
Abstract
Objectives
To test the hypothesis that depressive symptoms vary with high-sensitivity C-reactive protein (hs-CRP), among older adults with obesity.
Methods
This was a cross-sectional, secondary analysis of baseline data from two related lifestyle intervention trials. The study sample comprises 148 consecutively recruited, community-dwelling older adults (age >=65 years) without severe psychiatric illness and with body mass index >=30 kg/m2. Logarithmically transformed GDS was analyzed as the dependent variable. Independent variables included log-transformed hs-CRP and covariates: sex, age, and concurrent use of antidepressant medication at baseline. An additional analysis was performed using binary conversion of the GDS scores, wherein a cutoff score of 5 was considered positive for depressive symptoms.
Results
Sample mean GDS score was 2.7 (SD 3.0, range 0 – 14). A significant multivariate model of GDS scores (R2 = .089, F = 3.5, P = .010) revealed log-transformed hs-CRP (P = .017) and male sex (P = .012) as associated with depressive symptoms. Supplemental analysis demonstrated associations between depressive symptoms and log-transformed hs-CRP (OR 2.17, P = .001) and between depressive symptoms and male sex (OR 3.78, P = .013). Univariate logistic regression found hs-CRP to be associated with depressive symptoms.
Conclusions
In older adults with obese BMI, male sex and higher hs-CRP are associated with depression, even in a group with relatively minimal depressive symptoms. Hs-CRP may offer clinical utility as a biomarker for depression among older adults with obese BMI, even among those with non-severe psychiatric symptomatology.
Introduction
Older adults with comorbid obesity and depression represent an expanding population, and their adiposity and moods may be connected through a common inflammatory mechanism. Half of US adults are projected to have obesity by 2030, 1 and by 2050, the prevalence of depression among US adults is expected to have grown to 46 million, with prevalence among adults age 65 years or older increasing nearly five times more than among adults younger than 65. 2
Obesity implicates many of the risk factors for depression in old age; nevertheless, obesity in older age is not always found to be related to depression in older age.3,4 Relatively few studies of depression and obesity have focused on older adults, but cross-sectional and prospective evidence does suggest obesity may predict depression.5-7 Inflammatory processes appear to contribute to the development of neuropsychiatric comorbidities in obesity, 8 and consideration of these may improve understanding of the relationship between obesity and depression in older adults.
Elevation in a variety of peripheral inflammatory markers has been observed in depression. 9 Among these is the nonspecific, acute-phase reactant called C-reactive protein, which is elevated in infection or other acute inflammatory processes, and low-grade elevation in this marker was made possible with innovation of the high-sensitivity C-reactive protein (hs-CRP). Past studies have found cross-sectional and longitudinal association between hs-CRP and depression in older adults. 10 Odds of depression in older adults increase by nearly 50% with elevation in hs-CRP at or above 3.17 mg/L, 9 which corresponds with the 3.0 mg/L cutoff defined as designating high cardiovascular risk. 11 Excluding acute elevation >10 mg/L, the odds of finding hs-CRP level >1 mg/L are increased by nearly 30% in patients with depression compared to healthy controls. 12 Elevation in hs-CRP may precede development of depressive symptoms in older adults 13 ; and, mechanistically, elevations in hs-CRP may induce depressive symptoms through disruption of normal endothelial function at the blood-brain barrier. 14
Elevation in hs-CRP is a nonspecific physiologic and biochemical response, originating hepatically and with upregulation from proinflammatory cytokines. 15 Adipose tissue potently releases inflammatory cytokines 16 ; nevertheless, few studies in older adults have assessed a relationship between depression and hs-CRP among older adults with obesity. Improved understanding of the role of inflammation in the etiology of depression in older adults may reorder the importance of other etiologic factors for depression in this group, including the dynamic role of sex and the tendency for morbidity to increase with age, especially as depression risk increases with neurodegenerative illnesses, endocrine changes, medical illness, vascular changes. 17
Prior research has neglected the increasingly comorbid state of obesity and depression in older adults. We set out to determine whether depressive symptoms vary with hs-CRP among older adults with obesity.
