
Abstract
Peritoneal dialysis (PD)-associated peritonitis commonly arises from touch contamination events, however, it is important to be mindful of alternative etiologies and to take a detailed history and perform a root cause analysis for each episode. In fact, the PD effluent can be a window into intra-abdominal pathologies which may require surgical management. We present an unusual case of secondary enteric peritonitis due to foreign body bowel perforation from ingestion of a fish bone.
A 71-year-old female receiving automated peritoneal dialysis (APD) described a 3-day history of progressively worsening abdominal pain. The peritoneal effluent was cloudy and turbid. Initial peritoneal dialysis (PD) effluent cell counts demonstrated a total white count of 10,750 cells/μL (98% neutrophils). A presumptive diagnosis of peritonitis was made, and the patient was empirically started on intraperitoneal vancomycin and tobramycin. The peritoneal effluent culture reviewed a polymicrobial peritonitis with Klebsiella pneumoniae, Enterobacter cloacae, Streptococcus mitis, and Streptococcus anginosus. Given the polymicrobial nature of the peritonitis, a CT scan of the abdomen was performed demonstrating a radio dense object perforating the small bowel (Figure 1). The impression of the radiologist was that of a penetrating fishbone.
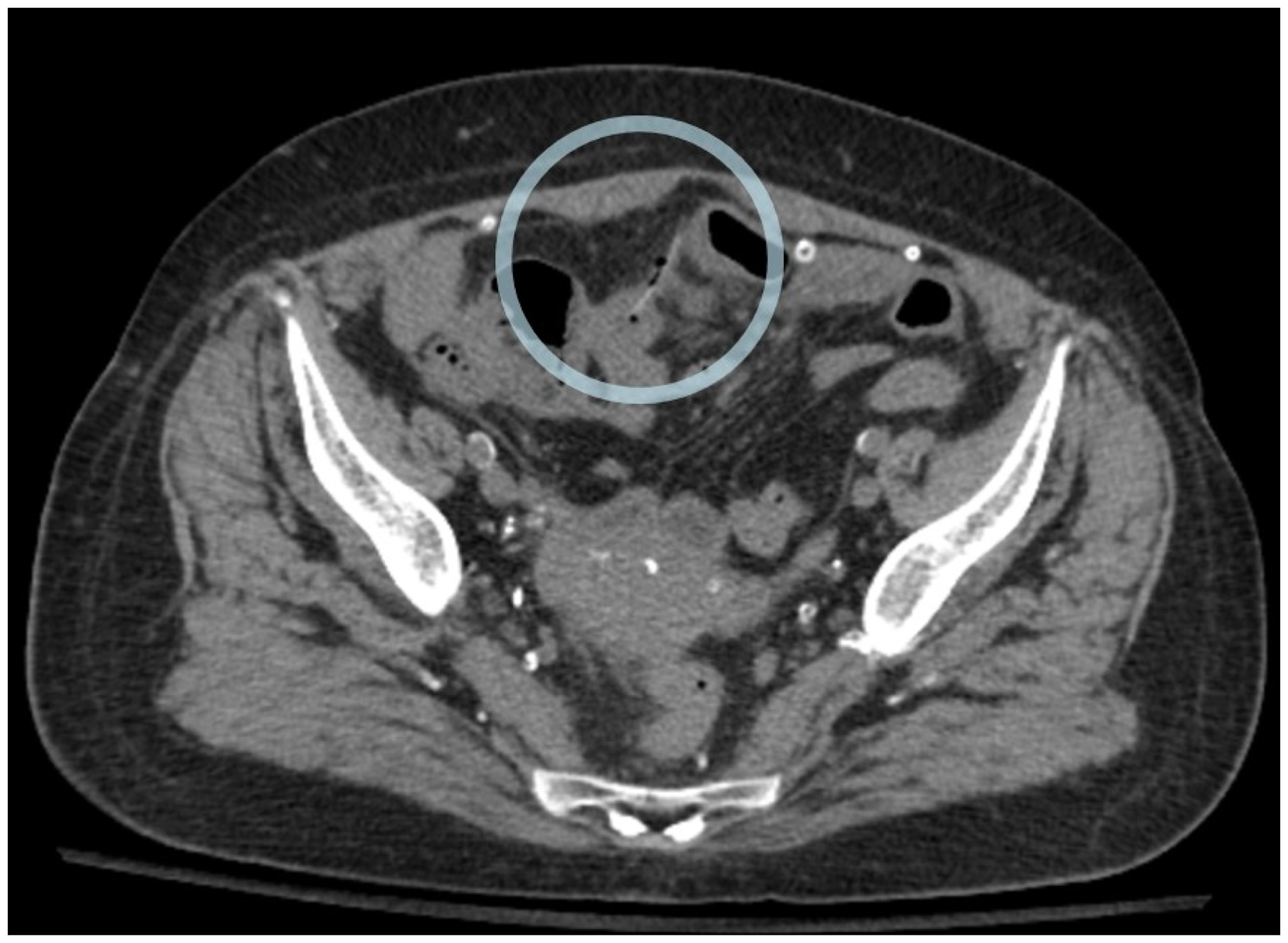
A 2.5 cm linear dense foreign object perforating an ileal loop in the central pelvis with extraluminal gas bubbles.
