
Abstract
Objective
To extend prior research by examining daily driving frequency as a predictor of cognitive decline and later diagnosis of Alzheimer’s disease.
Methods
1,426 older adults completed batteries of questionnaires and neuropsychological tests at baseline and yearly follow-ups (M = 6.8, SD = 4.9). Linear mixed effects models were estimated to examine whether daily driving frequency at baseline was predictive of cognitive decline while accounting for IADLs, mobility, depression, and demographics. Cox regression was used to examine driving frequency as a predictor of Alzheimer’s disease diagnosis.
Results
Less daily driving frequency was associated with greater decline in all cognitive domains over time except for working memory. Although driving frequency was associated with these changes in cognition, it did not uniquely predict the development of Alzheimer’s disease when accounting for other factors (eg, other IADLs).
Conclusions
Our findings extend prior research linking driving cessation to greater levels of cognitive decline. Future work might benefit from examining the utility of driving habits (especially changes in driving) as measures of everyday functioning in older adult evaluations.
Introduction
Although much research has focused on cognitive functioning as a predictor of everyday functioning (including driving) in older adults,1-4 increasing evidence suggests there may be utility in measuring everyday functioning as a predictor of cognitive decline and dementia. One longitudinal study found that reported early limitations in everyday functioning especially in instrumental activities of daily living (IADLs) (eg, medication and financial management) was significantly associated with cognitive decline and conversion from normal cognitive ability to MCI.5,6 Moreover, other findings comparing the trajectories of IADLs and objective cognitive decline across tests of reasoning, memory, and processing speed found that declines in functioning preceded cognition. 7 One factor believed to explain why everyday functioning can preceed cognitive decline refers to sensitivity of neuropsychological tasks as they may not be able to detect the subtle, earlier changes in cognition seen in older adults (eg, executive functions).6,7
Driving is an everyday task known to utilize cognitive functioning including executive functions (EF), attention, processing speed, memory, and visual perception. 8 However, EF and visual attention/processing, often measured via the Trail Making Test (TMT), Wisconsin Card Sorting Test (WCST), and Useful Field of View Test (UFOV), have shown the most robust associations with driving and account for age-related changes in cognition.9-11 However, more research is needed as no battery of neuropsychological assessments alone can determine whether an individual is fit to drive. 9 Another approach to identifying cognitive domains utilized in driving has focused on changes in driving habits as a result of diminished capacity to drive. Of which, both cessation (ie, the decision to stop driving) and restriction (ie, avoidance of challenging driving conditions) have shown associations with worse EF in normal and pathological (ie, mild cognitive impairment (MCI), dementia) aging trajectories.12-17 Moreover, research using global positioning system (GPS) tracking in vehicles has demonstrated the utility of naturalistic driving behavior metrics (eg, driving at night, acceleration, length of trips) to predict Alzheimer’s disease. 18
Though research has started to examine subtle changes in everyday functioning as early signs of MCI and dementia,5-7 these findings have not been extended to driving specifically. Despite driving being an IADL that also significantly utilizes cognitive abilities that often decline earlier (eg, executive functioning),19,20 to our knowledge only one study has examined it as a predictor of cognitive decline. Choi and colleagues found that driving cessation was associated with greater rates of cognitive decline. 21 However, that study only included an assessment of global cognitive functioning administered over the phone (Telephone Interview for Cognitive Status (TICS)), 22 which limit the generalizability of their findings. Driving has also shown associations with other functional variables (eg, life space mobility) and mental health factors (eg, depression) that have been found to significantly predict cognitive decline and dementia diagnosis.23-26 Moreover, examining more subtle variations in driving habits such as daily driving frequency as opposed to driving cessation may yield insight into earlier changes in everyday functioning and subsequent cognitive decline given that driving frequency is expected to change before the decision to stop. 14 Such evidence may contribute to an important goal of neuropsychologists to identify individuals who are at risk for cognitive and functional decline that is characteristic of dementia (eg, Alzheimer’s disease) as early as possible to maximize treatment opportunities that target modifiable risk factors and compensatory strategy use.27-29
The current study aimed to replicate and extend prior research findings connecting driving cessation to greater rates of objective cognitive decline by investigating other, more subtle variations in driving habits (ie, daily driving frequency) in relation to changes in cognitive functioning over time and dementia risk (ie, Alzheimer’s disease) in older adults. Specifically, the current analysis aimed to extend prior research via measuring cognitive functioning in a more comprehensive manner (including specific domains) using in-person administered batteries of neuropsychological assessments while accounting for depression, life space, and demographic variables associated with cognition.23,30,31 It was hypothesized that greater driving frequency (ie, number of days typically driven per week at baseline) will predict reduced rates of objective cognitive decline globally and in specific domains.
