
Abstract
Pediatricians need to be knowledgeable to adequately carry out their role in the support of breastfeeding, so assessing their knowledge of breastfeeding is vitally important. There are not English language validated questionnaires for pediatricians in the literature; however, in Spanish and Portuguese, there is the Breastfeeding Knowledge Survey (ECoLa, derived from Encuesta de Conocimientos en Lactancia). Our goal is to translate the ECoLa into English. The original survey consisted of true/false questions, including one with an image of a breastfeeding baby, multiple-choice questions featuring clinical cases, and two open-ended short questions. We used a translation approach that incorporated both forward and backward translations and a multidisciplinary committee to evaluate the translation process. During translation, four Spanish versions and seven English versions were considered prior to consensus approval of the final survey. The intraclass correlation coefficient between the English questionnaire and the original Spanish version was 0.85 (95% CI [0.60, 0.95]). A sample of 51 participants completed the survey, resulting in a Cronbach’s alpha of 0.78 for the English version (95% CI [0.70, 0.86]). The Breastfeeding Knowledge Survey is now accessible under a Creative Commons license, permitting its free re-use.
Key Messages
Currently, there are no validated English-language surveys assessing breastfeeding knowledge among pediatricians.
We translated a Spanish language survey which has been psychometrically tested for reliability and validity into English.
The translated survey is accessible as a Google Form and freely licensed on Creative Commons, offering a validated English instrument for assessing pediatricians’ breastfeeding knowledge.
Background
It is well established that pediatricians play a crucial role in both the initiation and continuation of breastfeeding (Handa & Schanler, 2013); however, to do so they must be well informed. Consequently, there is an interest in assessing pediatricians’ knowledge of breastfeeding. In 1992, Freed et al. (1992) highlighted a deficiency in breastfeeding knowledge among pediatric residents in the United States and suggested that knowledge was affected by personal experiences more than postgraduate training. Similarly, Williams and Hammer (1995) reported a low proportion of correct responses to breastfeeding management questions among pediatric residents in the United States. High self-confidence in the provision of breastfeeding support by pediatricians did not always align with actual breastfeeding knowledge levels in a study by Schanler et al. (1999). More recent studies have corroborated these findings, indicating a persistent lack of breastfeeding knowledge among pediatricians (Al Rifai et al., 2023; Pound et al., 2014; Smale et al., 2006).
In English, breastfeeding knowledge among pediatricians has been gauged using the Periodic Survey of Fellows of the American Academy of Pediatrics (AAP) which has been administered for over 2 decades. One of the strengths of this survey lies in its iterative nature, employing a consistent sampling framework, thus enabling the examination of temporal trends. For example, results demonstrated an enhancement in pediatricians’ breastfeeding knowledge over time in the United States (Feldman-Winter et al., 2017). Curricula to fill the gap in the medical knowledge of breastfeeding have been developed by the AAP (Bunik et al., 2006) and the Academy of Breastfeeding Medicine, “What Every Physician Needs to Know About Breastfeeding” (Feldman-Winter et al., 2010).
Various surveys testing pediatric knowledge of breastfeeding have been used in multiple contexts. For example, the survey conducted by Freed et al. (1995) was employed by Hillenbrand and Larsen (2002) to assess improvement following an educational intervention. The scoring system devised by Brodribb et al. (2008) to gauge the knowledge of Australian doctors was subsequently employed by Brun Barreiro et al. (2022) in Paraguay. However, despite their contributions to breastfeeding research, these surveys have not been validated, thus their theoretical constructs and psychometric properties, such as stability, have not been ensured.
In 2014, a survey developed by Pound et al. (2014) documented knowledge domains, assessed validity, and measured internal consistency; however, this questionnaire had limited reliability. Among the four domains, only one achieved a Cronbach’s alpha of 0.81, while the others scored 0.62, 0.60, and 0.21. Cronbach’s alpha ranks from 0 to 1. Usually values over 0.70 are considered acceptable, while those under 0.60 are considered doubtful, and under 0.50 are considered unacceptable. Despite this limitation, the questionnaire proved useful for measuring breastfeeding knowledge, and served as a foundation for the surveys of Al Rifai et al. (2023) and Esselmont et al. (2018), who combined it with the AAP’s breastfeeding curriculum knowledge test.
