
Abstract
This study investigated changes in nurses’ sense of calling during the COVID-19 pandemic, as well as possible reasons for these changes. A total of 440 nurses in Turkey responded to a single open-ended question about their work attitudes and experiences. Emergent Qualitative Document Analysis (QDA) was used to analyze the responses. Results demonstrated that nurses experienced both positive and negative changes to their sense of calling, sometimes simultaneously. The most frequently cited reasons for positive changes were nurses’ perceived job significance, their desire to serve humanity, and a sense of meaningful work. In contrast, terms describing their reasons for experiencing negative changes include exhaustion, underpaid, unappreciated, overwork, disengagement, risky, stress, and anxiety. This study provides the first evidence on how a sense of calling experienced by Turkish nurses has been affected by the COVID-19 pandemic. Implications for theory, research, and practice are explored.
The global COVID-19 pandemic has strained many social systems and institutions since its onset in early 2020, perhaps none more so than healthcare. As COVID-19 cases have mounted, health systems have encountered serious challenges in staffing and in delivering the care needed, and healthcare employees have shouldered a disproportionate share of the burden. Among all frontline workers, those in healthcare are at perhaps greatest infection risk given their constant exposure to positive cases. A recent report published by the WHO estimated that 14% of healthcare employees worldwide contracted COVID-19 within the first several months of the pandemic. It is estimated that this ratio probably varies between 3.8% and 19% (Harrison, 2022) and may have reached as high as 35% in low- and middle-income countries (World Health Organization, 2020a). In Turkey, one of the top 10 most impacted nations in the world in terms of number of COVID-19 cases, approximately 120,000 healthcare workers had contracted COVID-19 one year into the pandemic, which corresponds to 1/10 of the total healthcare employees in the country. The number of healthcare workers who died increased accordingly as well (Turkish Thoracic Society, 2021). In some ways, these grim realities are nothing new; in extraordinary times such as during natural disasters and pandemics, healthcare employees are always among the most dramatically impacted by health risks and increased workload demands. Despite the resulting physical and psychological health problems that accompany intense stress, healthcare workers have repeatedly demonstrated a willingness to set aside their personal needs and carry out self-sacrificing work in accordance with their professional ethics and responsibilities (Aliakbari et al., 2015).
Nurses, in particular, work very closely with patients and must cope with a high degree of exposure to illness. As a group, nurses frequently experience negative emotions such as fear, anxiety, eating and sleep disorders (Sun et al., 2020), yet are required to maintain high levels of performance regarding patient treatment and care (Zhou et al., 2021). The notion that work can be experienced as a calling has been described as relevant for people with a wide array of worldview commitments (e.g., both sacred and secular; Steger et al., 2010). A consensus definition of the construct remains elusive, but most scholars describe a calling as an internally or externally sourced sense of purposeful work carried out for the greater good (Dik & Duffy, 2009; Thompson & Bunderson, 2019). Such a view of work can function as an asset to nurses. Indeed, nurses with a calling empathize more effectively with patients and perform their services selflessly with a high level of motivation (Raatikainen, 1997). Research also demonstrates that nurses who view their work as a calling perform at a high level during extraordinary times such as the COVID-19 pandemic (Zhou et al., 2021).
Research is emerging that targets the role and function of a sense of calling during the pandemic (e.g., Zhou et al., 2021), but more is needed to investigate core questions such as how a sense of calling may have changed among employees during this period. Such research, including the present study, aims to shed light on the impact that “critical events” play as healthcare employees in particular navigate a very challenging emotional terrain (Restubog et al., 2020). Scholars have expressed that the macro and micro changes experienced in this period may cause both positive and negative shifts in workers’ perceptions towards some jobs. Accordingly, the attractiveness of some jobs may increase or decrease in parallel with changes in workers’ perceptions of meaningful of work (Steger et al., 2012).
The current study contributes to calling theory by exploring changes in one’s sense of calling and the sources of these changes among employees who face work-related Covid-19 exposure risk during this extraordinary crisis period. Work as a Calling Theory (WCT; Duffy et al., 2018), for example, proposes that perceiving a calling is linked to both positive and negative outcomes among workers who express that they are currently living out their callings. However, the specific mechanisms that influence the stability of one’s sense of calling, or whether living a calling promotes positive or negative outcomes (or both), remain poorly understood (Duffy et al., 2018). The purpose of this study is to shed new light on these possible mechanisms by qualitatively investigating changes in nurses’ sense of calling during the pandemic, as well as factors that may account for observed changes.
Calling in Turkish Culture
Research reveals that a sense of calling is consistently positively correlated with both work-related and general well-being, functioning both as predictor and outcome (see Duffy et al., 2018, and Thompson & Bunderson, 2019, for reviews). Much of the early research on calling emerged within highly individualistic Western cultures, such as the United States and Western Europe. However, the construct has been described as cross-culturally robust (e.g., Dik & Duffy, 2009), and research on calling has become a global phenomenon, with studies from six continents now available in the literature (Lysova et al., 2019). To date, the broad cross-cultural similarities (e.g., in how calling is conceptualized, and in its pattern of relations with criterion variables) are arguably more striking than the differences, yet some meaningful differences in emphasis pertaining to particular aspects of the construct are likely given the differences in cultural values across nations (Dik et al., 2019).
In Turkey, two cultural distinctives may influence the way workers engage their work as a calling. The first, a foundational philosophy of the Republic of Turkey, is an emphasis on cultural progress. This emphasis emerged after the Republic of Turkey was established in 1923 and has influenced social and radical reforms such as the adoption of the Latin alphabet, secularism, and the adoption of Western-based laws (Berkes, 1959). With the adaptation of these reforms, Turkey’s social and cultural integration with the Western world advanced rapidly, and cultural change in the direction of western civilization continues. The second is the influence of the Islamic faith. In Turkey, belief systems adopted during the post-Islamic period are in many ways similar to those that defined the pre-Islamic period (Kayacan, 2018), yet collectivist virtues and values have become more dominant in Turkish culture with the acceptance of Islam.
