peritonitis rates after introducing a PD education program (PDEP) with eight lessons delivered in a minimum of five session of 2 h long, when compared to the traditional training prior to the introduction of OSA (0.28 vs. 0.55 episodes/patient–year, p < 0.05). 62 In contrast, the PDOPPS international survey of training practices, which analyzed 1376 incident patients and 120 facilities, found no association between training duration and peritonitis risk. 20 This differed to a previous PDOPPS analysis of 209 facilities with a total 7051 mix of incident and prevalent patients in which a PD training duration of six or more (vs. <6) days was associated with a lower peritonitis risk (RR: 0.81; 95% CI: 0.68–0.96). 63 Although there is no consensus regarding the ideal training hours to be implemented in PD training programs, low certainty evidence suggests that it may be reasonable to train for a minimum of 15 h with formative (ongoing feedback) and summative with evidence of a learner's final mastery.
Staff-to-patient ratio
The number of patients a nurse can teach to perform PD varies depending on several factors, including the teaching approach used, the nurse's experience, the complexity of each patient's case, and the resources available. The staff-to-patient ratio during training is crucial to ensure personalized attention and effective learning. Generally, the ratio is kept low, often ranging from 1:1 to 1:3, to allow for ample interaction between the patient and the trainer.,19,20,44,58,60,64,65 This low ratio ensures that each patient receives tailored instruction and feedback, addressing specific concerns and questions that arise during the learning process and maybe the only aspect of training where there is a reasonable consensus.
Material
A variety of materials are utilized during PD training to facilitate learning and ensure that patients have all the tools needed for successful home dialysis. The ISPD Syllabus for training patients and caregivers has recommended assessing the learning style of the learner to individualize training and the use of Adult Learning Principles. 2 Training manuals and guides provide step-by-step instructions on the PD procedure, including how to prepare and administer dialysis solutions, handle equipment, and recognize and address potential complications, other visual aids such as picture cards, posters, brochures, prints, diagrams; videos illustrating the PD process and common troubleshooting techniques. These visual aids help reinforce the information presented in the manuals and in hands-on training. However, it is important to use language that is simple and at a sixth-grade reading level or below. 66 Simulation, usually low fidelity, apron or dummy, mimics a human abdomen thereby allowing patients to practice a bag exchange or connection /disconnection in an automated PD (APD) machine without the need for a real-life exchange.18,58,57–59 In addition, it is possible to ask the patient for a video or photographs of the space where they will undergo dialysis, to build the simulation scenario as similar as possible to their real environment. A well-designed patient training program should ideally incorporate real-life problem-solving techniques, an interactive electronic platform,65–67 an APD machine with automated instruction using audio, video, and animation, 70 and audio material to achieve proficiency. 44
A diversity of material is validated in several studies, however a well-structured training program with an observed structured assessment (OSA) may facilitate a patient's empowerment to perform the procedures at home.60,62 An example of OSA could be hand hygiene, where the nurse demonstrates the technique and explains the rationale, possibly using step-by-step images. At the end of the training, the patient should be able to reproduce the technique, demonstrating psychomotor competence. All stages of the training should have clearly defined learning objectives, and the patient must be assessed to determine whether or not they have achieved the required competence.
Strategies for training in a non-native language
Training PD patients in a language different from their native language can be effectively approached by incorporating multisensory and culturally responsive strategies. The literature suggests that a multisensory approach, which includes visual, auditory, and symbolic aids, can be beneficial in overcoming language barriers in PD training. 71 This approach involves using pictorial aids and symbols to reduce reliance on written language, which can be particularly useful for patients who may not be proficient in the training language. A hybrid approach to therapy, which combines traditional training methods with innovative tools, can further enhance learning. For instance, digital platforms or mobile applications that offer interactive modules in multiple languages can provide patients with additional practice and support outside of formal training sessions. Engaging family members or friends who speak an Indigenous language is crucial, not only during initial training and education but also for ongoing communication, particularly when problems arise later. Their involvement can bridge cultural and linguistic gaps, ensuring that care remains responsive. It is also valuable to consider peer patient support. 72 There is increasing evidence that peer-led models can enhance understanding, trust, and adherence, especially in communities where shared lived-experience fosters empowerment. 73
Overall, the integration of these strategies can create a more inclusive and effective training program for PD patients who are learning in a non-native language, ultimately improving their ability to manage their dialysis independently and safely.
