
Abstract
Background
Forced migration results in exposure to trauma, interrupted access to healthcare, and loss of social support and may increase dementia risk. Literature on refugees’ knowledge of dementia and its risk factors is scant. This study investigates refugee perspectives on dementia and their access to cognitive healthcare in the United States (US).
Methods
We conducted 6 focus groups and 30 individual in-depth interviews (total of 69 participants) with Arab, African, and Afghan refugees resettled in San Diego, California. Data was coded using inductive thematic analysis.
Results
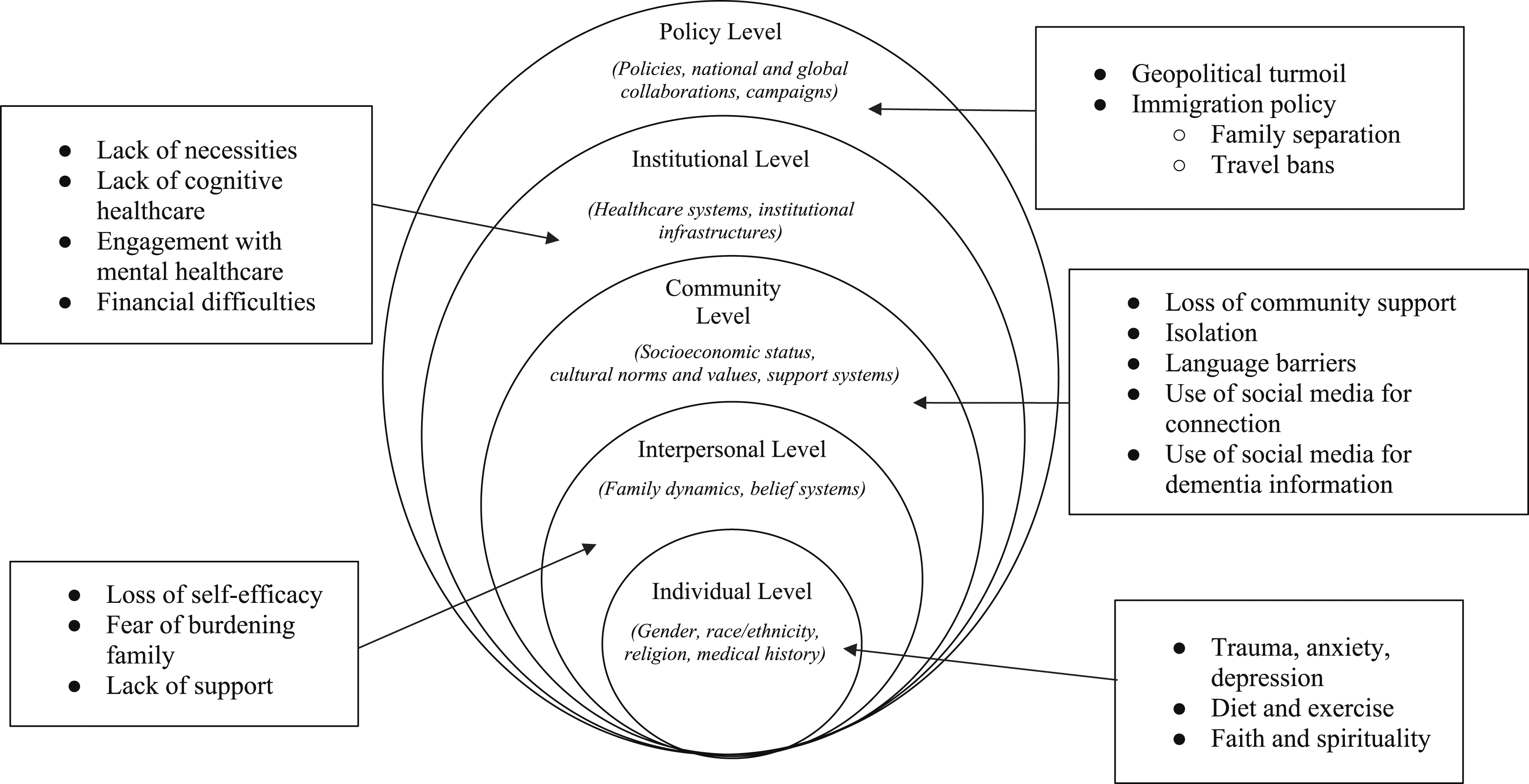
Organized by the socioecological model of health, the following themes emerged: (1) mental trauma due to migration was linked to dementia (individual); (2) fear of dementia and burdening caregivers due to limited support systems (interpersonal); (3) reliance on virtual communities for dementia information and the stress of local community loss increasing dementia risk (community); (4) healthcare providers, both in the US and in refugee camps, didn’t address cognitive health concerns (institutions); and (5) discriminatory immigration and healthcare policies as barriers to healthy aging (policy).
