
Abstract
Background:
Peritoneal dialysis (PD) technique survival is an important outcome for patients, caregivers and health professionals, however, the definition and measures used for technique survival vary. We aimed to assess the scope and consistency of definitions and measures used for technique survival in studies of patients receiving PD.
Method:
MEDLINE, EMBASE and CENTRAL databases were searched for randomised controlled studies (RCTs) conducted in patients receiving PD reporting technique survival as an outcome between database inception and December 2019. The definition and measures used were extracted and independently assessed by two reviewers.
Results:
We included 25 RCTs with a total of 3645 participants (41–371 per trial) and follow up ranging from 6 weeks to 4 years. Terminology used included ‘technique survival’ (10 studies), ‘transfer to haemodialysis (HD)’ (8 studies) and ‘technique failure’ (7 studies) with 17 different definitions. In seven studies, it was unclear whether the definition included transfer to HD, death or transplantation and eight studies reported ‘transfer to HD’ without further definition regarding duration or other events. Of those remaining, five studies included death in their definition of a technique event, whereas death was censored in the other five. The duration of HD necessary to qualify as an event was reported in only four (16%) studies. Of the 14 studies reporting causes of an event, all used a different list of causes.
Conclusion:
There is substantial heterogeneity in how PD technique survival is defined and measured, likely contributing to considerable variability in reported rates. Standardised measures for reporting technique survival in PD studies are required to improve comparability.
Introduction
Transfer from peritoneal dialysis (PD) to haemodialysis (HD) increases the risk of mortality 1 and healthcare costs by about threefold at 3 years 2 when compared to continuing of PD. While national and international registries show marked variability in the rates of transfer to HD across centres, 3,4 approximately one-third of the patients on PD will transfer to HD within 5 years of commencing PD. 5 Perceptions of technique survival may affect modality selection decisions and clinician perceptions of the value of the modality. The Standardised Outcomes in Nephrology-Peritoneal Dialysis (SONG-PD) initiative, based on the shared priorities of patients, caregivers and health professionals, identified technique survival as a critically important core outcome to be reported in all studies in patients receiving PD. 6
Despite the importance of this outcome, the terminology used in the literature is not consistent, with technique failure and technique survival both used. Both of these terms produce ambiguity in the events that comprise the outcome, particularly with respect to death. The SONG-PD process recommended technique survival as the preferred terminology to avoid the negative connotation of technique failure, although this leaves it unclear how to refer to specific events.
There is no widely accepted definition available for technique survival or transfer to HD. Important considerations in the definition include whether stopping PD is sufficient or if the use of HD is required, the duration of HD required, whether transplantation, death or recovery of kidney function are included, and the population to which this definition should be applied. Indeed, variability in the duration of HD required has already been shown to affect the reported rate of technique survival. For example, according to an analysis of the Australia and New Zealand Dialysis and Transplant (ANZDATA) registry, the rate of patients returning to PD by 1 year was 24% using the definition of minimum HD duration of 30 days, compared to 3% when 180 days were used. 7 Furthermore, causes of transfer to HD are varied, including peritonitis, patient choice and catheter problems, and no consensus exists on the recording or reporting of cause-specific transfer to HD across studies. 8
The aim of this study was to assess the scope and variability of the definitions of technique survival used in PD studies and to assess the different methodologies used to report rates and risk factors for transfer to HD. This was to better inform the development of a standardised measure for technique survival in PD, a necessary step to ensure consistent reporting of outcomes to enable direct comparisons of the effect of interventions across studies, thereby improving research efficiency, decreasing research waste and accurately informing decision making for all stakeholders, including patients, caregivers and clinicians.
Methods
Terminology
We used technique survival when discussing the outcome generally, the actual event (death, transfer to HD) when necessary for clarity and technique failure only when this was the specific term used in the included articles.
Search and selection criteria
The study review protocol was registered with PROSPERO 9 and conforms to the Preferred Reporting Items for Systematic reviews and Meta-Analyses checklist. 10 Studies eligible were randomised controlled studies (RCTs) reporting technique survival as an outcome or adverse event. All interventions were included. Patients aged 18 years or over who were currently or previously on PD for at least 1 day were included in the analysis. Studies not published in English and observational studies were excluded.