Materials and Methods
Participants
The current study included a subset of data from a larger longitudinal dataset collected via the Rush University Memory and Aging Project (MAP), an ongoing cohort study since 1997 examining healthy middle-aged and older adults at baseline in relation to trajectories of cognitive and functional decline, risk of dementia, and other factors. 32 MAP obtained written informed consent from each subject and included individuals with no known diagnosis of dementia at baseline and who were able to sign an Anatomical Gift Act at baseline. 33 The Rush Alzheimer’s Disease Center (RADC) and the institutional review board at the Louisiana State University Office of Research & Economic Development (IRB: IRBAM-20-0799) approved our use of the MAP dataset for research purposes. MAP recruited participants from retirement communities and subsidized housing facilities in eastern Illinois and throughout the Chicago metropolitan area. 34 In the current study, 1,426 individuals over the age of 50 who were licensed to drive, had driven in the past year, and completed a self-reported item on daily driving frequency at baseline were included. The current sample was included from a larger sample of 2082 individuals where 583 and 73 individuals were removed due to not having a driver’s license and not being a current driver (ie, has not driven in the past 12 months), respectively. Alzheimer’s disease diagnoses included as part of MAP were made according to National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer’s Disease and Related Disorders Association (NINCDS/ADRDA) criteria. 33 This included the interpretation of neurocognitive testing and clinical judgment made by a clinician (eg, neuropsychologist, neurologist, etc.). 33 Moreover the variable used in the current study only included Alzheimer’s disease diagnosis which did not include other forms of dementia.
Measures
Driving Frequency
Each participant completed a measure of self-reported daily driving frequency as per Shah et al. 35 Individuals indicated how many days per week they typically drive via endorsing one of 4 options: (1) 6 or 7 days, (2) 3 to 5 days, (3) 1 to 2 days, (4) less than once. Thus, larger scores indicated less driving frequency. This variable was only assessed at baseline.
Life Space
A modified Life Space Questionnaire (LSQ) was included to assess the extent to which individuals move spatially throughout their environment. 36 At baseline and each follow-up visit, participants indicated via “yes” or “no” the extent of their movement within 6 specific zones in the past week including (1) other rooms within your house or apartment, (2) immediately outside areas (eg, patio, deck, garage, or hallway), (3) areas outside the house or apartment (eg, a driveway, parking lot, yard, or courtyard), (4) within the neighborhood (5) immediately outside the neighborhood, (6) outside of the neighborhood, and (7) places outside of community/town. Life space scores were calculated by summing scores of each item (yes = 1, no = 0), so that larger scores indicate greater life space or movement.
Instrumental Activities of Daily Living
A modified measure of IADLs from the Duke Older Americans Resources and Services project was used in the current study. 37 Participants rated the extent to which they independently complete multiple activities (ie, (1) “No Help,” (2) “Help,” or (3) “Unable to do”) across 8 items including making meals, using the phone, housekeeping tasks, managing medications, paying bills, traveling within their community, and shopping. A composite score was made via summing the scores of all items where higher scores meant less independence in IADLs.
Depression
A modified, 10-item Center for Epidemiologic Studies Depression scale (CES-D) was used to measure the number of depression symptoms experienced. 38 Specifically, participants responded “yes” or “no” individually to a list of depression symptoms (eg, “I felt lonely,” “I felt depressed,” “I enjoyed life,” “I felt sad”) as whether they experienced each symptom much of the time in the last week. Scores for this measure were calculated by summing the scores of all items where a higher score indicated more depression symptoms.
Demographics
Sex and ethnicity were rated using a binary scale where participants had the option to select between female or male and Hispanic or Non-Hispanic, respectively, which were treated as categorical variables in the current analysis. Age at baseline, years of education, and study follow-up year were treated as continuous variables for analysis purposes. Participants were asked to indicate their race based on the following options: “White,” “Black or African American,” “American Indian or Alaska Native,” “Native Hawaiian or Caucasian,” “Asian,” “Other,” or “Unknown,” which were coded categorically. However, given the low number of individuals outside of White and Black or African American groups (ie, <20 participants), all groups besides White were combined into one category for analysis purposes. Consistent with prior research, 39 socioeconomic status (SES) was measured via 2 items asking participants to rank their current standing compared to (1) “all other people in the United States” and (2) “others in [their] community” in terms of education, money, and occupation. Each of the 2 items were presented to the participant as a 10-rung ladder where the highest runs represented those who are best off and the lowest represented those who were the worst off. As such, participants marked an “X” on the rung of the latter that best reflected their personal SES. The scores of the items were summed to create a composite score where higher scores meant higher SES.
