
Abstract
Background:
Human milk feeding rates in the United Kingdom are a public health concern. Changes to United Kingdom policy and practice are needed to improve lactation support. These should be informed by those with lived experience of human milk feeding and those who provide support.
Research Aim:
The aim of this study was to identify research, policy, and practice priorities for increasing human milk feeding rates using insights from a wide range of stakeholders. A secondary aim was to evaluate the influence of a World Café on individual attendees and their interactions within the organizations and communities of which they are a part.
Methods:
The research employed a participatory qualitative design, incorporating a cross-sectional survey and World Café discussions. World Café is a novel approach to engaging stakeholders in discussion, resulting in consensus-building and participatory-driven recommendations. A pre-event survey was completed by a self-selected sample of 67 participants; 37 of these (55%) took part in World Café discussions or an online focus group. World Café discussions and the online focus groups were recorded and transcribed verbatim. Following the World Café, 12 participants (32%) completed a post-event survey, and eight (22%) completed an additional follow-up survey at 2 months.
Results:
Priority policy and practice changes were identified, including enhancing education, the need for dedicated funding for human milk feeding support, the need to include family within support provision, and the need to change policy regarding media representations of infant feeding. In addition, World Café methodology proved valuable for facilitating networking and instigating changes in relation to support.
Conclusion:
World Café generated stakeholder agreed-on priorities for research and policy. Many of the recommendations from historical policy and guidance continue to be areas for further development.
Keywords
Key Messages
A better understanding of policy and practice priorities is needed to improve human milk feeding support.
World Café is a participatory tool well suited to facilitating change through stakeholder discussion but has, to date, not been used to explore human milk feeding priorities.
Participants identified areas of needed change in antenatal, child and adolescent, and healthcare professional education; human milk feeding support; family and partner involvement; and media representations of human milk feeding and infant formula.
Research events incorporating World Café can help to identify practice and policy priorities, facilitate network building, and provide a catalyst for change.
Background
The World Health Organization (WHO, 2020) recommends exclusive human milk feeding for the first 6 months of life to achieve optimal growth, development, and health. Thereafter, nutritious complementary foods should be offered alongside continued human milk feeding up to the age of 2 years or beyond. In this research, human milk feeding is defined as the child receiving any human milk either directly from the breast or expressed (Labbok & Starling, 2012).
Flexible and supportive family friendly policies are linked to improved human milk feeding initiation and duration (Chai et al., 2018; de Lauzon-Guillain et al., 2019). The United Kingdom (UK) has some of the lowest human milk feeding rates (Victora et al., 2016) and poorest family friendly policies across high–middle income countries, with many parents experiencing limited access to support such as paid maternity leave and flexible working opportunities (Chzhen et al., 2019). In addition, while the UK provides some support services through the National Health Service (NHS), the quality and availability of these varies across the country (Grant et al., 2018), and a lack of continuous funding means that charities and online groups are frequently relied on to fill the gaps in support (Regan & Brown, 2019). Furthermore, formula advertising policy in the UK could be a barrier to human milk feeding. Currently UK policy only incorporates some of the WHO international code for the marketing of human milk substitutes (WHO, 1981) into law, leaving a gap in policy permitting widespread advertising of follow-on infant formula. While a private bill passed through parliament with unanimous support in 2017 (Thewliss, 2017), no further progress has been made towards fully legislating any changes, suggesting that, to date, this has not been a policy priority. These factors illustrate that changes to UK policy and practice need to be implemented if human milk feeding rates are to improve.
In April 2022, as part of the leveling up agenda and supporting families program (Ministry of Housing, Communities & Local Government, 2021), the UK government pledged £302 million ($400 Million) for the creation of Family Hubs in 75 local authorities with £50 million of this to be dedicated to establishing human milk feeding support services (Department for Education, 2022). This announcement followed years of cuts to infant feeding services (United Nations Children’s Fund [UNICEF] UK, 2016), and it is not yet known what influence Family Hubs will have on human milk feeding support. The policies and practices developed for Family Hubs need to be grounded in the views, knowledge, and expertise of stakeholders who have experience of human milk feeding, and those who work to support infant feeding.
World Café is a participatory tool well suited to facilitating change through stakeholder discussion (Brown et al., 2005), and is grounded in the belief that communities have within them the wisdom and creativity needed to resolve difficult challenges, advocating that solutions and actions can be generated through conversation (Brown et al., 2005). Researchers using World Café employ an informal “cafe” style setting to bring together stakeholders to explore issues by discussing them in small table groups (Brown et al., 2005). The approach produces research data inclusive of potential solutions, benefiting participants through shared dialogue that can motivate participation in bringing about change (Löhr et al., 2020). World Café has been used to inform policy and practice in several domains, including disability issues (Bumble & Carter, 2021), sustainability (Silva & Guenther, 2018), health promotion and prevention (Recchia et al., 2022), and criminology (Page, 2023), but has, to date, not been used to explore human milk feeding policy and practice priorities.
The aim of this project was to identify research, policy, and practice priorities for increasing human milk feeding rates by drawing on insights from a wide range of stakeholders. A secondary aim was to evaluate the influence of a World Café event on individual attendees and their interactions within the organizations and communities of which they are a part.
Methods
Research Design
The research employed a participatory qualitative design. A mixed open and closed cross-sectional survey was used to gather context for a World Café event with follow-up surveys post-event, and after 2 months, to evaluate impact. In addition, data were collected in the form of transcribed World Café (Brown et al., 2005) discussions and an online focus group.
World Café is a constructivist approach to enquiry in which researchers and participants co-develop findings (Brown et al., 2005). This approach ensures that stakeholders who will benefit from the findings are involved in their construction, in line with the aims of this research. Ethical approval was obtained from the Staffordshire University Health, Science and Wellbeing ethics committee.
Setting and Relevant Context
This study was conducted in the UK, which has one of the lowest human milk feeding rates in Europe, with only 47% of babies exclusively fed human milk at 6–8 weeks post birth in England (Public Health England, 2020a) and 44% in Scotland (National Services Scotland, 2019). While attendance was possible nationwide, the location of the event was Stoke-on-Trent in the West Midlands of England, an area with below national average human milk feeding rates (Public Health England, 2020b). Parents in the UK have access to breastfeeding support through free at the point of access NHS services and social services, in addition to support provided by charities and the voluntary sector. However, the quality and availability of this support are not consistent across the country (Grant et al., 2018).
Sample
Inclusion criteria were that participants needed to be stakeholders with an interest in infant feeding. This included either having experience of providing human milk to their child, or working within, or currently in education for, roles that support human milk feeding behaviors. Participants self-identified as stakeholders through a volunteer opportunity sampling approach (Morse, 1990). Participants were self-selecting and no exclusion criteria were applied; however, as the event advertising materials and conduct were all in the English language, those who were unable to read or speak English did not attend.