Discussion
Despite being a heterogeneous group, refugees share specific experiences, knowledge gaps, and barriers to healthy aging. Tailored interventions and policies are needed to address this population’s cognitive health needs. This includes addressing their mental health and social support concerns as well as training clinicians to screen for/discuss dementia with aging refugee patients.
Keywords
Introduction
Dementia-spectrum disorders affect 55 million people globally, with estimates of triple the diagnoses by 2050. 1 As a chronic condition, dementia often results in long-term care needs and caregiver burden, with estimates of $500 billion worth of healthcare costs in the United States (US) alone. 2 The prevalence of dementia is higher among racial and ethnic minorities than in the general US population and there is growing concern that refugees may have a higher risk of dementia. 3 As forced migration increases, many refugees are aging in exile. In the US, specifically, African and Middle Eastern and North African (MENA) refugees constitute the largest refugee populations and these communities are among the fastest-growing aging groups.4-6 The intersection of forced migration and the growing aging population poses new challenges in domestic and global geriatric and dementia care.
Unlike other immigrant groups, exposures throughout the forced migration trajectory, such as exposure to violence, low socioeconomic status, discrimination, cultural barriers, trauma, and limited healthcare access are prevalent among refugee groups and may increase their risk of cognitive aging.7-12 While some literature touches on perceptions and attitudes towards dementia and cognitive aging within MENA and African non-refugee communities, few contextualize these attitudes and perceptions as they intersect with the migration and refugee experience specifically.13-15 Refugees have multiple risk factors for dementia, including high rates of uncontrolled hypertension, post-traumatic stress disorder (PTSD), and depression all of which are linked to cognitive decline in other populations.16-23 Despite this, refugee groups are rarely included in dementia research and prevalence rates remain unknown in this population. One recent study, for example, found that Arab-Americans fleeing war in their native countries reported poorer cognitive function than white Americans and Arab immigrants migrating from politically stable countries, suggesting a link between exposure to war and cognition. 3 There is also currently no consensus on evidence-based clinical practice for assessing dementia among refugees, likely resulting in largely undiagnosed cognitive impairment and dementia among refugees. Several European studies identified multiple barriers to diagnosing, assessing, and managing dementia in refugees, including language barriers, difficulties involving family members in care, and poor information exchange.24,25 Similarly, a meta-analysis on cognitive aging in Arab Americans lists several factors, including lack of validated screening tools and rampant anti-Arab discrimination, as barriers to proper diagnosis and management of dementia. 26 This is overlaid on already tenuous healthcare access for refugees and poses a significant public health challenge.27,28
Forced displacement and dementia pose two distinct public health challenges but there has been little exploration of the interplay between the two, despite projections that rates of both will continue to climb. 29 This exploratory qualitative study will investigate the perspectives of Arab, African, and Afghan refugees in San Diego, California on cognitive aging and assess their perceptions and knowledge of dementia. This preliminary research is critical to ensuring that future work, such as developing or adapting screening tools and establishing prevalence of cognitive impairment in different refugee populations, is sensitive to refugee perspectives and priorities.
Methods
Setting
San Diego is a large refugee resettlement hub in the US, with around 32,000 arrivals between 2002 and 2021. A majority of refugees in San Diego originate from the Middle East (including, in recent years, Afghanistan) and sub-Saharan Africa, amounting to 87% of the county’s refugee population. 30 A majority of refugees fled their countries of origin due to persecution, conflict, violence, or human rights violations. 31 San Diego is an ideal research location to conduct work on refugee health given its longstanding history of resettling newcomer migrants and a plethora of community-based institutions catering to their medical, socioeconomic, and legal needs.