Neuropsychological Assessments
Scores from neuropsychological tests were included to measure objective cognitive function in multiple domains consistent with a factor structure supported by prior research. 40 Episodic memory was measured via tasks including immediate and delayed recall trials from both Logical Memory (Story A) 41 and East Boston Story tests,31,42 Word List, Word List Memory, Word List Recognition, and Word List Recall. 43 Semantic memory was measured via tasks including Verbal Fluency,31,43 Boston Naming Test (15-item), 43 word reading test (15-item). 31 Measures of processing speed included Symbol Digit Modalities Test (SDMT), 44 Number Comparison,31,45 Stroop word reading and color naming. 46 Assessments of working memory included digit Span (forward, backward, and ordering).31,41,47 Measures of perceptual orientation consisted of Judgement of Line Orientation - 15 item (JOLO) and Standard Progressive Matrices.48,49 Averaged z-scores were used in analysis for each cognitive domain assessed as per prior research. 40 Global cognitive ability was calculated via the average of all tests. 40
Procedure
Individuals enrolled in MAP took part in responding to a series of questionnaires including demographics (eg, age, race, ethnicity, education, SES, etc.), measures of daily functioning (eg, mobility, IADLs), psychopathology symptoms (eg, depression), driving habits (ie, daily driving frequency) and others as well as a comprehensive battery of neuropsychological assessments at baseline and at annual follow-ups. 34 Notably, there was no set maximum number of annual follow-ups as data collection is on-going. However, in the current dataset, only 6 people had more than 20 years of assessments. Research personnel conducted all study sessions at the participants’ homes to avoid exclusively recruiting “healthy volunteers.” 34
Analyses
Separate mixed effects models (ie, for global cognition and each cognitive domain) were used to examine whether daily driving frequency significantly predicts cognitive decline while accounting for covariates and demographics. The first set of models included demographics (ie, sex, race, ethnicity, level of education, SES) as fixed effects predictors of cognitive decline along with time (ie, follow-up year) while the second set of models included the same predictors with the addition of life space, IADLs, and depression symptoms. All models included the interaction of driving frequency with time. A random intercept for participant and random slope for time were used to capture variability in baseline performance and rates of cognitive decline. The interaction of time by daily driving frequency was used to evaluate whether the effect of time on cognitive functioning depends on daily driving frequency.
Multivariate cox regression was used to examine the relationship between Alzheimer’s disease risk and daily driving frequency, which included covariates (ie, life space, IADLs, depressive symptoms, sex, race, ethnicity, level of education, SES) and a time-updated structure. The survival time variable was calculated based upon years to Alzheimer’s diagnosis or their last year of study follow-up (if not diagnosed within the study timeline). The first cox regression conducted included only demographics as covariates while the second accounted for demographics, IADLs, depression, and life space.
Results
Sample Characteristics
Demographic Profile of Older Adult Sample (N = 1426).
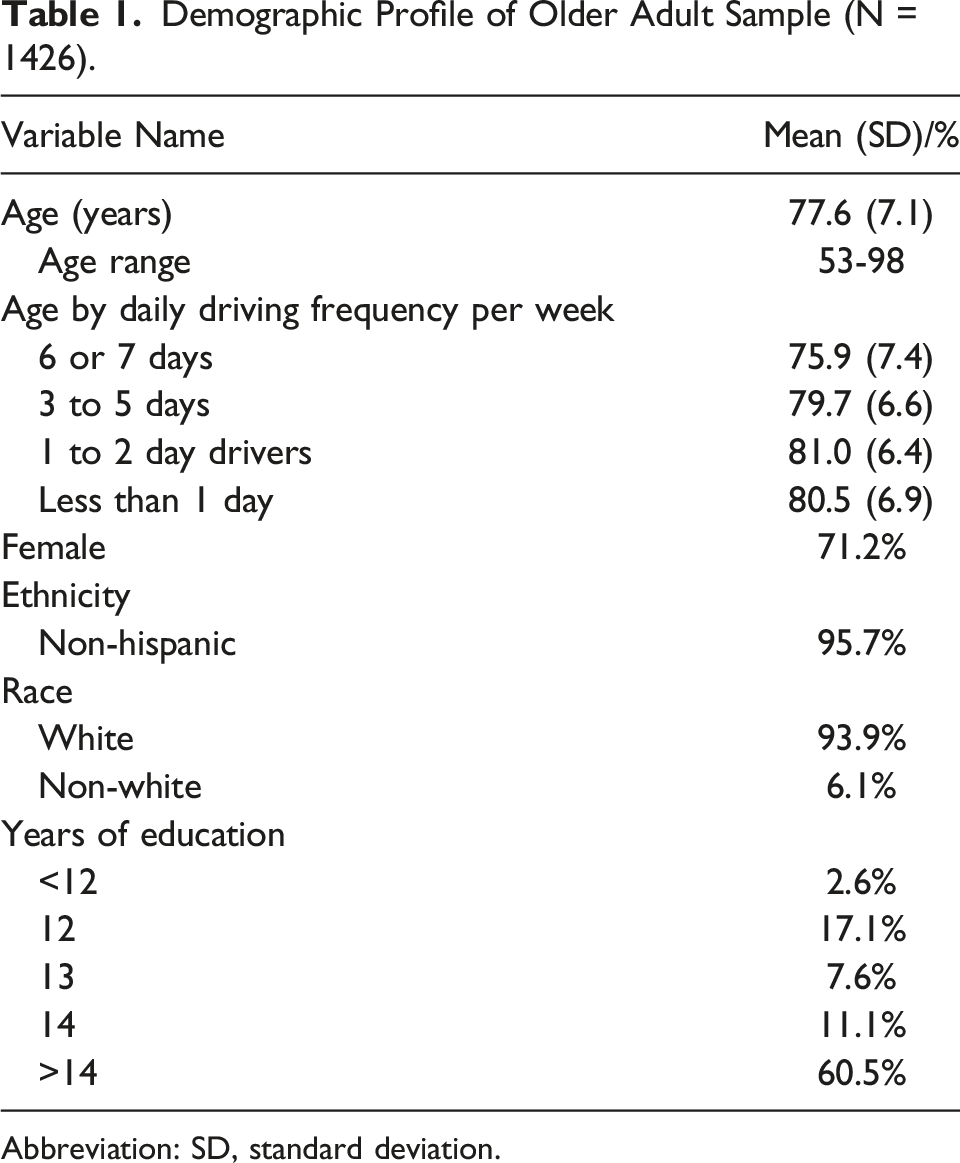
Abbreviation: SD, standard deviation.