Materials and Methods
Study Setting and Study Population
We examined secondary outcomes from baseline assessments (before any intervention) for 148 participants recruited consecutively for two lifestyle intervention trials (ClinicalTrials.gov numbers: NCT03329963, NCT04221750) at the Michael E DeBakey Veterans Affairs (VA) Medical Center in Houston, Texas, between November 2017 and August 2021. Studies recruited older adults (age 65 or older) living in the community and without substance use disorders (including alcohol use to excess), dementia, or other severe psychiatric illnesses (e.g., bipolar I or schizophrenia). Participants’ Mini Mental Status Exam (MMSE) score had to be above 24, as a screening for neurodegenerative disorders. 18 Participants were required to be obese (BMI ≥30 kg/m2) with stable body weight (±2 kg) for the 6 months preceding study entry and to be sedentary (participants could have exercised no more than twice per week and for no more than 1 hour per week). Initial screening excluded individuals with poorly controlled diabetes mellitus (fasting blood glucose >140 or A1c >8.5%) or if receiving insulin therapy. Other exclusionary conditions were uncontrolled hypertension (>160/90), severe cardiopulmonary disease (e.g., recent myocardial infarction or unstable angina), orthopedic impairments, neuromuscular diseases, malignancy within the past 5 years, terminal illness with life expectancy <12 months, osteoporosis, or use of medications that act on bones or induce weight loss. Sex and age were documented as of the baseline assessment. Participants provided informed consent before data collection. Internal Review Board approved the study protocols to ensure the ethical protection of study participants.
Depression
Depression symptoms were assessed using the 15-item Geriatric Depression Scale (GDS), collected among baseline measures in both trials comprising this study. The GDS is a tool designed for rating depression in older adults, found to be reliable and valid as a self-rating depression screening scale, with higher scores suggesting more depression. 19 GDS was analyzed primarily as a continuous variable, with logarithmic transformation due to positive skew in the sample. Additional analysis tests GDS as a binary variable, with a score of 5 or higher constituting depressive symptoms.20-24
C-Reactive Protein
Plasma high-sensitivity C-reactive protein (hs-CRP) was measured by immunoturbidimetric assay with analytical range .3–80 mg/L and up to 760 mg/L with dilution, with daily quality control testing assuring within-run coefficient of variation 5.0% and total coefficient of variation 7.5% according to manufacturer guidance, in a Beckman DxC 800 (Beckman Coulter Diagnostics, Brea, CA). 25 Samples were drawn early in the morning in the fasting state. All participants denied current or recent (within five days) symptoms of a systemic infection (e.g., fever, persistent cough, or swollen glands) prior to undergoing blood draws.
Hs-CRP values >10 mg/L are often considered suggestive of acute illness, 26 but accumulating evidence suggests chronic contributions from obesity and other non-acute processes can elevate CRP, thus underscoring the importance of avoiding exclusion solely based on CRP elevation. 27 Nevertheless, concern remained regarding undue influence from outliers, especially given the positive skew of the hs-CRP. Therefore, hs-CRP for the 9 participants with high hs-CRP (range 10.1 mg/L – 41.2 mg/L) were Winsorized to 10.0 mg/L. Following Winsorization, hs-CRP was logarithmically transformed to further adjust for skew.
Antidepressant Medication
Participant medications were documented during baseline assessment. Antidepressant prescription was binarily categorized for each patient; among these were 15 patients receiving a selective serotonin reuptake inhibitor, eight receiving a serotonin and norepinephrine reuptake inhibitor, six receiving bupropion, and 1 receiving vortioxetine. One patient prescribed lithium was also counted in this group. No participants were receiving steroids or hormone therapy.