Participants and Recruitment
Participants were recruited between December 2021 and September 2022 through snowball sampling with the initial recruitment support of our partner organizations who have a long-standing history within San Diego’s refugee community and who have previously collaborated with our institution and research collective. It was critical that we partner with community leaders and members who best understood the needs and values of our target population. These organizations include the: Family Health Centers of San Diego, a federally-qualified health center and major refugee healthcare provider, and ethnic-based community organizations including the Majdal Center, the Afghan Community Culture Center, and the Somali Family Services. Inclusion criteria were: (1) having a present or former refugee status and (2) identifying as Arab, Afghan, or African. Exclusion criteria were: (1) those unable to provide informed consent. Interested participants were contacted by phone to screen for inclusion and exclusion criteria and to collect verbal informed consent. Participants were then scheduled for either gender-concordant focus groups or individual interviews between March and December 2022. Participants were compensated with a $35 gift card for their time delivered after completion of the interview. Upon completion of the interview, interested participants were asked to share our study information with other community members who may fit our inclusion criteria.
Data Collection
A semi-structured, in-depth interview guide was developed by an interdisciplinary research team following a thorough literature review (Appendix A). The guide was piloted for feedback with community partners listed above. Interview questions explored participant understanding of dementia, their perceptions of personal risk factors for dementia, the role of the refugee experience in cognitive aging, and access to cognitive healthcare. Demographic information was collected at the time of study enrollment. Data was collected by team members with native fluency in Arabic, Dari, Pashto, and Swahili. We began with 6 focus groups lasting 60-90 minutes to identify recurrent topics, then conducted 30 individual interviews lasting 30-60 minutes to follow-up on particular themes. We conducted individual interviews until we reached saturation of themes. Focus groups included 2-5 participants from the same ethnic background, gender, and spoken language. Both individual interviews and focus groups were scheduled in-person or on a password-protected video conference platform to abide by local COVID-19 social distancing protocols. Interviews and focus groups were audio-recorded, transcribed in the target language, translated into English by certified interpreters, and reviewed for content and accuracy. All data was analyzed upon completion of data collection.
Data Analysis
Five team members with access to all the raw data independently reviewed and coded each transcript using ATLAS. ti software. The team met weekly to conduct this data analysis. All five members worked collaboratively to build a de-novo codebook and establish intercoder reliability using 20% of the dataset before dividing up the remainder of the dataset. All five team members participated in analyzing the data and codebook for broad categories or themes. Inductive thematic analysis was done through the identification of recurrent themes following Crabtree and Miller’s 5-step interpretive process. 32 We used the socioecological framework to contextualize our data and capture the various interactions between social structures and individual experiences in cognitive aging.33-35
Ethical Approval
This study was approved by the Institutional Review Board (IRB) at the University of California, San Diego (IRB# 201634, 190483). This study was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki. Our study embodies diversity, equity, and inclusion by studying not only a marginalized population in US healthcare (i.e. refugees), but also a diverse population within that subset. We partnered with community-based leaders (acknowledged below) to ensure recruitment was accessible, fair, and representative of our target populations.
Results
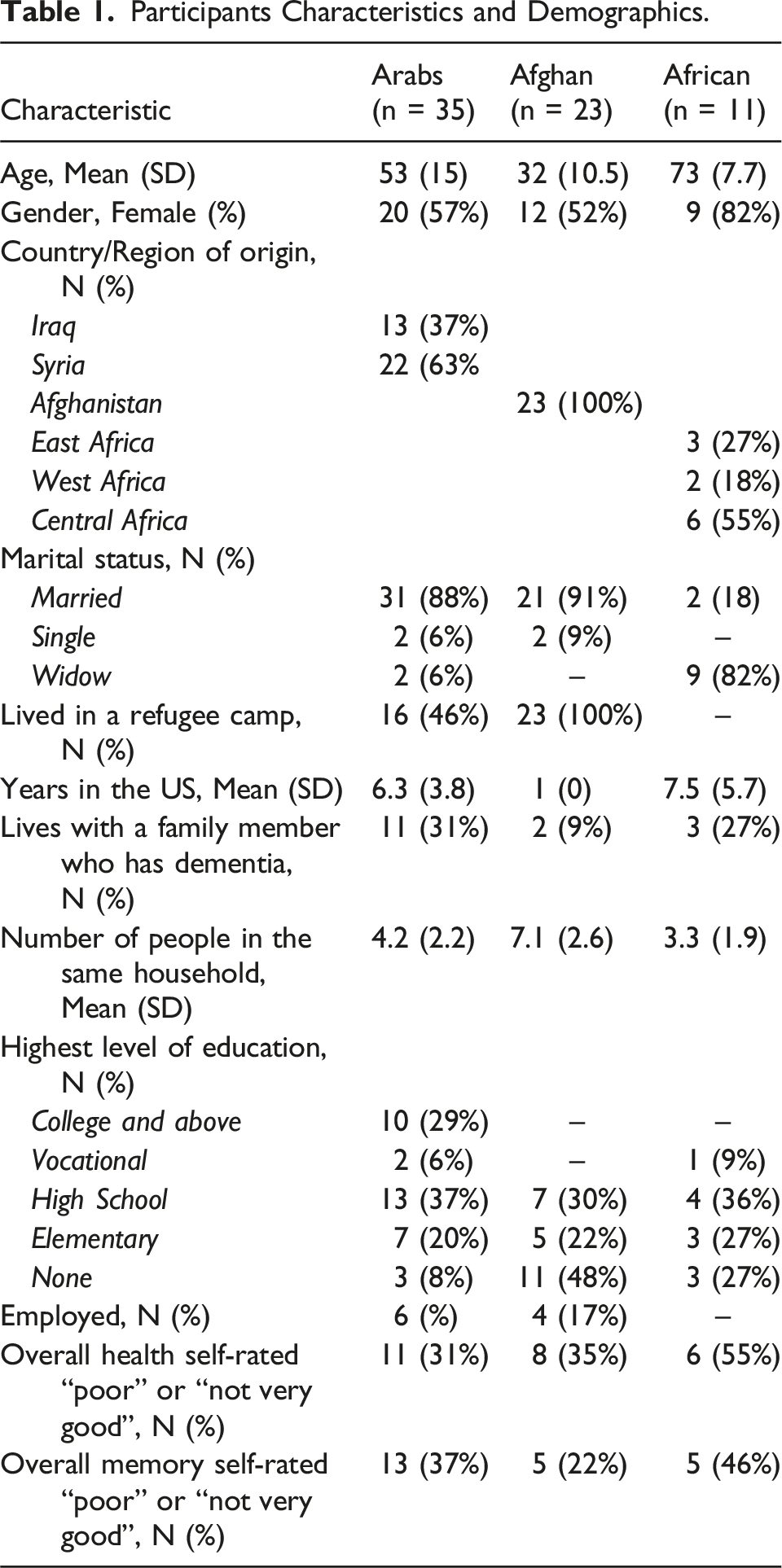
Participants Characteristics and Demographics.
Socioecological model of health: Refugee perceptions and understanding of dementia.
Individual Level
Participants had general knowledge of dementia as a neurologic disease resulting in memory loss, behavioral changes, and impaired cognitive function:
“[A] person who has Alzheimer's forgets things. they forget simple things. They forget chores they have to. […] There has to be a person to help them” (Arab Woman)