Advertisements were placed for a free research and networking event entitled “let’s talk about breastfeeding” on social media. Interested attendees were sent a link to complete event registration and informed consent forms via Qualtrics© (Provo Utah, 2022). Sixty-seven participants completed the pre-event survey and 37 (55.2%) of these attended the event, reasons for non-attendance are unknown. World Café is a relatively new approach, and therefore, explicit sample size guidelines do not exist. The sample recruited represents an adequate number for a medium-large project using interactive qualitative data collection methods (Braun & Clarke, 2013). Participants did not receive any monetary compensation, however those who attended the World Café in person were provided with lunch and refreshments.
Measurement
The pre-event survey was used to collect demographic information: role or interest in human milk feeding support; perceptions of human milk feeding support, promotion and maintenance, and policy; and research priorities. The post-event survey was used to collect feedback on the event format and influence on individual attendees. This survey also collated consensus statements, which were respondents’ suggestions for the most discussed issues, for each of the three World Café questions. After 2 months a final survey was used to explore the longer-term influence of the event. This survey asked about things that may have occurred since attending and collated numerical ratings on the usefulness of the event for outcomes such as raising awareness and making connections.
Principle three of World Café is to “explore questions that matter” (Brown & Isaacs, 2005, p. 78). Therefore, the questions asked in the World Café were designed by the first author to understand how information discussed at the event might be used, and to establish the research, policy, and practice priorities for improving human milk feeding support in the UK. The chosen questions were: (1) “What stood out for you in the research and experiences discussed today, and what do you hope to do with this new knowledge?” (2) “What do you feel are the immediate breastfeeding research priorities?” (3) “What do you feel are the biggest barriers to breastfeeding research influencing policy and practice, and how might we overcome these?”
Data Collection
Survey data collection commenced in April 2022, and the World Café event was held on May 26, 2022. The second survey was circulated immediately following the World Café and the longer-term follow up survey was circulated in July 2022. Informed consent to take part in all parts of the research was obtained during the pre-event survey.
The World Café event was held at Staffordshire University. The lead facilitator (AB) is a Health Psychologist with human milk feeding research expertise and lived experience of human milk feeding. The first principle of World Café is “setting the context.” To achieve this, researchers are responsible for “intentionally creating the flexible boundaries in which the group’s collaborative learning unfolds” (Brown & Isaacs, 2005, p. 49). This process requires “clarifying the relevant aspects of the larger situation” (p. 50) and articulating “beliefs or assumptions about the nature of the current situation” (p. 51). Therefore, to set the context, an opening presentation overviewed research findings from studies conducted at Staffordshire University, where the event was held. These papers covered a range of topics and methods including: intentions to mixed-feed in first-time mothers (Burton, Taylor, Swain et al., 2022), predictors of human feeding duration (Thurgood et al., 2022), body image and human milk feeding behavior (Fern et al., 2014; Morley-Hewitt & Owen, 2020), COVID-19 restrictions and the postpartum experience (Riley et al., 2021), and experiences of extended human milk feeding (Burton, Taylor, Owen, et al., 2022). The presentation also outlined areas identified as research, policy, and practice priorities by participants in the pre-event survey and depicted these as pie charts. How the research presented mapped on to these priorities was also discussed. In addition, an overview of current UK human milk feeding policy was presented. This approach to sharing the event organizers’ own research, in addition to current policy, transparently presented the position of the research team prior to commencing the World Café discussions, and clarified the perceived need for additional policy work to improve human milk feeding.
The process of World Café is guided by seven principles followed during the event, and detailed in Table 1. For this event World Café discussions were held in multiple rounds of 20–30 minutes and facilitated by pre-trained table-hosts (Page, 2020). All table hosts attended an online meeting to discuss World Café processes and were able to access pre-recorded training materials created by SP, a specialist on the conduct of World Café.
Event Agenda and World Café Sequence.
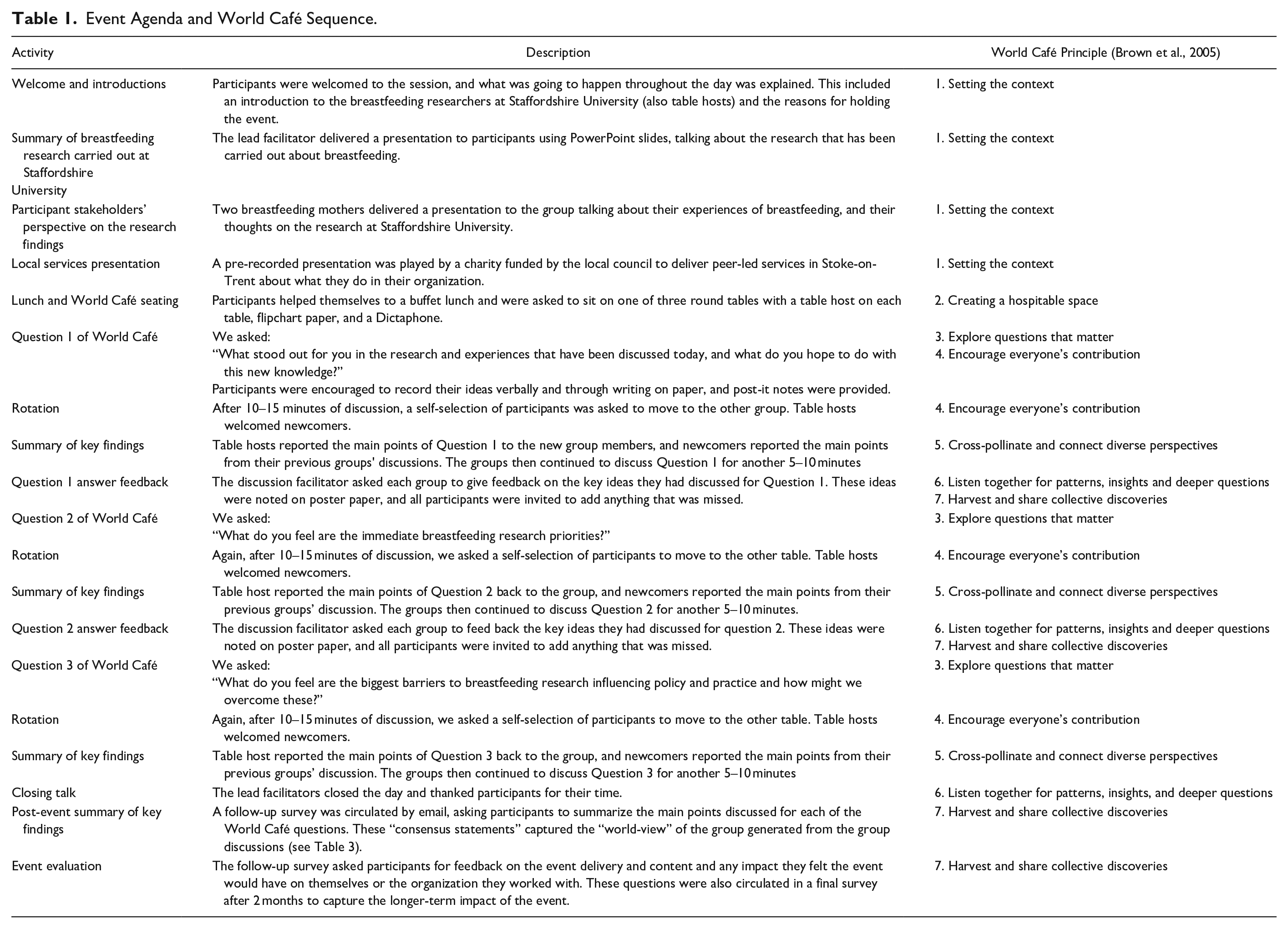
The lead facilitator presented instructions and ground rules for the conduct of the World Café on PowerPoint slides. All participants were asked to agree to be respectful of the views of others, not discuss the specifics of anyone’s experiences outside of the group, and to let the table host know if they shared anything that they would prefer was not included in the research. These rules were based on guidance for conducting focus groups (Braun & Clarke, 2013). All participants agreed to these rules verbally, and then discussion questions were posed. For in-person attendees, after each question, a few participants from each group moved to a different table where the discussions continued, facilitating an enhanced exchange of knowledge on each topic. Online participants took part in a single focus group. Discussions were audio-recorded and noted on flipchart paper by table hosts or participants, if they wished, or in the online chat function. Discussions were recorded and transcribed verbatim with all identifying information removed.
