
Abstract
Background:
Breastfeeding continuation rates are low in Ireland. The Breastfeeding Observation and Assessment Tool (BOAT) was developed to assist public health nurses in assessing breastfeeding challenges; however, little is known of its actual usage, the level of training experienced or desired by public health nurses, or their level of confidence in the support they provide to breastfeeding mothers.
Research Aim:
To identify the current practices and support needs of public health nurses who provide breastfeeding support in Ireland.
Method:
An online questionnaire was devised to collect respondents’ confidence with breastfeeding issues, caseload, and practices. It was distributed to public health nurses with a current child health caseload in one Community Healthcare Organization. Mann Whitney U tests were used to ascertain the relationship between public health nurses’ confidence level and those with qualifications in midwifery or as an International Board Certified Lactation Consultant (IBCLC).
Results:
The survey was completed by 66 public health nurses. Only 14 respondents (21.2%) indicated that they always used the BOAT. The most common reason for not doing so was a lack of education on its use (n = 17, 25.8%). Postholders also certified as IBCLCs were considered by participants to be the most appropriate professionals to resolve certain breastfeeding issues. Confidence levels to manage breastfeeding issues were highest among public health nurses with IBCLC credentialing (U = 12.5, p = .001) while no difference was seen when comparing those with a midwifery degree to those without (U = 184.0, p = .92). Face-to-face workshops and blended-learning approaches were ranked as the preferred formats for breastfeeding education (Median rank = 2).
Conclusions:
Breastfeeding education incorporating a face-to-face component is needed to support public health nurses who work with breastfeeding mothers, as is prioritization of recruitment in the community of public health nurses with IBCLC credentials.
Key Messages
The practice patterns and needs of public health nurses tasked with supporting breastfeeding clients in Ireland in the postpartum period are unknown.
A standardized assessment tool introduced in 2018 was consistently used by a minority of nurses at first postnatal visits. The reason most commonly given was a reported lack of education on its use.
Public health nurses with International Board-Certified Lactation Consultant credentials were considered the appropriate professional to support clients with breastfeeding challenges.
Resources identified by the public health nurses to support their work with breastfeeding mothers were: (1) dedicated public health nurses with International Board-Certified Lactation Consultant training and, (2) breastfeeding education incorporating a face-to-face element.
Background
Breastfeeding has health benefits for mother and baby (Rollins et al., 2016) but breastfeeding rates in Ireland are generally lower than the rest of the world (Victora et al., 2016). Although Irish breastfeeding initiation rates improved from about 57% in 2014 (Healthcare Pricing Office, 2016) to approximately 62% in 2020 (Health Service Executive [HSE], 2021b), the World Health Organization (WHO) reported in 2015 that only 15% of infants in Ireland were exclusively breastfed at 6 months of age (WHO, 2015). To address this drop off in breastfeeding rates, the most recent national Irish breastfeeding policy aimed to increase the duration of breastfeeding (HSE, 2016).
Public health nurses (PHNs) provide community care to individuals across the lifespan (Begley et al., 2004). Women after vaginal birth are normally discharged home within 48 hours of delivery. Under the National Healthy Childhood Programme, all mothers in Ireland are offered postnatal home visits from the PHN within 72 hours of discharge from the maternity hospital (Department of Health, 2016). Maternity care and the provision of support by PHNs is free to all parents in Ireland. PHNs are responsible for both the care of the postnatal mother in the community, and childhood development screening, and thus have an important role in identifying children who require early intervention (Children’s Health Ireland & Office of the Nursing and Midwifery Director, 2021; Department of Health, 2022), Mothers value the postnatal support and visits they receive from PHNs (Giltenane et al., 2021) and receiving two or more postnatal PHN visits has been positively associated with any breastfeeding (Leahy-Warren et al., 2014).
To assist midwives and PHNs in assessing women with breastfeeding challenges, the HSE (2018a) developed the Breastfeeding Observation Assessment Tool (BOAT) in 2018. It provides guidance for PHNs and midwives on the observation and assessment of a breastfeed at the first/primary postnatal visit and provides guidance on actions needed to resolve any challenges identified. The tool is composed of comments and questions specific to the maternal–infant dyad and is used during supervision of a breastfeeding mother to facilitate a robust assessment. A traffic light system is used to assess breastfeeding across several indicators. Green represents effective breastfeeding and amber indicates a need for support and the development of a care plan to support breastfeeding. This care plan may include a referral for additional specialist support. PHNs are educated about the use of the BOAT in HSE online modules and a written policy on its use has been produced (HSE, 2018a). However, little is known of its usage in practice.
The importance of breastfeeding training for healthcare professionals has also been recognized in national breastfeeding policy (HSE, 2016). For all PHNs, breastfeeding education is a key component of the Postgraduate Diploma in Public Health Nursing. Furthermore, PHNs have access to face-to-face continuous professional development programs on breastfeeding. In 2019 the HSE additionally developed two mandatory online modules for PHNs on breastfeeding (HSE, 2018b). PHNs can also access external breastfeeding education courses. Some PHNs opt to complete the International Board Certified Lactation Consultant (IBCLC) qualification (Association of Lactation Consultants in Ireland, 2022). In addition, to provide effective support to breastfeeding mothers, PHNs also need confidence in their own skills to do so. In self-assessments, PHNs in Ireland have previously rated themselves as having an overall high degree of confidence and competence in providing breastfeeding support (Mulcahy et al., 2012). Locally available dedicated IBCLC qualified PHN postholders were also highlighted in the national breastfeeding policy as a necessary resource for increasing breastfeeding rates in Ireland (HSE, 2016). However, at the time of writing, not all posts are filled and PHN views of these roles are unknown.