“This is a disease and not just about aging.” (African Man)
“I think that it is a disease where someone is not in their right mind–like they act, they just aren’t in their right mind.” (Arab Woman)
Participants believed stress, traumatic experiences, and mental ill-health related to their migration history were linked to dementia:
“What puts people at risk of dementia is when they’re thinking 24 hrs and there’s a burden on people and they’re stressed out.” (Afghan Man)
“[Dementia] comes about because of the way people live their lives…if they have a stressful life.” (African Woman)
“There are diseases that lead to dementia, such as depression and anxiety.” (Arab Man)
War and violence were listed as the impetus for migration for most participants. This specific set of exposures was perceived by participants as a risk factor for cognitive decline and many felt like they were prematurely aging as a result: “[Life in Iraq is a] life not worth living…The war hurt us a lot. Even when we left Iraq…the conditions were really difficult. The situation was really difficult as displaced people…It was never easy. So, of course, this affected [our brain].” (Arab Woman)
Participants believed in personal preventative actions to protect from premature cognitive aging and dementia. Many participants cited the importance of intellectual engagement, including having hobbies, reading, and generally keeping cognitively active:
“Old people have to read and make their brains work. They can’t keep stagnant. They have to keep their brains in use.” (Arab Woman)
“Going to school, you get busy and you keep learning new things so that makes our minds focus on that rather than worrying. This does prevent dementia.” (Afghan Man)
Many also noted the importance of a balanced diet and exercise for brain health:
“For dementia, there should be an [exercise] program like, for example, walking. At this age, we have to do some exercise.” (Arab Woman)
“Healthy food helps with the formation of healthy [brain] cells.” (Arab Man)
Faith, spirituality, and religious practice were also reported as common methods for slowing pathological cognitive aging:
“If you read the Quran – or it doesn’t have to be the Quran, whatever religion that you’re from – and pray, and always think about God, the chance of getting dementia is really low.” (Arab Woman)
Interpersonal Level
Participants expressed fear of dementia due to concerns of losing their memory, regressing to child-like behaviors, and losing a sense of ability and personal agency:
“The life of someone who has memory loss becomes nothing. They don’t remember or know anything about their life. Everything they’ve built is lost.” (Arab Woman)
“[Dementia] is what happens to the brain when people become just like children.” (African Woman)
Specifically, participants reported fear of emotionally hurting loved ones and being a burden. Women especially were concerned for their children and the difficult responsibility of elder care:
“Of course I have to worry a little about it. Not being able to remember my children, my family. This makes you feel like a burden.” (Arab Woman)
Participants also reported lacking the personal support system to be properly cared for, in their aging generally and for dementia specifically. Many noted the unique challenges faced by their smaller family unit sizes in the US as compared to their home countries:
“I know [dementia] is very dangerous, especially for old people like us that don’t have people around us like children or anyone else next to us. This is my fear.” (Arab Woman)
“If someone keeps having problems and no one around to calm them down, to listen to them, they’ll become depressed and eventually they’ll explode.” (Arab Woman)
“If you are an old person and are living with all these stresses, you have no one to talk to and all you think about is the torture you’ve been through, your memory will decline.” (African Woman)
Community Level
Participants expressed the loss of local community in the US as a source of acculturation stress. This isolation was cited as a major barrier to their current well-being and deemed an important source of dementia risk:
“Dementia comes about because of the way people live their lives...if they’re isolated and have no one to talk to.” (African Woman 3)
Many reported experiencing isolation throughout their refugee journey, including in refugee camps and in their resettlement in San Diego:
“I just stay by myself and isolated. I don’t tell people about the bad experiences that I had…I feel like this is impacting me a lot.” (Arab Woman)
