
Abstract
Peritoneal dialysis (PD) was historically the initial kidney replacement modality of choice for patients admitted to the intensive care unit, and there are several advantages to maintaining critically ill PD patients on their usual dialysis therapy. However, in this patient population, there are two contentious questions: how are the respiratory dynamics of mechanical ventilation impacted by the presence of dialysate within the abdomen, and what can be done to mitigate these potential effects? This review discusses the theoretical impact of PD on intra-abdominal pressure (IAP) and evidence for the effect of IAP on respiratory mechanics in mechanically ventilated PD patients.
Introduction
Peritoneal dialysis (PD) was historically the initial kidney replacement modality (KRT) of choice for patients admitted to the intensive care unit (ICU). 1 Although its popularity within ICUs has waned with increasing use of extracorporeal therapies (intermittent hemodialysis (IHD), slow low efficiency dialysis and continuous kidney replacement therapy), there are advantages to maintaining critically ill PD patients on their usual dialysis therapy. These include: reduced infrastructure requirements, improved hemodynamic tolerance, avoidance of additional vascular access procedures and their associated risks and avoidance of systemic anticoagulation. 2 Moreover, PD has been shown to be non-inferior to extracorporeal modalities for patients with AKI, and is endorsed by the International Society for Peritoneal Dialysis (ISPD) as an acceptable form of KRT for patients with AKI in all settings. 1 The focus of the current discussion, however, will be on the patient treated with maintenance PD who is admitted to the ICU.
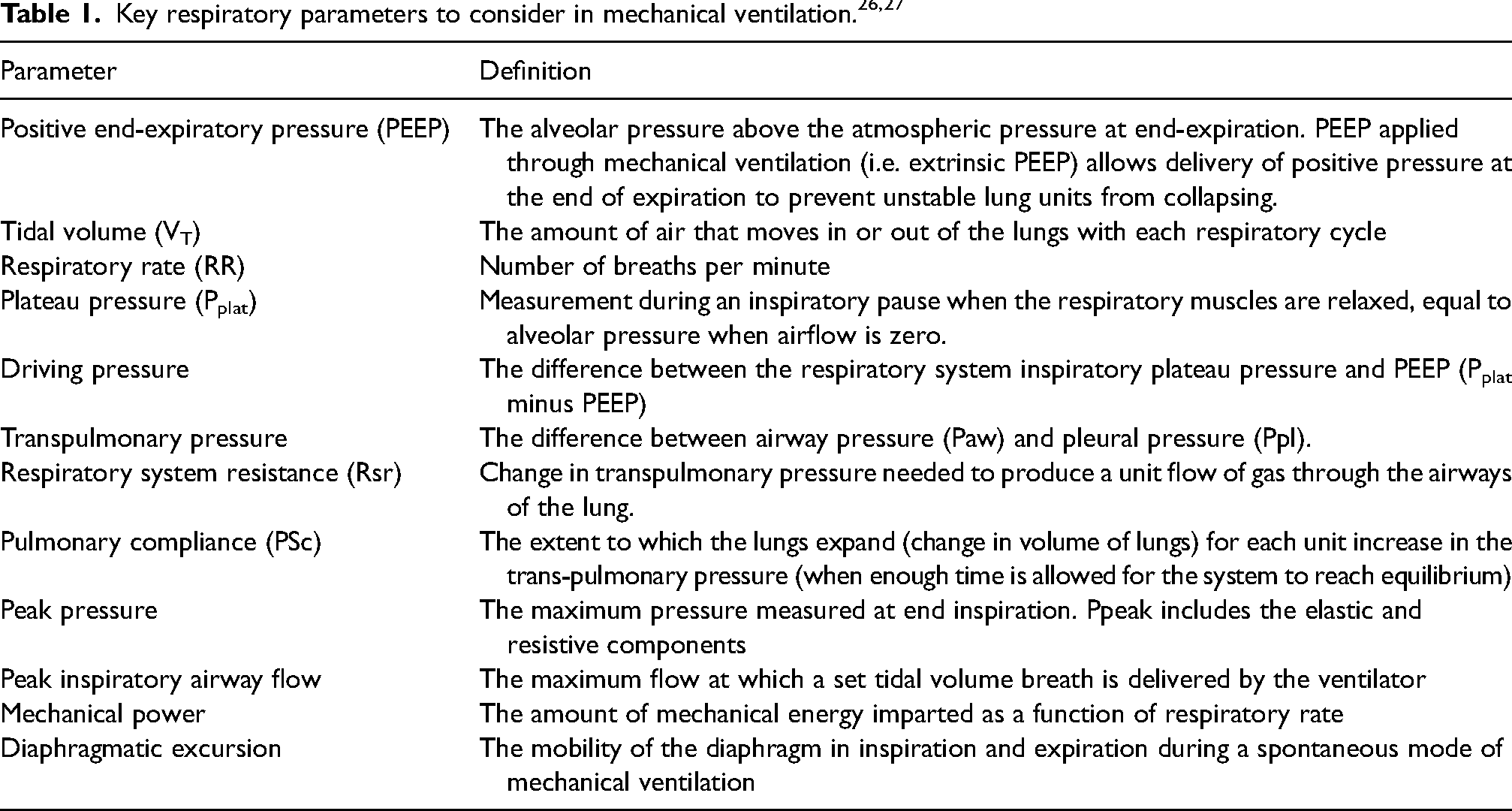