Driving Frequency & Cognition
Spearman Coefficients Between Driving Frequency and Variables at Baseline.
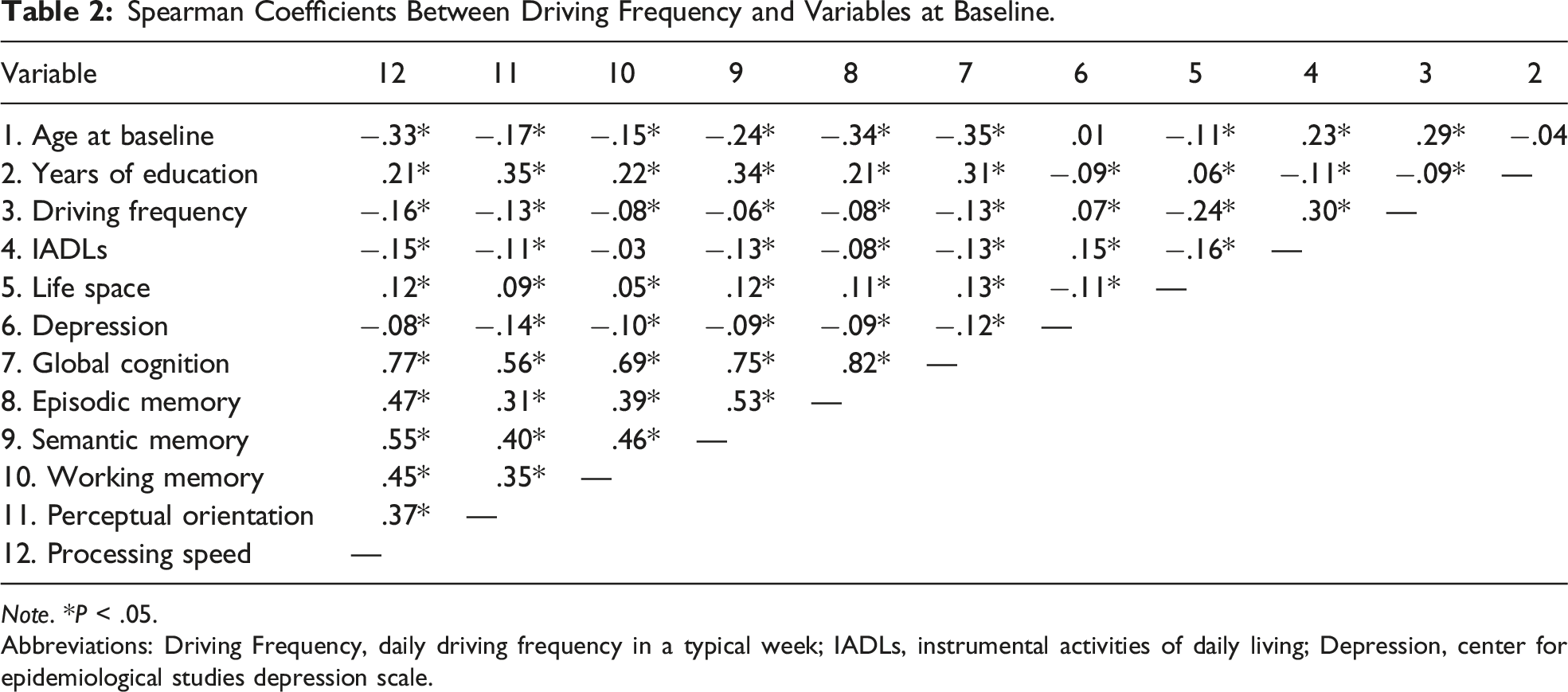
Note. *P < .05.