Pre PD training home visit and PD training in the home
PD training in the patient's home is intuitively appealing, as the patient's home is where they will ultimately perform their PD. However, studies evaluating home-based training are scarce.74,75
There are few published reports on the practice of a home visit prior to starting PD training to assess the patient's home environment. Two reports indicate that such a visit by a PD nurse may be beneficial to help the patient identify, for example, the best area for storage of supplies, most appropriate area to perform PD and suggestions on how to contain pets in the home when the patient is performing PD.76,77
A recently published study involving newly enrolled patients on PD at an Italian center reported a program whereby a team assessed the patients’ homes to ensure suitability before commencing treatment (duration time = 2 h). The training phase was then divided into two parts: an initial session at the hospital (duration = 3 h) followed by a subsequent session at the patient's home (duration = 3/4 h for 2 days). Video training was provided to the patient at home, which can be considered a form of home training.64,78 Home visits were an integral part of the training process, thereby allowing the PD nurse trainer to assess the home environment and ensure that it was conducive to safe and effective dialysis. During these visits, the nurse trainer evaluated the setup of the patient's dialysis area, ensuring that it met the necessary standards for cleanliness and organization.
Virtual training
Following the COVID-19 pandemic, virtual training and monitoring have become an increasingly popular and effective component of PD education.64,79 This modality offers several advantages, including flexibility and accessibility. Technology plays a significant role in enhancing the training process for PD. Advanced technological tools are utilized to improve both the learning experience and the ongoing management of the treatment. Some programs are beginning to explore use of modern technology, such as virtual reality (VR) technology to provide immersive training experiences. VR simulations can offer a hands-on experience without the risks associated with real-life practice, allowing patients to familiarize themselves with the process in a controlled environment. It offers a standardized learning protocol in which the different steps can be trained separately and put in the right order afterwards. The VR technology training experience relies on the user to feel like being in a different environment (immersion) and to interact with the items and stimuli around the user like in the real world (interaction). Studies with VR suggest that training time can be shorter, and that it allows more flexibility for healthcare professionals. However, professionals are adamant about the need for nurses to be present during the use of VR training.80,81
Use of technology
The use of digital technologies, such as mobile applications, e-learning platforms, and virtual simulations, have made it possible to customize teaching to the specific needs of each patient, improve knowledge retention, and provide constant access to educational resources. Studies have shown that mobile applications that include instructional videos, interactive reminders, and self-assessment modules improve patient competence and confidence in patients with CKD including PD. 82 In addition, virtual simulations offer a safe environment where patients and caregivers can safely practise techniques, increasing their skill and reducing the anxiety associated with managing PD. 83
The use of e-learning platforms and mobile applications also facilitates continuous learning and updating of knowledge in PD. Online platforms allow patients and care partners to access training materials anytime, anywhere, resulting in greater flexibility and convenience. Online courses can be designed with interactive modules, quizzes, and discussion forums to encourage active participation and sharing of experiences among participants, which have been shown to improve understanding of, and adherence to treatments. 84 Combining these technologies with face-to-face clinical support may create an effective hybrid approach to teaching PD, thereby optimizing both learning and patient care. However, it is important to recognize that the older the patient, the more comprehension problems they tend to have, so it will be important to evaluate the feasibility of virtual resources in this group of patients. 85
Training patients with other challenges
Equitable access to training must extend to individuals with cognitive deficits, learning difficulties, and hearing or visual impairments. 86 Tailored approaches such as simplified materials, assistive technologies, and alternative communication methods, are essential to ensure these patients are not excluded from PD. Without such accommodations, they may be denied the chance to manage their own care, leading to reliance on costly assistance that can restrict life participation.