As a collectivist culture, Turkish society socializes people to exhibit prosocial behaviors (Kumru et al., 2012)—and such behaviors have indeed been found to occur more readily among people raised in collectivist as opposed to individualistic cultures (Steelman, 1995). Turkish values related to work also include a view of work as a means of fulfilling God’s commands (Arslan, 2009), a way of establishing a social solidarity (Aldemir et al., 2003), and a role that should be carried out voluntarily and respected (Aygün et al., 2008). Work also is viewed as a means of making children proud of their families, and a sign of self-sacrifice for parents (Phalet & Claeys, 1993).
There is no term for ‘calling’ in Turkish language, but as Hermansen (2004) noted, peoples’ work-related efforts are linked with a broader sense the purpose of life within Islam. According to Islamic teaching, an inner motivator lies behind the behavior of humans—that of striving to gain God’s will, to serve humanity, and to live a moral life. When people are aware of their abilities and view them as God-given blessings, work can function as a source of life that provides meaning, motivating, and encouraging them to do good, and strengthening their connections with themselves and God (Millis, 2016). For these reasons, a Turkish adaptation (Uzunbacak et al., 2019) of the Brief Calling Scale (BCS; Dik et al., 2012) translated the term ‘calling’ as ‘love’ one experiences toward one’s job. Research evidence with a Turkish sample reveals that the important qualifications expected from a job are its compatibility with the values of the individual and its potential for providing a sense of achievement, being a beneficial to society, and being respected by society (Sunar, 2019). These values clearly align with how calling is conceptualized within the research literature.
Covid-19 and Nurses’ Sense of Calling
Many nurses enter the profession driven by a sense of calling (Emerson, 2017), which has been described as a highly valued professional attitude (Fowler & Tschudin, 2006). Emerson (2017) stated that for nurses, approaching the job as a calling means caring for those in need of care, making sacrifices, working with high motivation, believing in destiny, and working with purpose and passion. Nursing from this perspective contains a transcendent purpose and meaning (Afsar et al., 2018). Initial evidence suggests that nurses who are living a calling tend to perform at a high level and cope relatively effectively with pandemic-related challenges (Zhou et al., 2021). A recent qualitative study with nurses caring for COVID-19 patients revealed that while performing their duties, nurses can simultaneously experience positive emotions such as confidence, calmness, relaxation, and happiness, and negative emotions such as fatigue, anxiety, fear, and helplessness. Furthermore, among nurses, displaying high levels of effort and carrying out job responsibilities with gratitude has been linked to altruism (Sun et al., 2020). Indeed, evidence suggests that among doctors and nurses, making sacrifices for the public good, devoting oneself to helping others, and maintaining high motivation and a sense of meaning (Liu et al., 2021) all increase the likelihood of having a calling (Kim & Kang, 2020). These same behaviors are essential for approaching work as a calling during the COVID-19 pandemic (Kang & Shin, 2020; Kim & Han, 2021).
The effects of nurses’ calling on their attitudes, behaviors, and psychological experiences are among the unanswered questions in the calling literature (Afsar et al., 2018). Zhou et al. (2021) suggested that the effects of the COVID-19 pandemic on nurses should be examined in detail. In response, the aim of the current study is to investigate (using Emergent Qualitative Document Analysis) the extent to which perceptions of calling have changed for nurses in Turkey during the COVID-19 pandemic, along with factors that may have influenced potential changes. This population offers unique insight into the question of how challenging circumstances may foster both positive and negative changes in one’s sense of calling, and in the outcomes that workers experience as a result.
Method
Participants and Procedure
A purposive sampling strategy, that is, a non-random sampling method designed to help researchers identify a sample displaying characteristics of particular interest to the research question (Christensen et al., 2011), was used to recruit full-time nurses employed at the Isparta City Hospital and Süleyman Demirel University Research Hospital, both of which are assigned by the Ministry of Health as COVID-19 diagnosis and treatment hospitals in the Turkish province of Isparta. Before consenting to participate, participants were informed of the study’s purpose, what participation would entail, and the fact that they could cease participation at any time and for any reason. They were also informed that their participation would be confidential and their data would be anonymized. Recruitment materials were disseminated to potential participants by hospital administrators, who also were informed about the research and its purpose before agreeing to assist. All participants agreed to respond to the survey on a volunteer basis, with no extrinsic incentive provided.
Due to the COVID-19 global pandemic, data were collected via an online survey shared with nurses via WhatsApp by hospital managers. A total of 1146 nurses work full time in both hospitals, and 440 online questionnaires were completed, a response rate of 38.39%.
Of the 440 nurses in the sample, 91.8% were women and 8.2% were men. Approximately one-quarter of the sample (24.8%) were in the 18–29 age range; 27.9% were 30–39, 44.6% were 40–49, and 2.7% were in the 50–60 age range. Two-thirds (66.4%) self-identified as married and 33.6% as single. Reflecting their professional status, the sample was highly educated; 65.2% reported having a bachelor’s degree and 14.1% reported having a graduate degree (master’s and PhD); the remaining participants reported that their highest degrees were from vocational school (13.9%) or high school (6.8%). Slightly more than one-third (36.6%) of participants identified as a clinical nurse and 28.9% as an intensive care nurse; of those that remained, 15% worked in the surgery room, 9.3% in emergency, 7% in hemodialysis, and 3.2% in the other departments. In addition, 33.2% of the nurses report having 10 or fewer years of experience, 34.3% reported 11–20 years of experience, and 32.5% reported having more than 20 years of experience.