Abbreviations: Driving Frequency, daily driving frequency in a typical week; IADLs, instrumental activities of daily living; Depression, center for epidemiological studies depression scale.
Linear Mixed Effects Models of Driving Frequency and Time Predicting Cognition.
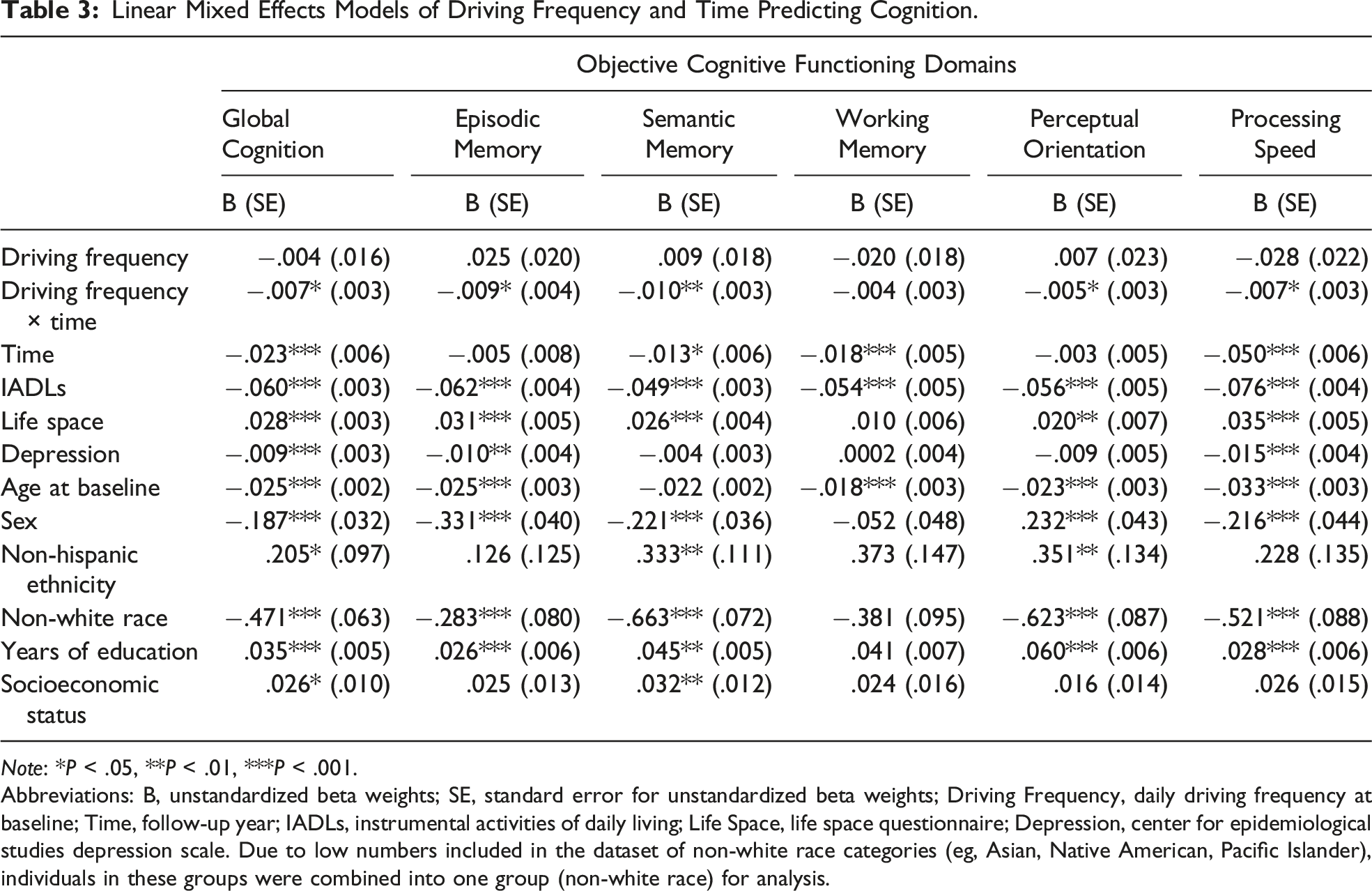
Note: *P < .05, **P < .01, ***P < .001.
Abbreviations: B, unstandardized beta weights; SE, standard error for unstandardized beta weights; Driving Frequency, daily driving frequency at baseline; Time, follow-up year; IADLs, instrumental activities of daily living; Life Space, life space questionnaire; Depression, center for epidemiological studies depression scale. Due to low numbers included in the dataset of non-white race categories (eg, Asian, Native American, Pacific Islander), individuals in these groups were combined into one group (non-white race) for analysis.