For critically ill PD patients presenting with respiratory failure, there are two contentious questions: how are the respiratory dynamics of mechanical ventilation impacted by the presence of dialysate within the abdomen, and what can be done to mitigate these potential effects? This remains a frequent topic of discussion in the collaborative management of these patients between nephrologists and intensivists. In critically ill patients with respiratory failure, mechanical ventilation is necessary to promote gas exchange and assist respiratory muscles in ventilating the lung – a brief overview of key respiratory parameters to consider is summarized in Table 1. A common concern with continuation of PD in the ICU pertains is the potential risk of increased intra-abdominal pressure (IAP) due to the instillation of dialysate that could theoretically compromise the effectiveness of mechanical ventilation and respiratory dynamics.
Intra-Abdominal pressure
According to the World Society for the Abdominal Compartment Syndrome (WSACS) 2013 Guidelines, IAP is defined as the steady-state pressure within the abdominal cavity. 3 The normal IAP is approximately 5–7 mmHg in critically ill adults, while intra-abdominal hypertension (IAH) is defined as IAP that is 12 mmHg or greater (and further sub-classified according to the magnitude of its elevation). Abdominal compartment syndrome (ACS) is defined as a IAP of 20 mm Hg or greater with new organ dysfunction. 3
Risk factors for IAH include: high body mass index (BMI), abdominal surgery, liver dysfunction/ascites, hypotension/vasoactive therapy, respiratory failure and excessive fluid balance. 4 Conversely, the risk of IAH is minimal in mechanically ventilated patients with positive end-expiratory pressure (PEEP) < 10 cmH2O, PaO2/FiO2 > 300 and BMI <30. 4 Slight increases in IAP from a higher starting value have been described to have limited implications in critically ill patients; for instance, an IAP of 16 mmHg may be insignificant if a baseline was 13 mmHg, whereas this could cause organ injury if the baseline value was 6 mmHg, 3 which is relevant when considering patients with obesity 5 or those with fluid chronically in their peritoneal space (PD patients, liver disease patients with ascites). However, in clinical practice, the baseline IAP value is usually unknown and the effect is difficult to quantify.