After providing their informed consent, participants were asked to respond (with no word limit) to the following question (in Turkish, translated here to English): “When you compare before the Covid-19 pandemic to now, has there been a change in your sense of calling, considering your passion, love, and the meaning that you attribute to your work? If there has been a change in your calling, please briefly explain the ways it has changed.” (A series of quantitative items, not included within the focus of this study, also were administered as part of the survey.)
Coding and Analyses
In this study, written responses to the open-ended question were coded using Emergent Qualitative Document Analysis (QDA), an inductive method (Altheide et al., 2008). The QDA method was preferred because of its exploratory nature, in contrast to the hypotheses-driven classical content analysis (Krippendorff, 2004). Although collecting data face-to-face with interviewees can increase the depth of the data they provide, a key advantage of QDA is its ability to collect responses efficiently from a large sample (Altheide et al., 2008). To carry out the analysis, four members of the research team independently used open coding to label each participant’s response in a concise but descriptive manner (Strauss & Corbin, 1998). During the coding process, participants’ statements were classified, categorized, and named according to their similarities and differences. In an iterative process, new statements that were similar to earlier statements were collected under the same codes, while unique statements formed the basis of new codes, until a total of 43 codes had emerged. These units (labels) were then grouped into more detailed sub-themes. For example, the labels “exhaustion,” and “disengagement” were sorted under the “Individual Reason” category (sub-theme). Subsequently, the categories were reclassified to form the final core themes that united all other sub-themes into an “explanatory whole” (Strauss & Corbin, 1998).
To ensure the trustworthiness of the analysis, a consensus approach between coders (Silverman, 2005) was applied. Ultimately, researchers achieved consensus on a final set of themes, categories, and codes. In an added step designed to enhance trustworthiness, the data and codes were sent to three experienced field experts to solicit their opinions on the appropriateness of the coding. Since all written data were in Turkish, the analysis process was also conducted in Turkish. All research data, categories, codes, and themes were then translated into English by a language expert and a field expert for the purpose of presenting the results.
Results
Two primary themes emerged from our team’s implementation of the QDA process: (1) Positive Change and (2) Negative Change. In addition to the labels that fall under either of these two main themes (41.1% of participant responses indicated positive change and 20.5% indicated negative change), 8% of participant responses described a mixed experience in which both positive and negative changes had emerged during the pandemic. These experiences were indicated under a third theme: “Both/And” (Positive and Negative Change). Also, nearly a third (30.4%) of participants stated that there was no change in their calling during the COVID-19 period. Many of these participants provided explanations about this lack of change. These findings fell under a fourth theme, “No Change.”
Positive Change in Calling, Category, and Label.
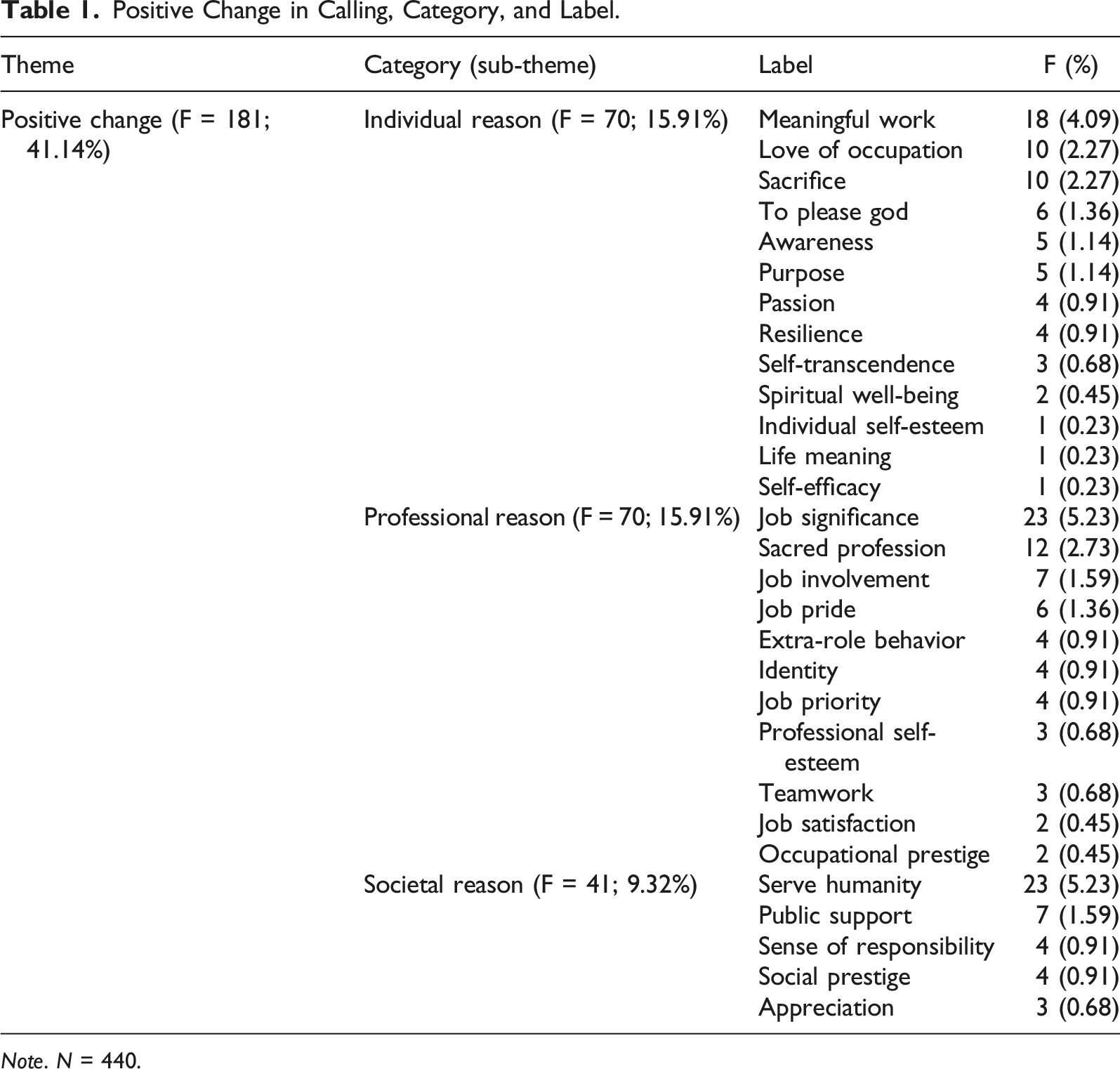
Note. N = 440.
