
Abstract
Peritoneal dialysis-associated peritonitis (peritoneal dialysis (PD) peritonitis) is a common complication of peritoneal dialysis associated with adverse events and mortality. Outcomes are poorer when two or more organisms are isolated in the dialysis effluent culture, known as polymicrobial PD peritonitis, which can be caused by an underlying secondary process, such as gastrointestinal tract pathology and, rarely, a foreign body. Here, we report a case of polymicrobial PD peritonitis due to a vegetable matter foreign body perforating the colon. The patient was conservatively managed with antibiotic treatment and subsequent colonoscopic removal of the foreign body without the need for peritoneal dialysis catheter removal. She continues to remain on peritoneal dialysis 18 months after the PD peritonitis episode.
Case description
A 67-year-old female with end-stage kidney disease on continuous cycling peritoneal dialysis (CCPD) presented to the emergency department with 1 day of abdominal pain and cloudy effluent. She was afebrile and tender on palpation to her lower abdomen, worst in the right lower quadrant. Her peritoneal dialysis (PD) catheter exit site appeared clean with no signs of tunnel or exit-site infection.
Her investigations revealed a normal white blood count (WBC) and a mildly elevated lactate of 2.5 mmol/L. Dialysis effluent was cloudy, and peritoneal fluid WBC was 14,878 × 106/L with 83% neutrophils. Her presentation appeared consistent with peritoneal dialysis-associated peritonitis (PD peritonitis).
She was empirically treated with intraperitoneal (IP) cefazolin and ceftazidime. Effluent culture grew Klebsiella pneumoniae, Enterobacter cloacae, viridans group streptococci, and Bacteroides cellulosilyticus, B. ovatus, and B. thetaiotaomicron, then was negative after 3 days of antibiotic treatment with improving daily cell counts (Table 1). As there was K. pneumoniae resistance and growth of anaerobic organisms, the patient's antibiotics were changed to IP cefazolin, tobramycin, and oral metronidazole. Antifungal prophylaxis with nystatin was prescribed.
Patient symptoms and lab investigations in response to treatment.
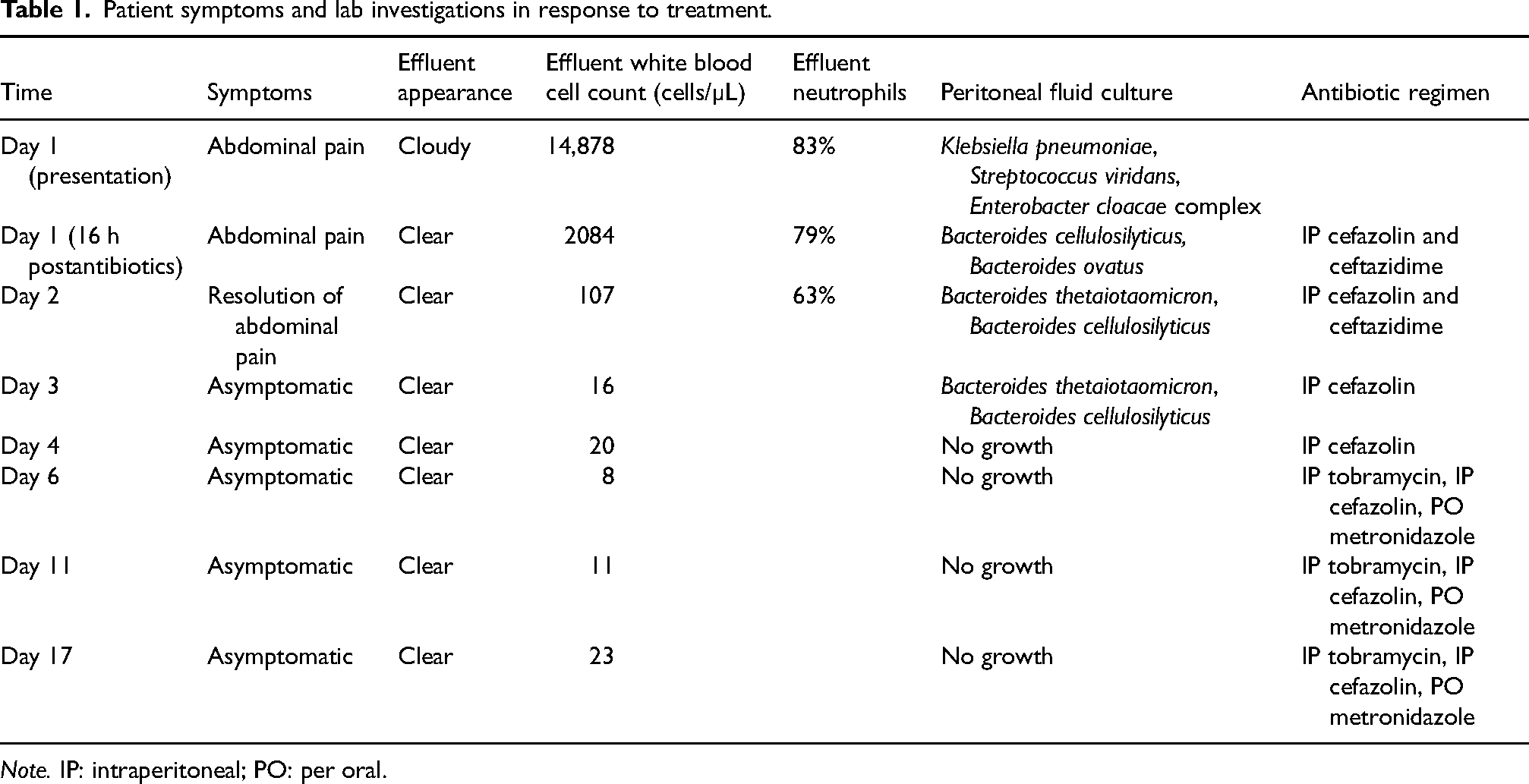