The aim of this study was to identify the current practices and support needs of PHNs who provide breastfeeding support in Ireland. The objectives of this study were: (1) to identify PHN reported usage of the BOAT; (2) to assess whether PHNs confidence in providing breastfeeding support is related to lactation education and training; (3) to identify to whom PHNs refer women with complex breastfeeding challenges; and (4) to identify PHNs’ preferred formats for future breastfeeding education and training.
Method
Research Design
This study used a cross-sectional online questionnaire design. The rationale for the cross-sectional design was that we were predominantly interested in the current breastfeeding support practices of PHNs. Use of an online questionnaire allowed us to reach all potential participants as the study invitation could be shared with eligible PHNs via email. The study received ethical approval from the School of Nursing and Midwifery Ethics Committee, Trinity College, Dublin.
Setting and Relevant Context
This study was conducted in one Community Healthcare Organisation (CHO) in Ireland. There are nine CHOs in Ireland and each one is responsible for delivery of community and primary based healthcare to people residing in their catchment area (HSE, 2014). At the time of questionnaire distribution, rates of exclusive breastfeeding at 3 months in the CHO where the study was conducted were comparable to the national rates (32.0% vs. 31.3%) while rates of any breastfeeding at 3 months were slightly higher (48.2% vs. 41.4%; HSE, 2021a).
Sample
Convenience sampling was used to invite PHNs with a current child health caseload in the CHO where the study was conducted to participate. Of 177 PHNs in the CHO at the time of questionnaire distribution, 66 (37.3%) participated.
Measurements
The questionnaire was developed based on a review of the literature and contained five core sections: (1) demographics, (2) caseload and current practice, (3) confidence in the breastfeeding support scale, (4) unresolved breastfeeding issues, and (5) preferred format for education and training. Supplemental Table 1 outlines the quantitative questions included in the present study, as well as the response types and options for each (see the online supplemental material). Responses to one open-ended question (“Have you any other comments you would like to add about your role as a public health nurse in supporting mothers who wish to and are breastfeeding?”) are also included in this paper.
Section three (confidence in breastfeeding support scale) was based on an adapted version of the Coventry University Breastfeeding Support Self-Efficacy Scale, originally developed by Wallace, et al. (2009) and translated to Mandarin for use in China (Ma et al., 2018). This scale has been used by midwives and health visitors in the United Kingdom (Wallace et al., 2018). It contains six questions on positioning and attachment and two questions on confidence in educating women about hand expression. Additional questions from Whelan et al. (2011) and Mulcahy et al. (2012) on confidence with breastfeeding support were adapted for use in this scale. The final scale contained 23 items and used 5-point Likert scales (1–5) to rate participants’ confidence in providing breastfeeding support. The maximum score was 115.
The HSE (2018a) recommends that PHNs refer mothers with unresolved breastfeeding challenges to other personnel. Participants were asked if they were the appropriate person to manage breastfeeding challenges (e.g recurrent mastitis, babies with tongue tie) or if they would prefer to refer them to an IBCLC PHN postholder.
To mitigate against measurement error bias (Ponto, 2015), eight experts in public health nursing, breastfeeding, and education reviewed the scale in terms of clarity and relevance (Polit et al., 2007). The expert panel rated each item on a scale from 1(not relevant / not clear) to 4 (very relevant / very clear). The proportion of the expert panel who rated the items 3 (relevant / clear) or 4 (very relevant / very clear) was calculated. Items with an Item-Content Validity Index (I-CVI) of < 0.83 for clarity or relevance were modified or deleted by the research team. The Scale-Content Validity Index (S-CVI) was calculated by determining the mean I-CVI for all items in the confidence in breastfeeding support scale. The S-CVI for clarity was 0.96 (SD = 0.08) and the S-CVI for relevance was 0.92 (SD = 0.11). The scale demonstrated internal reliability with a Cronbach's alpha of 0.972. The questionnaire was then pilot tested with 16 PHNs in another CHO and their feedback was used to check the internal reliability of the scale.
Other questions in the survey included PHNs preference for the format of breastfeeding educational programs and their views on what would help them support mothers who wished to breastfeed. The term “mother” was used throughout the questionnaire as this is the term commonly used by PHNs themselves and is in agreement with the HSE (2018a). The study authors acknowledge that not everyone who breast/chest feeds an infant identifies as a mother.
The HSE defines exclusive breastfeeding as “the infant has received only breastmilk from his/her mother, or expressed breastmilk, and no other liquids or solids with the exception of drops or syrups consisting of vitamins, mineral supplements or medicines” (Purdy et al., 2017, p. 11). Partial breastfeeding is defined by the HSE as children “receiving some breastfeeds, and some artificial feeds, either milk or cereal or other foods” (Purdy et al., 2017, p. 11). In this study we defined breastfeeding as exclusive or partial as defined by the HSE and include the process of feeding a mother’s milk to her infant either directly from the breast or by expressing (pumping out) the milk from the breast and bottle feeding it to the infant (WHO, 2018). Although expressed breastmilk may be given in different forms (e.g. tube feeding, cup feeding), expressed breastmilk in this study was defined as providing breastmilk by bottle (Noel-Weiss et al., 2012).
Data Collection
Data collection occurred between October 2020 and December 2020. Administrative staff (secretarial staff supporting Directors of Public Health Nursing) acted as gatekeepers and emailed all PHNs working in the CHO to disseminate information about the study. Only PHNs, who self-identified that they had a maternal and infant health caseload were invited to participate in this study. Data were collected anonymously using Qualtrics, an online data collection platform. The questionnaire was accessible via computer and other electronic devices to allow PHNs to complete the survey at a time and location of their choosing. No identifying information was collected from participants. Internet Protocol addresses, location data, and contact information were not collected. All participants provided electronic anonymous informed consent before taking part in the study.