The ECoLa (Encuesta de Conocimientos de Lactancia, or Breastfeeding Knowledge Survey; Gómez Fernández-Vegue & Menéndez Orenga, 2015) is a validated survey designed to assess pediatricians’ knowledge of breastfeeding in Spanish. It has also been adapted for use in Portuguese (Frazão et al., 2019) and in Latin American Spanish (Herrera Sterren, 2023). Our goal was to translate the Spanish Breastfeeding Knowledge Survey (ECoLa) into English, making this validated tool accessible to English-speaking pediatricians and researchers.
The Clinical Innovation
We translated the ECoLa survey based on Brislin’s method of forward and backward translations with a modified schema, as depicted in Figure 1. The rationale for this process of forward (to English), and backward (back to Spanish) translation, using independent translators—some with a medical background and others without—was to reveal equivalence or semantic and conceptual conflicts which could be discussed to enhance the translation.
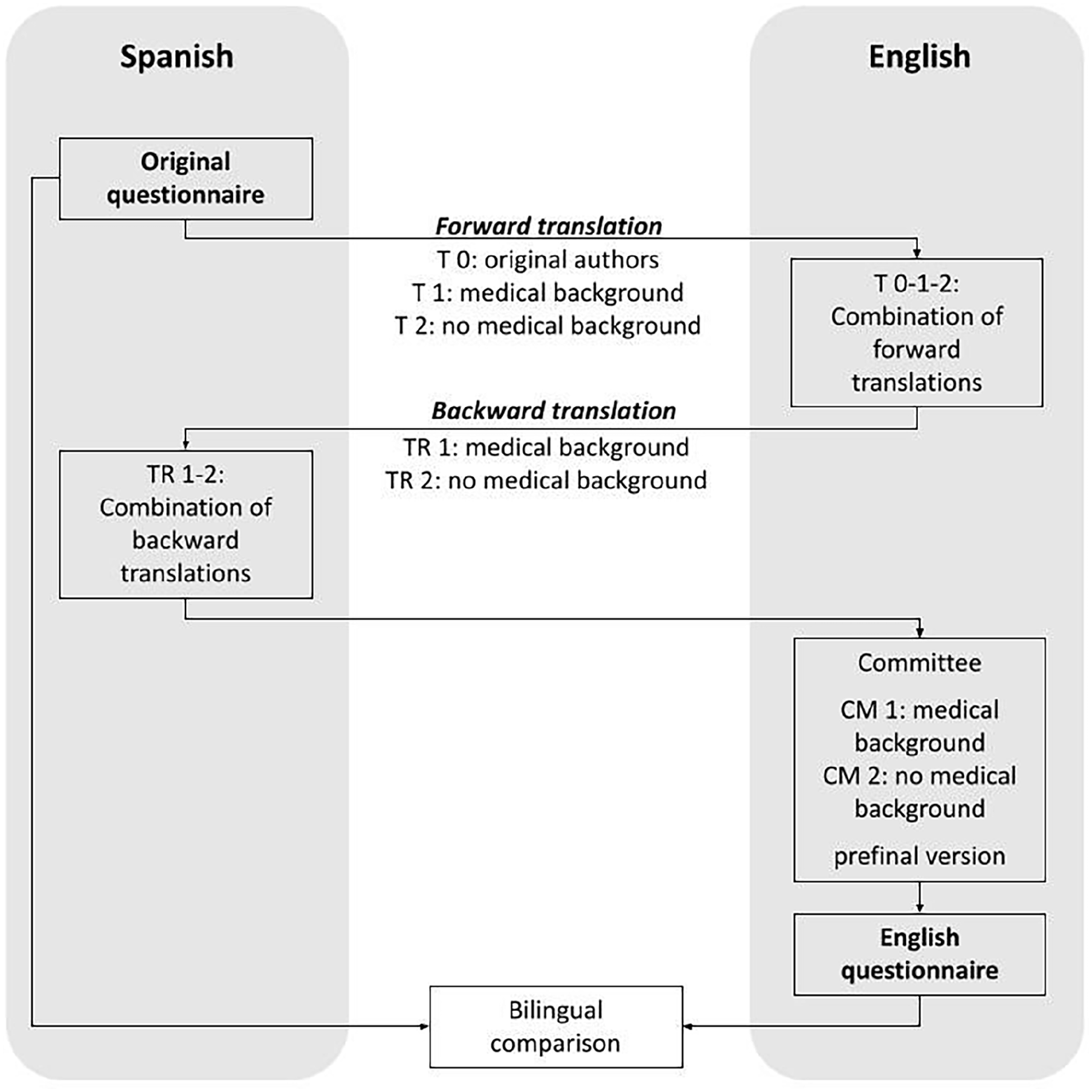
Schema of the Study Process. Schema Depicting the Translation Process From Spanish (Left) to English (Right), Then Back to Spanish, Comparison by a Committee, and Final Bilingual Comparison.
