
Abstract
Background:
Previous evidence suggests home-based dialysis to be more cost-effective than unit-based or hospital-based dialysis. However, previous analyses to quantify the costs of different dialysis modalities have used varied perspectives, different methods, and required assumptions due to lack of available data. The National Institute for Health and Care Excellence reports uncertainty about the differences in costs between home-based and unit-based dialysis. This uncertainty limits the ability of policy makers to make recommendations based on cost effectiveness, which also impacts on the ability of budget holders to model the impact of any service redesign and to understand which therapies deliver better value. The aim of our study was to use a combination of top-down and bottom-up costing methods to determine the direct medical costs of different dialysis modalities in one UK nation (Wales) from the perspective of the National Health Service (NHS).
Methods:
Detailed hybrid top-down and bottom-up micro-costing methods were applied to estimate the direct medical costs of dialysis modalities across Wales. Micro-costing data was obtained from commissioners of the service and from interviews with renal consultants, nurses, accountants, managers and allied health professionals. Top-down costing information was obtained from the Welsh Renal Clinical Network (who commission renal services across Wales) and the Welsh Ambulance Service Trust.
Results:
The annual direct cost per patient for home-based modalities was £16,395 for continuous ambulatory peritoneal dialysis (CAPD), £20,295 for automated peritoneal dialysis (APD) and £23,403 for home-based haemodialysis (HHD). The annual cost per patient for unit-based modalities depended on whether or not patients required ambulance transport. Excluding transport, the cost of dialysis was £19,990 for satellite units run in partnership with independent sector providers and £23,737 for hospital units managed and staffed by the NHS. When ambulance transport was included, the respective costs were £28,931 and £32,678, respectively.
Conclusion:
Our study is the most comprehensive analysis of the costs of dialysis undertaken thus far in the United Kingdom and clearly demonstrate that CAPD is less costly than other dialysis modalities. When ambulance transport costs are included, other home therapies (APD and HHD) are also less costly than unit-based dialysis. This detailed analysis of the components that contribute to dialysis costs will help inform future cost-effectiveness studies, inform healthcare policy and drive service redesign.
(1) What is already known about this subject:
Though numerous studies have costed aspects of dialysis care, none have provided comprehensive costs and the most recent UK guidelines on dialysis modalities reports uncertainty about the differences in costs between home-based and unit-based (hospital or satellite unit) dialysis.
(2) What this study adds:
This detailed analysis combines micro-costing, local and regional costing data (including both NHS and independent sector costing and transport costs), and as such is the most comprehensive costing study of dialysis modalities undertaken to date in a publically funded healthcare system. The results showed that nearly two dialysis patients could be treated at home via CAPD for approximately the same cost as one patient requiring transport and treated in an NHS hospital dialysis unit.
(3) What impact this may have on practice or policy:
As our study provides new and comprehensive data on the costs of each of the different components that contribute to the overall costs of dialysis, it will better enable healthcare systems, and in particular commissioners to model the costs of service redesign as well as inform future cost-effectiveness studies and clinical guidelines.
Background
Chronic kidney disease (CKD) is increasingly common due to a growing number of people with chronic health conditions such as diabetes and hypertension. 1 Globally, CKD affects approximately 11–13% of adults with the numbers expected to rise over the next decade. 2 When patients with more advanced CKD reach the stage of established renal failure (ERF), they usually require treatment in the form of renal replacement therapy (dialysis or transplant). 3
For many patients, transplantation is not possible due to patient comorbidities such as cancer or severe cardiac disease. Even when transplantation is possible, the average waiting time for a kidney transplant in the United Kingdom is 2.5–3 years. 4 As a result, most patients approaching ERF must choose a dialysis modality. There are four main dialysis modalities: home-based haemodialysis (HHD), continuous ambulatory peritoneal dialysis (CAPD), automated peritoneal dialysis (APD) and unit-based haemodialysis (UHD). Within the United Kingdom, UHD can be delivered in either a fully managed National Health Service (NHS) unit (usually on a hospital site) or within a unit run in partnership between the NHS and an independent sector provider (ISP), which can be either on or off a main NHS site.