MEDLINE, EMBASE and the Cochrane Central Register of Controlled Trials (CENTRAL) were searched from database inception (1964, 1947 and not applicable due to composite nature, respectively) to December 2019, with the search strategy provided in Supplementary Material. Medical subject headings and free-text terms for PD, continuous ambulatory PD, continuous cyclic PD, technique failure, technique survival and transfer to HD were combined with the search filter for RCTs. Titles and abstracts were screened by two of three assigned reviewers (EE and MT or MH) with studies excluded if they did not meet the inclusion criteria. The full manuscripts of potentially eligible studies were then reviewed by two reviewers (EE and MT or MH) for inclusion. Any disagreement was resolved through discussion and by a third reviewer if necessary.
Data extraction
Data extraction into a standardised spreadsheet was completed by two reviewers independently (EE and MT or MH), with each entry cross checked and inconsistencies discussed until resolved. In the case of multiple publications of a study, these were highlighted and grouped. Authors of articles were contacted if needed for clarifications regarding additional unpublished data.
Study setting, population and demographics were collected alongside the number of participants randomised and analysed, inclusion criteria (first PD episode or any PD episode, PD within a certain duration of kidney replacement therapy (KRT) commencement, inclusion from the start of KRT or from the defined time period after the start of KRT), country (or centre/s) and the number of events. Definitions recorded were PD start (catheter insertion, start or end of training and exchange for solute clearance) and definition of technique survival/technique failure/transfer to HD (duration of HD required, inclusion or censoring of other events, such as death or transplantation). Results extracted were the measure used (rate/probability/time to event), value reported with standard deviation and/or standard error/confidence