Training patients with urgent initiation of peritoneal dialysis
When PD is initiated urgently or unexpectedly, hospitalization supports the start of training for the patient and their care partner. Training can commence immediately or after 1‒2 weeks, depending on the patient's uremia level. It is preferable that PD training includes the materials mentioned above.87,88 Additionally, patients gain fundamental knowledge by observing the PD nurse perform the technique during their hospital stay, facilitating meaningful learning. Once the patient or family member demonstrates proficiency with the simulator, they can carry out the technique under supervision for evaluation and feedback. Training progresses gradually, adapting to the understanding of the patient and their family members, until discharge with the technique mastered and reviewed. This allows dialysis to continue once the patient is home. If the patient's clinical condition does not allow for training during the hospital stay, it is suggested that they be enrolled in an assisted dialysis program while they complete the training and meet the requirements for safe dialysis at home.
Practice points
Ensure Sufficient Training Duration ‒ While the ideal training hours are not firmly established, low-certainty evidence suggests that training for at least 15 h with ongoing feedback and formal assessments to certify proficiency may be reasonable. Tailor training time to patient needs, considering factors like age and comorbidities.
Maintain a Low Staff-to-Patient Ratio–A low staff-to-patient ratio is essential to ensure personalized attention and effective learning. Ratios typically range from 1:1 to 1:3.
Utilize Diverse Training Materials ‒ Incorporating a wide array of materials during PD training enhances learning. Use manuals, visual aids (such as picture cards, posters, and diagrams), and videos to demonstrate PD procedures. Simulation tools like low-fidelity dummies or aprons allow patients to practice bag exchanges and other techniques in a safe, controlled environment. Customized materials, like those that follow adult-learning principles, have been shown to empower patients and help them perform procedures effectively at home.
Offer Virtual Training Options ‒ Virtual training offers several advantages, including flexibility and accessibility. While in-person training is vital, incorporating virtual training sessions allows patients to engage with materials from the comfort of their homes. Programs should include video training, real-time monitoring, and virtual support. Consider using advanced tools like VR simulations to immerse patients in hands-on learning experiences without the risks of real-life practice.
Implement Technological Tools for Continuous Learning ‒ Digital tools like mobile applications, e-learning platforms, and virtual simulations enhance both patient training and ongoing care management. Mobile apps that offer instructional videos, interactive reminders, and self-assessments improve patient knowledge retention and confidence.
Ensure Regular Feedback and Assessments – Ongoing feedback and objective structured assessments (OSA) should be part of the training process. Patients or care partners should receive regular evaluations of their performance during training sessions.
Tailor Training to the Patient's Learning Style ‒ Customizing training to suit the individual learning style of each patient can lead to better outcomes. Use tools such as assessments at the start of the training to determine whether the patient learns better through visual, auditory, or hands-on methods. Adjusting the approach to fit the patient's preferences ensures that the information is absorbed more effectively and improves long-term retention. If training a group, be sure to include at least one educational material for each learning style.
Standardize Training with Structured Programs ‒ Introducing structured training programs with clearly defined lessons, objectives, and protocols can help ensure consistency in the training process.
Combine In-Person Training with Hybrid Approaches ‒ While in-person clinical support remains vital for PD training, combining it with virtual components (such as online courses, e-learning modules and discussion forums) can optimize patient education. A hybrid model that integrates face-to-face sessions with digital resources ensures that patients receive comprehensive and flexible learning support.
Begin PD training during the hospital stay of patients with urgent PD initiation. Take advantage of the opportunity for the patient to see the procedure as the nurse performs it. If this is impossible, it is suggested to opt for assisted dialysis.