Reflexivity
Researchers must examine positionings and explore how these may play a role in the construction of research findings. However, it is also important to acknowledge that perspectives are not singular or fixed, and therefore, full insight into positionings is an unachievable aim (Finlay, 2002). The opening presentation set out the researchers’ position that there are failings in current UK policy and practice and that improvements need to be made. This positioning informed the development of the project and shaped the questions asked at the World Café.
Co-construction of findings with participants is an interpretative process (Braun & Clarke, 2013) and, therefore, decisions made by the lead researcher were interrogated through discussion with the wider team of researchers, comparison, and cross-checking of unfolding ideas with the survey feedback and World Café transcriptions. These additional sources of evidence were reviewed to ensure the themes created did not miss any important topics captured by these additional forms of data. No modifications to themes were made following this review process. The engagement in reflexive practices (Finlay, 2002) by the research team was also used to interrogate their positioning in relation to the questions being explored.
Data Analysis
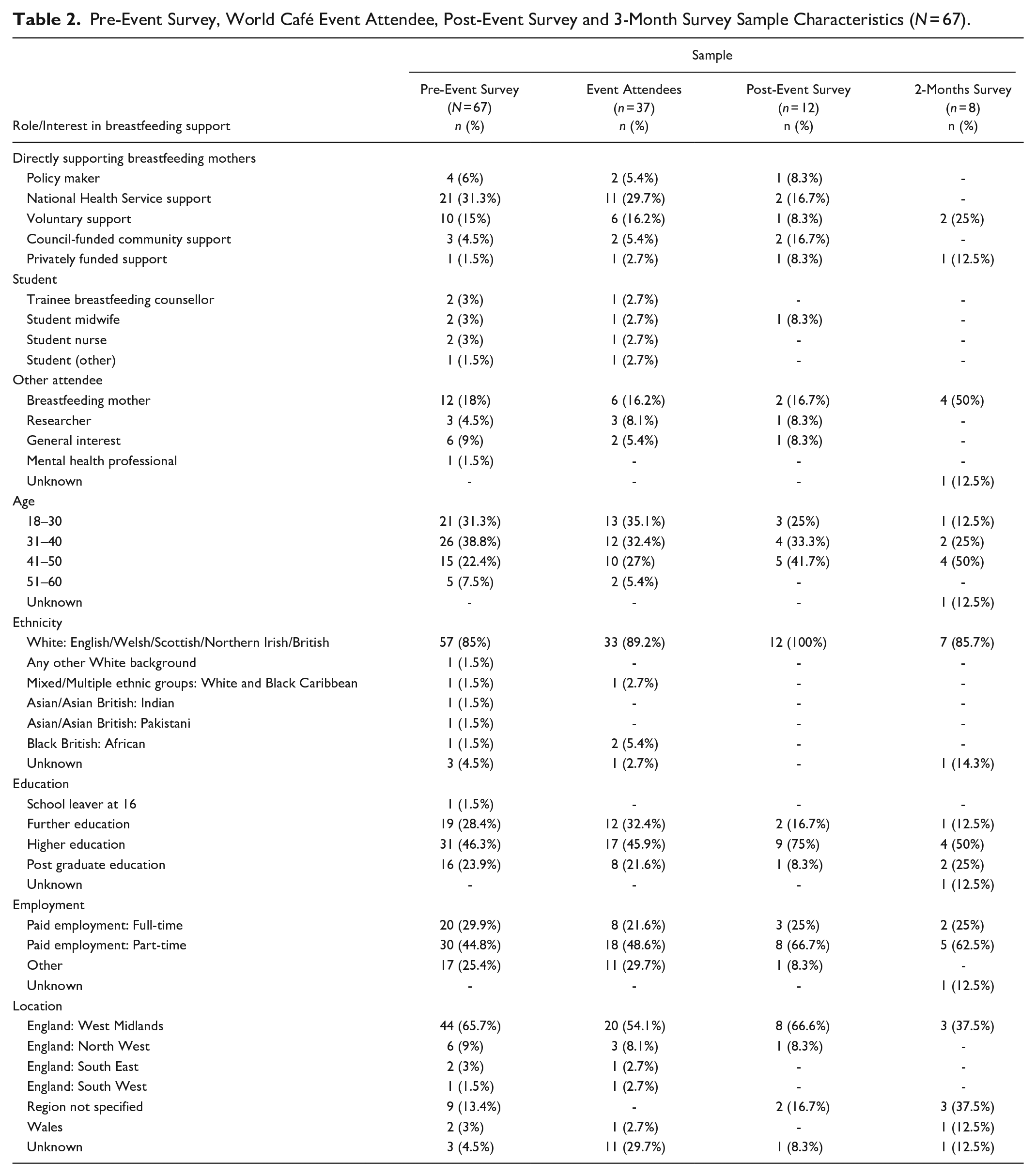
Demographic data were extracted from the pre-event survey and tabulated. A comparison of characteristics for survey completers and event attendees can be seen in Table 2.
Pre-Event Survey, World Café Event Attendee, Post-Event Survey and 3-Month Survey Sample Characteristics (N = 67).
Aim 1: Research, policy, and practice priorities
To inform the opening presentation for the World Café, the top research, policy, and practice priorities from the first survey were extracted into Excel and categorized by AB. For policy priorities, three categories were developed in which more than one response could be grouped: health and nutrition benefits and impacts, improved support, and encouragement and promotion of human milk feeding. Five more categories were represented by single responses: increasing human milk feeding in areas of deprivation, acceptance in society, creating safe spaces, training for midwives, and support for working mothers.