Data Analysis
Quantitative questionnaire data were analyzed using SPSS (Version 26). Descriptive and frequency statistics were used to characterize the sample and understand the current practice of the PHNs in relation to providing breastfeeding support (breastfeeding observation and use of the BOAT). Total breastfeeding confidence scale scores were calculated out of a maximum possible score of 115. Total mean and median breastfeeding confidence scores and individual item mean scores were also calculated.
Due to the non-normal distribution of the total scores regarding confidence in providing breastfeeding support, Mann Whitney U-tests were used to gain a better understanding of the relationship between having a midwifery or IBCLC qualification and confidence in breastfeeding support. Within responses scoring below the median for breastfeeding confidence, preferred healthcare professional to manage specific breastfeeding issues (“myself as PHN” or “IBCLC PHN postholder”) was compared for all participants in this group, and also for non-IBCLC qualified PHNs. Preferred formats for breastfeeding information were ranked from 1 (most preferred) to 10 (least preferred) and overall median ranks were calculated. Using Microsoft Word, the brief responses provided for the one open-ended question and open-ended reasons given for not always using the BOAT at a first postnatal visit were independently coded into themes by two authors (DC and ÉB). After this step DC and ÉB met to discuss and agree on the final themes.
Results
Less than half of respondents (n = 32, 48.5%) had been registered as a PHN for more than 5 years. The median number of breastfeeding mothers in respondents’ current caseloads was nine (Range 2, 30). Under one-third had a midwifery qualification (n = 21, 31.8%; Table 1) and most held some form of breastfeeding support qualifications or certificate, but few held an IBCLC qualification (Table 1). The majority (n = 44, 71.2%) reported that they had completed breastfeeding education in the last 3 years, of whom 36 (81.8%) reported the education as having been delivered face-to-face and 26 (59.1%) reported it as having been delivered online.
Participants’ Experience and Educational Levels (N = 66).
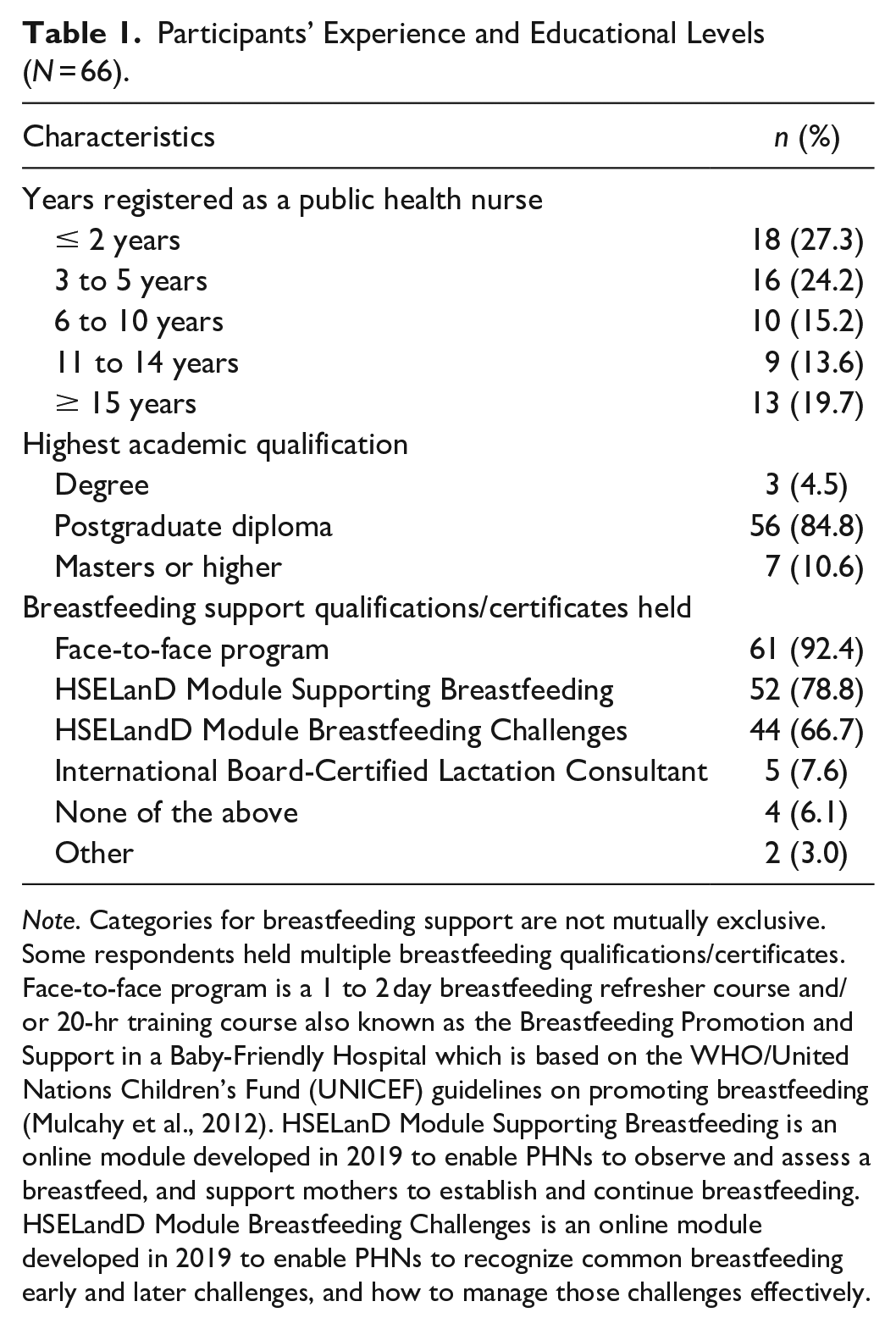
Note. Categories for breastfeeding support are not mutually exclusive. Some respondents held multiple breastfeeding qualifications/certificates. Face-to-face program is a 1 to 2 day breastfeeding refresher course and/or 20-hr training course also known as the Breastfeeding Promotion and Support in a Baby-Friendly Hospital which is based on the WHO/United Nations Children’s Fund (UNICEF) guidelines on promoting breastfeeding (Mulcahy et al., 2012). HSELanD Module Supporting Breastfeeding is an online module developed in 2019 to enable PHNs to observe and assess a breastfeed, and support mothers to establish and continue breastfeeding. HSELandD Module Breastfeeding Challenges is an online module developed in 2019 to enable PHNs to recognize common breastfeeding early and later challenges, and how to manage those challenges effectively.