Post-training
Peritonitis is a leading cause of hospitalization and PD discontinuation for patients on PD. 89 Peritonitis is also one of the most feared outcomes for patients. 90 Thus, prevention of peritonitis is of great importance. There are indications that not all patients adhere to PD exchange protocols after the initial training on PD has been completed and these patients are at greater risk of developing peritonitis, especially gram-positive peritonitis from touch contamination.89–92
After PD start, patients usually have 24-h telephone support through nurses in the PD unit and they are seen every one to three months in the outpatient PD clinic by a MDT where available.2,95 This is a time when the PD nurse can check with the patient and care partner in person and assess how they are managing in the home, examine the patient's PD catheter exit site for signs of infection, and review the patient's treatment records and medications. It is also a time when the PD nurse could give a patient simple refreshers on different topics using five-item quizzes on, for example, hand hygiene, and by using ‘What if?’ scenarios, to review with the patient potential complications to think through and resolve. 18 Optimal frequency of clinic visits, patient preference for virtual visits and improved clinical outcomes with remote monitoring for APD all need further study.93–95
MDT meetings (sit-down, in person or virtual) involving nurses have been shown to be associated with better patient care outcomes for patients on in-center haemodialysis and those who are pre-dialysis.98,99 However, we could find no published research on best practices or patient outcomes for such MDT meetings of the Home PD Team for patients on PD and the involvement of PD nurses. To understand current practices for MDT meetings in PD units, we conducted an informal email survey of members of the ISPD Nursing Committee across 8 countries (September 2024); all of whom practiced in home PD units. We found that the practice of MDT meetings for PD patients varied considerably from only for unstable patients as needed, to all PD patients during regular meetings held weekly, monthly, every two months, or every three months (either separately or immediately before or after a home PD clinic, sometimes virtually). Moreover, who is considered part of the MDT also varied widely; for some centers, only the nephrologist or nurse practitioner and PD nurses were involved, while for others the nephrologist, PD nurses, social worker, and dietitian were involved. One home PD unit included a pharmacist and one a community nurse; others invited the social worker, dietitian or psychologist, as needed. While such MDT meetings likely ensure all members of the team are aware of the patient's current issues and may improve patient outcomes, including peritonitis rates, more research is needed. Such MDT meetings may also provide an excellent opportunity for education for PD nurses, to ask questions, and to learn from other team members, as well as other team members to learn from PD nurses; however, these MDT meetings do involve considerable time for all health care professionals involved. 100 Even though there is no standard for these MDT/Home PD Team meetings, we would suggest that all PD nurses learn to take an active part in them.
There is low certainty evidence that regular PD nurse home visits, as part of a multifaceted quality improvement initiative and using a home visit form for comprehensiveness, may be associated with a lower incidence of peritonitis and may help extend the patient's time on PD.,18,91,94,99–104,130 During the home visit, not only can the PD nurse assess the patient's adherence to the PD procedure, but also assess the home environment for safety and risks, appropriate exit-site care supplies, PD supplies, medications, and offer support to the patient. The PD nurse can re-educate the PD patient and care partner if indicated, suggest changes to the home environment, document the details of the home visit and plan for further interventions with the Home PD Team. While guidelines recommend visits by a PD nurse early/on first PD at home, then reassessment with repeated home visits as needed and at yearly intervals, more studies are needed to determine the optimal frequency and timing for these visits.89,107,108 In some contexts, however, it may be difficult for the PD nurse to carry out in-person home visits due to safety concerns and time involved. In such cases, it may be possible for the PD nurse to carry out a virtual visit. The authors of one exploratory study suggested that a virtual visit would allow for a review of the environment, review and reinforce knowledge about the connection and disconnection technique, as well as care at the PD catheter exit site 109 ; though, it should be noted, this was a small, single center, pilot study (n = 30) and there was no follow up of outcomes.
Re-education to prevent peritonitis is also recommended for patients on PD after: prolonged hospitalization; change in the patient's dexterity, vision or mental acuity; change in PD supplies; change in care partner; or after interruption in PD. 89 Most important, after an episode of peritonitis/or peritonitis with an exit-site infection, the authors of guidelines and research studies (as part of multifaceted quality improvement initiatives) have also emphasized that the PD nurse should review with the patient and care partner (in a non-judgemental way) where there was a possible break in the PD procedure or overlooked exit-site infection to try to prevent another episode of peritonitis.89,94,108–111 The latest ISPD recommendation is that the overall peritonitis rate should be no more than 0.40 episodes per year at risk and the percentage of patients free of peritonitis per unit time should be targeted at >80% per year 89 ; for PD catheter exit-site infections, the overall exit-site infection rate should be no more than 0.40 episodes per year at risk. 107 However, an earlier survey observed that not all PD nurses (50%) were aware of their PD units’ peritonitis rate or what it should be. 114
Practice points
Post training, all patients on PD should:
Have access to 24-h telephone support. Be seen in an outpatient PD clinic by Nephrologist/Nurse Practitioner and PD nurse every one to three months (with access to other members of the MDT where available).
