
Abstract
This study aimed to develop a questionnaire for evaluating total sedentary time (ST) and ST with cognitive activity, and to examine the association between ST and cognitive function among Japanese older adults. The questionnaire to evaluate ST comprised 12 items regarding behavior in specific settings, including 8 items on ST with cognitive activity, in a usual week. Older adults aged ≥75 years who participated in a health check-up assessing cognitive function completed the developed questionnaire and subsequently wore an accelerometer and recorded a diary of ST with cognitive activity for a week as validity measures. Cognitive function was assessed with neuropsychological tests covering 4 domains: memory, attention, executive function, and processing speed. Fifty-two participants were included in the validity analysis. Spearman’s correlation coefficient indicated fair-to-good agreement between the questionnaire-measured and the diary-measured time for ST with cognitive activity (r = 0.59, p < 0.001), but this was not the case for total ST. Bland-Altman plots showed that the questionnaire-measured total ST contained proportional bias (r = 0.51, p < 0.001). Multiple regression analysis (n = 49) showed longer questionnaire-measured ST with cognitive activity was significantly associated with better neuropsychological test scores (attention: β = -0.38, p = 0.025; executive function: β = -0.46, p = 0.003; and processing speed: β = 0.31, p = 0.041), while total ST was not associated with better cognitive performance. The developed questionnaire showed acceptable validity to measure ST with cognitive activity, which was found to be protectively associated with cognitive function.
Background
Sedentary behavior is to be avoided by older adults according to increasing evidence on its association with adverse geriatric-relevant health outcomes. 1 Although most research has found that excessive sedentary time (ST) is associated with adverse health outcomes, 2 some cohort studies reported a protective effect of sedentary behavior in specific settings on certain outcomes, especially mental health aspects such as cognitive function.3-7 Recently, it has been suggested that sedentary behavior needs to be classified and reconsidered in detail by type (e.g., computer use [cognitively active] vs. watching TV [passive]). 1 In turn, evaluating not only total sedentary time (ST) but ST in specific settings can help to clarify its influence on older adults’ health.
Sedentary behavior such as reading, using computers, or doing crosswords were found to be protective factors for cognition.3,4,7 These activities are cognitively demanding and can therefore be considered as “cognitive activity”.8,9 A variety of cognitive activities usually performed in a sitting position were reported to be protective factors for cognitive function. 6 However, these previous studies assessed cognitive activity using a few items or categorical variables of activity frequency; thus, the association between detailed ST with cognitive activity and cognitive function have not been examined. Sedentary older adults who engage in sedentary activities with cognitive activity for long periods may be more likely to retain their cognitive function. To obtain more clear evidence, a questionnaire assessment of detailed ST with cognitive activity is therefore needed.
Some questionnaires have been developed to evaluate sedentary behavior among older adults in specific settings, and a few items regarding ST with cognitive activity were used.10-14 Although these questionnaires included reading or using a computer, they referred to “hobbies” or “other sedentary” activities and did not cover other cognitive activities such as playing board games, doing crossword puzzles, or playing sudoku.10-14 Given that more concrete and multiple items were found to improve the accuracy of measurement of ST with cognitive activity by self-report questionnaire, ST with cognitive activity should be assessed using more detailed items.12,15 Therefore, the present study aimed to develop and validate a questionnaire for evaluating ST with cognitive activity as well as total ST, and to explore the association of its measurements with cognitive function among Japanese older adults.
Materials and Methods
Procedure and Participants
Data collection was conducted as part of a health check-up for older adults aged 75 years or older in Obu city, Japan. In the briefing meeting about the results of their health check-ups, older adults were recruited as participants for this study. All participants provided informed consent before participation. This study was conducted in accordance with the guidelines proposed in the Declaration of Helsinki, and the study protocol was reviewed and approved by the research ethics committee of the National Center for Geriatrics and Gerontology.
Cognitive function was assessed at the health check-up, and other evaluations were conducted during the 2 months after the health check-up. After the health check-up, participants were asked to wear an accelerometer and record a diary of ST with cognitive activity for a week beginning the next day. At the end of the week, participants mailed the accelerometer and diary to our institution. To encourage participants’ response, we offered a 2,000 JPY (19 US D) voucher card to those who completed the survey. Among the 106 individuals who received the explanation about the study, 72 completed data collection.
Measures
Questionnaire
The developed questionnaire for older adults assessed total ST and ST with cognitive activity per day. The questionnaire comprised 12 items regarding sedentary behavior in specific settings, including 8 items on ST with cognitive activity, in a usual week (Supplementary file). Based on the recommended procedure, 16 the original Japanese questionnaire was translated into English for future research through forward translation, back translation, and back translation review by a specialized translation agency (Ulatus, Crimson Interactive Pvt. Ltd.).