Breastfeeding Observation and Use of the BOAT
Fifty-five PHNs (83.3%) reported that they always observe mothers breastfeeding at their first postnatal visit. Only 14 PHNs (21.2%) indicated that they always use the BOAT during a first visit and a further 34 (51.5%) sometimes used it during this first visit. The most reported reason for not always using the BOAT was a lack of education on its use (Table 2). Of those who selected “other,” four PHNs clarified that they did use the tool if they had a “breastfeeding issue” (PHN 24), while two explained that they had been unable to “get hold of” (PHN 45) the tool in their area.
Breastfeeding Support Provided by Public Health Nurses Not Routinely Using the Breastfeeding Observation Assessment Tool (BOAT; N = 52).
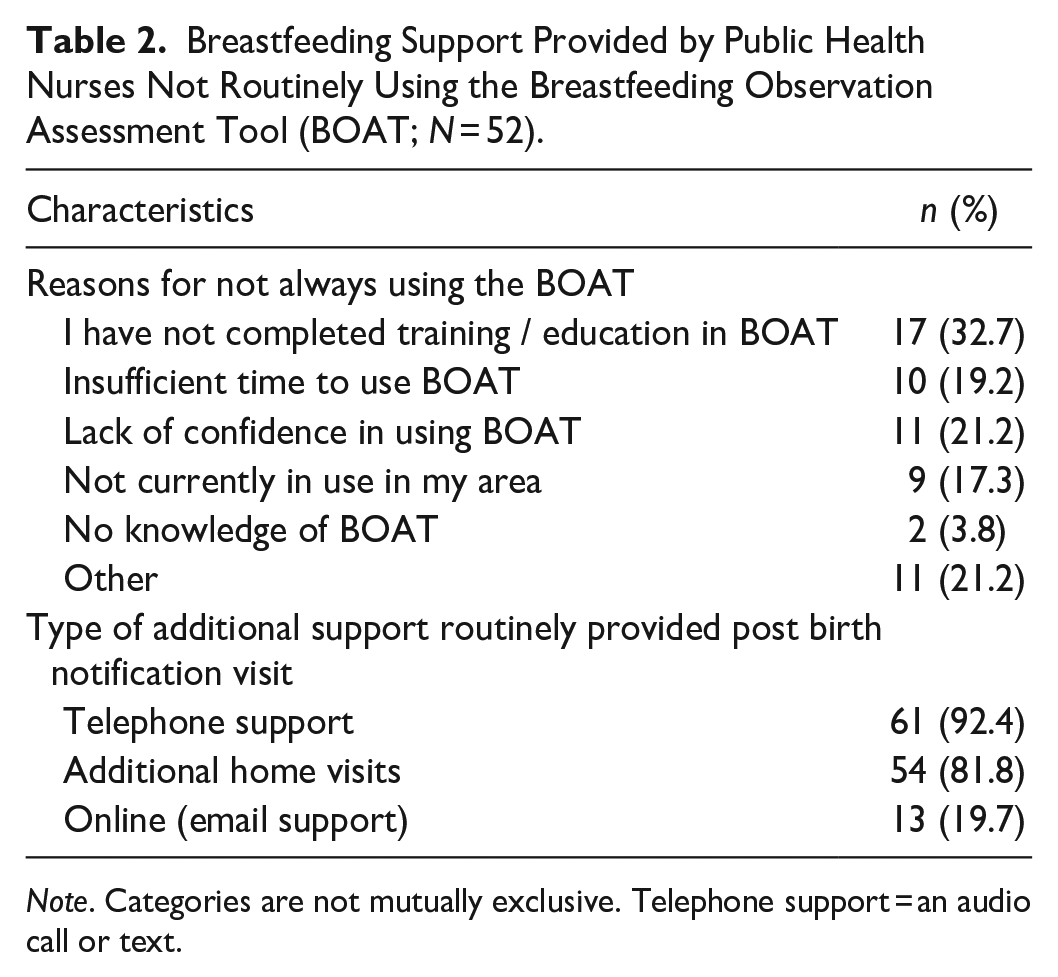
Note. Categories are not mutually exclusive. Telephone support = an audio call or text.
Confidence in Supporting Breastfeeding
Fifty-two (78.8%) participants completed the confidence in breastfeeding support scale. These PHNs had a mean total confidence level of 74.4 (SD = 14.73). There was no statistically significant difference in confidence scores between people who held a midwifery qualification (Mdn = 81.5) and those that didn’t (Mdn = 68.5), U = 184.0, p = .92. On the other hand, PHNs who had completed the IBCLC qualification had statistically significantly higher total confidence levels (Mdn = 101.0) compared to PHNs who had not completed the IBCLC qualification (Mdn = 68.5), U = 12.5, p = .001.