For research priorities, four categories were developed in which more than one response could be grouped: health and nutrition benefits and impacts, support interventions, current rates of human milk feeding in the UK, and intentions to formula feed. An additional eight categories were represented by single responses: societal impacts of formula feeding, tongue tie, pressure from healthcare professionals to feed with human milk, barriers to human milk feeding, taking medications while human milk feeding, the impact of Covid-19, supporting human milk feeding without stigmatizing formula feeding, and assisted feeding. Category allocation was reviewed and agreed upon by JT.
The percentage of responses in each category was calculated and represented as two pie charts, one for research priorities and one for policy and practice priorities. These were displayed to participants as part of the opening presentation to enable responses from all participants in the pre-event survey to contribute to the construction of the consensus reached during event discussions.
World Café discussions
World Café aims to develop a participant-led worldview on a topic of interest (Brown et al., 2005). This participatory form of thematic analysis encourages participants to give feedback and agree on the key themes of interest (Page, 2023). The World Café used a hybrid delivery, meaning that full discussion between online and in-person attendees was challenging. Brown and Issacs’ (2005) guidance recommends that World Café is used flexibly rather than as a rigid set of rules. They state that “the approach you choose for whole-group conversation depends on the café’s purpose and the ways that sharing discoveries can be most useful to your desired outcomes” (p. 149). Therefore, rather than seeking feedback after each rotation to establish themes, the method was pragmatically adapted to request that event attendees provide feedback on the priority outcomes of their discussions as part of a follow-up evaluation survey, ensuring that both in person and online attendees could equally contribute. Participants were asked to state what the main topics discussed by their groups were in relation to the following three questions: “What stood out for you in the research and experiences that have been discussed today, and what do you hope to do with this new knowledge?” “What do you feel are the immediate breastfeeding research priorities?” “What do you feel are the biggest barriers to breastfeeding research influencing policy and practice?” Responses were treated as statements of consensus which would otherwise have been made verbally at the event.
Facilitating participants to identify the core themes of consensus in this way enabled a co-created starting point for themed analysis. The consensus statements generated were short (e.g., “education around breastfeeding for children”). The first author, a researcher experienced in several forms of pattern-based qualitative analysis, extracted the consensus statements from Qualtrics into a Microsoft Excel spreadsheet. These were reviewed and grouped into similar areas (e.g., “family influence” and “need for more support”) and then labeled.
This involved an interpretive approach to inquiry, and therefore, for transparency on the process examples of the consensus statements grouped under each theme are shown in Table 3. Themes were then cross-checked against the notes taken on poster paper and in the chat box during the World Café. Transcripts were also read, and data for each theme was extracted into separate Word documents. Very few examples of the “body image” theme were evident in the World Café discussions, despite being raised by four respondents in the post-event survey; this may have represented a “new” area of interest for participants following the research presentations. As body image was not discussed in the World Café in-depth as a priority, it was not included as a theme in later analysis. This decision was made as direct quotes on this topic from the world café did not exist, preventing the in-depth analysis required for theme development. The transcripts were re-read to check for any additional potential consensus areas that may have been missed. No additional themes of discussion were evident, illustrating that these statements captured the worldview of those attending the event.
Post World Café Event Survey Consensus Responses.
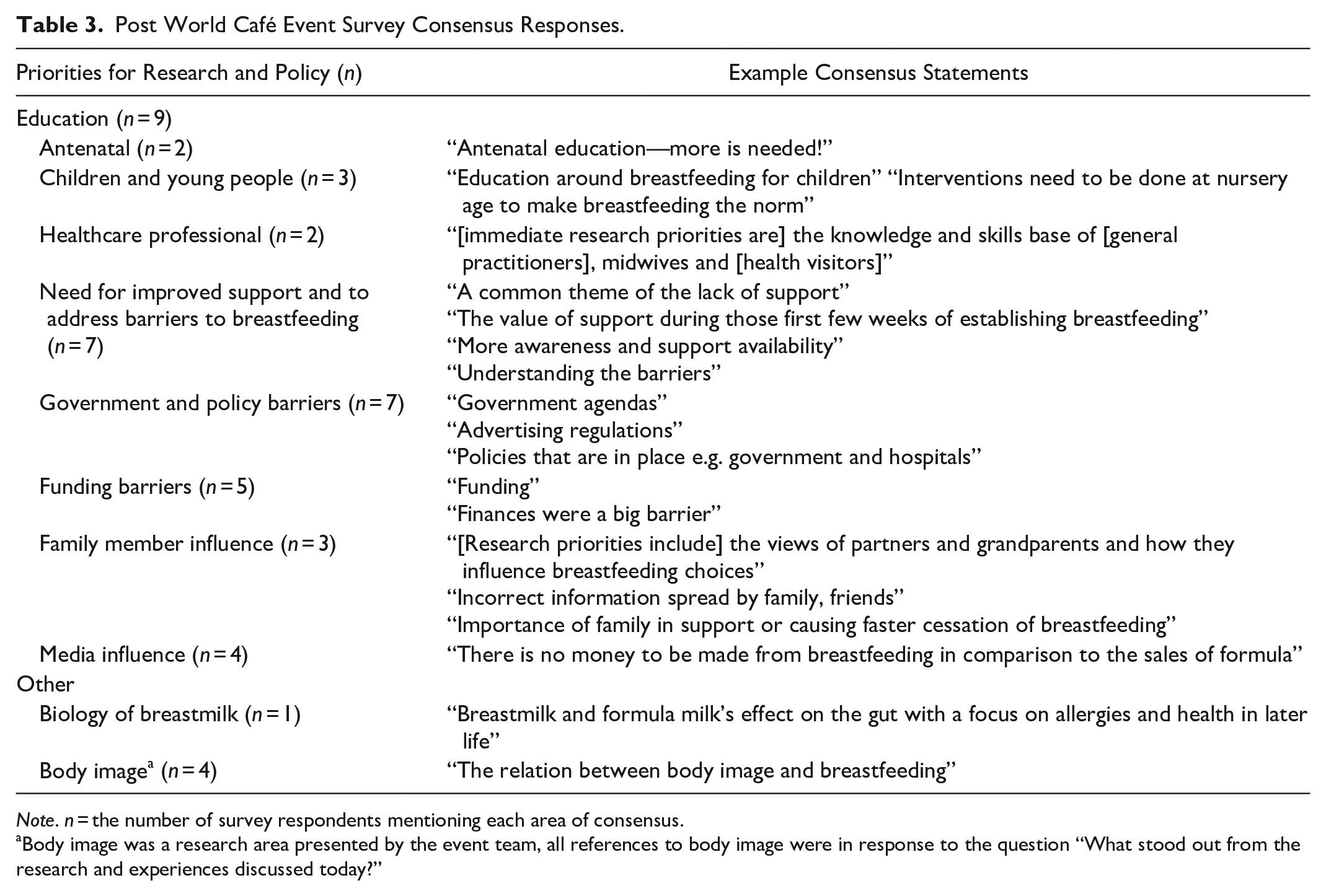
Note. n = the number of survey respondents mentioning each area of consensus.