On initial assessment, the patient did not report any changes to dietary habits, changes to bowel frequency or quality, and no contaminating events. She had no history of chronic abdominal pain and no prior history of PD-associated peritonitis. After the computed tomography (CT) findings were suggestive of a penetrating fishbone, a retrospective history was obtained specifically inquiring about fish ingestion. The patient described breaking a period of vegetarianism by ingesting the fish, Gerres oyena or common silver-biddy, 3 days prior to the onset of her pain, and 6 days prior to her presentation with cloudy effluent.
Admission to hospital and surgical consultation was obtained, and the patient underwent emergent laparoscopic foreign body retrieval, primary repair of enterotomy and omental patch. Intra-operative photograph was obtained by the surgical team demonstrated the fishbone piercing through the bowel wall (Figure 2). The PD catheter was left in situ but PD halted. Postoperatively, the patient improved clinically with resolution of her abdominal pain, however, a PD effluent sample obtained on postoperative day 7 demonstrated an elevated white cell count of 7321 cells/μL (89% neutrophils) with a negative culture. A subsequent effluent sample on postoperative day 14 demonstrated a persistent white cell count of 622 cells/μL (52% neutrophils) with growth of Bacillus infantis. A CT scan with enteric contrast was performed and did not demonstrate any ongoing bowel perforation or injury. Given the refractory peritonitis, the patient underwent surgical PD catheter removal and was transitioned to home hemodialysis.

Fishbone exiting the ileum with surrounding purulence at the site of perforation.
Peritonitis secondary to visceral injury is associated with significantly increased mortality compared to all-cause peritonitis.1 The 2022 International Society for Peritoneal Dialysis (ISPD) peritonitis guidelines recommend consideration of a secondary enteric etiology in cases of polymicrobial peritonitis with involvement of enteric pathogens.2 Abdominal imaging and surgical assessment are warranted in such cases. Typically, in cases of PD-associated peritonitis secondary to bowel perforation, the PD catheter is removed at the time of abdominal surgery. In this case, retention versus removal of the PD catheter was not explicitly discussed between the surgical and nephrology teams resulting in the ultimate retention of the catheter. Upon reflection, this highlights the importance of proper communication between various specialties. Ideally, decisions around PD catheter management should be made in a multidisciplinary manner with input from the surgical, dialysis, and infectious disease care teams.
In conclusion, we described a case of polymicrobial, enteric peritonitis secondary to bowel perforation. Our case highlights the importance of considering intra-abdominal pathologies which require surgical intervention upon the diagnosis of PD-associated peritonitis particular in the context of multiple enteric organisms.
Footnotes
Declaration of conflicting interests
Jeffrey Perl has received consultant fees from Baxter Healthcare, Davita Healthcare, Otsuka Canada, AstraZeneca Canada and liberDi Dialysis. He has also received honoraria from Baxter Healthcare, Davita Healthcare, Fresenius Medical Care, AstraZeneca Canada and US Renal Care. He holds stock or stock options in liberDi Dialysis. Jeffrey Perl is the editor-in-chief of Peritoneal Dialysis International and had no role in the editorial handling of this manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed consent to participate
Written consent was provided by the patient to publish this case report.