The construct measured by ECoLA is basic breastfeeding knowledge for pediatricians, assessed and judged by 14 breastfeeding experts in the field and delineated into seven areas. Breastfeeding is a multifaceted concept and pediatricians must possess knowledge across various domains or aspects of breastfeeding. The areas covered include physiology, public health, issues related to the early days and later stages of breastfeeding, assessment of latch, maternal factors, and attitudes (Gómez Fernández-Vegue & Menéndez Orenga, 2015). The topic of issues related to the early days and later stages of breastfeeding can be quite broad, including everything from common problems to less frequent and complex issues. To address basic knowledge, this survey focused on information deemed essential for pediatricians rather than covering the full spectrum of breastfeeding knowledge. Following the definitions provided by Yourkavitch and Chetwynd (2019), this survey addressed topics such as human lactation as a physiological phenomenon, breastfeeding intention, breastfeeding initiation, feeding using devices, and, notably, direct breastfeeding and human milk feeding. Additionally, it encompassed questions regarding common lactation-related conditions and the compatibility of maternal medication with breastfeeding.
The ECoLa consists of 14 true/false questions covering all topic areas except attitudes. One of the questions features a picture of a breastfeeding baby, and there are seven multiple-choice questions covering all the topic areas except physiology. Multiple-choice questions include a clinical case representative of common consultations in a pediatric setting, for instance, a consultation about a crying baby experiencing a growth spurt. Additionally, there are two short-answer questions: one prompting respondents to list five criteria for assessing latching, and another asking for a reliable website for checking compatibility of drugs with breastfeeding. For each correct answer and each latching assessment criterion, the surveyed person scores one point, up to a maximum of 26 points, which is equivalent to 100%. We suggest using the percentage of correct answers instead of the absolute number of correct answers because we find it more intuitive to say 50% correct answers than 13 points. This survey has been reported to take an average of 12 minutes to complete in its Spanish version (Olvera-Álvarez et al., 2022).
The comparison between the original and forward–backward translated versions was conducted by a committee consisting of a coordinating translator, an English philologist, and three clinical researchers, including two Spanish natives who were the original creators of the ECoLa, and one English native. Committee members were tasked with evaluating each item and selecting from the options “No mistake/Nuances/Mistake,” while also identifying any differences observed. Any item labeled as “Mistake” by a committee member was regarded as a possible source of misunderstanding, this item underwent thorough examination and discussion within the committee prior to generating a pre-final consensus version. For instance, in one item, the term “drug information sheet” was translated as “prospect” during the forward and backward translations. This mistake was traced back to the first translator without clinical background, and it went unnoticed by the philologist merging the translations, as well as by the language professionals on the committee. Once they received an explanation about the term “drug information sheet,” a consensus was reached.
Two additional English translations were suggested by committee members, one with a medical background and one without, both of whom had access to all versions. During the committee meeting, a final version was agreed upon through consensus. In total, four Spanish versions (including the original) and seven English versions were considered throughout the process. Detailed documentation was maintained for each step of the translation process, including tracking possible sources of misunderstanding identified by committee members. The final English survey was tested by administering it to a convenience sample of 13 bilingual participants, and later in Spanish with a time difference of 1–2 weeks to assess agreement between the original and translated questionnaires. The Intraclass Correlation Coefficient was 0.85 (95% CI [0.60, 0.95]).
Survey Usage
To explore the survey’s application, we surveyed via email a convenience sample of 51 English speaking participants in the United States. The survey was administered using a Google Form.
In our sample, the median percentage of correct answers (see the online Supplemental Material for the correct answers) was 62% (interquartile range [IQR] 50, 77). In this sample, 27.4% of participants achieved 70% of correct answers, and 72.5% did not reach this threshold. Typically, the survey score is analyzed alongside another variable of interest to assess its correlation with breastfeeding knowledge. This variable could include the participant’s facility, allowing for the identification of facilities with poorly implemented breastfeeding curricula, or attendance at a breastfeeding training course to evaluate participants’ improvement in breastfeeding knowledge.