The 12 items regarding sedentary behavior in specific settings and validity measures of total ST and ST with cognitive activity are summarized in Table 1. These items were selected based on a review of other questionnaires.10-14 Items (3) to (6) and (8) for ST with cognitive activity in Table 1 referred to activities with relatively high cognitive demand among 23 everyday activities according to the rankings of cognitive psychologists. 17 In addition to these activities, we added “driving a car,” “paid or nonpaid work,” and “using a computer or smartphone” to the items on ST with cognitive activity, as those who engage in these activities have high cognitive function.18-20
Items in the Developed Questionnaire and the Validity Measure.
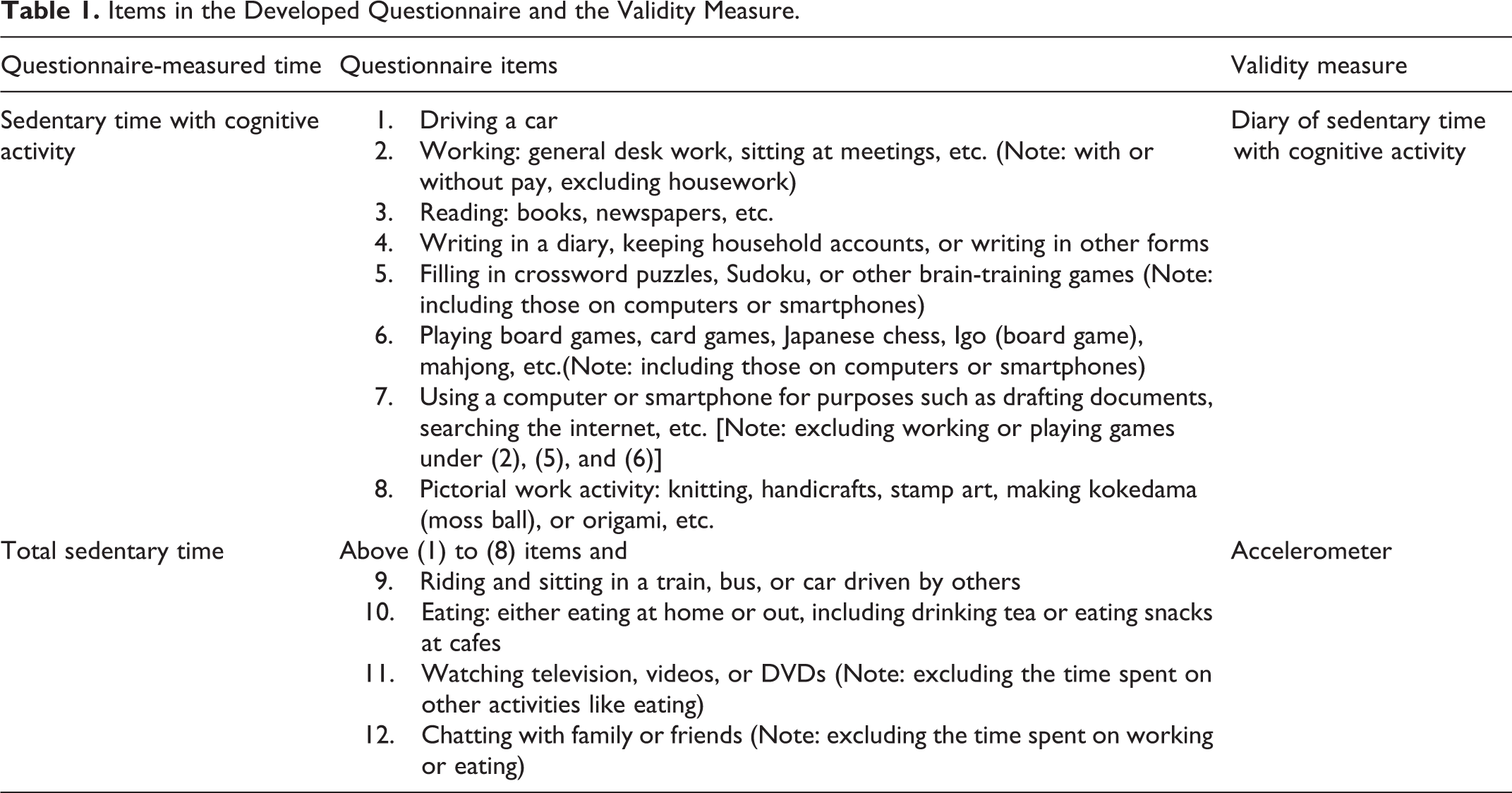
Participants were asked, “When thinking about a typical week (7 days) and not including special situations, such as traveling for fun or being hospitalized, how often do you perform the following activities while sitting or lying down? For each activity, please respond with the number of days per week and the approximate duration per day you perform the activity.” Although other questionnaires ask participants to report the ST over the past 7 days,10,12 we asked for the time in a habitual week to exclude unusual events such as trips or hospitalizations. We did not separate weekdays and weekends because another cohort study we conducted showed that most older adults were not employed 6 ; therefore, we assumed there were no obvious differences in their activity pattern between weekdays and weekends. After drafting the questionnaire, we confirmed the ease of respondence by asking a convenience sample of 21 older adults in a health class to complete the questionnaire. The original questionnaire item, “Do nothing in particular,” was found to be difficult to answer; thus, we excluded it from the final questionnaire.