Dialysis is a relatively high-cost treatment, with previous commentators estimating that the UK NHS spends over £500 million per year on dialysis. With the growth in CKD and dialysis demand, this figure is likely to have risen significantly over the past decade. 5,6 A rapid review of previous economic evaluations of dialysis modalities conducted as part of this study found numerous studies that attempted to quantify the costs of dialysis. 7– 10,11,12,13,14,15,16,9 In general, the authors of these studies concluded that peritoneal and home dialysis modalities were likely the most cost-effective. However, there were limitations to these studies, including varying perspectives of the analysis; use of assumptions in the costings due to lack of data (e.g. applying the same overhead cost and equipment costs to multiple modalities); use of interviews to gather data, which may have introduced bias, difficulty in establishing overhead costs and omission of particular costs (e.g. transport costs). Consequently, existing studies were not considered robust or comprehensive enough for the most recent National Institute for Health and Care Excellence (NICE) report. 17 Within this report, NICE state that there is uncertainty about the differences in costs between PD and HD due to uncertainty around current UK dialysis costs as well as uncertainty around transport costs. Additionally, when comparing UHD and HHD, NICE conclude that there is uncertainty around cost. 17
Given the lack of robust and complete contemporary costing data, we decided to undertake a study to understand the cost of dialysis modalities in Wales, a country within the United Kingdom with a population of 3.1 million. Healthcare in Wales is provided by the publicly funded NHS and delivered via seven regional health boards. Specialist renal services such as dialysis and transplantation are commissioned on behalf of the seven health boards by the Welsh Renal Clinical Network (WRCN). In 2019, there were 17 UHD centres across Wales; 6 (35%) were hospital-based units managed by the NHS and 11 (65%) were satellite units run by various ISPs in partnership with the NHS. The ISP units provide equipment, consumables and (if required) buildings and nursing staff.
Healthcare services in Wales (including nephrology) have been challenged to adopt a value-based healthcare (VBHC) approach, with a need to develop robust costing models that enable measurement of value. 18 Our aim in the current study was to undertake a top-down and bottom-up methods costing study, working with the WRCN and managers /clinicians from each of the individual renal units in Wales so that we could compare directly the costs of home and unit-based dialysis to provide a comprehensive and costed model of different options to inform decision-making in the United Kingdom.
Methods
Costing methodology
Our costings were sought from one UK nation (Wales), which has a health board-based system of NHS commissioning rather than a competitive internal market system as in England. However, Wales has both urban and rural demands on healthcare delivery and some of the most socioeconomically deprived areas of the United Kingdom.
To generate a balanced estimate of costs, a hybrid approach of top-down and bottom-up micro-costing was used. Micro-costing enables the precise cost assessment of health interventions and requires three basic steps: deciding the costing perspective (i.e. healthcare provider or societal), identifying resources used to deliver care and grouping cost categories for valuation. 19– 21 For the bottom-up micro-costing approach, information was obtained directly from medical and administrative staff within the WRCN and from senior managers, consultants, nurses and allied health professionals in kidney units across Wales. For some cost categories, top-down costing was applied using values obtained from national sources such as the Patient Level Information and Costing System (PLICS), the WRCN and the Welsh Ambulance Services NHS Trust (WAST). 22,23
All costs were estimated from the NHS perspective and expressed in 2018–2019 prices. Only direct medical costs for each dialysis modality were included. We did not include indirect costs such as productivity losses, medications (other than drugs required to directly enable the dialysis process), nor the additional social care support that may be needed for home dialysis patients. To simplify comparisons for UHD, data are presented on either fully managed NHS units or for those off-site units where ISPs provide nursing staff, consumables, buildings and overheads.
Staff costs
The quantity and pay grade of staffing required to deliver each dialysis modality was obtained from bottom-up micro-costing using data supplied by multidisciplinary teams across Wales and published in the WRCN Workforce Establishments audit. 24 Staff costs were based on NHS Employers pay scales and included on-costs. 25,26 For ISP dialysis units (where the ISP contract included nursing staff), staff costs were included in the overall cost of ISP UHD and (for reasons of commercial sensitivity) were not displayed separately. The nationally recommended nurse: patient ratio (per dialysis shift) in Wales for both NHS and ISP units is 1:3 (as per WRCN service specification) with a 70:30 qualified: non-qualified split. At present, there are no UK wide workforce recommendations for home therapy staff to patient ratios. From correspondence with colleagues across the United Kingdom, it is apparent that there are significant differences in ratios between units (which may reflect different roles/delivery of training vs. caring for prevalent patients). According to feedback from multiple UK units, the median home therapy staffing was 1:17 for PD and 1:12 for HHD. Since our staffing numbers in Wales are higher than this, we have included costing for both the Wales workforce and the presumed average UK workforce within our results section.