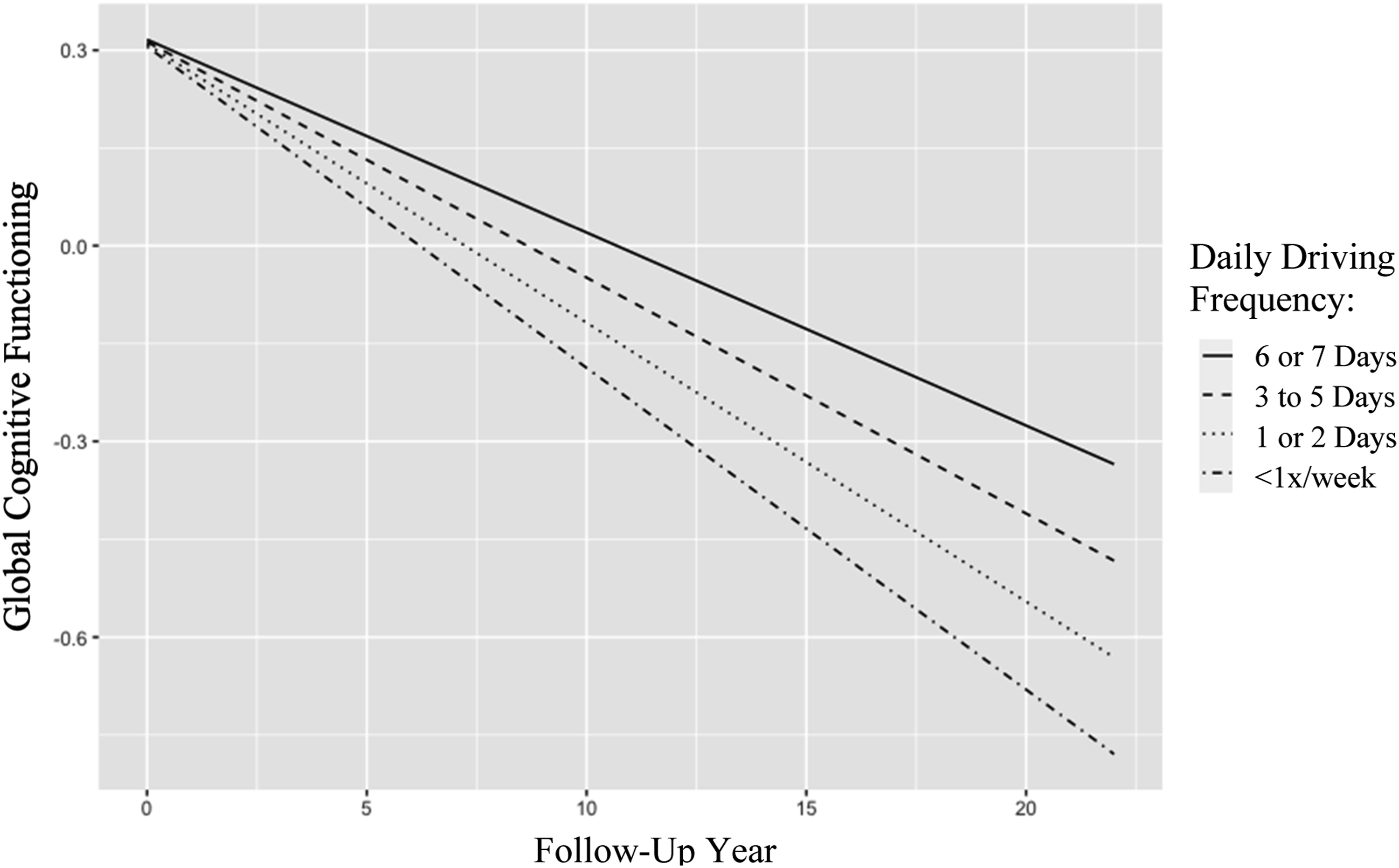
Daily driving frequency by follow-up year predicting global cognitive functioning. Note: Daily Driving Frequency, number of days typically driven per week at baseline; Follow-Up Year, year of follow-up assessment.
Post-hoc analyses were run to determine which between-subjects differences were driving the relationship between driving frequency and global cognitive decline. The driving frequency variable was dummy coded into 3 separate variables (ie, Less than 1 day, 1 or 2 days, and 3 to 5 days each coded as 1 vs. not (coded as 0)). Of which, all 3 variables and their interaction as well as IADLs, life space, depression, and demographics were in a mixed-effects model predicting global cognition over time. Among all driving variables and their interactions, results indicated only the interaction between driving 3 to 5 days per week and follow-up year was significant (F(3, 1422) = 8.215, P < .001). This suggests that subtle differences in driving frequency are driving associations with cognitive decline.