Statistical Analysis
Univariate and multivariate linear regression models for logarithmically transformed GDS score used the following independent variables, entered into the model in a single block: logarithmically transformed hs-CRP, age, sex, and antidepressant use. Logarithmically transformed values of hs-CRP were used, due to a non-normal distribution of hs-CRP in the sample.
The database was scrutinized to confirm its statistical appropriateness for linear regression. 28 The data met most assumptions for linear regression (i.e., non-zero variance, no perfect multicollinearity, independence of errors, normally distributed errors, and independent observations). Nevertheless, some criteria limit the appropriateness of linear regression. Because the outcome variable GDS score is bounded by minimum and maximum values, because heteroscedasticity is present in the outcome variable, and because the relationships tested were not necessarily expected to be linear, an additional analytic approach may be appropriate, such as logistic regression. This method would also ensure clinical relevance, by setting a threshold level of outcome variable established as meaningful in prior research.
As an additional step, logistic regression modeling of depressive symptoms (i.e., GDS score of >= 5) was performed by block-entering the same predictor variables entered into the linear regression models. Again, both univariate and multivariate models were created. Pseudo-R2 values were calculated using the Nagelkerke approach. 29 Assumptions testing for logistic regression was completed. 30 All analyses were performed with listwise exclusion of missing variables and 2-sided tests with alpha of .05 in SPSS version 28 (Chicago, IL, USA).
Results
Characteristics of Participants.
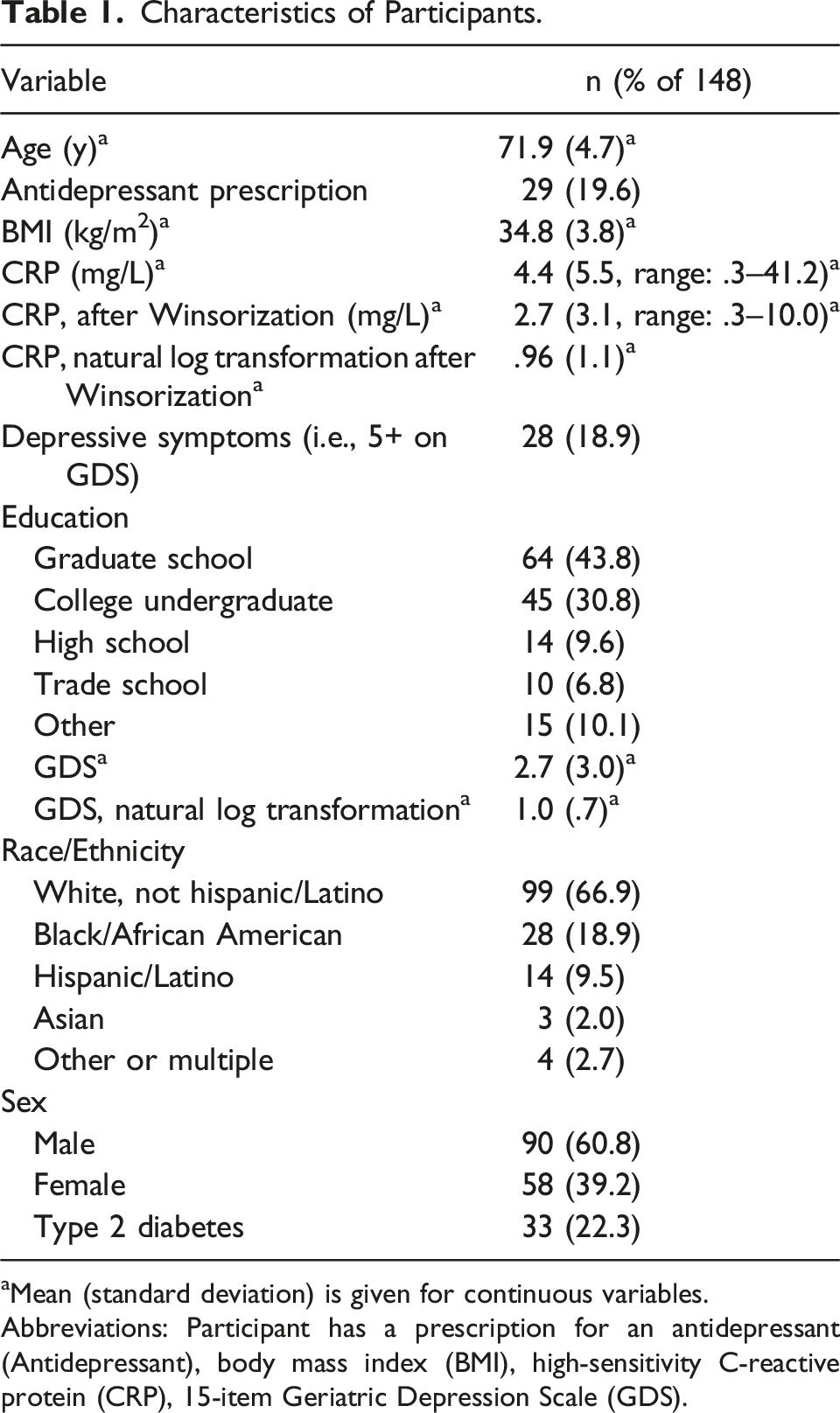
aMean (standard deviation) is given for continuous variables.
Abbreviations: Participant has a prescription for an antidepressant (Antidepressant), body mass index (BMI), high-sensitivity C-reactive protein (CRP), 15-item Geriatric Depression Scale (GDS).
Linear Regression Modeling of ln(GDS) for 148 Participants.
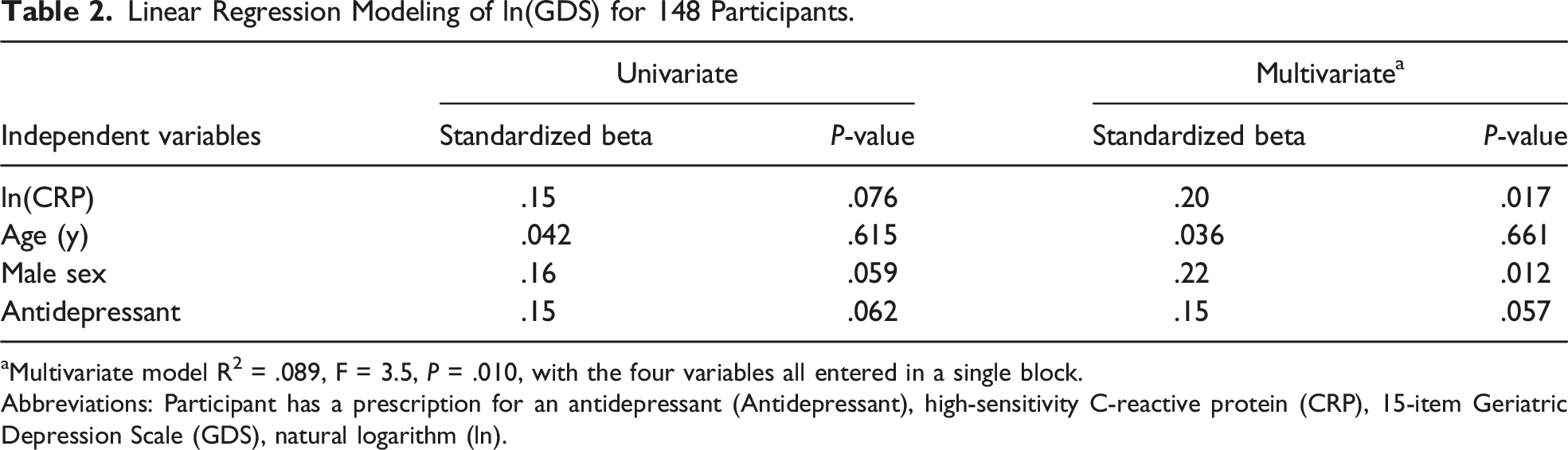
aMultivariate model R2 = .089, F = 3.5, P = .010, with the four variables all entered in a single block.