Peritoneal dialysis and IAP
In ambulatory patients, PD is known to affect respiratory mechanics and diaphragmatic function via its impact on IAP..6,7 Among patients with normal respiratory function at baseline, 2L of dialysate dwelling during continuous ambulatory peritoneal dialysis (CAPD) resulted in a statistically significant reduction of maximum inspiratory and expiratory pressures, 8 while a separate study showed reduction in total lung capacity, vital capacity and functional residual capacity with the same volume of dialysate. 9 Conversely, studies have suggested potential for diaphragmatic adaptation in its force-length relationship in CAPD patients in the sitting position, which could improve breathing mechanics, potentially via tonic stretching of the diaphragm from the dialysate fluid.10,11
For critically ill patients, the impact of IAP on respiratory mechanics may be expected to differ (compared to ambulatory patients), given that they are usually in the supine position. A single-centre prospective cohort study of 20 mechanically-ventilated patients with acute kidney injury (AKI) who underwent a total of 44 high-volume PD sessions (using automated cyclers, a dialysate volume of 2L per cycle and 18–22 exchanges per day) 12 showed that 45% of patients had increased IAP (>7mmHg) at baseline, and with PD treatment, IAP showed only a temporary increase, returning to near baseline on the third day of dialysis. More specifically, the IAP in the dry state was 8.3 +/–4.4 mm Hg, increased to 12.5 +/–6.3 mm Hg in the filled state, and subsequently decreased to 9 +/–4.2 mm Hg post-dialysis (in the dry state). Despite this temporary increase in the IAP, patients treated with PD had a progressive increase in pulmonary compliance and improvement in their PaO2/FiO2 ratio from 239 +/–84 to 266 +/–88 (i.e. no impairment to respiratory mechanics). The same group subsequently compared respiratory mechanics in mechanically-ventilated patients during high-volume PD versus IHD. 13 They likewise showed a progressive improvement in pulmonary compliance and oxygenation (which was attributed to achieved ultrafiltration), and a stable ventilatory mechanics resistance. Outcomes for the PD and IHD groups were similar in terms of oxygenation and pulmonary compliance, though the IHD group did have a larger improvement in respiratory system resistance compared to the PD patients. 13
In mechanically-ventilated patients, the supine position affords the lowest IAP, as compared to the semi-recumbent position (head of bed at 30 degrees or 45 degrees elevation), which increases the IAP by ∼4 and 9 mm Hg respectively. 5 Supine IAP has been shown to positively correlate with BMI and comorbidity6,14; meanwhile, time on maintenance PD and daily total ultrafiltration has been shown to have a negative correlation with IAP. 14 These clinical features, as well as other risk factors for increased IAP including, positive fluid balance and vasoactive therapy 4 are important considerations when tailoring the PD prescription for critically ill patients and deciding whether PD remains feasible in the context of their critical illness. For critically ill PD patients who are ventilated, their dialysis can be optimized with a greater number of cycles, increased time on the cycler in a 24-h period (e.g. 8 cycles per 24-h period), and the use of hypertonic solutions (if necessary) to achieve both adequate clearance and ultrafiltration. Such prescriptions have been shown to be feasible in randomized trials studying use of PD in AKI15,16 and could allow for a reduction in fill volumes, if necessary, to manage IAP.
Finally, should respiratory parameters (such as those described in Table 1) be disturbed and thought to be attributable to PD, the presence of a PD catheter allows for immediate evacuation of fluid to mitigate this. Furthermore, ultrafiltration can be intensified by using hypertonic solutions to improve the overall fluid status of patients without requiring hemodialysis and the procedural-related risks associated with switching. 13
PD and proning (COVID-19)
Numerous publications have demonstrated the feasibility of achieving successful outcomes with PD in critically ill patients requiring prone position ventilation for COVID-19 pneumonia, particularly in the context of resource constraints that characterized the pandemic, including the limited availability of extracorporeal therapies.17–19 In one case series of seven patients, acute PD was successfully implemented without detrimental effects on respiratory mechanics or need for modality change. The main complication was fluid leakage (in 71% of patients), but this was noted as mild and readily resolved. 17 Similar results were shown in a study with 37 patients performing acute PD after bedside PD catheter insertion – no adverse events were reported, and patients had similar Sequential Organ Failure Assessment (SOFA) scores and ventilation requirements before and after PD catheter insertion with adequate KRT parameters achieved. 18
Given the intermittent nature of proning (e.g. occurring multiple times per day), manual exchanges are often performed to minimize interruption of their dialysis – this therefore requires extensive collaboration among the ICU team, nephrologists and allied health in coordinating the delivery of therapy.