Post training, the PD nurse should:
Visit the patient on PD in the patient's home after completion of home training, then as needed with a minimum of yearly home visits. During this home visit, take the opportunity to re-educate the patient (and care partner) as indicated, offer support to the patient, and document and report issues observed back to the Home PD Team Re-educate the patient on PD at each clinic visit, for example, provide each patient (and care partner) simple refreshers on a rotating list of topics Actively participate in MDT meetings to review, discuss and update the patients’ plans of care. During this MDT meeting, take the opportunity to ask questions and learn from the other team members. Review with the patient for possible causes (in a non-judgemental way) after each episode of PD-related peritonitis. Participate in collection of data and review of the PD unit's peritonitis and exit-site infection rates.
Outcomes
There is limited and mostly very low certainty evidence regarding the impact of PD teaching interventions on clinical and patient-reported outcomes. To date, there have only been four RCTs, which have all focused on the effects of retraining on PD infection.65,113–115
In an open-label, parallel-arm RCT involving 104 patients receiving PD from six centers in Korea, Chang et al., 115 reported that, compared with conventional retraining (at week 1 and month 2, n = 53), frequent retraining (at months 4, 5, 6, 7, 8, 10, 12, 15, 18, 21 and 24, n = 51) did not significantly alter the frequency of exit site infection (ESI; primary outcome) or any PD-related infections (including peritonitis) at months 3, 6, 9, 12, 18 or 24, although the event rates of the two groups did change significantly over time. There were also no significant differences in the other secondary outcomes of health-related quality of life (HRQOL), hospitalization, HD transfer or patient survival. Patients aged ≥60 years in the frequent retraining group did experience less peritonitis, although this subgroup analysis of a secondary outcome was exploratory and hypothesis-generating only. Similarly, Ljungman et al. 116 found no significant difference in time to first peritonitis episode (HR: 0.84, 95% CI: 0.65–1.09) in a multi-center, multi-national, parallel arm, open-label RCT of PD retraining at regular intervals (1, 3, 6, 12, 18, 24, 30 and 36 months) versus usual care in 671 incident PD patients across 57 European centers. There were also no significant differences in the secondary outcomes of peritonitis rate, HD transfer or peritonitis-related hospitalization time. In a 3-arm RCT of one-on-one technique inspection every 2 months versus oral education every 2 months versus usual care in 150 incident patients receiving PD at a single Chinese center, Xu et al. 65 observed similar risks of peritonitis in the three groups, although the technique inspection group experienced a lower risk of first non-enteric peritonitis than in the usual care group (HR: 0.33, 95% CI: 0.12–0.92). HD transfer and patient survival were comparable. Finally, in an open-label, parallel arm RCT of a retraining program (a knowledge and practical assessment and a one-on-one retraining session) 90 days after starting CAPD versus usual care involving 130 participants aged ≥55 years at two Hong Kong PD centers, Leung et al. 117 reported no significant differences between the intervention and control groups with respect to peritonitis rates (risk ratio: 0.88, 95% CI: 0.34−2.27, respectively, p = 0.78) and ESI rates (risk ratio: 1.44, 95% CI: 0.66−3.14, p = 0.35). Collectively, the available evidence indicates that retraining may make little or no difference to the risk of PD infection or other PD outcomes, although the certainty of evidence is reduced by high risk of bias, imprecision and/or indirectness.
It should be noted in the above four RCTs on retraining, all the studies had several limitations acknowledged by the authors.65,113–115 The main limitations were: some patients on PD declined to participate in the studies (did not want to attend repeated retraining sessions) or were excluded; others who enrolled in the studies dropped out of the studies or were lost to follow up (death, transfer to haemodialysis, transplantation, transfer to assisted PD, recovered kidney function, transferred to another centre, withdrawal from the study); and, because of low peritonitis rates and the large numbers of patients excluded from the studies, dropped out of the studies or lost to follow up, these studies were underpowered to show significance. Xu et al. 65 suggested that further research is needed to develop multifaceted retraining methods that will be well accepted by patients, while the optimal timing and frequency of retraining needs to be determined.