Language and cultural barriers were challenges in adapting to the US and played a role in hindering integration and worsening isolation:
“Here we’re far away from our work, our family, and our loved ones. The things that we were used to there are a bit different from here.” (Arab Woman)
“The first year is hard…when you came to America you’re met with discrimination and oppression. So at the beginning of settling in a new country, it’s really difficult.” (Arab Woman)
Many reported challenges in passing on their cultural values and traditions to their children, which furthered feelings of estrangement within their host country:
“Life is different here. Some people are getting ignored by their kids so they get sad and their mental health gets affected. Kids don’t want their parents anymore and this is affecting the parents.” (Arab Woman)
As a result, many participants relied on virtual communities. Many praised tools such as YouTube, WhatsApp, and other forms of social media as a way to remain connected with people of similar experiences and as a source of enrichment. Participants often cited these platforms as places to get information about dementia:
“Social media helps us a lot. Like now we’re together sharing our stories because of social media. These technologies are a tool that allowed communication between us and those we love.” (Arab Woman)
“We gain information through reading books, articles, social media. When we’re watching television, there are ads, so we get information from that too…Also we can access information through social media or reading newspapers.” (Afghan Man)
“When I have some sort of disease, before I go to the doctor, I search it up on Google to see what I should do about it… So the most important thing is YouTube. I use it a lot.” (Arab Woman)
Despite the loss of social networks experienced during the migration journey, most participants emphasized the importance of community and social connection, especially as a form of protection from dementia. Community-based programs facilitated their rebuilding of community:
“When we first came here…we heard there were programs at the International Rescue Committee. We decided to start there and communicate with more people. In a year, we learned how to go out, we signed up for adult school; everything became easier and we didn’t feel like we’re out of our country.” (Arab Woman)
Institutional Level
Participants who lived in refugee camps before resettlement in San Diego had more positive experiences with US healthcare institutions than their counterparts who did not spend time in refugee camps. Participants who experienced life in refugee camps reported lack of access to basic needs, high cost of medications, long wait times for medical care in refugee camps:
“They bring you food even if it’s not good for you…It’s not like we aren’t thankful, we are, we’re thankful for any thing that keeps us alive. But there are some things better than others.” (Arab Man)
“There was definitely no [quality] healthcare in the camps, there was no healthcare in the hospital that was inside the camps.” (Arab Woman)
“[At] the camp…there were no bathrooms, no water, no electricity, no floors. So it was a really bad situation and there were also sicknesses... It was really harsh conditions.” (Arab Woman)
As a result, when comparing their experience in mismanaged refugee camps to more organized American healthcare systems, they had more positive perspectives:
“[In America], services are good. I wouldn’t say otherwise…Our life in America is different from other countries…Everything is provided, they provide you a place to work, everything here is provided…If you want to live, you can live.” (Arab Man)
Participants who resettled directly in the US reported frustration with the healthcare system including lack of efficiency, difficulty navigating the multi-tiered referral systems, and delays in care:
“The only hard thing here is waiting for your turn and sitting in the lobby for hours while your body is hurting and they tell you to wait like 15 to 20 days for your turn to come. This is the hardest thing here. In Iraq, as soon as we feel pain, we go to the doctor and the doctor lets us in right away to treat us but here it’s different. Here they have all the equipment but the wait time is excessive. I feel like people get even more sick until a doctor sees them.” (Arab Woman)
“[In America] every day there’s a new doctor that I have to go to get better. And I don’t feel like I’m getting better. [In Syria], the doctor understands me right away. But here, there are like a million stories and a million lab work and a million nurses. So as a result your sickness worsens instead of getting better.” (Arab Woman).