Abbreviations: Participant has a prescription for an antidepressant (Antidepressant), high-sensitivity C-reactive protein (CRP), 15-item Geriatric Depression Scale (GDS), natural logarithm (ln).
Logistic Regression Modeling of Depressive Symptoms a for 148 Participants.
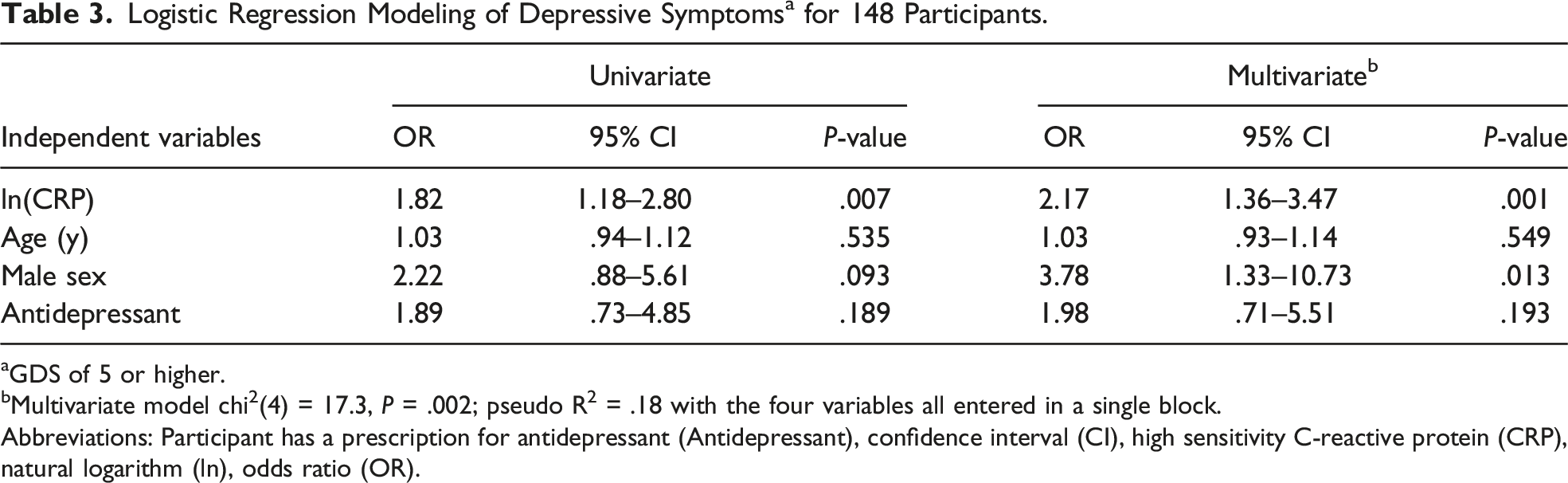
aGDS of 5 or higher.
bMultivariate model chi2(4) = 17.3, P = .002; pseudo R2 = .18 with the four variables all entered in a single block.
Abbreviations: Participant has a prescription for antidepressant (Antidepressant), confidence interval (CI), high sensitivity C-reactive protein (CRP), natural logarithm (ln), odds ratio (OR).
Discussion
This was a cross-sectional study of secondary data to determine whether hs-CRP varies with depression symptoms among older adults with obesity and without severe psychiatric illness. Multivariate modeling suggested that higher hs-CRP was associated with depression in this group, independent of the effects of sex, age, and antidepressant prescription. Depressive symptoms and hs-CRP were significantly related in univariate logistic regression but not when using linear regression. Findings are notable given the relatively low-grade of depression described in the sample and the relatively low grade of hs-CRP elevations in the group.