interval, missing data and rates of loss to follow up. Reasons for transfer to HD were summarised as: if reported (y/n), list of reasons included, number of reasons allowed (one or more) and proportion of events by reason. Administrative censoring rates, if reported, were included alongside death, transplant and recovery of kidney function rates and measures used. Missing data were coded as missing.
Results
Study characteristics
From the 200 articles retrieved, 25 studies were included (Figure 1), of which 2 were multinational and 13 were multicentre with 12 single centres. Four studies included children and adults. 11 –14 No studies included children only. All included studies were parallel-design RCTs, where various interventions were examined: eight studies of PD solution (16–18, 24, 26–29 and 1022 participants), one study of PD modality (chronic ambulatory PD vs. continuous cyclic PD) (14 and 82 participants), eight studies of type of catheter/connector (11–13, 15, 19, 22, 30, 32 and 1360 participants), four studies of exit site treatment (20–21, 31, 35 and 781 participants), one study of timing of commencement of PD (25 and 122 participants), one study of subcutaneous implantation of PD catheter (23 and 59 participants), one study of the number of dialysate exchanges (34 and 139 participants) and one study of treatment of peritonitis (33 and 80 participants).
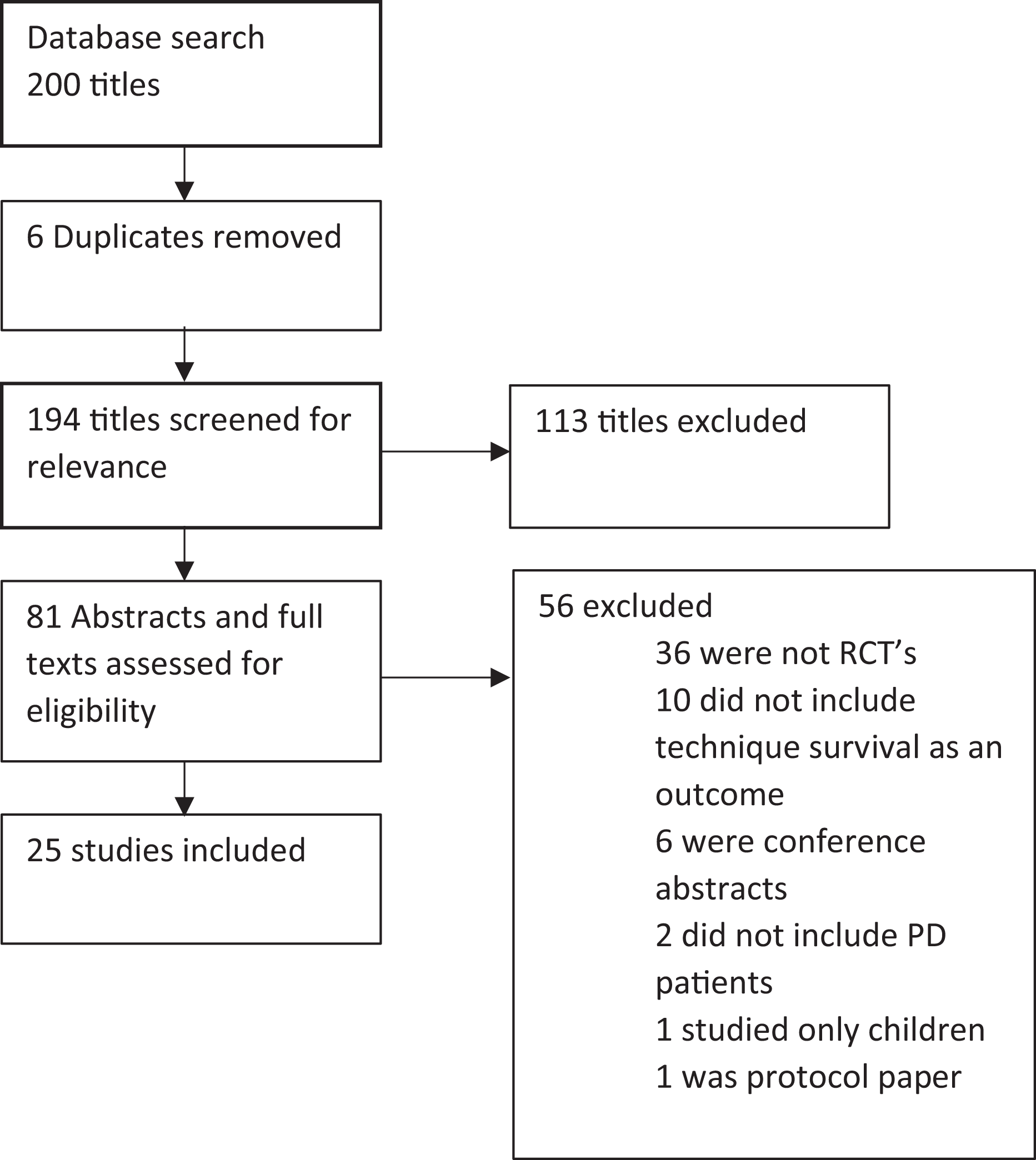
Flowchart for data extraction and reasons for exclusion of studies.
The year of publication ranged from 1994 and 2019. The follow up time ranged from 6 weeks to 4 years with a median follow up time from 3 months to 34 months. The median number of total participants in the studies was 145, ranging from 41 to 371 with 3645 participants over all studies. (Table 1) Technique survival was a secondary outcome in 20 studies (11, 13, 15–17, 19–26, 28, 30–35 and 2970 participants), included in a list of outcomes in three studies, where the primary outcome was not clear (12, 14, 29 and 223 participants) and listed as an outcome in two articles, which were secondary analyses of studies (18, 27 and 452 participants).