Despite these differing perspectives on US healthcare, participants across the board reported that providers did not address their cognitive health needs, including providing dementia screening, counseling them on dementia risk, and answering questions about cognitive health and memory:
“[My physician] has never talked to me about [dementia] or given information. [Dementia] is a big problem we’re hearing about in the community.” (Arab Woman)
One caveat, however, is many participants reported engaging with mental healthcare systems, including getting screened for PTSD, depression, and anxiety and getting therapy services. While some acknowledged the stigma associated with mental healthcare, few cited it as a deterrent to seeking mental health support. Rather, they stated more pressing health concerns and financial constraints as barriers to psychiatric care:
“When I first started going to a psychologist I thought the doctor would write a report that I’m not good and I’m [mentally unstable] but, it turned out, he helped me to live my life in America.” (Arab Man)
“One must go to a psychiatrist in order to talk about [our traumas]…You cannot go to a cardiologist or a nephrologist–only a psychiatrist. But I don’t have the time… [If I] didn’t have that much stuff going on and they were free, I would go.” (Arab Woman)
Policy Level
Participants reported frustrations with immigration policies and geopolitical turmoil as general barriers to healthy physical and cognitive aging:
“As refugees, we’ve been here for six years and we didn’t get anything, we didn’t get any green card or visas or anything…This was the thing that caused me stress and made me unhappy. I really reached rock bottom... This affected us a lot.” (Arab Woman)
These policies resulted in challenges with family separation, worsening feelings of isolation and stress among participants, and, overall, negatively impacted cognitive health:
“Some of my sons are still left in Afghanistan. I worry about my kids, like not knowing if they’re eating well, not knowing if they’re alive. Thinking about my family back home…things like this cause dementia.” (Afghan Woman)
“One of my children, it has been ten years since the last time [I’ve seen them]…Of course it’s going to impact my health, like my memory and my health.” (Arab Woman)
For Arab participants, in particular, many were affected by the Trump-era travel bans and their ongoing ramifications:
“[In Jordan] my son could come visit us…But here it’s not like that. Even visiting is so difficult…I applied for a visa for him a year and a half ago and we still didn’t hear anything…I don’t understand why it’s difficult, like we’re not doing anything bad. We’re working and we’re getting lawyers and we’re trying to figure this out but it’s just not working.” (Arab Woman)
Discussion
This study uses a socioecological framework to highlight understandings, perceptions, and attitudes towards dementia in refugee populations resettled in San Diego. Our findings emphasize participants’ rich understandings of dementia and cognitive aging, as well as relevant risk factors encountered throughout their migration trajectory. Participants also reinforce previously cited barriers to adequate healthcare and healthy aging in immigrant groups, including challenges with healthcare systems, community integration, language and cultural discordance, and lack of social support.36-38 These results are consistent with prior studies exploring public knowledge and attitudes toward dementia and, more generally, healthy aging, particularly in other underserved or immigrant communities.39-44 Our study, however, remains one of few to explore the specific nuances experienced by refugees, which vary from other immigrant and underserved groups. For example, one study exploring attitudes towards dementia in Syrian refugees similarly demonstrated an understanding of dementia rooted in trauma and significant challenges access cognitive healthcare and social support. 41 Another study in Vietnamese migrants, largely political refugees, echoes many of barriers to care, including cultural and language discordance, also expressed by our participants. 39
Based on our results, we identified four areas of intervention to address these lacunae in dementia and cognitive healthcare for refugee communities: (1) improving medical and social services workforce engagement in cognitive aging needs, (2) developing appropriately validated and disseminated clinical care guidelines, (3) building on population strengths and developing community-based interventions, and (4) addressing overarching immigration and healthcare policy needs.