Body image was a research area presented by the event team, all references to body image were in response to the question “What stood out from the research and experiences discussed today?”
To produce the final narrative, the first author reviewed the Word document created for each consensus theme. These documents were also reviewed and agreed upon by the second and third authors who, together with the first author, co-created the theme narrative.
Aim 2: Evaluation of the Success of the Event
Ratings of event impact from post-event surveys were extracted and means calculated (Table 4). Qualitative post-event survey data were extracted into a Word document and reviewed by the first author to produce a narrative account of the feedback received. The first author also completed follow-up discussions with some attendees who requested it to gather additional verbal feedback on any influence the event may have had. Field noted minutes of these discussions were used to inform the narrative account.
Means and Standard Deviations (SD) for Post-Event Perceptions of Event Impact.
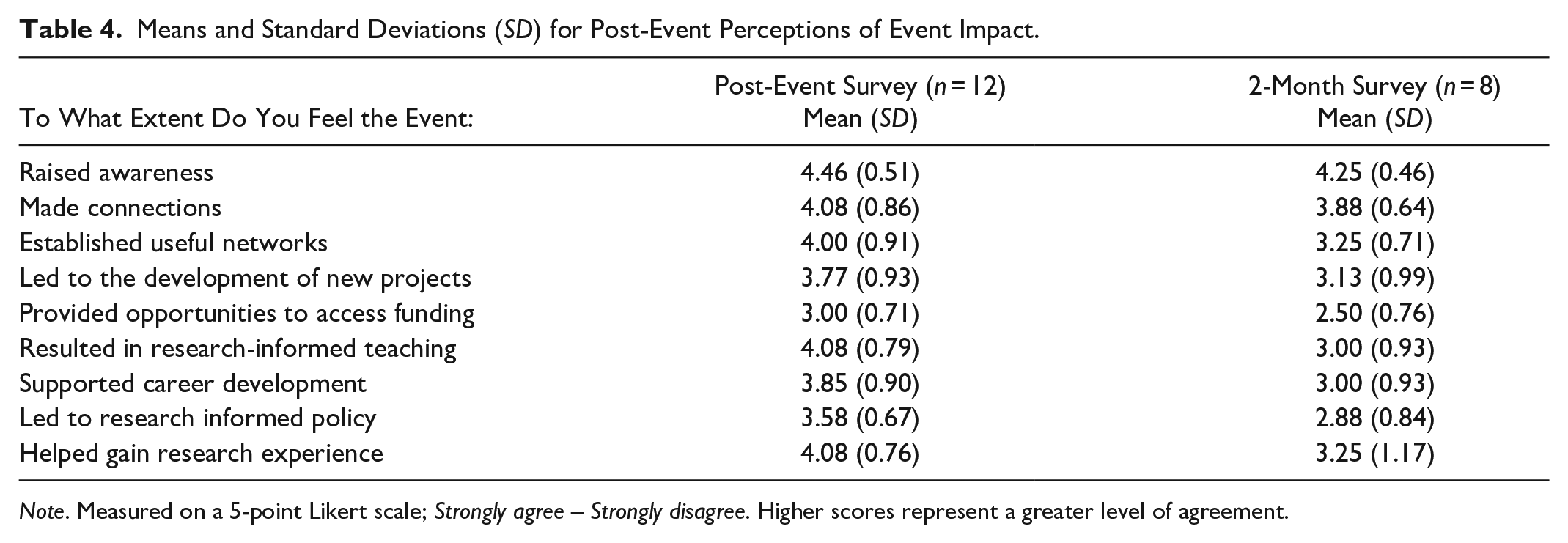
Note. Measured on a 5-point Likert scale; Strongly agree – Strongly disagree. Higher scores represent a greater level of agreement.
Results
Characteristics of the Sample
Participants all identified as female and varied in age and background; 15 attended in person, and 22 attended online. Most worked directly supporting human milk feeding through policy-making, National Health Service (NHS) services, council provision, voluntary support, or private services. Others included students, researchers, human milk-feeding mothers, and those with a general interest. Further details can be found in Table 2.
Aim 1: Research, Policy, and Practice Priorities
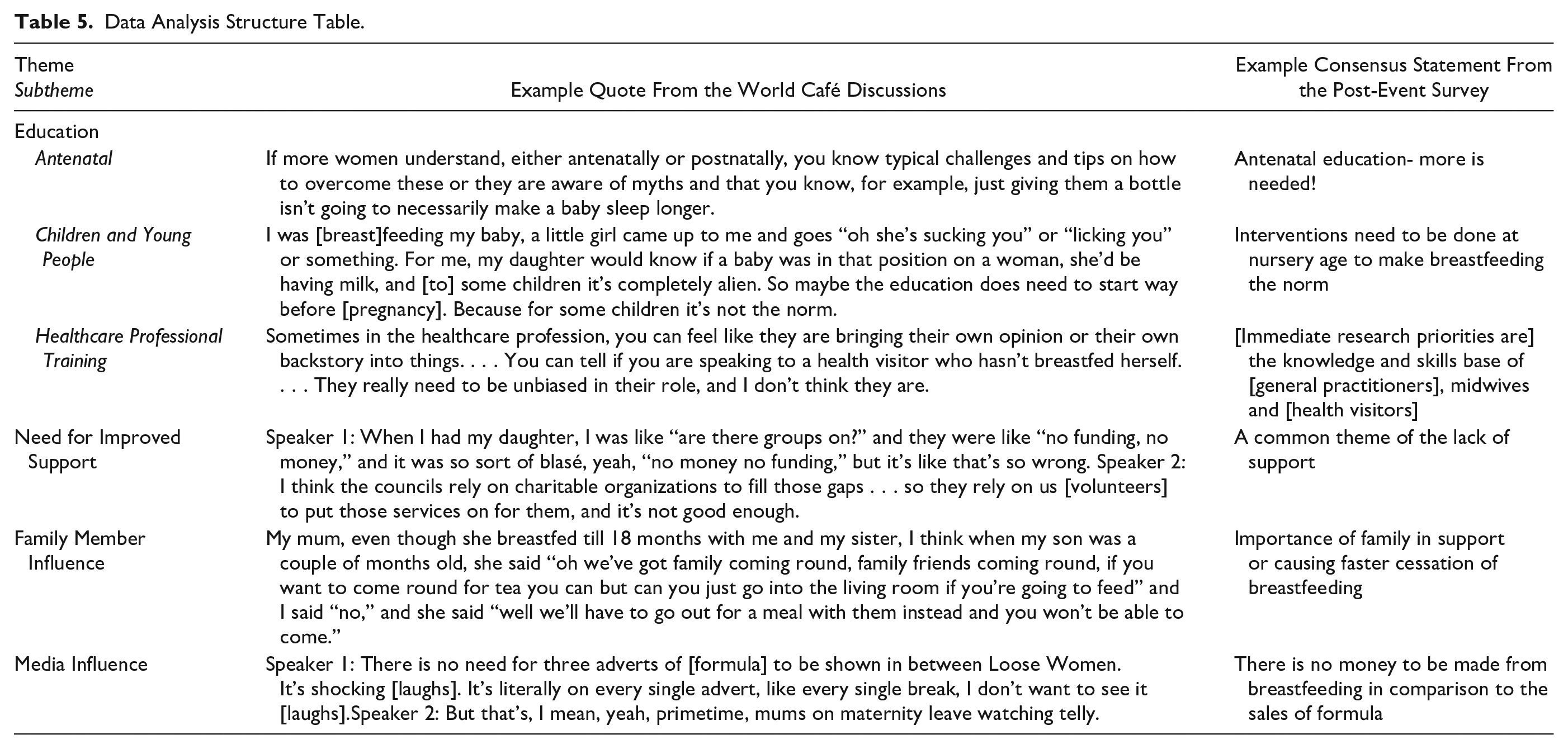
An overview of the theme structure developed can be seen in Table 5. Consensus statements related to four key areas: education (antenatal, children and young people, healthcare professional training), need for improved support, family member influence, and media influence. Each of these is discussed and supported by direct quotes from the World Café discussions. In the narrative, the terms “Speaker 1” and “Speaker 2,” and so forth, are used to indicate turn-taking. Quote examples are taken from a range of speakers. Given the nature of the data collection and the rotation of speakers, it is not possible to allocate different designations for each participant. The tracking of participants from group to group is not advocated as part of the World Café method as it would be an intrusion on the natural nature of discussions between participants (Brown et al., 2005).