Characteristics of included studies.
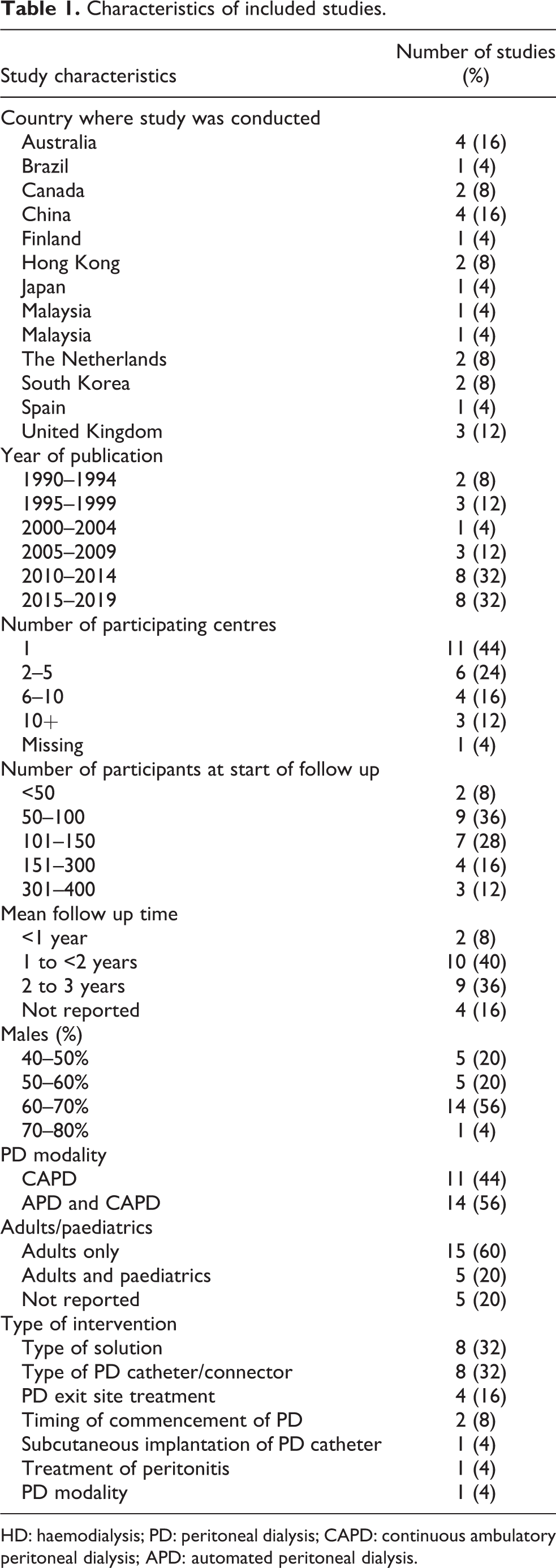
HD: haemodialysis; PD: peritoneal dialysis; CAPD: continuous ambulatory peritoneal dialysis; APD: automated peritoneal dialysis.
Thirteen studies included ‘incident’ PD patients only (11–12, 14–15, 17–19, 24, 26–27, 29, 32, 34 and 1460 participants), with two studies stating, ‘new to PD’ (28 and 86 participants) or ‘starting CAPD’ (23 and 59 participants). Three studies specified prevalent only (16, 22, 35 and 852 participants), whereas seven studies included both incident and prevalent PD patients (13, 20–21, 25, 30–31, 33 and 1188 participants). In studies with prevalent patients, one study specified a duration of KRT of over 6 weeks as inclusion criteria (16 and 118 participants). The other studies did not specify incident/prevalent patients as an inclusion criterion (Table 2). No studies defined the start of PD, apart from two studies, where time between PD catheter insertion and usage was part of the intervention (23, 25 and 181 participants).
Table of population included and technique survival definitions.a
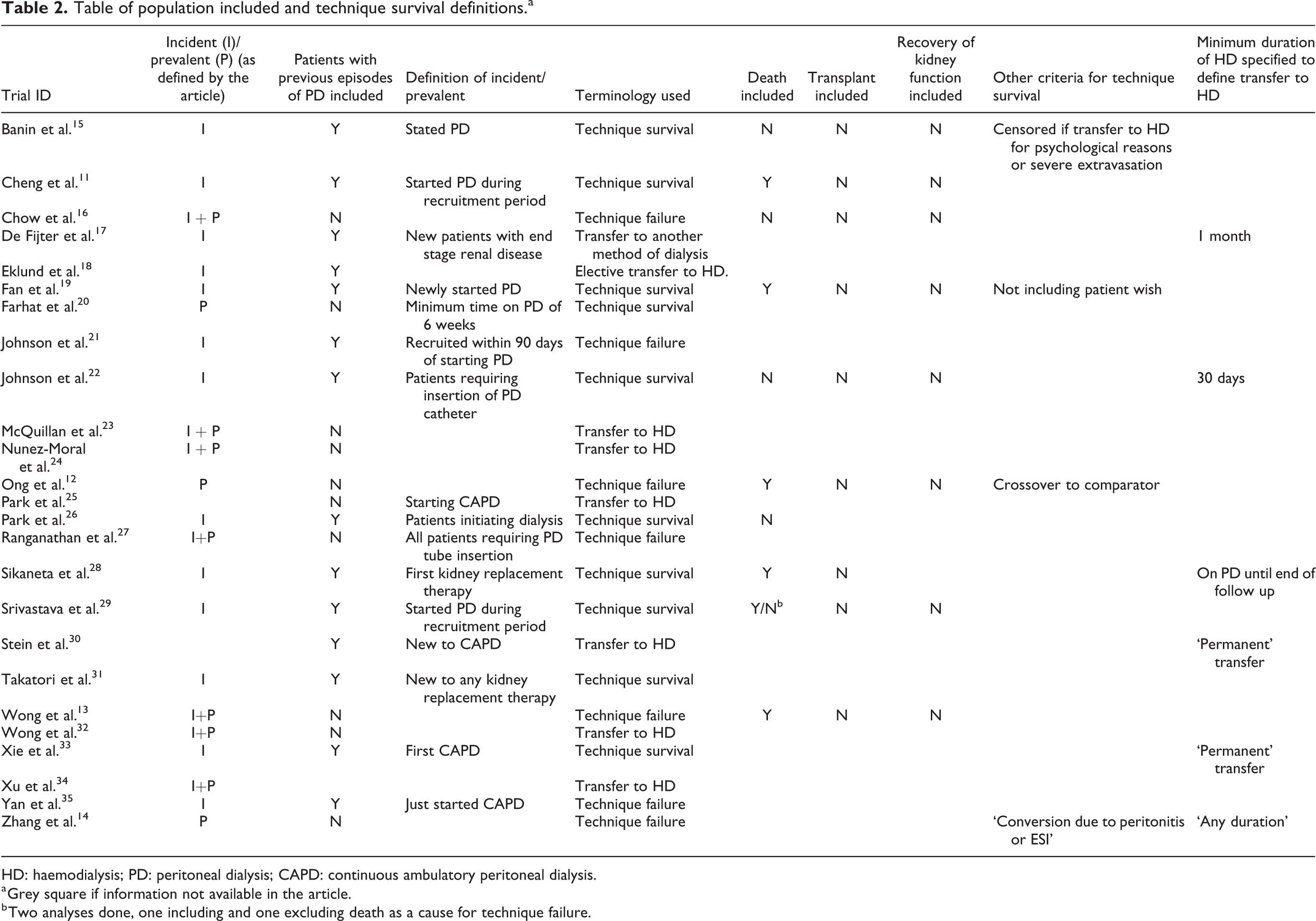
HD: haemodialysis; PD: peritoneal dialysis; CAPD: continuous ambulatory peritoneal dialysis.
a Grey square if information not available in the article.
b Two analyses done, one including and one excluding death as a cause for technique failure.
Definitions of technique survival
Three different terms were used for the outcome, with ‘technique survival’ in 10 studies (11–12, 16–17, 19, 24, 26–27, 29, 32 and 1112 participants), ‘transfer to HD’ in eight studies (14–15, 20–21, 23, 28, 31, 33 and 777 participants) and ‘technique failure’ in seven studies (13, 18, 22, 25, 30, 34, 35 and 1756 participants). These three terms had three different combinations of events comprising the outcome with 17 different definitions in total. Transfer to HD was included in the definition in all studies. When the terminology used was ‘transfer to HD’, it