Note. IP: intraperitoneal; PO: per oral.
Due to the polymicrobial peritonitis concerning for possible gastrointestinal pathology, a computed tomography (CT) scan of the abdomen was performed revealing a thin linear hyperdense structure measuring ∼3 cm in length appearing to traverse the wall of the descending colon from the lumen to the adjacent mesentery without evidence of focal inflammation or surrounding locules of gas to suggest perforation (Figure 1).
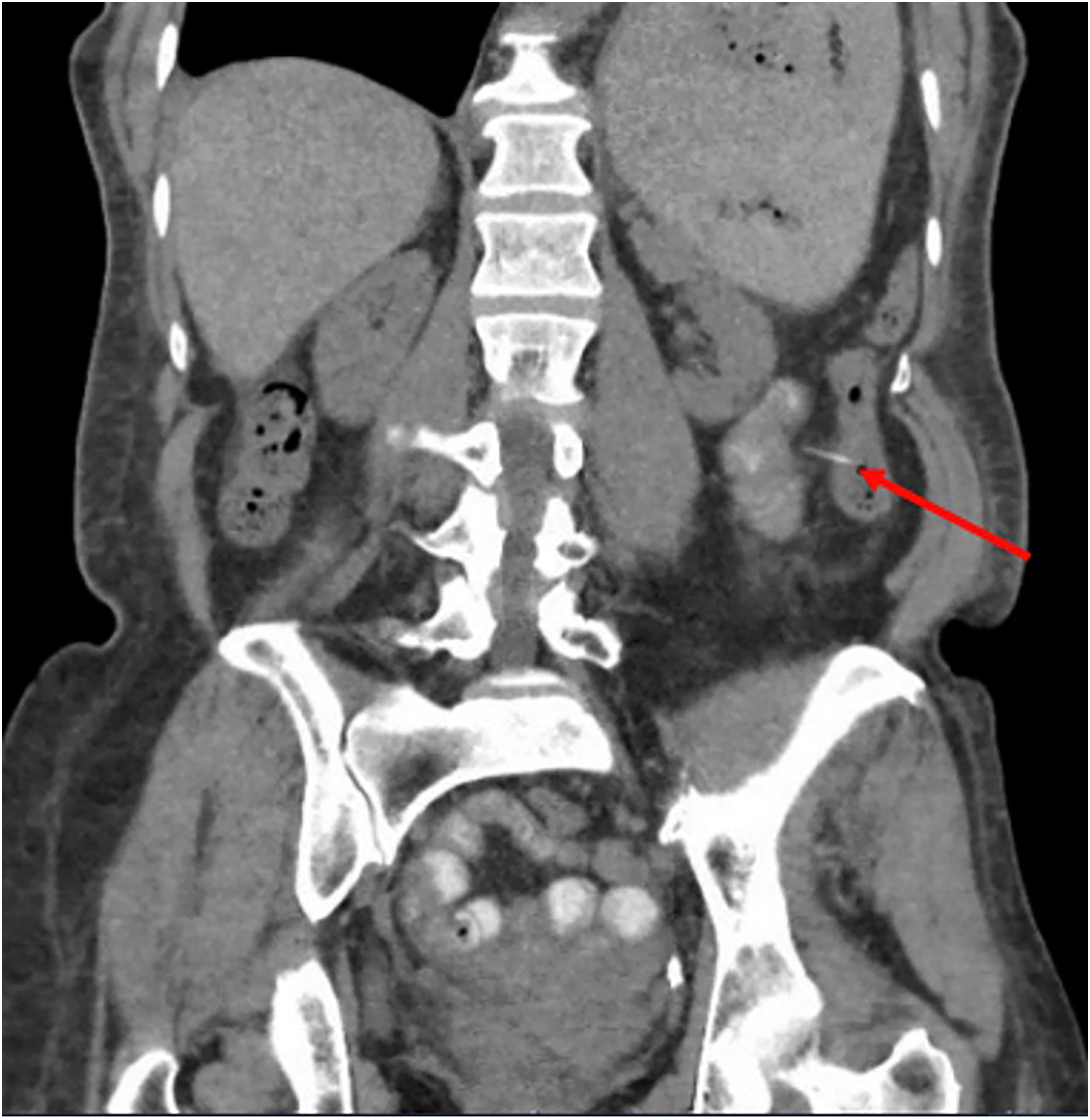
Abdominal computed tomography revealing the presence of a colonic foreign body. The arrow points to ∼3 cm hyperdense linear structure traversing the wall of the descending colon from the lumen to the adjacent mesentery.
Gastroenterology was consulted and performed a colonoscopy, whereby they visualized and removed a 3 cm soft linear foreign body from the ascending colon (Figure 2). The foreign body, resembling an apple stem, was sent to pathology and analysis revealed the foreign body was composed of vegetable matter (Figure 3). The patient denied any known ingestion that was directly responsible for the linear foreign body.