Referring to the data cleaning rules for the International Physical Activity Questionnaire (IPAQ), those who reported >960 min of total ST were identified as over-reporting, based on the assumption that individuals spend an average of 8 hours per day sleeping. 21 In order to confirm the test-retest reliability of the developed questionnaire, we asked individuals in a research institution (n = 26; mean age, 39.5 ± 7.9 years; women, n = 17; education, 18.0 ± 3.1 years) to respond to the questionnaire across a two-day interval. The test-retest reliability was evaluated using single-measure intraclass correlation coefficients [ICC (1, 1)] and 95% confidence intervals (CI), and those who reported >960 min of total ST were not excluded, to enable us to examine if participants provided similar responses to the first and second questionnaire. ICC showed excellent agreement for total ST [ICC (95%CI) = 0.96 (0.90–0.98)] and ST with cognitive activity [ICC (95%CI) = 0.99 (0.98–0.995)].
Accelerometer
The validity of questionnaire-measured total ST was confirmed by comparison with data from an accelerometer using a tri-axial monitor, Active style Pro HJA350-IT (ASP; Omron Healthcare, Kyoto, Japan). The use of the ASP for identifying sedentary behavior was validated using the Douglas Bag method in a controlled laboratory setting22,23 and activPAL with a built-in inclinometer in a free-living setting. 24 The ASP measures sedentary behavior as ≤1.5 metabolic equivalents 25 in 60-sec epochs. Participants were instructed to wear the accelerometer on the right or left side of the waist during waking hours and to remove it during sleeping and water-based activities (e.g., bathing or swimming). Non-wear time was set at intervals of ≥60 consecutive minutes of 0 metabolic equivalents (METs), with allowance for up to 2 min of observation of some limited movement (<1.0 METs) within these periods. 26 Valid data were defined as including wear time for at least 4 days and 10 or more hours per day. 27 In line with a previous study recommending 5 or more days of monitoring for predicting sedentary behavior in older adults, 28 all participants included in the analysis except for two had 5 or more days of data.
Diary of sedentary time with cognitive activity
A 7-day diary of ST with cognitive activity was used as the validity measure for questionnaire-measured ST with cognitive activity. The format of the diary was set to record the start and end time of participants’ engagement in each cognitive sedentary behavior [(1) to (8) items] during the week. The sum of the recorded time provided the daily ST with cognitive activity per day. All participants who completed the diary had 6 or more days of data and were thus included in the analysis.
Cognitive function
Cognitive function was assessed using the National Center for Geriatrics and Gerontology-Functional Assessment Tool (NCGG-FAT).29,30 Participants were accompanied by well-trained staff to ensure that the correct test protocols were followed. In the present study, cognitive impairment was assessed based on the following 4 cognitive domains: memory (word list memory-I [immediate recognition] and word list memory-II [delayed recall]), attention (an electronic tablet version of the Trail Making Test part A [TMT-A]), executive function (an electronic tablet version of the Trail Making Test part B [TMT-B]), and processing speed (an electronic tablet version of the Symbol Digit Substitution Task [SDST]). These tests have acceptable test-retest reliability and moderate-to-high correlations with scores of widely-used conventional neurocognitive tests among community-dwelling older adults. 29
Statistical Analysis
Data distribution was skewed for questionnaire-measured ST with cognitive activity (skewness = 1.26, kurtosis = 1.91, p for Shapiro-Wilk test < 0.001), while it was normal for questionnaire-measured total ST (skewness = 0.34, kurtosis = 1.14, p for Shapiro-Wilk test = 0.15). Although the Shapiro-Wilk test was significant at p < 0.01, the data distribution of the validity measures showed less skewness (accelerometer-measured total ST: skewness = 0.87, kurtosis = 1.03; diary-measured ST with cognitive activity: skewness = 0.67, kurtosis = -0.60). In the validity analysis, the difference and correlation between the questionnaire-measured time and the validity measure for ST with cognitive activity were examined using a non-parametric test (Wilcoxon’s test and Spearman’s correlation coefficients [ρ]), while those for total ST were examined using parametric tests (t-tests and Pearson’s correlation coefficients [r]). Bland-Altman plots of total ST and ST with cognitive activity were created to confirm systematic error between the questionnaire-measured time and validity measures. Fixed and proportional biases were examined using limits of agreement and Pearson’s correlation coefficients (r), respectively.