Consumables and equipment
For UHD in NHS units, a bottom-up micro-costing approach was used, with a cost applied to each item required to enable a patient to have a session of UHD. For ISP UHD, the cost of equipment and consumables is included in the overall UHD cost. For ISP UHD, the costs described reflect the average cost of services provided by different ISPs operating across Wales (for reasons of commercial sensitivity further distribution data is not shown).
For home therapies, cost data for equipment and consumables was obtained from the WRCN all-Wales home therapies purchasing framework. The framework includes multiple ISPs and was established so that purchasers in the public sector may obtain value for money in their purchasing while being assured that their procurement is compliant with UK and EU legislation. 27,28
For some aspects of home therapy, renal units had to purchase items that were not included on the home therapies framework. These costs were obtained directly from each unit.
Given that there are different costs attached to different PD fluid prescription, data was obtained from local renal units to understand the proportion of patients on each type of PD fluid so that a weighted average cost of fluid could be applied. For costing of HHD, it was assumed that each patient was undertaking ×5/week dialysis (the most common HHD prescription in Wales).
Additional costs for home dialysis
For home dialysis patients, additional costs were also required for reimbursing patients for utilities, installing dialysis equipment and for regular outpatient dialysis review clinics. These costs were obtained from the WRCN (installation, utilities) and from PLICs (clinics). One-off expenses such as home installation were converted into equivalent annual costs (based on length of time on HHD).
Dialysis access procedure and intervention costs
All dialysis patients require an access procedure, either an arteriovenous fistula (AVF) or tunnelled dialysis lines for HD or a PD Tenckhoff catheter for PD. For most patients, PLICS data was used to obtain the cost of access procedures, and the costs shown include the cost of the procedure, inpatient stay and follow-up clinics. Cost data was adjusted to account for the fact that 20% of HD patients required the AVF procedure twice and 10% of PD patients require the procedure twice. The weighted annual costs were calculated from WRCN data on the average duration of UHD/HHD and PD within Wales (38, 19 and 21 months, respectively).
Vascular access intervention costs were based on our all-Wales data showing that for prevalent patients 70% have access via AVF and 30% have access via central venous catheters. Of the patients with an AVF, 15 in every 100 patients require an AVF intervention each year – which has been costed into the annual cost. For patients with access via central venous catheters, the commonest and costliest intervention was fibrinolytic infusion, which has also been included in the annual cost.
Transport costs for unit dialysis
Within Wales, 60% of patients rely on NHS provided transport. The costs of transporting patients to and from UHD were obtained using a top-down costing approach with data supplied by the Welsh Ambulance Service Trust. The centralised running costs related to the renal transport hub and the planning and control centre were divided equally among all patients utilising NHS transport services. Annual cost per patient of ambulance transport involved calculating a weighted cost per average ambulance mile per patient. To take into account that different categories of ambulance carry different costs, the cost was weighted in relation to category of ambulance, that is, the proportion of patients requiring a two-man and one-man crew ambulance. To take into account that not all journeys involve the transport of the same number of patients, the cost was also weighted in relation to vehicle utilisation, that is, the average proportion of journeys involving the transfer of one, two, three and four patients. The calculated weightings were used to calculate a representative cost per average ambulance mile per patient. The average distance between a patient’s home and their unit is 6 miles, and this figure was used to calculate the average cost of ambulance transport per patient per year.
Monitoring costs
All patients received routine tests (bloods and microbiology tests) directly related to provision of dialysis care. Cost data was adjusted for the fact that in some ISP units, blood tests were included in the UHD cost as part of the contract.
Overheads
For NHS UHD, the overhead categories included in the costing are shown below (Table 1).
NHS UHD overheads.a
NHS: National Health Service; ISP: independent sector provider; UHD: unit-based haemodialysis.
a For ISP dialysis in off-site, non-NHS units, capital and overheads were included in the overall UHD cost.
Ethics approval
The study has full approval from Health and Care Research Wales Research Ethics Committee.
Results
The annual costs of different dialysis modalities in Wales are summarised below (Table 2). All costs are shown as cost per patient per year.
Cost per patient per year of therapy for each dialysis modality.