Ascites and intra-abdominal pressure
There is literature suggesting that ascitic fluid in patients with liver disease can impair respiratory dynamics, mainly by a decrease in chest wall compliance, causing increased work of breathing.20,21 A study of eight cirrhotic outpatients with tense ascites showed the development of a high lung elastic load and positive end-expiratory alveolar pressure even in the supine position, and that large volume paracentesis (>3.5L in all cases) unloaded the inspiratory muscles, decreasing their activation and consequently improving respiratory function. 21 Further substantiating this, a study of 30 ambulatory patients with cirrhosis and ascites performed pre- and post-paracentesis evaluations and found improvement in ventilatory parameters, as well as a subjective reduction in dyspnea and fatigue. 22
However, there is a paucity of literature describing the effect of ascitic fluid on IAP or respiratory mechanics in critically ill patients undergoing mechanical ventilation, despite the fact that liver disease and ascites are often cited as a risk factor for development of IAH. This likely relates to the fact that clinicians are hesitant to place patients with severe liver failure on mechanical ventilation due to their high mortality risk and poor prognosis.23,24
A ventilated patient with ascites can be treated with paracentesis to lower the IAP, to address any respiratory mechanics deemed to be affected by IAP. While PD patients are similar in that they have fluid in their abdomen dwelling for periods of time, the fill volumes and dwell times typically are adjusted to minimize any perturbation in IAP that could affect respiratory dynamics – fill volumes for PD are generally lower than the volume of ascitic fluid in cirrhotic patients (e.g. 2L or less as opposed to >3.5L), and drainage of the fluid on the cycler is done more frequently than paracenteses. Notably, the higher volumes of ascitic fluid (compared to PD fill volumes) would be expected to confer a more pronounced increase in IAP and potentially influence respiratory mechanics to a greater degree. 25
Instances where PD may not be the best option
There are clinical scenarios where extracorporeal therapies are favoured over PD. For instance, the treatment of toxicities or severe metabolic disturbances requiring rapid correction (e.g. life-threatening hyperkalemia) may necessitate enhanced clearance via emergent IHD. From a volume perspective, there are also instances where hemodialysis or continuous kidney replacement therapy may be favoured due to the speed at which fluid can be removed – for example, severe acute respiratory distress syndrome or flash pulmonary edema may necessitate emergent ultrafiltration that can be more rapidly achieved with hemodialysis. However, one must also consider the time taken to insert a vascular access for hemodialysis and assemble the equipment and personnel required to carry out the therapy. Depending on the amount of time this takes, the use of a hypertonic 4.25% solution via a patient's existing PD catheter may be more time-efficient, given that 300–400 mL per hour of ultrafiltration can be achieved early in the dwell. The development of abdominal catastrophe (peritonitis from a visceral source) or abdominal surgeries that breach the integrity of the peritoneal cavity would also preclude continuation of PD. Finally, in all ventilated patients receiving PD, regular monitoring should be done for complications of their dialysis therapy such as movement of the PD fluid from the peritoneal to the pleural cavity (PD hydrothorax) that could be indicative of ACS and suggestive of the need to transition from PD to an extracorporeal modality.
Conclusion
The management of a PD patient who is critically ill and mechanically ventilated presents several challenges, in part due to uncertainty about the impact of dialysate on IAP and respiratory dynamics. Despite this concern, the current literature suggests that maintaining most patients on PD has no significant detrimental effects on their mechanical ventilation parameters or respiratory outcomes. PD patients in the ICU must have their respiratory parameters continually re-assessed to determine whether their dialysis prescription can be optimized to meet ultrafiltration or clearance goals, and to ascertain whether a change in clinical status warrants transitioning to an extracorporeal therapy. Continuous collaborative discussions between intensive care and nephrology teams are essential to advancing the care of this patient population.
Footnotes
Author contributions
Conceptualization: Robert R. Quinn, Joanne M. Bargman. Data curation: Ryan J. Chan, Robert R. Quinn, Joanne M. Bargman. Supervision: Robert R. Quinn, Joanne M. Bargman. Writing – original draft: Ryan J. Chan. Writing – review & editing: Ryan J. Chan, Robert R. Quinn, Joanne M. Bargman.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.