The associations between questionnaire-measured total ST, ST with cognitive activity, and cognitive function were examined using multiple regression analysis. The NCGG-FAT score was set as the dependent variable, and the questionnaire-measured total ST and ST with cognitive activity were set as independent variables. A transformation was used to improve the normality of the data distribution for ST with cognitive activity (log [ST with cognitive activity + 0.5]) (Yamamura, 1999). Although the total ST value contained ST with cognitive activity, multicollinearity was not considered because there was not a high correlation between total ST and transformed ST with cognitive activity (r = 0.49, p < 0.001) (Franke, 2010). The initial model was not adjusted (Model 1), and then adjusted for age, sex, and educational years (Model 2). All statistical analyses were performed using SPSS version 25 (IBM, New York City, NY, USA). The level of statistical significance was set at p < 0.05 for all analyses.
Results
Participant Characteristics
Among the 72 participants who completed data collection, those who reported >960 min of total ST (n = 13) and were missing data for the questionnaire-measured ST with cognitive activity (n = 7) were excluded, resulting in 52 participants (mean age, 78.3 ± 2.7 years; 46.2% female; 12.2 ± 2.2 education years) for the validity analysis of ST with cognitive activity. In addition, participants with missing data for the total ST validity measure, namely the accelerometer (n = 1), and questionnaire-measured total ST (n = 2) were excluded, leaving 49 participants for the validity analysis of total ST and the examination of the association between STs and cognitive function. No participants had dementia, but 10 out of 52 participants (19.2%) showed cognitive decline in one or more domains identified by test scores below 1.5 standard deviations of the age- and education-specific mean for healthy older adults in our cohort database (data not shown). Out of 52 participants, 51 demonstrated memory function over the age- and education-specific mean.
Validity of Developed Questionnaire
The validity measure had a median (25–75th percentile) of 482.7 min (430.2–585.0) for total ST and 186.2 min (96.1–294.0) for ST with cognitive activity. Both questionnaire-measured STs showed no significant differences in the Wilcoxon’s test when compared with their respective validity measures (total ST: z = -1.04, p = 0.299; ST with cognitive activity: z = -1.46, p = 0.145; Table 2). Spearman’s coefficient showed a fair-to-good correlation for ST with cognitive activity between the diary and questionnaire measures (p = 0.59, p < 0.001), but no correlation was found for total ST.
Differences and Correlation between Questionnaire-Measured Time and Validity Measure for Total Sedentary Time and Sedentary Time with Cognitive Activity.
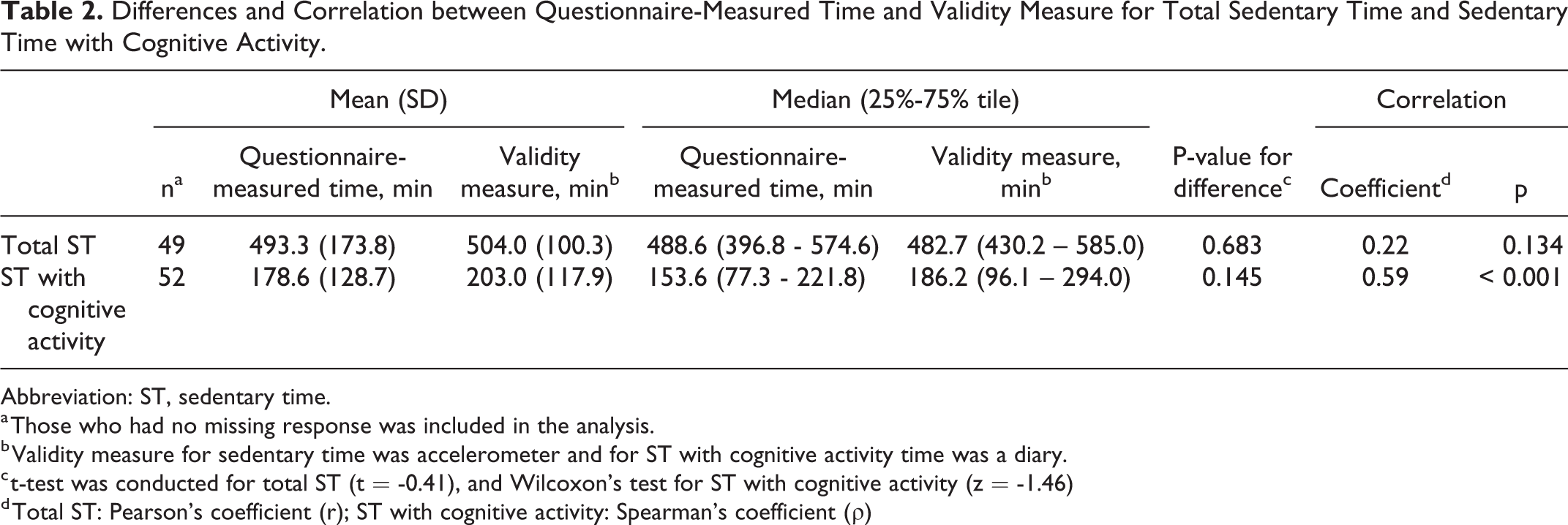
Abbreviation: ST, sedentary time.