Negative Change in Calling, Category, and Label.
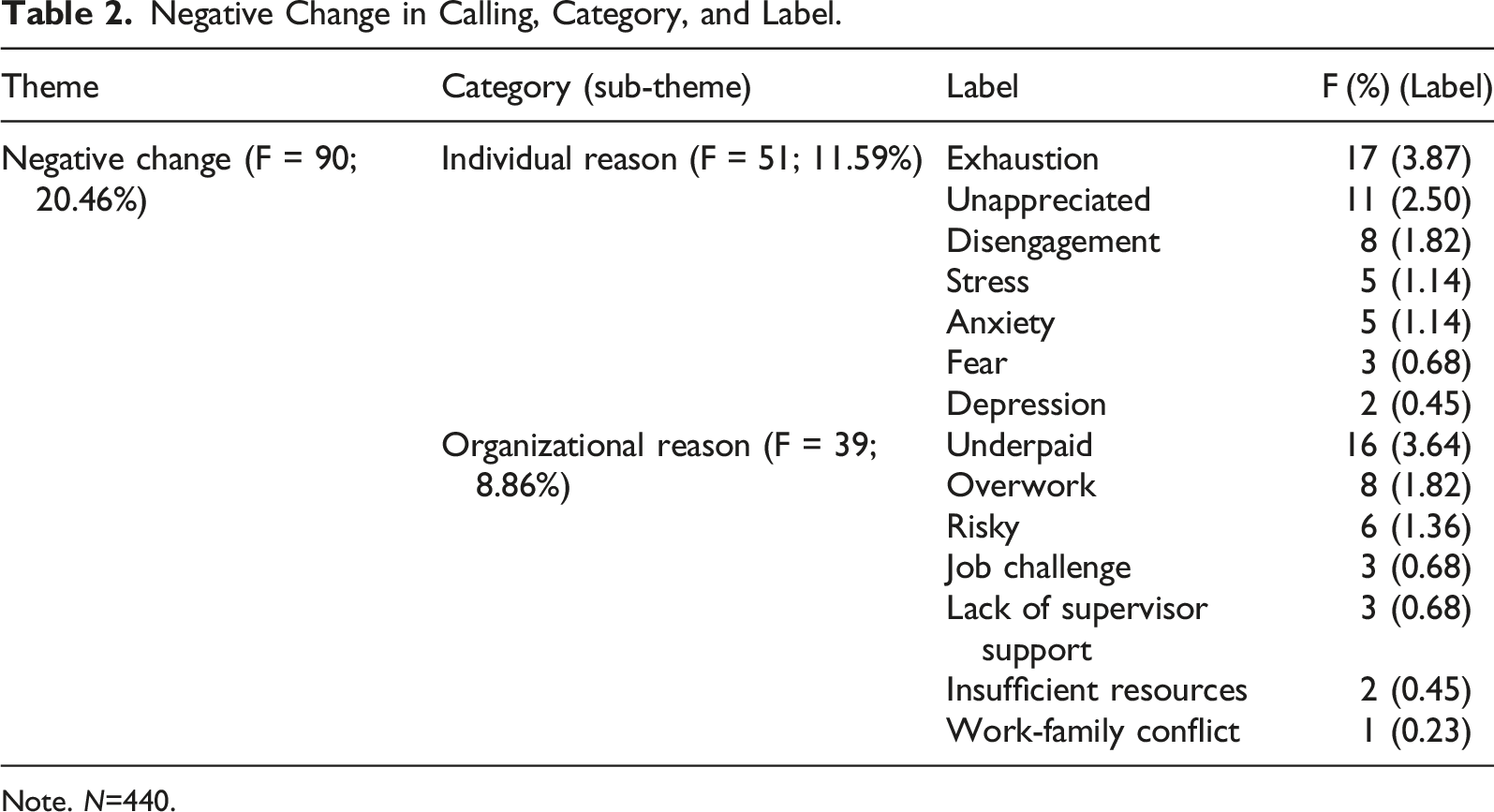
Note. N=440.
Positive Change
The first theme was positive change. A total of 41.1% of participants indicated an increase in their sense of calling during the COVID-19 period. The reasons for this change formed the basis of the categories and labels presented in Table 1. The theme “positive change” emerged from 29 labels, which were further sorted into three broader categories as follows: Individual Reason (15.91%), Professional Reason (15.91%), and Societal Reason (9.32%).