Scores for individual items of the breastfeeding support scale are presented in Supplemental Table 2. Overall, PHNs had higher mean confidence for supporting breastfeeding mothers with attachment and positioning, while mean confidence was low for issues including providing advice on use of breast pumps, tongue tie, pre-term infants or unwell babies, and mothers with a history of breast surgery.
Confidence and Referral to an IBCLC PHN Postholder
Participants were asked to report if they should refer women with a range of unresolved breastfeeding challenges to an IBCLC PHN postholder or manage these scenarios themselves (Figure 1). A majority of PHNs believed that an IBCLC PHN postholder should care for mothers with a history of breast surgery (n = 34, 82.9%), or recurrent mastitis (n = 31, 75.6%), and unresolved nipple pain (n = 29, 70.7%). In contrast, PHNs identified that they, instead of the IBCLC postholder should care for mothers with previous breastfeeding difficulties (n = 27, 64.3%), perceived low milk supply (n = 31, 73.8%), and infants with slow weight gain (n = 33, 80.5%).
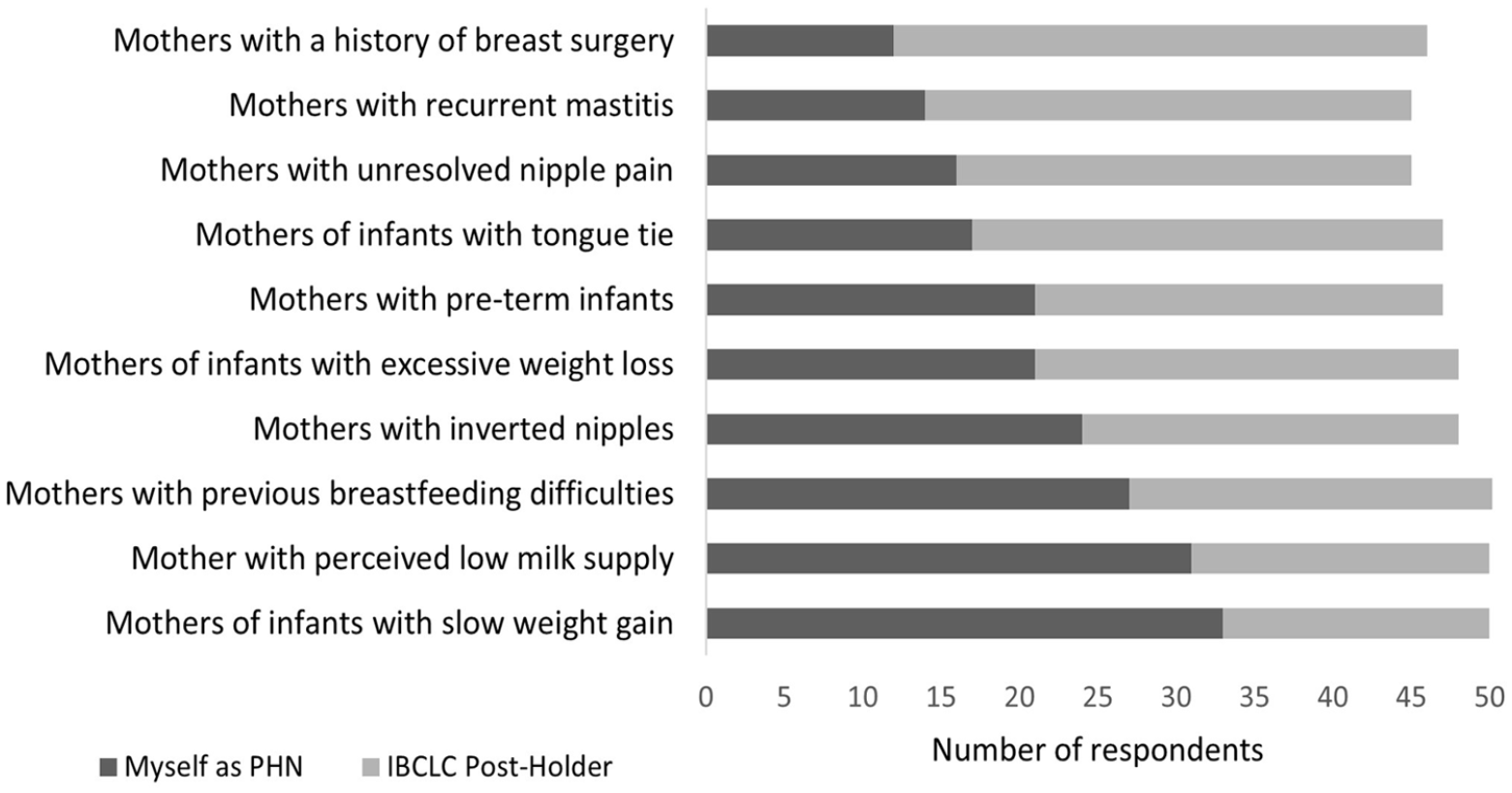
Public Health Nurses’(1) Opinions on the Most Appropriate Professional for Unresolved Breastfeeding Issues.
When responses were restricted to those from PHNs without the IBCLC qualification who had below median total scores (< 68.5) on the breastfeeding support confidence scale, it became apparent that, for many unresolved breastfeeding issues, PHNs with low confidence in providing breastfeeding support more often considered an IBCLC postholder the appropriate professional to provide care in such instances (Figure 2). These PHNs also considered an IBCLC PHN postholder the most appropriate professional to care for mothers with a history of breast surgery (n = 18, 94.7%), and recurrent mastitis (n = 17, 89.5%), but at higher levels than when all the respondents were considered together.