Driving Frequency & Alzheimer’s Disease Risk
One cox regression revealed that less daily driving frequency (as the only predictor) significantly predicted greater risk for Alzheimer’s disease (See Figure 2). Moreover, daily driving frequency had a hazard ratio of 1.21 (P = .004) which suggested that those who drove less, had a 21% greater risk for diagnosis. While accounting for IADLs, life space, depression, and demographics at baseline, daily driving frequency no longer significantly predicted risk for Alzheimer’s disease (hazard ratio = .93, P = .547). Within this model, age at baseline (hazard ratio = 1.06, P = .001) and IADLs (hazard ratio = 1.38, P < .001) were the only significant predictors of risk for Alzheimer’s disease. Survival probability of daily driving frequency by follow-up year predicting diagnosis of Alzheimer’s disease. Note: Daily Driving Frequency, number of days typically driven per week at baseline; Follow-Up Year, year of follow-up assessment.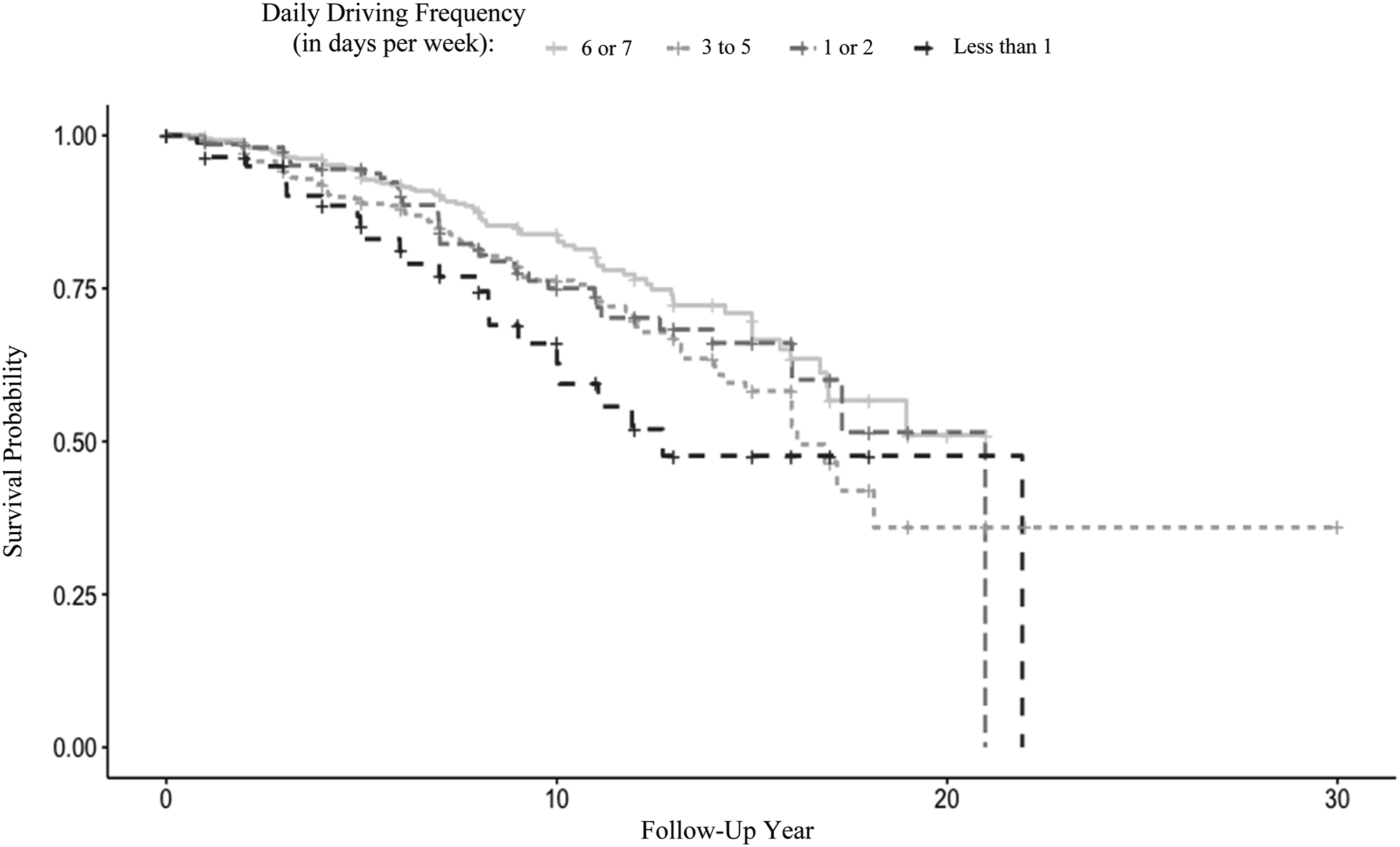
Discussion
The current study aimed to replicate and extend prior research findings connecting driving cessation to greater rates of objective cognitive decline by investigating other driving habits (ie, daily driving frequency) in relation to changes in cognitive functioning over time in older adults while accounting for other variables linked to cognitive decline such as IADLs, depression, mobility (ie, life space), and demographic variables. Consistent with prior research that suggests driving utilizes a wide variety of cognitive abilities, 8 the current study found that driving frequency was associated with greater cognitive decline globally and across most specific domains.