was assumed but not explicitly stated that death was censored in all the studies. In studies using the technique survival/failure terminology, the outcome included death as an event in five studies (12, 16, 22, 26, 30 and 950 participants), it was a censoring event in five studies (11, 13, 19, 24, 27 and 902 participants) and it was not explicit how it was treated in the remaining seven studies. Transplantation was a censoring event in nine studies (11–13, 16, 19, 22, 26–27, 30 and 1706 participants) although it was not explicit that it was censored in the remaining 16 studies (Table 2). One study included changing from the randomised treatment allocation to the comparator (change in PD disconnect system from carex to ultra) as an event in the outcome ‘technique failure’ (22 and 363 participants).
Four studies reported a minimum duration of HD to define a transfer to HD: 30 days (2 studies, 214 participants), 11,19 ‘continued HD until end of follow up’ (1 study, 101 participants), 26 ‘any duration of HD’ (1 study, 371 participants). 34 Two studies defined transfer to HD as ‘permanently transferred’ without further definition (2 studies, 166 participants). 13,28 The remaining 19 studies did not specify a minimum duration of HD. In seven studies (17, 18, 25, 29, 32, 34–35 and 1016 participants), it was unclear what criteria were used to define transfer to HD.
Reporting of technique survival
The percentage or number of events included in the definition of technique survival were reported in 22 studies (11–12, 14–24, 26, 28–35 and 2948 participants) although the follow up period varied and rates were not provided in any study. Twenty-two studies (11–22, 24–27, 29–30, 32–35 and 3354 participants) compared technique survival rates between the intervention and control arms, of which 21 used time to event analysis (11–22, 24–27, 29–30, 32, 34–35 and 3274 participants) and 1 used odds ratio (33 and 60 participants), while the remaining three studies were unclear how technique survival was evaluated (23, 28, 31 and 291 participants).