To simplify assessing the results of the full survey, Questions 18 and 21 can be omitted to create a shortened version, thus simplifying data management, as these questions require short free-text answers. In our sample, without these two questions, the median percentage of correct answers was 65%, (IQR 53, 75). A higher percentage of 39.2% of participants achieved 70% or more correct answers, while 60.8% did not reach this threshold. In Figure 2 we included the scoring of both the complete and reduced versions of the survey. Internal consistency was assessed, yielding a Cronbach’s alpha of 0.78 (95% CI [0.70, 0.86]) for the complete version of the survey. In the shortened version, Cronbachs’s alpha was 0.65 (95% CI [0.52, 0.79]).
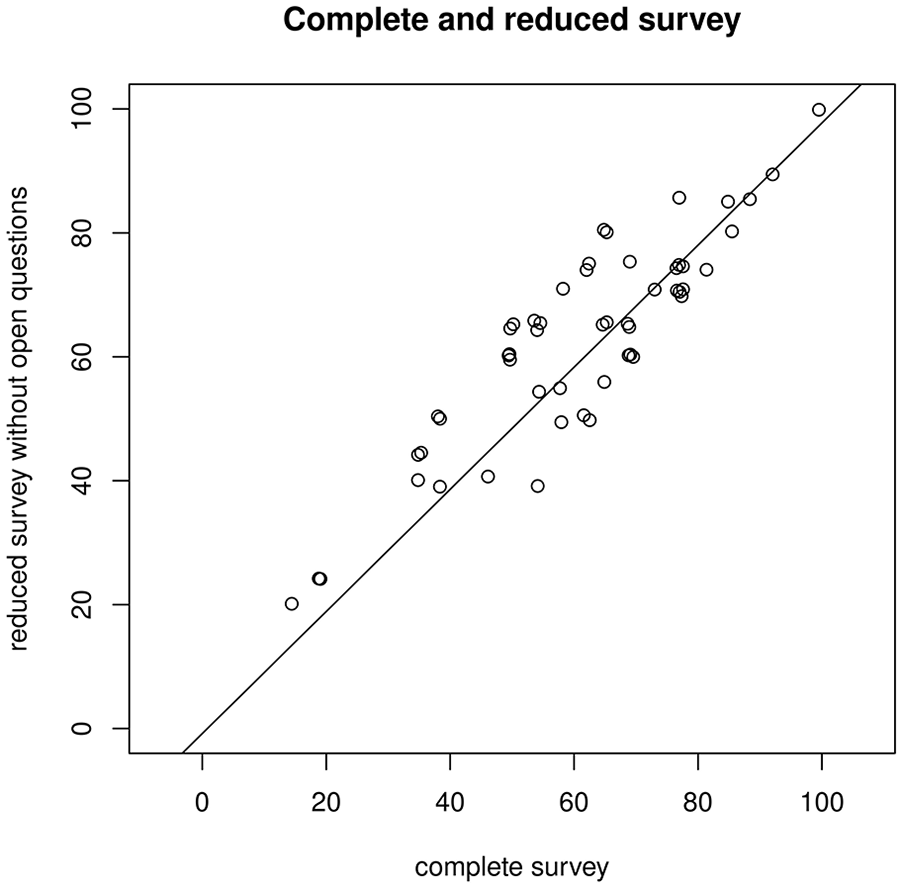
Complete and Reduced Survey. Dotchart Displaying Each Participant’s Scores in Both the Complete and Reduced Versions of the Survey.
Limitations
Limitations of the English version stem from weaknesses inherent in the original Spanish version. For example, the original survey did not assess communication skills or attitudes towards breastfeeding. Other tools, such the Iowa Infant Feeding Attitudes Scale, could be employed for these purposes. The survey also focuses on a basic knowledge of breastfeeding for pediatricians. As a result, it may not be suitable for differentiating among individuals with higher skill levels. The psychometric properties of the English version were not thoroughly assessed; only internal consistency was measured using Cronbach’s alpha. It is important to note that psychometric properties can be sample-specific, and thus a more comprehensive evaluation would be beneficial.