Data Analysis Structure Table.
Theme 1: Education
The pre-event survey highlighted that 23.1% of respondents (n = 6) felt that education was the most important policy priority. World Café discussions reinforced this priority, and consensus statements in the post-event survey confirmed this as being a community worldview. Participants highlighted three priority areas for enhanced education: (1) antenatal, (2) children and young people, and (3) healthcare professional training.
Antenatal
A consensus was that human milk feeding information and exposure to support need to be prioritized earlier in pregnancy. A student midwife explained:
[Human milk feeding is] touched on at booking to have a look at it further down the line . . . and then at 34 weeks, as well when we sort of go through the birth plan it’s briefly touched on. . . . [If your baby is born] before 36 weeks you’ve missed that conversation so you’ve missed all that information, and as well if you’re premature obviously you’re encouraged to breastfeed or express and then it’s, like, but actually you’ve not had any education about that at all, so you’ve missed a lot. I think it needs to be a lot sooner.
The group felt that delay in infant feeding related discussion was compounded by regular exposure to formula marketing. It was felt that this indicated that formula feeding was expected, leading to the purchase of bottles and a mental shift towards using formula:
Wherever you shop . . . you are overwhelmed with all these different bottles, glass bottles, pink bottles, purple bottles, anything-you-want bottles, and then [for breastfeeding] you’ve just got like some breast pads that’s it. . . . So how exposed to [breastfeeding] are you? And I intend to breastfeed, but I’ve bought bottles, thinking . . . so I’ve already set myself up to fail.
It was agreed that early exposure to infant feeding information and support should be standard care. For example:
Not to pressurize anyone, but just to offer [appointments with an antenatal feeding team or breastfeeding support group] to everyone . . . to give them, like, an insight into what it will be like, rather than having all this information when the baby is actually born, and then being overwhelmed by a baby, the information, feeding, issues with feeding and what not.
It was agreed that educating pregnant women about myths and potential challenges would help to empower and prepare them to overcome barriers:
If more women understand, either antenatally or postnatally, you know typical challenges and tips on how to overcome these or they are aware of myths and that you know, for example, just giving them a bottle isn’t going to necessarily make a baby sleep longer. . . . If women know these things, then actually when, if a challenge arises either, they know where to seek support from, you know, a peer supporter, peer support group or a healthcare professional, and maybe it’s just going to help their confidence a little bit more if they think actually this isn’t the right information, and we’re just kind of arming these women a little bit better.
Children and Young People
Another consensus was that providing education on infant feeding during pregnancy is too late and that there should be a focus on educating children and young people. Some observed that children often did not know what human milk feeding was:
I was feeding my baby, a little girl came up to me and goes “oh she’s sucking you” or “licking you” or something. For me, my daughter would know if a baby was in that position on a woman, she’d be having milk, and [to] some children it’s completely alien. So maybe the education does need to start way before [pregnancy]. Because for some children it’s not the norm.
Attendees suggested that education should begin when children start to learn about anatomy or even earlier:
I work in a nursery class in a school, and I’ve actually sneaked it in before, when we were looking at farms and where food comes from. . . . When we’ve talked about milk, and I’ll sit there in circle time and go “that comes from cow’s boobies,” and the children all like collapse in laughter, it’s like, well they do, and then that conversation starts and I’m like, “well I feed my baby from mine.”
The discussion also explored whether there may be a backlash from parents towards talking about human milk feeding in schools. This was felt to reflect cultural sexualization of breasts: Speaker 1: “as soon as you say [human milk feeding to parents] they start thinking of the sexualized side of it.” Speaker 2: “Exactly, [they think] “I don’t want my children to know about that.”
Attendees felt that the solution was to introduce information about human milk feeding through the biology curriculum. This was preferable to inclusion as part of sex education to avoid risk of sexualization: “One of the girls over there was saying her 7-year-old was just being taught about some body parts, not like sex education, but body parts. . . . So maybe then just bringing up the functionality of breasts.”
Another area in which it was felt that education could be facilitated was through children's books, by ensuring that nurseries and early education settings provided books including both human milk and formula feeding examples:
Speaker 1: But then also books, I’ve made sure there has [sic] been mums that have been breastfeeding as well as bottle feeding, because I just think that little bit of education from that age is really important. Speaker 2: That’s a really good point actually, yeah, about like, I’ve never even thought of it like that when you see, like, babies and bottles in books and stuff, like that’s setting it in their mind from a really young age, isn’t it, then and normalizing it?
Healthcare Professional Training
There were concerns about healthcare professional training and the influence that negative healthcare interactions could have on human milk feeding.
I remember [a friend] saying this to me [that] they’re saying, “the health visitor [said] you’re not superwoman, like, and I was like determined to breastfeed but she was always trying to put me off.” She’d said to our friend, “he’s had all the goodness now, you know, anything else is just extra, so if you feel like you want to give up you’re not superwoman, give up.” So, she did give up! Because, well, he’s had all the goodness now, after a week! And I was like, “argh,” because she was breastfeeding fine!