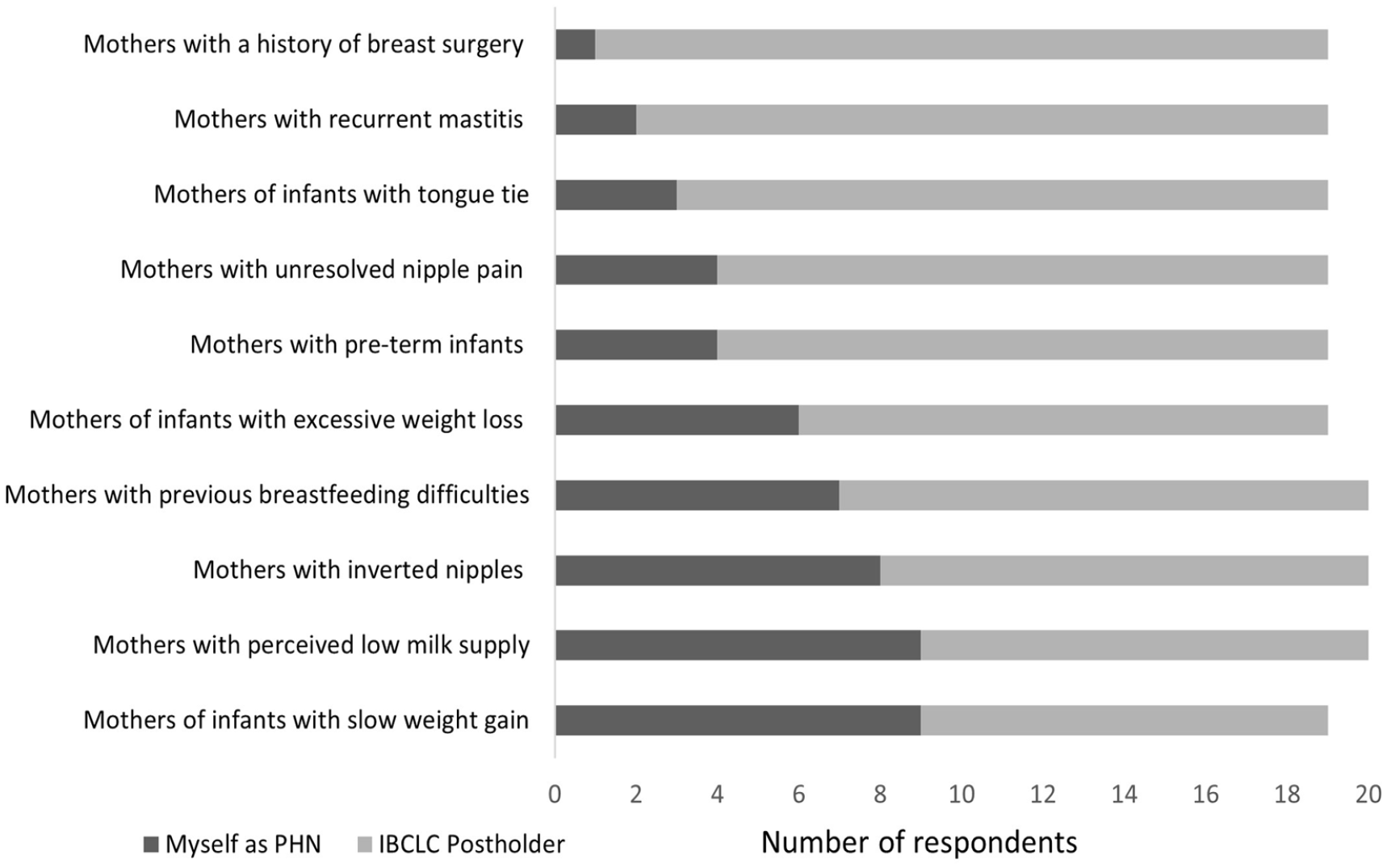
Selections of Public Health Nurses With Low Confidence Scores on the Breastfeeding Support Scale Regarding the Most Appropriate Professional for Unresolved Breastfeeding Issues.
Support Needed to Assist PHNs With Providing Breastfeeding Support
About 60% of PHNs believed face-to-face workshops (n = 40, 60.6%) and mandatory and continuing breastfeeding education and courses (n = 39, 59.1%) would help them to support mothers in breastfeeding (Supplemental Table 3). Almost half considered more time with mothers (n = 32, 48.5%) and peer support from a PHN with an IBCLC qualification (n = 32, 48.5%) important. Very few PHNs wanted peer support from a non-IBCLC qualified PHN (n = 10, 15.2%).
Regarding preferred formats of breastfeeding information, face-to-face skills workshops (Mdn rank = 2), blended learning (Mdn rank = 2), and observation of another PHN colleague experienced with breastfeeding support (Mdn rank = 3) were the highest ranked options (Table 3). Short in-service educational sessions (Mdn rank = 6), local and national breastfeeding policies and guidelines (Mdn rank = 8), and other formats for receiving breastfeeding information (Mdn rank = 10) were the lowest ranked options.
Preferred Formats for Breastfeeding Information (N = 43).