Implications for Practice
Validated surveys can serve as a convenient tool for comparisons with other regions, offering valuable insights. Breastfeeding knowledge, as measured with the questionnaire, is a numeric continuous variable. Researchers or teachers may be interested in categorizing it into different categories. Typically, these categories are set as follows: ≥ 85% excellent, 70%–84% good, 55%–69% poor, and < 55% very poor. For instance, Mexico has a low breastfeeding rate of 33.6% of exclusive breastfeeding at 6 months (González-Castell et al., 2023) and limited social support for breastfeeding (Luna et al., 2021). When the ECoLa was administered in this country to 478 health workers Olvera-Álvarez et al. found that 48.8% of the 86 pediatricians scored 70% or more with this survey (a good score; Olvera-Álvarez et al., 2022). In contrast, in Spain, a good score was achieved by 57% of pediatric resident participants when a nationally representative sample of 177 participants was surveyed (Gómez Fernández-Vegue & Menéndez Orenga, 2019). Notably, in Mexico, 26.7% of the pediatricians who participated in the study answered less than 55% of the questions correctly (a very low score). In contrast, 12% of the pediatricians who participated in the study conducted in Spain answered less than 55% correctly. In Spain, instances of very low scores in breastfeeding knowledge were predominantly found in hospitals where breastfeeding training was not formally implemented, whereas very low scores were nearly nonexistent in hospitals with a structured breastfeeding curriculum (Gómez Fernández-Vegue & Menéndez Orenga, 2019). Various studies have reported low scores in breastfeeding knowledge among family physicians in Mexico, with 51% to 58% of participants failing to answer 55% of the answers correctly (Olvera-Álvarez et al., 2022; Rangel-Junquera et al., 2023; Trujillo-Martínez et al., 2022).
In Brazil, a study surveyed all 454 enrolled students at the Faculty of Medicine of Alagoas, with 205 respondents, final-year medical students answered a mean of 67% of the questions correctly (Frazão et al., 2019). These results suggest room for improvement in breastfeeding education.
In Brazil, a clear difference in breastfeeding knowledge was identified before and after the formative period in the maternity ward. Scores in the first formative years, prior to this maternity ward rotation, ranged from a mean of 39% to 45% correct answers. These scores increased to a mean of correct answers ranging from 61% to 67% afterward the rotation was completed. (Frazão et al., 2019). Similarly, in Spain, residents who received specific breastfeeding training achieved a median score of 80.8% correct answers, which was clearly higher than the median of 57.7% for those who did not receive it (Gómez Fernández-Vegue & Menéndez Orenga, 2019).
Physicians who are less knowledgeable about breastfeeding may not perceive the need for training (Wallace & Kosmala-Anderson, 2006), or they may view tasks such as assessing a latch as relatively unimportant (Baerg et al., 2021). Relying on ill-prepared pediatricians to seek training on their own is not an optimal strategy. Implementing a screening pro-cess for educational needs may be a more appropriate approach until standardized breastfeeding curricula are fully integrated.
Conclusions
An English version of the Breastfeeding Knowledge survey designed to assess breastfeeding knowledge among pediatricians has been released under a Creative Commons 4.0 Attribution – Share Alike license, eliminating the need for formal permission from the authors. To our knowledge, it shows the most robust psychometric properties of available breastfeeding knowledge surveys tailored for pediatricians. It is applicable across a linguistic spectrum including English, Portuguese, European Spanish, and Latin American Spanish, that enables researchers to compare findings across regions.
Supplemental Material
sj-docx-1-jhl-10.1177_08903344241254344 – Supplemental material for English Translation of the Breastfeeding Knowledge Survey for Pediatricians
Supplemental material, sj-docx-1-jhl-10.1177_08903344241254344 for English Translation of the Breastfeeding Knowledge Survey for Pediatricians by Miguel Menéndez Orenga, Daniel Porter and Marta Gómez Fernández-Vegue-Vegue in Journal of Human Lactation
Supplemental Material
sj-docx-2-jhl-10.1177_08903344241254344 – Supplemental material for English Translation of the Breastfeeding Knowledge Survey for Pediatricians
Supplemental material, sj-docx-2-jhl-10.1177_08903344241254344 for English Translation of the Breastfeeding Knowledge Survey for Pediatricians by Miguel Menéndez Orenga, Daniel Porter and Marta Gómez Fernández-Vegue in Journal of Human Lactation
Footnotes
Acknowledgements
We thank English teacher, César Muñoz, for his help with translating the questionnaire.
Authorship Contribution Statement
MMO: Conceptualizaition, Methodology, Investigation, Formal analysis, Writing - Original Draft, Project administration.
MGFV: Conceptualization, Methodology, Writing - Review & Editing, Project Administration.
DP: Investigation, Writing - Review & Editing.
Disclosures and Conflicts of Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplementary Material may be found in the “Supplemental material" tab in the online version of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.