We highlight the importance of hs-CRP and inflammation in investigations of depression, particularly among older adults with obesity. Data supporting the role of inflammation in depression are extensive, 31 but the correlation between hs-CRP and depression has been thought to diminish with age. 32 Our results suggest that inflammation is a vital correlate with depression in older adults with obesity, even when the inflammation and depression are relatively mild.
Others have similarly found a cross-sectional relationship between CRP and depression in a sample of older Italian adults with metabolic syndrome 33 and elsewhere between depression and hs-CRP for apathy but not depression per se.26,34 Our findings contrast with Dutch and Australian studies that found no cross-sectional relationship between hs-CRP and depression among older adults.20,35 Differences between these studies and the present study include our context (i.e., baseline measures from a lifestyle trial), our inclusion criteria requiring obesity, and the geo-cultural distinctness of the represented populations.
We observed a greater risk of depression in males compared to females, at least within multivariate models. This finding may contrast with prior studies wherein females have shouldered a larger burden of morbidity in obesity-depression relationships.36,37 The role of sex in depression in older age has been controversial; notably, some work suggests a diminishing excess burden of depression in postmenopausal females, 38 and others observing the opposite. 39 Further study may elucidate physiological and social mechanisms supporting a mediating or moderating effect of sex on the inflammation-depression relationship among older adults.
Strengths and Weaknesses
This study offers a focused perspective on older adults with obesity within the larger emerging public health crisis involving obesity and depression. We examined a niche sample with obesity and sedentary lifestyles but without severe diabetes, severe psychiatric illness, nor a variety of other specified correlates of obesity. Our cross-sectional design and multivariate regression approach facilitated consideration of multiple variables simultaneously. The emergence of significant findings despite relatively low-grade variation in hs-CRP and depressive symptoms may point to the importance of these variables as potential components or markers of a pre-clinical syndrome.
Limitations principally stem from our use of secondary data in the study; the trials comprising this study were not explicitly powered for our targeted variables. The study is conceptually limited because obesity, depression, and inflammation have myriad etiologies in older age. This complexity could explain why multivariate findings were significant when univariate were not. Sample size limited the number of possible control variables, and narrow distribution of racial/ethnic groups and of education variables thwarted our inclusion of these variables. Analytic methods were limited by minor infringement on the assumptions of linear regression testing. Additional (logistic regression) analysis offset these concerns but was itself limited by dichotomization of the dependent variable, even as this approach was supported in the literature.
Conclusions
The intersections among obesity, inflammation, and depression in older adults constitute a complex angle with emerging public health priority. We observed that low-grade variations in depression and inflammation may be related, among older adults with obesity. Future research should determine the prospective relevance of these baseline measures and assess the value of hs-CRP as a longer-term predictor of depression and other neurologic changes in older adults with obesity. Mechanistic studies (including hormonal signaling, extent of adiposity, and social aspects of obesity) should be leveraged to better unpack the multifaceted relationships among obesity, inflammation, and depression cooccurring in older age—particularly as components of a premorbid phenotype for age-associated neurologic changes. Finally, intervention studies should be developed to target metabolic and inflammatory pathways in the prevention and treatment of depression and cognitive decline.
Footnotes
Acknowledgments
We thank the participants for their cooperation and Arjun Paudyal for study coordination.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Kunik is an unpaid member of the board of the Houston & Southeast Chapter of the Alzheimer’s Association, and he performs guardianship evaluations for the county probate court. Dr. Villareal is on the Clinical Trials Advisory Panel (CTAP) for the NIH-National Institute on Aging (NIA) and the Data and Safety Monitoring Board (DSMB) for several NIH-supported clinical trials. The other authors have nothing to disclose.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Health (RO1-DK109950) and the VA Office of Research and Development (CX002161). This work was also partially supported through the use of resources and facilities of the Houston Center for Innovations in Quality, Effectiveness and Safety (CIN13-413). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health, the Department of Veterans Affairs (VA), or Baylor College of Medicine.