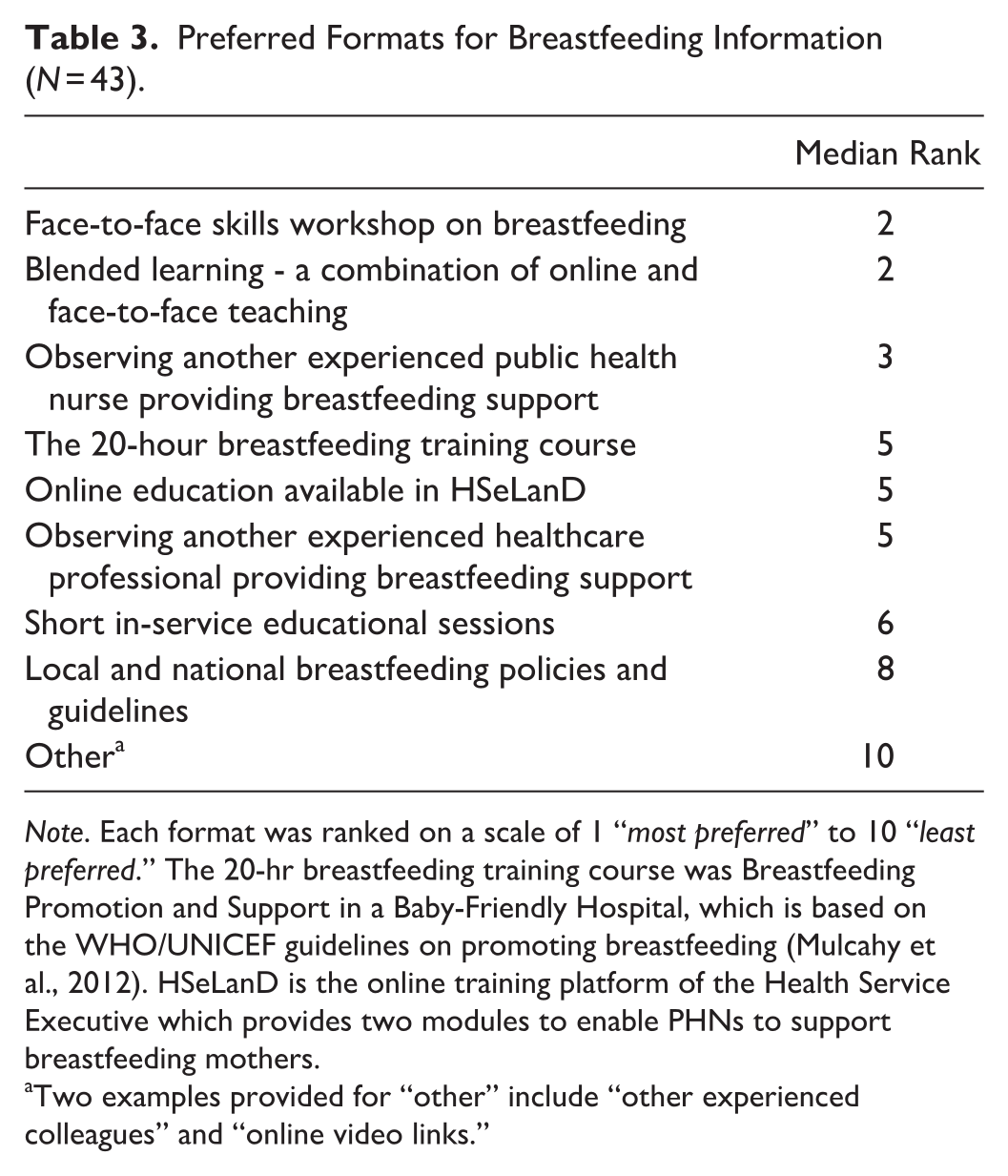
Note. Each format was ranked on a scale of 1 “most preferred” to 10 “least preferred.” The 20-hr breastfeeding training course was Breastfeeding Promotion and Support in a Baby-Friendly Hospital, which is based on the WHO/UNICEF guidelines on promoting breastfeeding (Mulcahy et al., 2012). HSeLanD is the online training platform of the Health Service Executive which provides two modules to enable PHNs to support breastfeeding mothers.
Two examples provided for “other” include “other experienced colleagues” and “online video links.”
Open-Ended Comments
Twenty-four PHNs responded to the open-ended question “Have you any other comments you would like to add about your role as a public health nurse in supporting mothers who wish to and are breastfeeding?” Some responses affirmed that PHNs had an important role in breastfeeding; “the potential to really make or break a woman's breastfeeding journey” (PHN 10). However, there were also comments about barriers that limited the capacity of PHNs to provide this support, for example “caseloads so big we cannot give mothers the time they deserve” (PHN 1). The need for breastfeeding education was also mentioned with one PHN explaining that “I am delighted [to] support these mums in their choice to breastfeed but ongoing education is so essential to support me in my role” (PHN 29). Similarly, the importance of having dedicated PHN IBCLC postholders in the local area was mentioned. As one PHN explained, “not every PHN has the experience or the interest to provide breastfeeding support to mothers” (PHN 10). Respondents also commented on the discrepancies in advice given to parents on breastfeeding from acute maternity services and then primary care services, with one respondent lamenting that “mothers get conflicting advice from everyone” (PHN 17).
Discussion
The aim of this study was to identify current practices and support needs of PHNs who provide support to breastfeeding mothers in one CHO in Ireland. Although many PHNs reported observing a mother breastfeeding at their first postnatal visit, only a minority reported using the BOAT. PHNs who held an IBCLC qualification were more confident in providing breastfeeding support across a range of breastfeeding issues. PHNs considered face-to-face breastfeeding workshops as particularly important in supporting them in their role with breastfeeding mothers.
The PHNs in this study reported high confidence in some aspects of breastfeeding but low confidence in supporting breastfeeding mothers with preterm infants or those with a history of breast surgery. Mulcahy et al. (2012) also identified that PHNs had low levels of competence in supporting mothers who are breastfeeding preterm, as well as unwell babies. In the present study PHNs reported low levels of confidence in supporting mothers who wish to use a breast pump. Some women who completed the National Maternity Experience Survey in 2020 reported that they did not get adequate advice on the use of a breast pump while in the maternity unit (Murphy et al., 2022). Since rates of breast pump usage among mothers are currently unknown in Ireland, as is also the case in the United Kingdom (McInnes et al., 2019), usage rates should be recorded so that breastfeeding education for PHNs can adequately reflect current breastfeeding practices.