a Those who had no missing response was included in the analysis.
b Validity measure for sedentary time was accelerometer and for ST with cognitive activity time was a diary.
c t-test was conducted for total ST (t = -0.41), and Wilcoxon’s test for ST with cognitive activity (z = -1.46)
d Total ST: Pearson’s coefficient (r); ST with cognitive activity: Spearman’s coefficient (ρ)
Bland-Altman plots are shown in Figure 1. The Bland-Altman plots of total ST show large positive correlations and proportional bias between accelerometer- and questionnaire-measured times (r = 0.51, p < 0.001) (Figure 1a). Participants with shorter total ST as measured by the accelerometer underreported their total ST on the questionnaire; conversely, those with longer total ST on the accelerator overreported their total ST. On the other hand, the plots of ST with cognitive activity showed no systematic error between diary- and questionnaire-measured times (Figure 1b). The limits of agreement (mean ± 1.96 standard deviations) were -364.9 to 343.7 min/day for total ST and -244.0 to 195.2 for ST with cognitive activity.
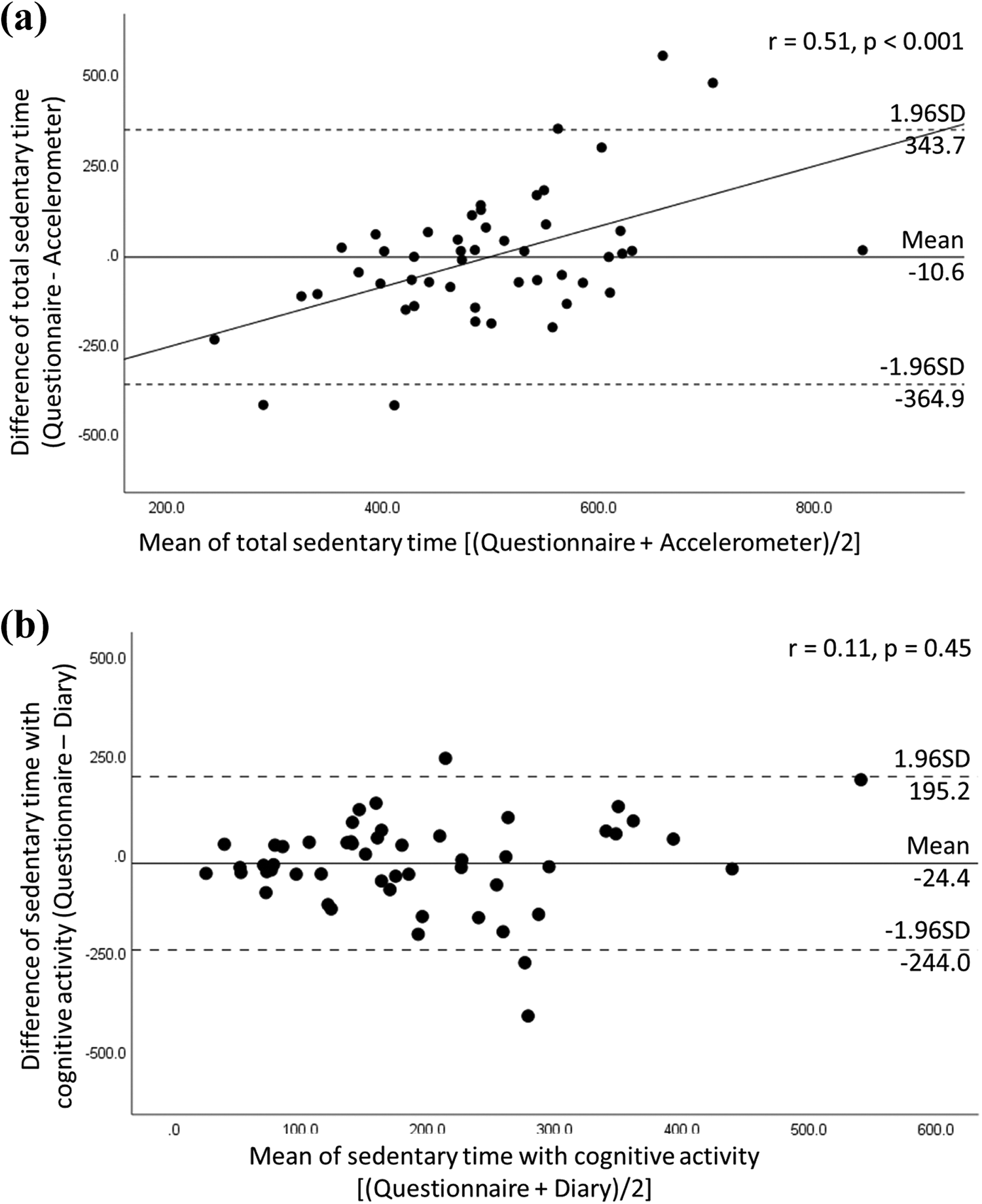
Bland-Altman plots of total sedentary time (a) and sedentary time with cognitive activity (b). Those who had no missing response and ≤960 min of sedentary time were included in the analysis [(a) n = 49; (b) n = 52].
Associations Between Questionnaire-Measured Time and Cognitive Function
The descriptive statistics for the questionnaire-measured time of the 49 participants and the multiple regression analyses for questionnaire-measured time and cognitive function test scores are summarized in Table 3 and Table 4, respectively. ST with cognitive activity was significantly associated with better test scores after adjustment for age, sex, and educational year (TMT-A time: β = -0.38, p = 0.025; TMT-B time: β = -0.46, p = 0.003; and SDST score: β = 0.31, p = 0.041), while total ST was not associated with any test scores.
Descriptive Statistics for Questionnaire-Measured Time Among Analyzable Sample (n = 49).a
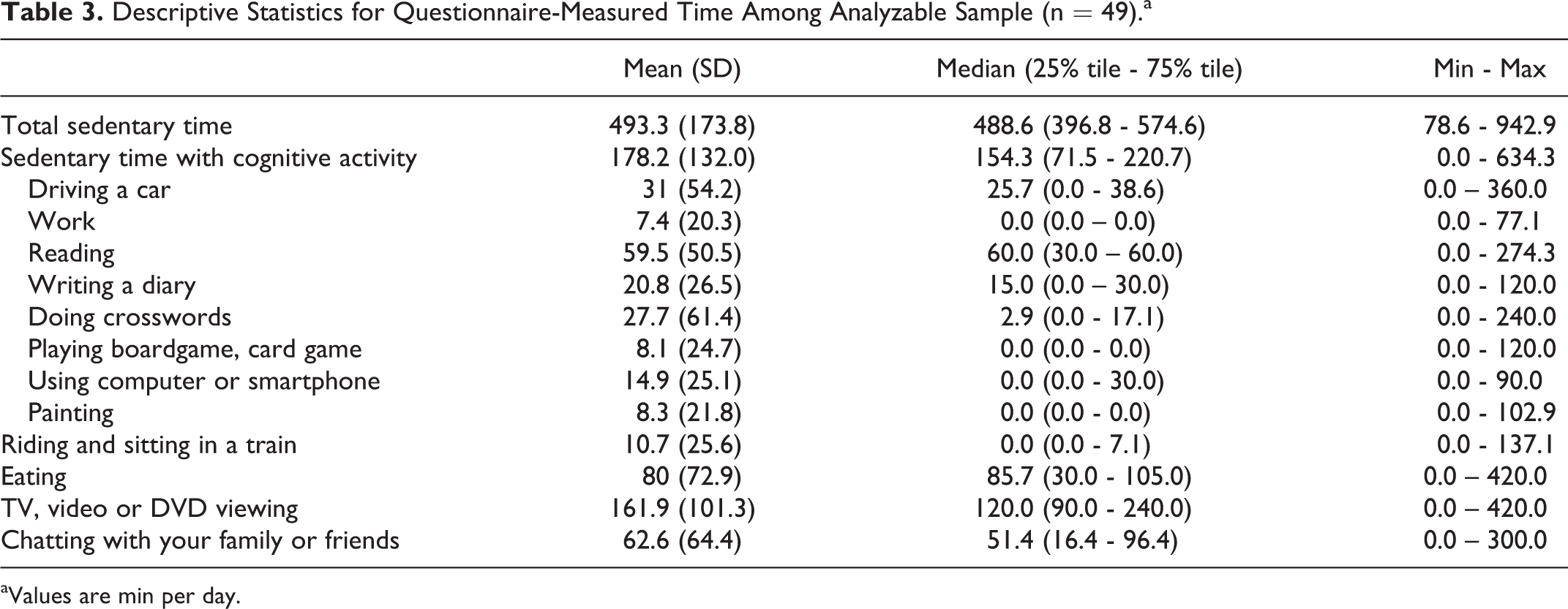
aValues are min per day.