Although research on driving and cognition has largely focused on neuropsychological measures as predictors of driving performance and behavior, it is possible that variations in driving habits along with other everyday functioning tasks (eg, managing finances) may precede detectable changes in cognitive functioning on neuropsychological measures.5,7,50 Our findings extend those from Choi and colleagues 21 that connect driving cessation to greater rates of global cognitive decline over time by demonstrating that daily driving frequency was associated with cognitive decline globally and across specific domains (ie, processing speed, perceptual orientation, episodic memory, semantic memory). Findings from the current study also bolster the literature connecting driving habits to cognitive decline given that specific, factor analysis-derived domains of cognitive functioning were assessed via commonly-used neuropsychological tests.34,51,52
The current study provides further evidence to suggest driving habits predict cognitive decline. As opposed to driving habits that occur later in time (ie, cessation), our results suggest cognitive functioning and declines in cognition may be influenced by more subtle variations in driving that occur earlier in time such as daily driving frequency. 14 It was notable that follow-up analyses revealed baseline differences between driving 6 or 7 and 3 to 5 days per week explained most of the association between driving frequency and cognitive decline. We also found that the overall results for driving frequency predicting cognitive decline remained significant even when analyses were limited to those with at least average levels of cognition at baseline (−.5 SD or higher) which suggests baseline cognition does not fully explain this relationship. 53 This finding adds to the evidence that suggests daily driving frequency may be an earlier indicator of cognitive decline and may contribute to broader efforts in neuropsychology to identify earlier behavioral markers of decline.27-29 As such, future research should seek to investigate other between-subjects (eg, miles driven, restrictions/avoidance of driving situations/conditions) and within-subjects variations (or changes) in driving habits over time in relation to normal and pathological levels of cognitive and functional decline.
The current study also found that individuals who drove less days per week were more likely to develop Alzheimer’s disease when driving was the only predictor, which suggest driving habits may have some utility for predicting dementia onset. However, driving frequency was no longer predictive when accounting for IADLs, life space, and depression, which may be explained by stronger associations between these variables and driving frequency shown in prior research.35,54 Notably, the authors were not able to identify any research examining whether driving cessation (or any other driving habit) predicts incidence of MCI or dementia diagnoses. Future research should explore the utility of driving habits as quick-to-assess and cost-effective predictors of cognitive decline and risk for Alzheimer’s disease.
Our findings also add to broader literatures that connect indicators of worse functional mobility (eg, life space), subjective mental health (eg, depression), and less access to resources (ie, SES, level of education) to greater rates of cognitive decline over time.23,30,31,39,55 When accounting for some of these factors (ie, IADLs, depression, life space, age, SES, years of education), driving frequency still significantly predicted cognitive decline across most domains over time. Notably, there may be some practical benefits to measuring driving habits given they can be assessed quickly and in a straightforward manner (eg, Were you ever licensed to drive? When did you stop driving? How many days do you typically drive per week?). Given these advantages and the unique associations observed with cognitive decline, driving habits may be particularly poised for use in future research; especially longitudinal studies with greatly limited time and space for questionnaire items.
It is important to note the limitations of the current study. Despite the benefits of measuring constructs (eg, driving habits) via minimal numbers of items, the current study only included one item on daily driving frequency in the current analysis, which may increase risk for measurement error. Moreover, daily driving frequency was the only driving habit included in the current study. Future research should work to incorporate different driving habits such as avoidance (eg, nighttime driving) especially since this variable has been associated with worse cognition. 13 Daily driving frequency was also only measured at baseline in this study. Given that no known studies on driving habits as predictors of cognitive decline measure this construct at follow-up intervals, future research assessing changes in these variables in relation to changes in cognitive ability over time may also be useful. Additionally, future work on driving habits might include more objective measures of driving behavior such as GPS to track real-world behavior. 18 However, future research on the utility of self-reported driving habits is still needed given the lack of reliability and validity in this area. Moreover, self-reported driving habits may provide a useful alternative when GPS data is not available and may cost significantly less to evaluate. Although the current study adjusted for race, ethnicity, and SES, our sample had low variability in these parameters, which limits the generalizability of our findings to other populations.
The current study sought to extend prior research on driving cessation as a predictor of cognitive decline by examining another driving habit (ie, daily driving frequency) in relation to decline. Results showed that less daily driving frequency was uniquely associated with greater objective cognitive decline globally and in specific domains. These findings add further support for the utility in measuring driving habits as potentially early predictors of future cognitive and functional decline. Future research should examine other between and within-subjects variations in driving habits in relation to decline in older adults.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.