The category of Individual Reason represents participants’ internal factors influencing their experience of positive change, such as their personality or psychological states. Within this category, Meaningful Work (4.09%), Love of Occupation (2.27%), and Sacrifice (2.27%) were the most prevalent labels. Some participants stated that they understood the importance of their job in a more powerful way during the pandemic and found more meaning in their work, which in turn increased their sense of calling. To illustrate, Participant 405 (female, age 44) stated, “Changed positively. I have noticed that my job is very necessary and important and meaningful.” Others emphasized that the love they feel toward their work during the pandemic strengthened their sense of calling. For example, Participant 128 (male, age 26) stated, “Changed positively. My love towards my job increased because people care and respect us more than ever.” Sacrifice was another key individual reason that contributed to an increased sense of calling during the COVID-19 period. To illustrate, Participant 109 (female, age 50) stated “Changed positively. I have felt like a soldier who is fighting in the front to protect others.” Some nurses also explained that the increase in a sense of calling emerged from their effort please and glorify God. Others expressed new awareness of the importance of the work. Still others noted that they perceive their work as their purpose in life, or described a strong passion for the work. Others described a renewed sense of resilience during the crisis. Finally, some nurses reported feelings of self-transcendence (e.g., a sense of “We instead of I”), spiritual well-being, individual self-esteem, life meaning, and self-efficacy.
Job Significance (5.23%) and Sacred Profession (2.73%) were the most important labels among the second category (Professional Reasons) of factors spurring an increased sense of calling. These labels reflect participants’ better understanding the importance of their work and the value it provides. To illustrate this type of Job Significance, Participant 32 (female, age 40) stated, “Changed positively. I have understood more the importance of requirements and responsibilities of my job.” Similarly, the notion of nursing as a Sacred Profession was illustrated by Participant 149 (female, age 48): “Changed and I have believed and thought that my job is holy.”
The following additional labels were among the reasons why participants experienced a positive change in their calling in the Professional Reason category: Job Involvement (e.g., “Yes. I have felt more committed towards my job than ever.” Participant 394, female, age 42); Job Pride (e.g., “I have experienced tremendous changes, I have noticed that being a soldier is not in the military, it is an honor to work with self-sacrificing people.” Participant 149, female, age 48); and Extra-Role Behavior which is described as being voluntarily helpful to others or to the organization, extending effort beyond the role requirements without expecting anything in return (e.g., “I have felt very proud while doing my job without any expectation.” Participant 135, male, age 35). Furthermore, some participants stated that they felt more committed to their job and reminded themselves the importance of their job (Identity). Others changed their priorities and put their work first above everything (Job Priority). Still others increased the feelings of respect they held toward their jobs (Professional Self-Esteem). Some participants also experienced a stronger sense of camaraderie with colleagues (Teamwork); increased job satisfaction; and or an increased sense of pride towards the job.
Societal Reasons were the third category in the theme of positive change. This category identifies the perception of serving others and gaining the appreciation and support of the public. The two most important labels in this category were Serve Humanity (5.23%) and Public Support (1.59%). Gaining a renewed appreciation for how important the nursing profession is for human life and a sense of benefiting society informed the Serve Humanity label (e.g., “Once again, I have realized that nurses are important for other people. I love my job as always.” Participant 300, female, age 39). Some participants stated that their calling increased because they found the opportunity to help others through their job and enjoyed helping people (e.g., “Yes, this job is a gift given by God so that I can help others.” Participant 153, male, age 32). An increased sense of gratitude for healthcare employees by society and heightened societal support of nurses during the COVID-19 period were also expressed by some of the participants as the reasons for the increase in their sense of calling toward their job.
The final labels in this category were Sense of Responsibility, increased Appreciation from society, and a stronger sense of Social Prestige.
Negative Change
Approximately one-fifth (20.46%) of participants stated that there was a decrease in their calling during the early part of the pandemic, resulting in the second theme, Negative Change. This theme emerged from 14 labels, which were sorted into two broader categories (see Table 2). The categories were Individual Reason (11.59%) and Organizational Reason (8.86%), respectively.
Within the Individual Reason category, Exhaustion (3.87%), Unappreciated (2.5%), and Disengagement (1.82%) were the most prevalent labels. Some participants described feeling worn out during this period. For example, Participant 350 (female, age 25) stated, “I have been feeling that my patience has decreased since the beginning of pandemic. I am exhausted and my calling has decreased.” Other participants emphasized that they felt unappreciated continuously during the pandemic (“Changed negatively. I don’t feel fully appreciated; I feel completely as if my value is overlooked.” Participant 381, female, age 27). Some participants stated that their love and passion for their work decreased during the pandemic, and they became alienated from their work. Thus, these participants experienced “disengagement.” To illustrate, Participant 73 (female, age 39) stated, “My calling has changed negatively. I got demotivated and disengaged because of the changes during the pandemic management.”
Other individual reasons tied to negative changes in nurses’ sense of calling were stress, anxiety, fear, and depression. Some participants stated that their stress levels increased during the pandemic; they felt more anxious and panicked, they went to work with fear and even sought psychological treatment for depression, all of which caused negative effects on their sense of calling.
Organizational Reasons were the second category in the theme of negative change. The three most important labels in this category with the highest frequency of responses were Underpaid (3.64%), Overwork (1.82%), and Risky (1.36%). Some participants stated that the income distribution was unfair and highlighted that they were not paid what they deserved (e.g., “There have been lots of times that I have felt regretful to have this job. There are salary differences among my colleagues. Some of us have had the chance to work flexibly, some of us don’t have the chance to use flexible hours, and this is unfair.” Participant 368, female, age 41). Other participants stated that their extremely heavy workloads reveal an injustice (e.g., “Unfortunately, my calling changed negatively, actually calling is an issue that I have always been questioning however, work overload decreased my calling.” Participant 368, female, age 41). Nurses also reported experienced substantial risk of getting infected by the virus and perceived these potential risks as a survival threat (e.g., “We have felt and focused on the risks of getting infected.” Participant 419, female, age 39).