It was acknowledged that some of these challenges could be influenced by training and experience, and that infant feeding awareness needs to be a priority for healthcare professionals. For example, health and social care professionals themselves were thought to be anxious about providing infant feeding support: “The girls are currently training in breastfeeding and antenatal [care] in the children’s centers and I’ve spoken to them, and they’ve said ‘oh it’s overwhelming, we don’t feel prepared to, to teach this’ . . . because they’ve never experienced it.”
This lack of training and experience was believed to lead to deficits in the delivery of support:
Sometimes, in the healthcare profession, you can feel like they are bringing their own opinion or their own backstory into things. . . . You can tell if you are speaking to a health visitor who hasn’t breastfed herself. . . . They really need to be unbiased in their role, and I don’t think they are.
Theme 2: Need for Improved Support
The pre-event illustrated that support was the main priority for policy, including antenatal, but especially from birth and the first few weeks (n = 12; 46.2%). In addition, 16% (n = 4) felt that support interventions were the most important focus for future research. The event discussions confirmed these priorities.
It was agreed that support groups were essential components of antenatal and postnatal care. It was felt that peer support helped to encourage and normalize human milk feeding and that opportunities for group exposure should occur earlier in pregnancy:
Speaker 1: Just, you know, [going to peer support groups while pregnant] you see mums who’ve got older and younger babies and you can see [human milk feeding] happening, and they’re talking about their experiences and you can ask them, and I can guarantee, like, all the mums that are in my support group, all of them want to talk about everything, like they are so open about things, so I’m trying to–Speaker 2: It normalizes it.Speaker 1: Yeah, it does, yeah.
However, there was also a consensus that budget cuts were a threat to such opportunities and had, in some cases, already reduced access:
Speaker 1: When I had my daughter, I was like “are there groups on?” and they were like “no funding, no money,” and it was so sort of blasé, yeah, “no money, no funding,” but it’s, like, that’s so wrong. Speaker 2: I think the councils rely on charitable organizations to fill those gaps . . . so they rely on us [volunteers] to put those services on for them, and it’s not good enough.
Theme 3: Family Member Influence
It was agreed that infant feeding decisions were not made in isolation and that family members and other social contacts played an important role. This was felt to be overlooked in most support provisions which focus largely on the mother.
Family was acknowledged as a source of support but, even when supportive of human milk feeding, cultural norms and lack of education or knowledge about infant feeding could bias these interactions:
My mum, even though she breastfed till 18 months with me and my sister, I think when my son was a couple of months old, she said “oh we’ve got family coming round, family friends coming round, if you want to come round for tea you can but can you just go into the living room if you’re going to feed” and I said “no,” and she said “well we’ll have to go out for a meal with them instead and you won’t be able to come.”
Family and partner attitudes were perceived to be a major contributor to some women stopping human milk feeding before they were ready:
Speaker 1: They put doubt in you, [e.g., my mum] saying “are you sure you are doing it right, she’s just fed, why is she feeding again?” . . . It makes so much of a difference on your success to breastfeeding.Speaker 2: Yeah, because people try and fix things, don’t they? So, you, you know, you go to your mum and you’re tired and when you’re breastfeeding, mums—sometimes their idea is [to] just give them a bottle just to get them to feed, because that’s what they think is the right thing. Whereas mum just wants to tell her mum that she’s just tired and that’s OK.
Solutions to these barriers were proposed, including addressing the lack of public education about human milk feeding and sharing information on other ways family members can bond with the baby. However, there was also a feeling that more research is needed to develop effective solutions:
I would love to hear from families, so like mums, dads, grandparents, . . . what their perceptions are of breastfeeding and what they think is acceptable, to see how that’s then impacting mum, because for some mums that is their only support group, and their mums may have come from a generation of formula.
Theme 4: Media Influence
There was a strong feeling that representations of infant feeding in both print and television media were barriers to human milk feeding normalization. Greater visibility and positivity regarding human milk feeding in popular television shows and adverts was desired:
You still don’t see it anywhere, like, people aren’t having babies on [a soap opera] and then breastfeeding them, they never are like, but why aren’t they? Why can’t they just sit there delivering their line and actually they’ve got a baby in their arms? I don’t understand why it isn’t pushed from different angles. . . . There’s such a thing about inclusivity and making sure that we’re representing different communities, but who is representing breastfeeding mums, like where do you see that?
It was also agreed that more should be done to regulate media portrayals and reduce the visibility of formula resulting from follow-on formula advertising:
Speaker 1: There is no need for three adverts of [formula] to be shown in between [a daytime talk show]. It’s shocking [laughs]. It’s literally on every single advert, like every single break, I don’t want to see it [laughs].Speaker 2: But that’s, I mean, yeah, primetime, mums on maternity leave watching telly.
Aim 2: Evaluation of the Success of the Event
The post-event surveys illustrated that the biggest event influences were perceived to be raising awareness, making connections, establishing networks, and gaining research experience (Table 5). Qualitative feedback illustrated how the event helped to inform the practice of attendees who were providing infant feeding services: “I am going to think about encouraging pregnant families to [attend] local pre-natal support groups for breastfeeding], to help inform them before their baby arrives, as early education can help debunk some of those myths [about human milk feeding]”; “[I am going to] incorporate [the research findings] as we plan future volunteer peer support training and groups for families.” Additionally, the event established useful networks across the city and beyond: “I made connections with the ladies on my table, sharing our jobs and how we could help one another in the future.”
Feedback from online attendees was positive (“[the best bit was being] able to join online without long travel!”), although some commented that the online discussion format was less engaging than for those who attended in person: “More small group discussion would have been useful for [the] online group. [It] felt like some people just wanted to watch/listen and not join in/share ideas.” “[Making connections was] more difficult due to being online.”
The first author offered follow-up one-to-one meetings to attendees. A charity representative delivering services in Stoke-on-Trent explained how the event highlighted a lack of healthcare professional (HCP) awareness of the support they provided. Attendance helped to raise awareness of their services, resulting in practice change through an increase in HCPs making contact, including some requests from midwives and health visitors to attend support groups to see how they work. This enabled the charity to engage directly with local HCPs to raise awareness of their services and encourage signposting and referral. In addition, 7 months after the event, one participant, with prior experience of formula and expressed-milk bottle feeding, contacted the research team to inform them that they had reached 4 weeks of human milk feeding their newborn and that the workshop had broken down barriers and boosted their confidence to human milk feed in public.
Discussion
This paper reports on the conduct and evaluation of a World Café event and a simultaneous online focus group designed to facilitate knowledge exchange and networking and establish consensus on research and policy priorities for improving human milk feeding support. Several agreed priorities for research and policy were identified: improved education for antenatal care, children and young people, and healthcare professionals; the need for improved infant feeding support through the provision of enhanced funding; and the influence of family members and media representations on human milk feeding uptake, continuation, and maintenance.