Although many PHNs in this study reported observing a mother breastfeeding at their first postnatal visit, only a minority reported always using the BOAT. A recent audit in another CHO found that only 35% of PHNs were using the BOAT at the primary visit but, following receipt of BOAT education, use increased to 91% (Flynn, 2022). The BOAT has been incorporated into Child Health Charts since the study was completed and thus current rates of use may be higher.
PHNs in this study also perceived management of unresolved feeding issues as sometimes going beyond the scope their role. Indeed, some mothers do need a higher level of breastfeeding support that requires input from a lactation specialist, described as “lactation acuity’’ (Mannel, 2011). This is recognized in the BOAT guidelines, which recommend referral of unresolved breastfeeding challenges to a HSE breastfeeding specialist (HSE, 2018a). As other studies have highlighted, an integrated model of support and provision, accessible to women at the right time, can improve breastfeeding (Gallegos et al., 2020; Rollins et al., 2016). In our study, PHNs with an IBCLC qualification reported higher confidence levels in providing breastfeeding support, while non-IBCLC qualified PHNs with lower confidence in providing breastfeeding support tended to view IBCLC postholders as necessary for resolving many breastfeeding issues. Child health caseloads may vary substantially between PHNs, who are generalist providers of community-based care from “cradle to grave” (Begley et al., 2004). There was a substantial range in the number of breastfeeding mothers on respondents’ current caseloads. Consequently, some PHNs may garner more practical experience in providing breastfeeding support than others, depending on the area in which they are based. These results strengthen the case for a clear pathway of referral to a dedicated PHN IBCLC postholder in the community. The HSE stipulates that the IBCLC person employed to support PHNs in their breastfeeding role must be a PHN. An integrated team-based approach could lead to a better support of PHNs and management of breastfeeding problems in the community.
In this study, PHNs placed strong emphasis on the need for face-to-face breastfeeding and/or blended delivery workshops and education to support them in their role with breastfeeding mothers. The HSE is planning on implementing a face-to-face workshop to support the presently offered two online breastfeeding modules. The implementation of these workshops at the local level could focus on the practical and technical skills of breastfeeding. Furthermore, the use of high-fidelity lactation simulation models in conjunction with problem-solving scenarios could also be considered. High-fidelity simulation models have been shown to be very effective in the education of healthcare professionals on technical skills (Hurley et al., 2021) and have been viewed by midwifery students as very useful in learning the psychomotor and technical skills of breastfeeding (Grabowski et al., 2021). The use of simulation models could be beneficial for the continuous professional development of PHNs, especially those who have a small caseload of breastfeeding mothers. Future research should investigate the impact of the planned face-to-face breastfeeding workshops for PHNs and the appointment of dedicated PHN IBCLC postholders on breastfeeding continuation rates and PHN confidence in supporting breastfeeding mothers.
Limitations
The timing of the survey distribution (early during the Covid-19 pandemic) represents a limitation to the study. The pandemic had a major impact on community and public health nursing services in Ireland across the study period with assessments and health promotion often partially conducted over the phone and physical assessments carried out subsequently. This may have limited PHNs’ opportunities to use the BOAT. In addition, there were no dedicated IBCLC PHN postholders in place in the CHO where the study was conducted so an IBCLC-qualified PHN was instead contacted by PHNs for advice and support of complex cases. This PHN also contacted some clients directly to discuss their concerns and met with some clients face-to-face if indicated. Face-to-face education and training for staff was also severely impacted by the pandemic and the lockdown orders across the country. A further limitation was that participants were asked to rank their preferred format of breastfeeding education. The items listed included the formats of education available at the time of data collection and some were not exclusive categories. The study was limited in that the sample was generated from one CHO.
Conclusions
In conclusion, although online education is a flexible and cost-effective means of providing education, PHNs need breastfeeding education that incorporates a face-to-face element to support them in their work with breastfeeding mothers. This should be provided on a regular basis to ensure PHNs remain up to date in their breastfeeding knowledge, including developments like the BOAT. In addition, there is need for prioritization of recruitment of dedicated IBCLC PHN postholders in the community as many PHNs felt that an IBCLC PHN postholder was the appropriate person to provide support to breastfeeding women experiencing a variety of breastfeeding challenges, and IBCLC-qualified PHNs were more confident in providing breastfeeding support than non-IBCLC qualified PHNs.
Supplemental Material
sj-docx-1-jhl-10.1177_08903344231172991 – Supplemental material for The Support Needs and Current Practices of Public Health Nurses in the Republic of Ireland Who Provide Support to Breastfeeding Mothers: A Cross-Sectional Survey
Supplemental material, sj-docx-1-jhl-10.1177_08903344231172991 for The Support Needs and Current Practices of Public Health Nurses in the Republic of Ireland Who Provide Support to Breastfeeding Mothers: A Cross-Sectional Survey by Annemarie Walsh, Rachel McCluskey, Deirdre Cassidy, Gerardine McGoldrick, Claire Howlin, Kathryn Muldoon, Éadaoin Butler and Gobnait Byrne in Journal of Human Lactation
Footnotes
Acknowledgements
The authors wish to thank the following for their assistance with this study: the Health Service Executive Nursing and Midwifery Planning and Development Unit, the survey’s reviewers and pilot testers, the directors of public health nursing and gatekeepers who facilitated access to public health nurse participants, and the participants themselves.
Author Contributions
Disclosures and Conflicts of Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a grant provided by the Health Service Executive, Ireland (Project 10200).
Supplemental Material
Supplementary Material may be found in the “Supplemental material” tab in the online version of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.