Other organizational reasons for negative changes to nurses’ sense of calling were Job Challenge, Lack of Supervisor Support, Insufficient Resources, and Work-Family Conflict. Nursing was more challenging during the pandemic for reasons such as the close proximity to patients who had tested positive, and the meaningful but taxing sense of empathy nurses experienced towards patients with possibly deadly health conditions. Nurses also reported experiencing great difficulty establishing a healthy work-family balance as they had to spend more time at work than usual, resulting in reduced time with their family members. Many participants stated that they had not received the necessary support from their managers during this period, and that their calling was negatively affected by insufficient resources in the hospital.
Positive and Negative Change (Both/And)
Some participants (8%) described a mixed experience marked by both positive and negative changes to their sense of calling. When their statements were examined, we found that all of them duplicated labels previously identified in the categories of positive changes and negative changes. Thus, these participants’ responses were compatible with the statements gathered under the two primary themes. Some participants stated that their calling increased by working with more devotion during the pandemic, but at the same time, their calling was negatively affected because of fears of contracting COVID-19 (Sacrifice label in positive change, Anxiety label in negative change). To illustrate, Participant 440 (female, age 44) stated, “I have always been a hardworking nurse who works with self-sacrifice. And I have worked with more sacrifice and calling during Covid-19 pandemic period. But I can’t help thinking and being anxious about getting infected. This situation has affected my calling sometimes.” Another participant stated that her calling increased, but that she was simultaneously adversely affected by unfair practices (Love of Occupation/Underpaid; e.g., “Changed positively but along with the love I have for my job, I think we are underpaid, and it is not fair. I love being a nurse, but this unfair payment makes me sad.” Participant 190, female, age 44). Another participant stated that although her love for the profession decreased due to the intense workload, she also experienced the joy that comes from providing benefits to people voluntarily (Extra-Role Behavior/Job Challenge). Some other reasons that cause both positive and negative changes to a sense of calling during the pandemic were Spiritual well-being/Overwork; Benefit Others/Unappreciated (e.g., “Even though I have sometimes felt unappreciated when on my job during the Covid-19 pandemic period, helping people in need makes me happy.” Participant 95, female, age 29); and Job Satisfaction/Fatigue.
No Change
Almost one-third (30.4%) of participants stated that there was no change in their calling during the COVID-19 period compared to before, and some participants made statements about the reasons for the lack of change. To illustrate, Participant 247 (female, age 51) stated, “No change. We are required to be ready all the time for the patients’ treatments” and Participant 420 (female, age 41) stated, “No change. I have loved my job before the pandemic. I have always done my job in line with scientific and patient oriented, I can say that I already have the awareness of having this job.”
Discussion
A total of 59% of healthcare employees fighting both behind the scenes and on the front lines of the COVID-19 pandemic are nurses, and the global workforce of nurses is currently around 28 million (World Health Organization, 2020b). Nurses are perhaps especially valuable in Turkey, where the number of patients per nurse is 431, more than four times the average for nurses in other OECD (OECD, 2020) countries. Nurses in Turkey had endured heavy workloads prior to the pandemic, but the demands associated with COVID-19 stretched their capacities even further. For example, Lucchini et al. (2020) reported that the increased number of intensive care patients has caused a 33% increase in the nursing workload. Recognizing their value and galvanized by a sense of purpose, nurses have described themselves as soldiers on the front lines (Sadang, 2021). Accordingly, many have performed their duties with a stronger sense of calling than before the pandemic (Kim & Han, 2021). Yet despite their shared sense of purpose, healthcare employees are uniquely vulnerable to the physical and psychological consequences of the pandemic. Beyond increased exposure to COVID-19, many have experienced anxiety and depression and have expressed reluctance to fight on the front lines if given a choice (Que et al., 2020). Understanding the competing influences on a sense of calling—both purpose and sacrifice—is an important goal for the next wave of research on calling (Duffy et al., 2018). The present study, which has qualitatively examined the direction and reasons for change in a sense of calling among nurses during the pandemic, is well-suited to pursue this goal.
Results from the qualitative analysis of answers provided to the study’s open-ended question revealed that more than 40% of nurses reported positive changes to their sense of calling during the early stages of the COVID-19 pandemic. Reasons that participants provided for positive changes to their sense of calling included positive internal resources of the individual and positive professional and social effects increase calling. The first of the individual reasons described as leading to positive change was the experience of the work as meaningful. Qualitative research is not well-equipped to test theory, but notably, this result is consistent with WCT, which positioned meaningful work as a critical connector between perceiving and living a calling (Duffy et al., 2018). Meaningful work is also an established predictor of intrinsic motivation, involvement, engagement, and commitment (Dik et al., 2020). As several scholars have noted, workers who find their jobs meaningful and live out calling may experience objective career success as well, in part because their persistence in a job creates opportunities to develop additional skills and obtain additional qualifications (Dobrow & Tosti-Kharas, 2011; Hall & Chandler, 2005). Along with meaningfulness, career commitment enhanced by calling reveals sense of satisfaction (Thompson & Bunderson, 2019). Participants also expressed an increased sense of calling prompted by enduring physical and psychological difficulties, sacrificing their families and private lives to accommodate increases in working hours. Self-sacrifice has also been described as a core part of living a calling (e.g., Bunderson & Thompson, 2009). This result is consistent with recent research in Korea, a country with a blend of Western and Eastern characteristics comparable to Turkish culture, which revealed that employees reported a strong calling and sacrifice to help others with the intention of overcoming the national crisis through their high citizenship awareness (Jang, 2020; Park, 2020).