The causes of transfer to HD were reported in 16 of 25 studies (Table 3) (11, 14–15, 17–19, 23, 25–26, 28–30, 32–35 and 1933 participants). The most commonly reported cause for transferring to HD was peritonitis, which was reported in 14 of these 16 studies (11, 14–15, 17–18, 23, 26, 28–30, 32–35 and 1679 participants). Of these studies, one study specified ‘persistent elevation of effluent white cell count, fungal infection or fungal superinfection’ (33 and 80 participants), six studies specified relapsing/recurrent/refractory/prolonged peritonitis (11, 14–15, 26, 29, 34 and 472 participants), one study reported ‘PD related infection’ (35 and 371 participants), while the remaining six studies reported only ‘peritonitis’ as a cause (17, 18, 23, 28, 30, 32 and 756 participants). Additionally, three studies specified exit site infection (11, 15, 23 and 168 participants) and one study specified tunnel infection (18 and 185 participants), but it was not clear in other studies how exit site infections were classified. One study specified ‘catheter-associated infection’ (19 and 132 participants) without specifying whether this included peritonitis.
List of causes for transfer to HD.a
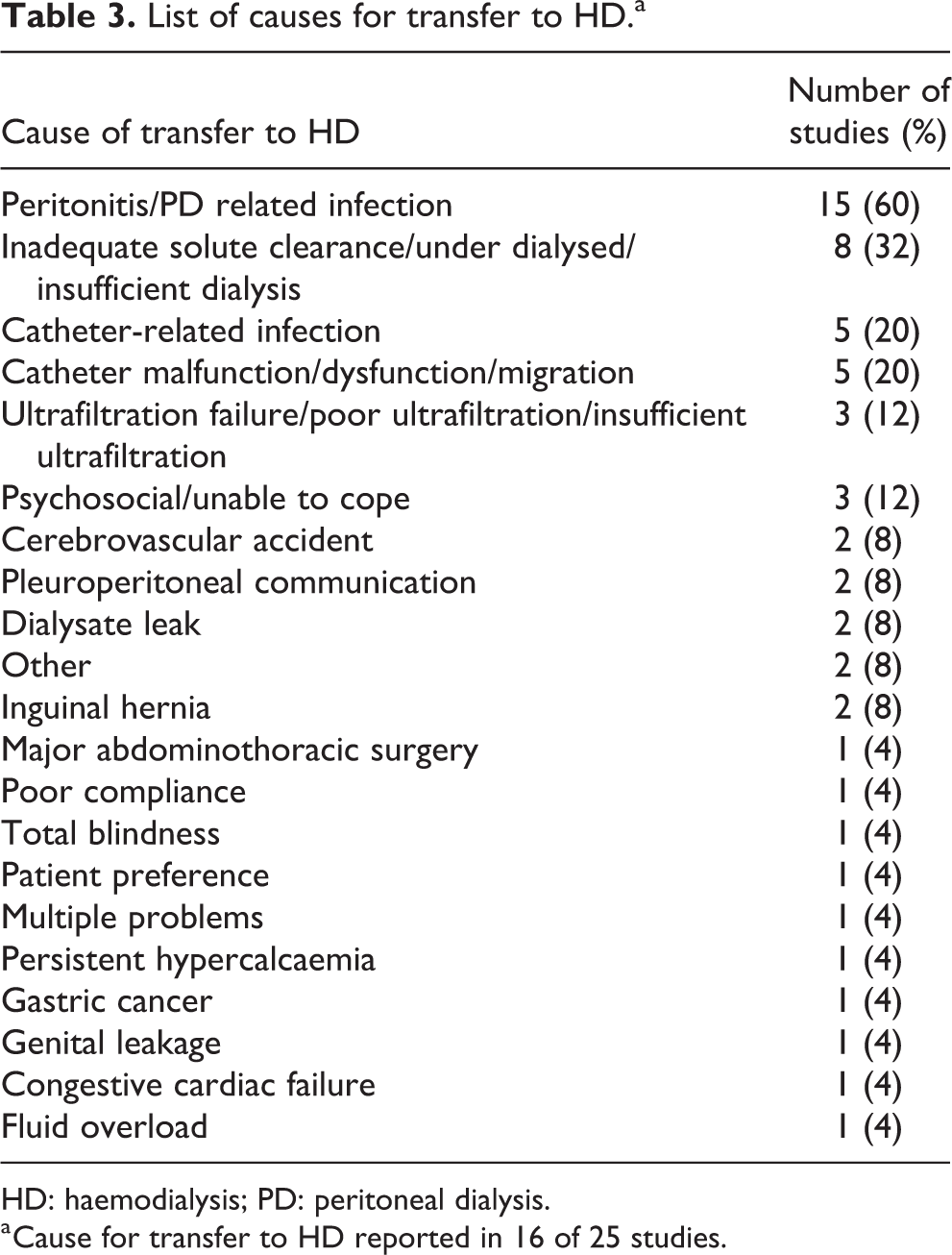
HD: haemodialysis; PD: peritoneal dialysis.