Workforce Engagement
As described in our institutional-level findings, no participant reported receiving counseling or screening about their cognitive health from their medical providers, despite many reporting feelings of premature cognitive aging and memory challenges. Their general gestalt of increased dementia risk due to trauma exposure and mental ill-health is correct and well-documented in the literature.17-23 It’s therefore critical for medical providers to recognize migration history, particularly forced migration, as a notable risk factor for accelerated cognitive aging and to ensure proper screening, prevention counseling, and referral to specialty care. Many studies recommend using immigration history as a social determinant of health and recognize its importance for contextualizing the medical history. 45 Further training for providers in primary care settings, as well as providers engaged in cognitive healthcare, is needed to reaffirm the importance of migration in clinical decision-making generally, and cognitive healthcare specifically.
In addition to addressing provider knowledge, it’s also important to support clinicians who interact with refugee patient populations. Prior literature highlights provider challenges in carrying out this work, particularly with logistical constraints (e.g. limited time, language barriers).24-26 More public health funding needs to be allocated to ensure access to clinic-based interpretation services, social workers, and administrative support. Similarly, these barriers to care are often echoed by patients who report difficulty navigating a complicated healthcare system. Refugee populations are known to better engage with US healthcare systems when linked with care navigation and case management services.46,47 In particular, the community health worker model increases appropriate utilization of healthcare services while ensuring culturally-concordant care and investment in community growth.48,49 Training community healthcare workers to recognize the importance of cognitive health can both increase awareness for cognitive healthcare amongst elder refugee populations and empower patients to bring up such topics with their providers.
Interestingly, our participants demonstrated a relative acceptance of mental healthcare services. Given the relationship between mental ill-health and dementia, and the high rates of mental illness in refugee groups, it’s critical to interlink our approach to both disease processes in this population.24,25 Mental healthcare workers have high rates of contact with refugees and may be a useful provider pool for increasing cognitive health education, screening, and referral. Further research is needed to assess benefits and challenges of partnering mental healthcare workers in cognitive healthcare.
Clinical Guideline Development
It is important to note that refugee groups aren’t a monolith – they hail from various socioeconomic experiences, cultural groups, and linguistic backgrounds. Nevertheless, they share many unifying attributes, specifically with trauma exposure (be it pre-, during, or post-resettlement). In this particular way, the refugee experience can be universalized. Our participants’ perspectives reflected this reality: despite variations in health literacy amongst the different groups, all had a general understanding of dementia and their mental health history as a risk factor. While we mustn’t lump all refugees into one category when generating care plans, such exposures may be universal for all displaced populations and may simplify the question of whether to educate or screen certain patients for dementia. 50 Future research is needed to assess the validity of available screening tools and their appropriateness for this population. Adaptations may be necessary to account for literacy level, language barriers, interactions between migration history and cognitive function, etc. 25 How we screen individual refugees may vary, but refugee status should be an important social determinant of health affecting the clinical decision of when to screen.