Some nurses also stated that they are pursuing God’s will by serving other people and described experiencing increased spiritual well-being as a result. Within the work role, spiritual satisfaction can evoke or strengthen a sense of calling (Bunderson & Thompson, 2009), marked by a “transcendent summons” to serve others (Dik & Duffy, 2009). Similar to results of a recent qualitative study of nurses by Sadang (2021), many nurses in our sample described their work and its societal importance as a source of purpose in their lives. Self-transcendence was another individual characteristic identified as a contributor to an increased sense of calling. Nurses devoting themselves to benefitting humanity by putting their own lives and fears aside during the pandemic were able to focus on their work more effectively, instead of focusing on the negative changes they experienced (Chiang et al., 2007). Many nurses in our sample also described feeling more valuable and more competent during the pandemic, consistent with increased experience of competence identified in other studies examining a sense of calling (e.g., Dobrow & Tosti-Kharas, 2011). Increased passion and meaningfulness were also described as factors that increased nurses’ sense of calling. This result highlighted the importance of calling in Turkish culture. As a collectivist society, prosocial behaviors are perceived as virtues in Turkey. Although the concept is not often referred to as “calling” in Turkish culture, the converging influences of Islam and Western individualism prompt many to pursue to what they perceive as God’s will with the hope of a peaceful afterlife as a result of their dedication to benefitting others and take more responsibility towards society through their work. As a result, a sense of calling has become an increasingly important factor in establishing both career-related well-being and prosocial attitudes within Turkish culture. The roles of faith and culture are only indirectly represented within existing calling theory such as WCT (Duffy et al., 2018). Results from this study suggest that such factors may warrant more direct inclusion within WCT and other theoretical approaches. A “cultural lens approach” offers one strategy for more deliberate consideration of cultural influences in how calling links to outcomes (Dik et al., 2019).
In terms of professional reasons for an increased sense of calling, job significance was the most frequently stated factor. Although job significance and meaningful work show similarities, they are distinct constructs. For this reason, we label them separately. Finding or creating a job meaningful is about why a person does it, what that job means to the person, or the whether the job makes meaningful contributions to the lives of others (Miller, 2008; Rosso et al., 2010). Participants’ statements about job significance revealed that the nurses perceive their jobs as important, evoking careful attention to their duties.
Among the professional reasons, nurses described feeling more connected to their work during the pandemic. Some described themselves as heroes, and the sense of dignity and pride that came from fighting the disease on the front lines positively affected their calling during a time when many employees were afraid of approaching the hospitals. Extra-role factors, identity and job priority were among the reasons that strengthened the sense of calling for others. Indeed, some nurses described viewing their work as calling more than ever when they worked hard and recognized their work as a central part of their lives. This evidence aligns with other research establishing teamwork, job satisfaction, and job dignity as influences that contribute to a sense of calling during the pandemic (Villar et al., 2021).
The third and last sub-theme related to the positive change of calling was societal reasons. Many nurses stated that they had a better understanding of the contribution of their work to humanity. Many described an enhanced experience of pleasure and responsibility that comes from serving others during a public health crisis. Given that positive societal impact is at the center of calling (Dik & Shimizu, 2019; Thompson & Bunderson, 2019), the nursing profession is perhaps uniquely suited to stimulate and maintain this approach to work (Villar et al., 2021). Although the service that nurses provide to society is nothing new, their increased sense of appreciation and value during the pandemic has increased morale within the nursing profession (Sadang, 2021). Regardless of the reason, a strengthened sense of calling is a desired outcome both at the organizational and individual level. Workers’ sense of calling not only increases desired positive outcomes such as work engagement, job satisfaction, organizational citizenship behavior, and job performance (e.g., Park et al., 2016; Ziedelis, 2019) but it also enhances their career commitment of individuals (Duffy et al., 2011). If a nurse experiences high career commitment and associates the nursing profession with a higher purpose of life, the probability of leaving the current job and showing deviant behavior in the workplace is, theoretically, reduced. Also, employees with high levels of calling have a tendency to stay in their current organization and experience more satisfaction and participation (Afsar et al., 2018).
Some participants reported negative changes to their sense of calling during the pandemic, driven primarily by experiences of exhaustion and underappreciation. Nurses expressed feeling exhausted, tired, and worn out both physically and emotionally during the pandemic, a finding consistent with other research on workers enduring crisis-related demands (Sun et al., 2020; Sadang, 2021). Other nurses expressed dismay over injustices regarding comparatively low salaries, increases in workload, and other factors that can be attributed in part to poor management. Some expressed that they had considered changing their jobs or quitting in response to these concerns. With intense feelings of overwork, some nurses stated that they were alienated from their profession, their enthusiasm for the work was almost gone, and their calling decreased as a result, all factors consistent with work disengagement. Others described experiencing an uptick in stress, anxiety, fear and depression, a finding supported by other studies of mental health consequences faced by nurses during the pandemic (e.g., Hu et al., 2020; Tan et al., 2020). Feelings of being unappreciated were also noted, as were fears rooted in risks that come from constant exposure to COVID-19, and fear stemming from the prospects of infecting family members. Finally, some participants noted a lack of supervisor support and insufficient resources, factors that had previously been identified by Bailey and Madden (2016) as linked to a sense of meaninglessness in employees. From a theoretical perspective, perceptions of unappreciation, lack of support, and few resources may be considered aspects of (a poor) psychological climate, one of the moderators proposed within WCT as part of the mechanism through which workers living a calling experience negative rather than positive outcomes (Duffy et al., 2018). However, exhaustion stemming from the work itself is not well captured by the theory, perhaps in part due to its focus on psychological rather than health outcomes. Nevertheless, it represents another factor that warrants consideration in further theoretical development.