Multiple Linear Regression Analyses on the Contribution of Total Sedentary Time and Sedentary Time with Cognitive Activity to Cognitive Function (n = 49).a
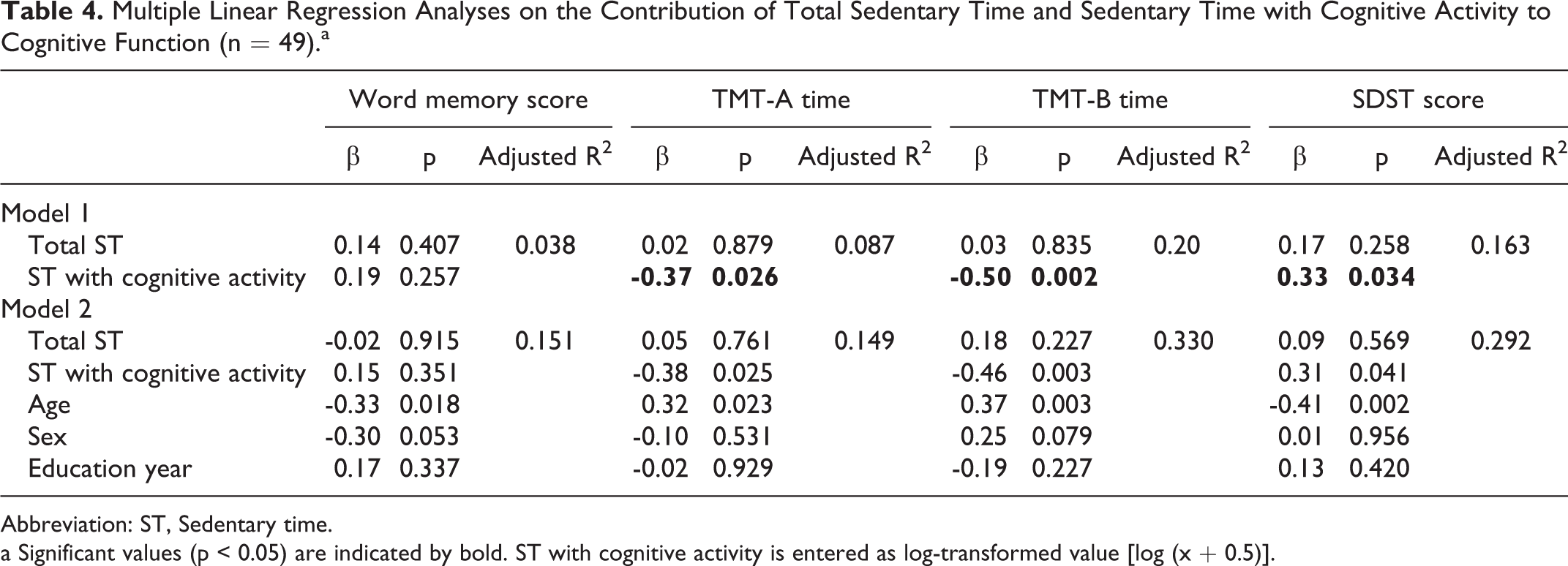
Abbreviation: ST, Sedentary time.
a Significant values (p < 0.05) are indicated by bold. ST with cognitive activity is entered as log-transformed value [log (x + 0.5)].
Discussion
The present study developed a questionnaire to evaluate total ST and ST with cognitive activity among older adults. We confirmed the validity of the questionnaire and the association of its measurements with cognitive function. Questionnaire and diary measures of ST with cognitive activity were correlated. Questionnaire-measured ST with cognitive activity was also associated with cognitive function, while questionnaire-measured total ST was not correlated with accelerometer-measured ST and included proportional bias and a wide range of the limits of agreement.