With respect to other PD teaching interventions, including training methods and educational interventions, a narrative review of 18 non-randomized studies did not identify any intervention which convincingly modified PD outcomes. 3 Most of the studies focused on PD-related infection outcomes and the certainty of evidence was greatly reduced by high risk of bias, imprecision, inconsistency and/or indirectness.
Measures of outcomes
Incorporating patient-reported outcomes into practice
Outcomes have been described in this guideline on the impact of PD teaching interventions on clinical and patient-reported outcomes. Most studies report outcomes relating to PD infections with few reporting quality of life or life participation or other outcomes that may represent patient experiences or more important areas relating to life for a patient on PD. The expectation that research will involve patients’ experiences in order that outcomes are relevant for patients and care partners, as well as health care professionals and researchers, is well documented. 118
This focus on patient experiences has been supported by the Standardized Outcome in Nephrology (SONG) PD initiative. This project involved shared priorities of >900 patients, care partners, and health professionals from 68 countries who identified that PD-related infection, cardiovascular disease mortality, technique survival, and life participation were the four critically important core outcomes to be measured in every clinical trial in PD.119,120 Patients believed life participation, while a subjective measure, depended on how much people wanted to do and would be understood differently for different people, in different cultures. 119 The recently published ISPD guidelines on prescribing PD also recommend that the life goals of the patient should be incorporated into the PD care plan through discussion and shared decisionmaking.121,122 For example, the PD nurse being able to adapt the PD treatment into the patient's daily routine would be considered very important.
Whilst outcomes are important in research, often measures used in research are not used routinely in practice. A shift in thinking therefore is to consider data as an ongoing improvement methodology. Involving the perspectives of patients with kidney failure, including those on PD, has been shown through surveys to be able to monitor for areas of concern and to track improvements in quality care. Patient Reported Experience Measures (PREM) can be powerful in capturing patients’ perspectives in large data sets, as has been shown in the UK. The 2023 survey from the UK of 11,647 patients with kidney failure, indicated that two of the low scoring themes were communication and sharing decisions.123,124 Similar results from the 2022 survey of 252 patients on PD in the province of British Columbia, Canada, indicated that areas for improvement were communication between members of the care team and the patient or family members, and opportunities for collaborative goal setting. 125 Likewise, in a PREM survey under development in the United States, two items ranked highly important by patients on home dialysis were that staff and nephrologists should listen carefully to the patient and support a treatment plan that works for the individual patient. 126 All of these studies indicate the importance of effective communication. PD nurses as well as the whole MDT need to consider ways to enhance and improve their communication with patients and families, as well as how to initiate shared decision making and collaborative goal setting.120,125–127
As part of continuous quality improvement, each local PD unit needs to consider how the patient experience is captured and measured relating to PD training. These appraisals will differ from assessment tools designed to check proficiency of the learner but will provide more detail on effectiveness of communications and patient involvement in setting treatment plans.
Future research
Given the central importance of training by the home PD nurse in being able to successfully maintain a patient on PD at home, this Position Paper aims to provide guidance rather than recommendations on the principles of such training. The authors also acknowledge that there is limited, very low certainty evidence to support these proposals and strongly encourage further research. Future research studies will be required to investigate integration of novel technology and training approaches into the PD training framework and health professionals’ perspectives on its usability for PD, both from PD nurses and patients. There is a need for further robust research to establish evidence to guide best practice on educational interventions. More research is required on (a) the importance of pre-training assessments prior to training to individualize training programs; (b) the education, knowledge, skills and attributes necessary for the home PD nurse; (c) effectiveness and safety of use of other licensed health care nurses and non-health care assistants in a home PD unit; (d) the optimal frequency of PD clinic visits; (e) patient preference for virtual clinic visits versus in-person clinic visits; (f) the optimal frequency and timing of home visits by PD nurses; (g) best practices for or patient outcomes from MDT meetings of the Home PD Team for patients on PD and who should be members of the Home PD Team; (h) research is needed to develop multifaceted retraining methods that will be well accepted by patients, while the optimal timing and frequency of retraining needs to be determined; and, finally, (i) thoughtful consideration on how best to capture and measure the patient experience related to PD training.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Author contributions
All authors wrote, reviewed and edited the manuscript and approved the final version of the Manuscript.