a Cause for transfer to HD reported in 16 of 25 studies.
Two studies reported only peritonitis-related transfers to HD without mentioning other causes (30, 34 and 407 participants), with the remaining 14 studies having a different list of reasons in each case (11, 14–19, 23, 25–26, 28–29, 32–33, 35 and 1644 participants). ‘Ultrafiltration failure’ or ‘poor ultrafiltration’ was reported in two studies (14, 26, 183 participants) with one study specifying ‘volume excess caused by insufficient ultrafiltration’ (29 and 41 participants), a further four studies instead reported ‘inadequate solute clearance’ (17–19, 35 and 766 participants) without further elaboration and one stated insufficient dialysis. 34 Fluid overload was reported alongside inadequate solute clearance in one study (35, 371 participants).
Discussion
Despite the critical importance of technique survival in PD, a SONG-PD core outcome and the primary outcome for the largest PD study to date (The Peritoneal Dialysis Outcomes and Practice Patterns Study P-DOPPS), 36 our study demonstrates it remains inconsistently defined and reported in RCTs of PD patients. There was substantial variability in the reported outcome, including in its definition (transfer to HD with or without death), minimum duration of HD required, the terminology used by researchers and clinicians, the population to which it is applied, the definition of PD start, reasons given for the event and the exact measures used.
A key constituent of the definition of technique survival is the duration of HD required to qualify as a transfer to HD, and an ANZDATA registry analysis of the impact of differences in this demonstrated a longer survival time with longer duration of HD used in the definition (median technique survival time of 2.0 years using 30 days compared with 2.4 years using 365 days). 7 This difference is partly due to the likelihood of returning to PD, which was much higher with the 30-day (24%) compared to the 180-day (3%) definition. 7 This demonstrates that the definition used will affect the reported results. Only six of the studies identified in this review reported how the duration of HD was used to define technique survival, using four different approaches, with some using unclear definitions or insufficient detail to allow for meaningful comparison of results between studies.
While a transfer to HD had been commonly used to define technique survival, whether mortality is included in the definition significantly impacts the rates reported. The Registre de Dialyse Peritoneale de Langue Francaise 37 reports transfers to HD and death separately, whereas the ANZDATA registry reports technique survival as a composite of transfers to HD and death, 38 in addition to ‘Death-censored technique failure’. Defining technique survival as transfer to HD with, or without death, provides different perspectives as including death will highlight the impact of co-morbidity but excluding death may highlight differences in practice patterns. Such heterogeneity in the approach to defining technique survival will likely make a large difference in reported rates. For example, in a recent UK Renal Registry analysis assessing PD patients 1 year after the commencement of therapy, 14% of PD patients had transferred to HD, 5% had died and 10% had been transplanted. 39 Given the difference in its definition between registries, the heterogeneity identified in our study about whether death contributed to the definition of technique survival was not surprising. However, in the 15 studies using the terminology of technique survival/failure, limited reporting of events contributing to the outcome leaves significant uncertainty about the exact interpretation of technique survival.
Transferring to HD is a complex event with numerous potential causes, which can co-exist, and the relative contribution of these varies with the duration of PD. 40 Furthermore, any differences in transfers to HD in RCTs are likely to be driven by large changes in one or two of the possible causes, for example, changes in peritonitis rate, rather than a smaller overall reduction in all possible causes. The overlap between the different recorded causes in these studies was unclear, such that it was not possible to compare causes for transferring between studies. Efforts should be made to standardise how the causes of transfers to HD are defined.