The results of the current study were similar to those of other studies on the validity of older adults’ total ST as measured by questionnaire and accelerometer.10-14 The wide range of the limits of agreement with proportional bias may have been caused by recall response, which suggests older adults who had low sedentary levels were likely to underestimate their total ST, while those who had high sedentary levels were inclined to overestimate it. On the other hand, the Bland-Altman plots showed that the questionnaire-measured total ST had small mean bias (-10.6 min/day) against the accelerometer-measured ST. In other questionnaires, a large mean bias was reported (-3.6 h/day to -81.9 min/day).10-14 One reason for the different results between the present study and other studies may be that we used a relatively large number of items in the developed questionnaire (12 items) compared to Clark et al. (2013) 31 (5 items) or Gardiner et al. (2011) 10 (7 items), which enabled a more detailed assessment of sedentary behavior and resulted in a more accurate evaluation of total ST. Another reason may be that Visser and Koster 13 and Van Cauwenberg et al. 12 used the ActiGragh GT3X as the validity measure for total ST. The ActiGragh GT3X is likely to overestimate ST against the ASP used in the present study and the activPAL3 inclinometer (mean difference was 63.7 to 89.3 min/day in working adults), 24 which caused large mean bias in other studies. Although it is difficult to evaluate total ST as a continuous variable using the developed questionnaire, further research may be able to rank total ST as a categorical variable (e.g., a tertile or quartile) using the questionnaire and analyze the association between total ST and various health outcomes.
Questionnaire-measured ST with cognitive activity had a significant moderate correlation and no systematic error against the validity measure, the diary of ST with cognitive activity. For older adults, ST with cognitive activity may be a specific activity and therefore easier to precisely recall. The limits of agreement of ST with cognitive activity showed a wide range, and some participants were beyond the mean bias ± 95% CI in the Bland-Altman plot, which may have contained the wrong answer (Figure 1b). Although participants responded to the questionnaire by themselves in this study, responding with the support of trained staff is desirable in order to decrease the likelihood of incorrect responses. These findings suggest that the developed questionnaire has acceptable validity for evaluating ST with cognitive activity.
Questionnaire-measured ST with cognitive activity was associated with cognitive function, while questionnaire-measured total ST was not. This finding regarding ST with cognitive activity is consistent with the findings of systematic reviews and meta-analyses that examined cognitive leisure activities and future risk of cognitive impairment. 9 Although questionnaire-measured ST with cognitive activity was not significantly associated with cognitive function in the memory domain, this may be caused by the fact that almost all participants had above-average memory score and vary according to the type of ST with cognitive activity, as other cohort studies reported late-life cognitive activity was associated with better memory performance.32,33 Future research could examine the association between sedentary behavior and cognitive function in detail using the developed questionnaire.
The main strength of the present study is that it is the first to develop a questionnaire to evaluate total ST and ST with cognitive activity. In addition, the detailed items of the questionnaire lead to higher validity for assessing total ST compare with other questionnaires for older adults.10,12,13,15 The main limitation is that the small non-random sample was limited to relatively healthy older adults who could participate in health check-ups, and there is a possibility that the validity of the questionnaire varies when used with other populations. In addition, there were many missing values and overreporting of sitting time per day. Furthermore, although we instructed participants to respond to the questionnaire by themselves, the respondents should be accompanied by trained staff when completing the questionnaire to obtain valid data. Moreover, the validity measure of ST with cognitive activity, namely the diary, was not an objective method. An ideal method would be using a wearable camera (e.g., SenseCam 34 ) to make a videorecording of participants’ activity, but we used a feasible method considering participants’ burden. Another limitation of the present study was not performing factor analyses on the questionnaire. Such a validation study would be an interesting direction for future research.
In conclusion, the present study involved the development a questionnaire to evaluate total ST and ST with cognitive activity among older adults. Our findings suggest that the questionnaire measure of ST with cognitive activity showed acceptable validity and had an association with cognitive function, while the measure of total ST had a systematic error. Using the questionnaire, future research could measure ST with cognitive activity and calculate the rank of total ST among older adults simultaneously and examine the detailed association with cognitive function.
Supplemental Material
Supplemental Material, sj-pdf-1-jgp-10.1177_08919887211006468 - Development of a Questionnaire to Evaluate Older Adults’ Total Sedentary Time and Sedentary Time With Cognitive Activity
Supplemental Material, sj-pdf-1-jgp-10.1177_08919887211006468 for Development of a Questionnaire to Evaluate Older Adults’ Total Sedentary Time and Sedentary Time With Cognitive Activity by Satoshi Kurita, Takehiko Doi, Kota Tsutsumimoto, Sho Nakakubo, Hideaki Ishii and Hiroyuki Shimada in Journal of Geriatric Psychiatry and Neurology
Footnotes
Authors’ Note
The datasets used in this study may be available upon reasonable request to the corresponding author.
Acknowledgments
We would like to thank the Obu city office for their help with participant recruitment.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work received financial support through the Funds of Obu City Local Government and JSPS KAKENHI (Grant Numbers JP18K17995 and JP20K19665).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.