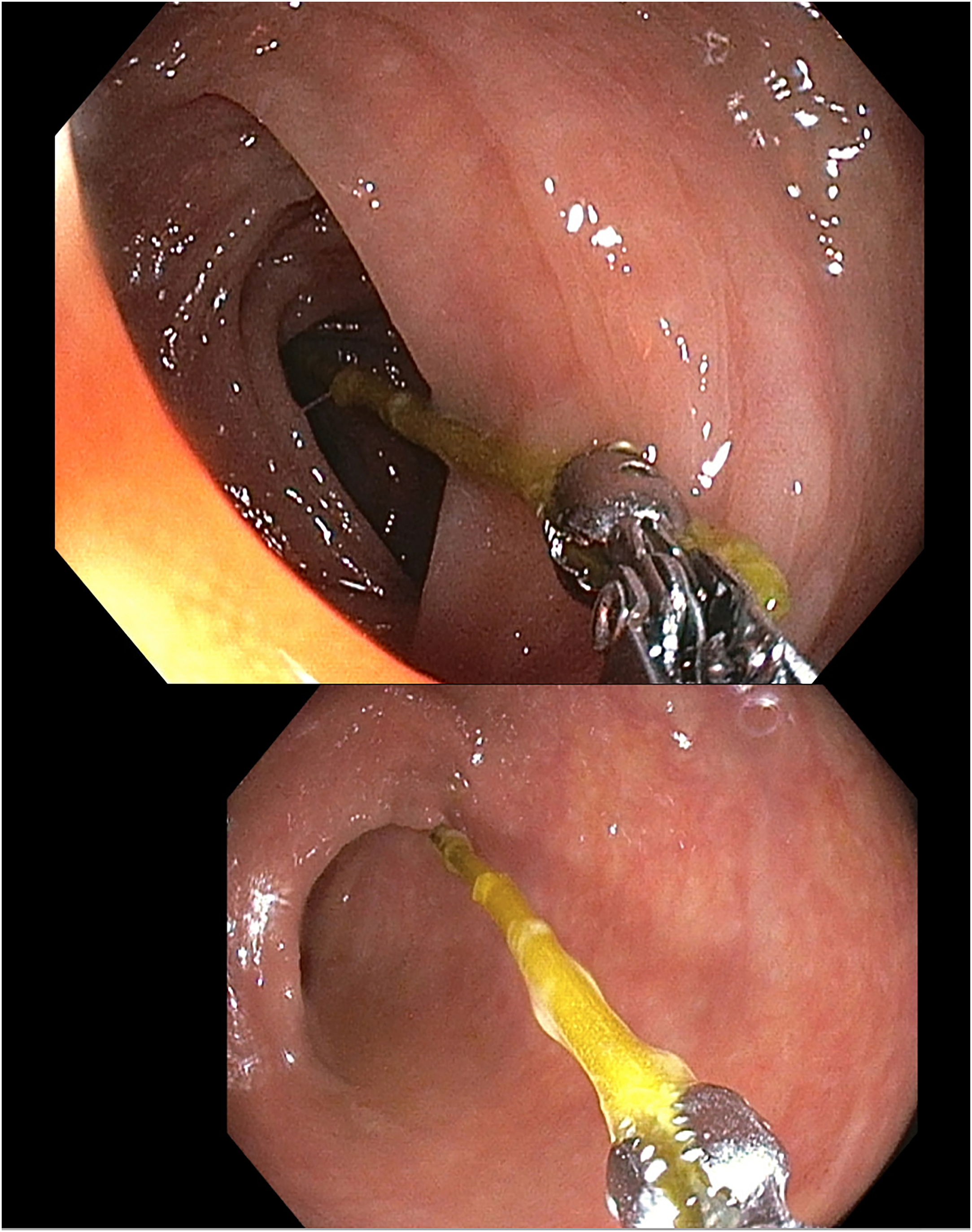
Endoscopic retrieval of a foreign body.