Building on Community Strengths
Despite the loss of community throughout the refugee journey, this population’s resilience is well-documented.51,52 Many rebuild communities in their host countries or find ways to remain in contact with old personal networks, as evidenced by our participants’ robust uptake of social media tools. Supporting refugees in building and strengthening such communities is critical to ensuring their long-term integration and well-being in resettlement. Furthermore, tapping into these pre-existing networks (e.g. social media groups, community centers, ESL class cohorts) provides opportune spaces to pilot public health interventions, such as brain health education initiatives.53,54 Such an approach has the dual impact of (i) disseminating public health information about cognitive aging, specific refugee-related risk factors, and engagement with cognitive healthcare providers; and (ii) investing resources into building community, which can combat much of the reported isolation and acculturation stress experienced by this population.
Overarching Immigration and Health Policy Changes
Many participants highlighted immigration challenges and family separation policies as sources of stress affecting their mental and physical well-being. The refugee experience is one rife with trauma and it is incumbent upon host communities to mitigate that trauma’s impact and long-term consequences. While further research is needed to assess whether “treating” trauma will improve cognitive health outcomes, a trauma-informed approach to immigration policy can limit new stress and compounding of prior trauma exposure experienced by refugees upon resettlement. Examples of such policy actions can include prioritizing family reunification, ensuring prompt and low-cost access to mental healthcare, providing access to care navigation, social work, and case management services upon arrival, and funding community-based initiatives to improve social integration and belonging.
Limitations
This study has a few limitations. While our sample size is considerable, our participants were recruited via snowball sampling, which may have led to an over-recruitment of participants knowledgeable about or with secondary exposure to dementia and who were eager to discuss cognitive health topics. Additionally, while we captured the experience of participants from various socioeconomic backgrounds, migration experiences, and countries of origin this work may not be generalizable to refugee populations resettled in other parts of the country or the world, as access to cognitive healthcare and dementia education may vary. It is important to understand that qualitative research does not seek to be generalizable, often starting as a way to reflect the perspectives and needs of a community and serve as a springboard to further work. 55 This study captures the perspectives of refugees alone – future work is needed to assess the perspectives and experiences of other people in this care pathway, from immigration workers, to medical providers, to community leaders and sponsors. Additionally, further research is necessary to quantify refugees’ cognitive health outcomes as it relates to various exposures and risk factors they face on their migration journeys.
Conclusion
Our study examines perceptions and attitudes towards dementia in a diverse refugee population resettled in the US. Based on our findings, we suggest four areas of intervention to improve this marginalized patient population’s experience with cognitive healthcare and ensure equitable pathways to healthy aging. We call for expansions in workforce capacity, projects to strengthen community resilience, future research on dementia risk factors in migrant groups, and implementation of justice-driven immigration and healthcare policies.
Supplemental Material
Supplemental Material - Attitudes Towards Dementia Among a Diverse Group of Refugees Resettled in the United States
Supplemental Material for Attitudes Towards Dementia Among a Diverse Group of Refugees Resettled in the United States by Dahlia A. Kaki, Lana Bridi, Purity Mwendwa, PhD, Maryam Aso, Rawnaq Behnam, Nissma Bencheikh, Behnan Albahsahli, MPH, Xara Khan, Raghad Aljenabi, Alissa Bernstein Sideman, PhD, MPH, Alison Moore, MD, MPH, Tala Al-Rousan, MD, MPH in Journal of Geriatric Psychiatry and Neurology.
Footnotes
Acknowledgments
First and foremost, we would like to thank our participants for their time, trust, and perspectives. We are grateful to the various staff members and administrative leadership at Family Health Centers of San Diego, the Majdal Community Center, the Afghan Community Culture Center, and the Somali Family Services in El Cajon, San Diego for providing in-kind support for the development of study procedures, onboarding of study staff, participant recruitment, and participant interface. Lastly, we would like to thank the Displacement and Health Research Lab members for their assistance with data collection, interview transcription and translation, and feedback throughout the research process and manuscript preparation.
Author Contributions
All authors made substantial contribution to the concept and design of the study, data acquisition and analysis, and manuscript drafting and preparation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was made possible by funding from the National Heart, Lung, and Blood Institute Grant #K23HL148530 (recipient: Tala Al-Rousan), the National Institute on Aging T35 Grant #AG26757 (recipient: Dahlia A. Kaki) and #K01AG059840 (recipient: Alissa Bernstein Sideman), and the San Diego Resource Center for Advancing Alzheimer’s Research in Minority Seniors Grant #P30AG059299 (recipient: Alison Moore). Funders had no involvement in study design, data collection, analysis or interpretation, or writing of the report.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.