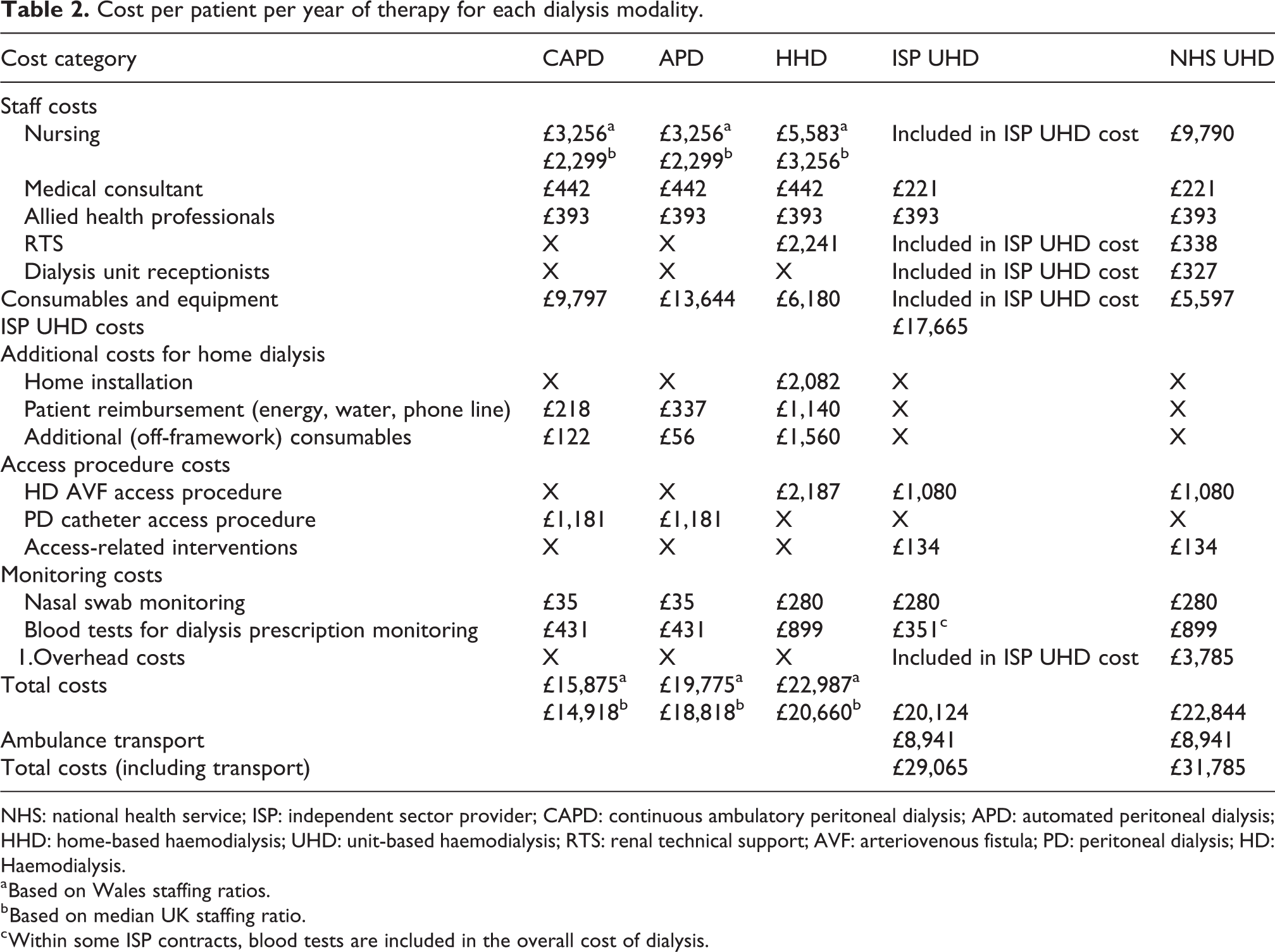
NHS: national health service; ISP: independent sector provider; CAPD: continuous ambulatory peritoneal dialysis; APD: automated peritoneal dialysis; HHD: home-based haemodialysis; UHD: unit-based haemodialysis; RTS: renal technical support; AVF: arteriovenous fistula; PD: peritoneal dialysis; HD: Haemodialysis.
a Based on Wales staffing ratios.
b Based on median UK staffing ratio.
c Within some ISP contracts, blood tests are included in the overall cost of dialysis.