Technique survival has been shown to vary with the duration of PD, with a higher event rate earlier in the treatment course. 37,39,40 The population included, whether incident or prevalent, will therefore potentially affect the reported rate of technique survival, so reasonable comparisons of technique survival rates require accurate reporting of the study population. To achieve this would require both a comparable definition for start date (e.g. catheter insertion date, commencement of training or exchanges to improve solute clearance) and clear definitions of incident/prevalent status using minimum/maximum time on PD, which was only mentioned in three studies. This again highlights the complexity in trying to compare different studies with limited information on study methodology.
Limitations of this study included the possibility of publication bias, although it is unlikely that this would directly affect the definitions of technique survival used. Observational studies and registry reports were not included, as this was likely to lead to an unmanageable increase in the number of studies included, while RCTs not reported in English were also excluded, although this made no difference to the results. Children were not included in this review, but this was to avoid duplication in the literature. A previous review did not find technique survival as a reported outcome in studies of this population. 41
Technique survival is an important outcome from the point of view of both health economic and patient outcomes, emphasising the need to identify and understand interventions that can improve this outcome. These results demonstrate the difficulties in understanding and comparing the impact of interventions on technique survival when standardised reporting and outcomes are not used. This work represents an important first step in the SONG-PD technique survival work stream, helping to develop standardised definition and reporting of technique survival in all PD studies, and highlights the need to consider issues such as the need for a standardised time on HD to be accepted as an event, and whether a range of outcomes may be necessary for different studies, while ensuring the results are accessible to patients. Furthermore, if consistent reporting of technique survival can be applied across both studies and registries, this will facilitate quality improvement attempts to address the marked variability found between and within countries.
Supplemental material
Supplemental Material, sj-docx-1-ptd-10.1177_0896860821989874 - Outcome measures for technique survival reported in peritoneal dialysis: A systematic review
Supplemental Material, sj-docx-1-ptd-10.1177_0896860821989874 for Outcome measures for technique survival reported in peritoneal dialysis: A systematic review by Emma Elphick, Matthew Holmes, Matthew Tabinor, Yeoungjee Cho, Thu Nguyen, Tess Harris, Angela Yee Moon Wang, Arsh K Jain, Daniela Ponce, Josephine SF Chow, Annie-Claire Nadeau-Fredette, Adrian Liew, Neil Boudville, Allison Tong, David W Johnson, Simon J Davies, Jeffrey Perl, Karine E Manera and Mark Lambie in Peritoneal Dialysis International
Footnotes
Acknowledgement
The authors would like to acknowledge the contribution to the discussion by Dr Robert R Quinn.
Author contributions
ML, DWJ, SJD, KEM, AT and NB conceived and designed the study. EE, MH and MT performed the search, screening and data extraction. EE wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: ML has received honoraria from Fresenius Medical Care, Baxter Healthcare and NxStage and a research grant from Baxter Healthcare. DJ has received consultancy fees, research grants, speaker’s honoraria and travel sponsorships from Baxter Healthcare and Fresenius Medical Care, as well as consultancy fees from AWAK and Astra Zeneca, speaker’s honoraria from Ono and travel sponsorships from Amgen. He is a current recipient of an Australian National Health and Medical Research Council (NHMRC) Practitioner Fellowship. JP has received speaking honoraria from Astra Zeneca, Baxter Healthcare, DaVita Healthcare Partners, Fresenius Medical Care, Dialysis Clinics Incorporated, Satellite Healthcare, and has served as a consultant for Baxter Healthcare, DaVita Healthcare Partners, Fresenius Medical Care, and LiberDi. NB has received unrestricted educational grants, travel grants or honoraria from Baxter Healthcare, Amgen, Astra Zeneca, Roche Pharmaceuticals and FMC. YC has received research grants and speaker’s honoraria from Baxter Healthcare and research grants from Fresenius Medical Care and Amgen. She is a current recipient of an Australian NHMRC Early Career Fellowship. AYW has received grants from Baxter Corporation and Sanofi Renal and received speaker honorarium from Fresenius Kabi and Sanofi Renal. AL has received speaker’s honoraria from Baxter Healthcare. JC has previously received speaker’s honoraria and research funds from Baxter Healthcare, Fresenius Medical Care, Roche Pharmaceuticals and Amgen. AKJ has received consultancy fees, research grants, speaker’s honoraria from Baxter Healthcare and AWAK Technologies. ACNF has received research grants from Baxter Healthcare and scholarship from Fonds de Recherche du Québec – Santé.
Ethical approval
Not applicable.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.