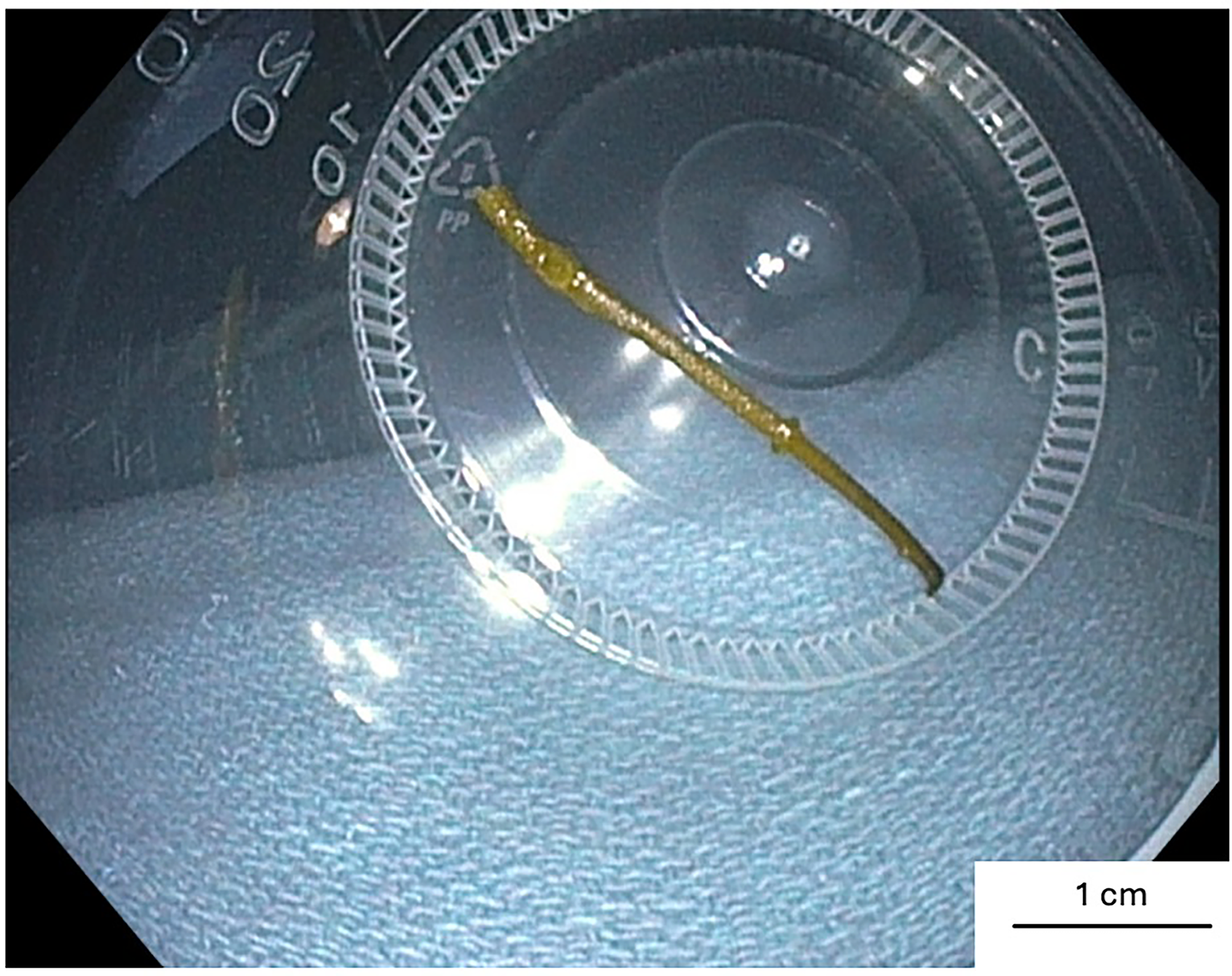
Vegetable matter foreign body.
After the vegetable matter foreign body was removed, PD was held for 2 days, then the patient resumed CCPD and completed a total of 3 weeks of IP cefazolin, tobramycin and oral metronidazole. Currently, she remains on PD 18 months after this episode of foreign body PD peritonitis.
To conclude, foreign bodies have been identified as a rare cause of PD peritonitis by way of bowel perforation and infection through adherent biofilm.1,2 It is estimated that 80% of foreign bodies pass through the gastrointestinal tract asymptomatically and endoscopic removal is required in ∼20%. 3 Perforation, usually due to sharp foreign bodies, occurs in < 1% and can be fatal. 4
In other cases, foreign bodies may erode through the bowel wall into the abdominal cavity without causing leakage of bowel contents and are found incidentally on imaging. 5 It is thought that the rates of detection of foreign bodies will continue to rise due to the increased use of imaging modalities such as CT scans and an aging population.2,6 Optimal management of gastrointestinal foreign bodies causing PD peritonitis is often challenging and requires a comprehensive approach determined on an individual basis.
Footnotes
Acknowledgements
None.
Authorship
MC wrote the manuscript; TM reviewed and edited the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed consent to participate
Not applicable.
Informed consent to publish
Not applicable.