Participants agreed that support for human milk feeding is not currently being effectively delivered. It has been argued that investment in such support now would lead to later cost saving as the economic influence of low human milk feeding rates is substantial (Pokhrel et al., 2015). Participants highlighted the need for improved antenatal education, including awareness of the benefits of human milk feeding, challenges that might be encountered, and sources of support. Family Hubs (Department for Education, 2022) represent an opportunity to develop new ways to address this gap in service provision. Consensus was also present in relation to the influence of family and partners on human milk feeding behavior. The whole family approach to support services advocated by the Family Hub initiative may help to counter the negative effect that family and partner attitudes towards human milk feeding may have. However, this can only be achieved if a family-led approach to infant feeding support is incorporated into services, which is dependent on Local Authority decision-making being informed by best practice, as outlined in the WHO and UNICEF’s (2003) global strategy for infant feeding, and the UNICEF UK Baby Friendly Initiative. The impact evaluation for new service development would best incorporate tools to evaluate human milk feeding rates to learn from any successes or challenges.
In line with the WHO and UNICEF’s (2003) global strategy for infant feeding and the UNICEF UK Baby Friendly Initiative, participants also highlighted a need for the inclusion of human milk feeding within school curriculums. This recommendation is yet to be fully realized, and recently, the Royal College of Paediatrics and Child Health renewed a call for breastfeeding to be part of personal, health, and social education within schools to fill knowledge gaps and normalize human milk feeding in the UK (Royal College of Paediatrics and Child Health, 2022). Review evidence suggests that primary and secondary teachers are mostly supportive of including such content within their curriculum, but lack the expertise and time to do this (Singletary et al., 2017).
Another priority was education for healthcare professionals. This finding illustrates that little has changed since Dykes’ (2006) literature review, in which it was highlighted that practitioner education should be a global priority for change. Dykes’ (2006) recommendations included person-centered counseling skills training, involvement of the voluntary sector and peer supporters in health professional training, mentoring for practitioners, post-registration training, and national standards for human milk feeding education. These changes have not been effectively enacted to date. Healthcare professionals are generally motivated to support human milk feeding but may lack practical skills. For example, medical students lack confidence in practical skills to support human milk feeding, such as assisting with latch, despite mostly regarding human milk feeding support as an important part of a doctor’s role (Biggs et al., 2020). It can be argued that UK medical schools are not effectively preparing doctors to support human milk feeding (Biggs et al., 2020). There is clearly a desire for improved education within both schools and medical training, and our participants expressed a consensus that some misinformation was believed to stem from a lack of lived experience of human milk feeding by the healthcare professionals themselves. We therefore agree with Dykes’ (2006) recommendation that reflective practice and the involvement of voluntary and peer support organizations within training would facilitate the integration of embodied and vicarious learning. Research to establish how this can be achieved should be prioritized to inform future interventions.
Formula advertising and promotion remain a challenge for facilitating human milk feeding, and the participants advocated that change is needed. The most effective solution for this would be to incorporate all the WHO international code for the marketing of human milk substitutes (WHO, 1981) into UK law. This would ensure that marketing of human milk substitutes is prevented, supporting a cultural shift towards normalizing human milk feeding. Campaigns to prompt consideration of this change in policy are urgently needed.
The use of World Café to explore human milk feeding research and policy priorities has proved to be a valuable tool. Clear priorities for future research and policymaking were established based on a wide range of stakeholder views. These priorities fit with past research and align with international human milk feeding initiatives and guidance. The post-event surveys and discussions identified how participation directly benefited attendees through new knowledge to incorporate into service provision, directly supporting human milk feeding for at least one attendee, and through establishing new network links, both raising awareness of existing services and providing avenues for future collaboration. While the inclusion of online participation helped to widen participation and support nationwide attendance, the networking and shared learning elements were less effective, with participants feeling that they had missed out. Despite this, the event encouraged networking and established group consensus regarding human milk feeding priorities.
Limitations
In a World Café setting, participants discuss their thoughts with a wide range and number of people and it is possible that concerns over confidentiality or feeling comfortable voicing their opinions may have created barriers to full discussion (Page, 2023). In addition, participants were all intrinsically motivated to voluntarily attend an event to improve human milk feeding and the sample lacked diversity, particularly in terms of ethnicity. This may mean that dissenting views, which may be held by a broader demographic, could have been absent from the findings. The nature of a World Café and the rotation of participants throughout groups limits the possibility of tracking which attendees are quoted in the findings. While the authors have taken care to present examples from a range of participants across the discussion groups, this may be considered a limitation. Furthermore, we relied on self-selection and recruited our participants using advertisements placed on social media. Further advertising, and more targeted invitations to attend, may have broadened the characteristics of our sample.
There was a large dropout from the initial survey to attendance at the event. This is likely to be due to the difference in time commitment between the completion of a survey and attendance at a World Café. Many of our participants were working age and the event was held during work hours, which is a potential limitation. However, those who did attend were a representative sample when compared to those who completed the survey (Table 2). In addition, we included the contributions of all survey respondents in our opening presentation, meaning that these voices were able to be part of the conversation. We did not seek reasons for nonattendance as this additional data collection was not covered by our ethical approval; this is an important learning point for others to consider as obtaining reasons for non-attendance would be of value for informing the conduct of future World Cafés.
Some of the researchers had lived experience of human milk feeding which participatory researchers advocate reduces power dynamics between researchers and participants and reduces barriers for participants to engage in conversations. Typically, a worldview is achieved by rotations of people to different group discussion tables and through summaries provided to wider delegates from each group discussion after each question has been adequately explored (Brown et al., 2005). This study did not have the World Café whole group summaries following each question and, instead, a follow-up survey approach was chosen to provide opportunity for participants to identify priorities from the discussions. The post-event survey was completed by 12 of the 37 attendees (32%), and therefore, this adaptation to the method may have been limited in effectiveness. However, had a full group discussion taken place it is not anticipated that all attendees would have verbally contributed ideas to develop the consensus statements, so the influence of this change may not be particularly profound. Furthermore, final follow up was conducted at 2 months. Longer-term follow-up would be beneficial to explore change more effectively, and should be a consideration for future research.
Conclusions
This study was the first to apply World Café methodology to lactation research and has established priorities for research and policy, including enhancing education, the need for dedicated funding for human milk feeding support, the need to include family and partners within support provision, and the need to change policy regarding media representations of human milk feeding and infant formula. In addition, World Café proved valuable for facilitating networking, establishing priorities, and bringing about change in relation to human milk feeding support.
Footnotes
Acknowledgements
The authors would like to thank Victoria Riley, Naomi Ellis, Heather Cassidy, and Sarah Dean for their support with the event.
Correction (December 2024):
Article updated online to correct minor textual errors and a citation in the Limitations section.
Author Contributions
Disclosures and Conflicts of Interest
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Since the completion of this project AB has commenced training to become a peer supporter with The Breastfeeding Network. The authors declare no other conflicts of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a Staffordshire University impact funding grant.