Our results also point to a need for calling theory to consider a broader array of outcomes than those included within WCT. During the pandemic, the emotional and physical exhaustion of nurses, their feelings of being unappreciated due to unfair organizational practices and high levels of anxiety reduced their sense of calling and decrease their efficiency, productivity, and job satisfaction. The result is often absenteeism, turnover intentions, and an inability to retain the trained and experienced workforce in an organization (Gray et al., 2021; Nayeri et al., 2009). However, healthcare employees have been affected seriously and felt the heavy burden of Covid-19 pandemic (Armocida et al., 2020), thus an increase in psychological problems such as anxiety and depression along with these negative experiences during the pandemic is probably unsurprising. A more expansive theoretical focus than that currently included within WCT should attend to such outcomes.
Importantly, for some participants, these positive and negative influences on a sense of calling co-existed. This paradox was also found in Sadang’s (2021) qualitative study of nurses during the pandemic, many of whom described the challenges and risks as held in tension with the honor, privilege, and self-satisfaction in their oath as professional nurses.
Limitations and Directions for Future Research
One of the limitations of this study is that the research data were obtained through a single open-ended question using an online questionnaire. Although this data collection strategy was necessary given the challenges of conducting research during the pandemic and due to the heavy working hours of the nurses, it clearly prioritizes breadth over depth. Interview-based approaches would extend this study by gathering richer, more in-depth qualitative data. Another limitation is that data were collected at a single time point. Subsequent research would benefit from follow-up or longitudinal designs capable of examining change over time, especially given the evolving and fluid nature of pandemic realities in providing health care. Qualitative research, by nature, is theory-generating rather than theory-testing. For example, while we found WCT helpful in framing our study and explaining results, follow-up research using quantitative methods to directly test WCT propositions, perhaps with additional outcome variables that extent beyond those currently targeted by WCT, represents an important next step.
Finally, the regional focus of this study, having been conducted among nurses in Turkey, raises questions about the transferability of its results. Subsequent research should examine nurses in other nations and cultures as well, especially those where the pandemic is similarly intense, to compare the findings and examine differences.
Implications for Practice and Policy
Our results show that positive change in nurses’ sense of calling can be caused by individual reasons such as meaning, purpose, spirituality, self-sacrifice, and passion, as well as by both professional and social experiences such as the importance of the work, sacredness of work, teamwork, public support, and social prestige. However, facing relatively low salaries, excessive workload, health risks, and suboptimal management practices have made many nurses feel exhausted during this crisis period, prompting some to think of quitting. A sense of calling is frequently described as being motivated by a power beyond the person, but constant exposure to negative conditions is likely to have a deleterious impact no matter how strong a person’s motivation. Considering the indefinite duration of pandemic-related pressures, national and local decision-makers would do well to emphasize the contribution of nurses and take steps to support their growing needs. This includes attention to fairness in the workload distribution and meaningful efforts to provide adequate opportunity for rest. Again, being underpaid has a strong effect in nurses' perceptions of injustice. Financial reasons such as not earning the wages they deserve despite their high efforts, pay that is disproportionately low given the level of risk their work demands, lower wages compared to their colleagues and/or other healthcare employees doing the same job, and inadequate protection of their personal rights have left some nurses feeling undervalued and discriminated against and has caused a decrease in their sense of calling. On a policy level, we urge national and local decision-makers to prioritize salary increases for nurses, implement a balanced wage policy within the labor force, and improve protections of nurses’ personal rights.
Access to psychological support tailored to foster coping with burnout, stress, exhaustion, anxiety, and depression is advised as well, although ultimately structural changes are needed to address the sources of these concerns. A study conducted during the pandemic in Turkey revealed that 42.6% of nurses needed psychological support (Aksoy & Koçak, 2020), and the pandemic’s impact is likely not limited to short-term distress; healthcare employees in particular may experience trauma-related disorders and acute stress in the long term (Autin et al., 2020). Organizations can use multi-pronged approaches to ameliorate these negative effects by providing safe work environment and implementing trauma career counseling approaches which include evaluation of trauma symptoms, use of ecological frameworks to conceptualize associations between traumatic experiences and work, developing coping strategies, and promoting career adaptability (Barrow et al., 2019). The current study also highlights how the sense of calling experienced by some nurses decreased during the pandemic period. A strong sense of calling, in theory, acts as an internal compass for navigating hardships, thereby promoting resiliency (Hall & Chandler, 2005). It also is linked to satisfaction and career adaptability (Xie et al., 2016). For these reasons, it is important in the healthcare sector for human resources, career counselors, and managers to help employees retain and indeed strengthen their callings. Simple but genuine expressions of gratitude for the indispensable work nurses do may help add meaning to their work (Afsar et al., 2018). Early training for prospective nurses would also do well to paint a realistic picture of the profession’s challenges and rewards, pointing out the profound need and also the inherent value and dignity of providing care to the ailing.
Conclusion
Our study provides new insight into the types of changes people experience in their sense of calling, especially during extraordinary or crisis periods. More specifically, the study reveals changes in nurses' sense of calling, as well as potential sources of these changes, within in Turkish culture using an exploratory, qualitative approach. This study is also among the first to investigate a sense of calling within the context of Turkish culture. Results reveal that during the Covid-19 period, most nurses have experienced changes in their calling in positive and negative directions, sometimes simultaneously. More participants reported positive changes than negative changes, and the reasons offered for positive changes included finding their job and life meaningful, experiencing love toward their job, and experiencing renewed passion or spirituality. Other reasons included their desire to help others, the experience of strong connections to their job, a sense that the job is sacred, and a sense of pride in the work. Serving humanity and sensing support from society influenced positive changes in their sense of calling as well. On the other hand, the exhaustion of nurses during the COVID-19 period, the inequalities in the workload and wage distribution, and their belief that they are not given enough value and support are among the chief reasons for negative change. Discovering the mechanisms behind how a sense of calling is experienced in times of crisis offers a guide for practitioners on how to strengthen and protect their callings, and help others do the same.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.