Discussion
The results of our study indicate that from an NHS perspective, CAPD was less costly per patient than any other dialysis modality. Our findings support previous studies who also found PD to be the least costly of dialysis options assessed. 8 , 9,11 With regard to other home therapy modalities (APD, HHD), the costs of therapy were broadly similar to the cost of UHD; however, when transport costs were included (60% of UHD patients in Wales require transport), UHD was significantly more costly. Additionally, it should be noted the treatment cost of HHD includes ×5 per week treatment as compared to ×3 per week treatment in UHD. We have shown that in spite of similar staffing ratios, ISP UHD costs seem slightly lower than NHS UHD costs. For reasons of commercial sensitivity, we are unable to clarify whether this relates to consumable costs, staff costs, overhead costs or a combination of all three. Given the potential clinical and quality of life benefits of HHD, our study confirms that if we define value as outcome per unit cost, this therapy is high value as compared to UHD.
Our study is the most detailed costing analysis undertaken in this field in the United Kingdom and our micro-costing approach provides a detailed breakdown of how different cost categories (including transport) influence the overall treatment cost. Our costings were sought from one UK nation (Wales), which has a health board–based system of NHS commissioning rather than a competitive internal market, which is found in England. Wales has both urban and rural demands on healthcare delivery. The findings of our study are directly applicable to other NHS units across the United Kingdom and could also act as a useful framework for units outside the United Kingdom who wish to better understand their dialysis costs. Unlike many of the previous studies, we have kept assumptions to the minimum. We believe that our study adds to the current knowledge base and can help model the cost of service redesign, inform future policy guidelines as well as providing data for future cost-effectiveness studies.
Although our study was underpinned by detailed costing information, there were limitations. Firstly, the study was undertaken on data obtained only from Wales and many factors such as staffing ratios, reimbursement policies and dialysis vintage may vary in other regions. It has become clear from benchmarking work that the home therapy nursing ratios in Wales are higher than in some parts of the United Kingdom – which may reflect the fact that many units in Wales are relatively small (and thus unable to realise economies of scale) and also some units cover large geographical areas so that staff may spend a lot of time travelling between patients which reduces the staffing efficiency and requires higher numbers of staff members within the team. In terms of dialysis vintage, we have observed many patients are called for transplant soon after starting home dialysis which is common reason for stopping dialysis and likely explains the relatively short median duration of therapy. Clearly on an individual patient basis, cost of therapy will vary with dialysis vintage, for example, if a patient remains on home therapies for 5 years, the annual costs fall to £15,078 and £20,067 for PD and HHD, respectively. A further limitation of our study is that we did not include the cost of assisted PD. In Wales, there is only a single provider of assisted PD and thus (because of commercial sensitivity) we were unable to include the cost within the current manuscript. Though very few patients in Wales are currently using assisted PD, we are aware that in other regions a significant proportion of patients are using some form of assisted PD.
Another drawback of our study is that we measured only direct medical costs to the NHS. Future studies could take a societal perspective by comparing differences in productivity loss costs between modalities for patients and carers whose paid employment might be reduced due to dialysis. Previous studies have justified their decision to not include productivity losses as they reasoned this would not be appropriate given the majority of dialysis patients are of retirement age. 7,14 However, this is not true of all dialysis patients, and in particular, many home dialysis patients are younger and of working age, with HHD patients having a median age of 55. 29 The omission of loss of productivity costs is an important issue to raise, and future economic evaluations should capture these losses, as different modalities are likely to have differing impacts on productivity losses, which could have a bearing on cost-effectiveness. This micro-costing was part of a larger qualitative study with patients and carers to better understand their motivations and experiences of choosing a treatment option, which could provide valuable information about how choice of dialysis modality can effect employment and assist in quantifying productivity losses. 30
Another important question for future research is whether increased use of home dialysis requires extra costs associated with an integrated health and social care infrastructure to support patients and carers at home. Finally, as this study was primarily focussed on the cost of providing dialysis (rather than managing the complications of CKD stage 5), we did not assess medication use. Research indicates that this may be of relevance to the wider costs since HHD patients may require less hypertensive medication or less phosphate binders due to the frequency of dialysis. Clearly this may further improve the cost-effectiveness profile of HHD. 31
Conclusion
This micro-costing offers a comprehensive, transparent costing of different dialysis modalities. From an NHS perspective, home dialysis (in particular CAPD) confer significant less cost than unit-based therapies and a drive to increasing home therapies aligns with a VBHC approach. The lack of robust evidence in this field has been highlighted and this micro-costing and its methods will help inform future cost-effectiveness studies, healthcare policy and drive service redesign.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was granted by the Wales Research Ethics Committee (ref. 19/WA/0020).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by Health and Care Research Wales (Research for Patient and Public Benefit grant 2018).