
Abstract

Keywords
Key Messages
Simulation-based experiences provided an opportunity for lactation interns to obtain valuable clinical experiences.
Virtual clinical lactation simulation can be a viable method for teaching clinical and communication skills to lactation interns, thus increasing the work force of International Board Certified Lactation Consultants.
Simulation-based experiences allow structured assessment of interns’ clinical skills through a variety of teaching methods and the use of technology.
In March of 2020, most of the United States received “stay at home” orders to decrease the transmission rates of COVID-19. All sectors of life were affected, including lactation education and lactation resources. Many private practice International Board Certified Lactation Consultants (IBCLC) had to pivot their practices to provide telehealth only. The pandemic forced facilities to restrict or deny a student's access to onsite clinical preceptors. Lactation interns were no longer able to complete their clinical hours. In the short term, this prevented interns from graduating, taking the International Board of Lactation Consultant Examiners (IBLCE) exam, and pursuing employment opportunities. The long-term implications are a diminished lactation workforce and reduced access to care for breastfeeding families. This article describes how one West Coast university developed a low-cost virtual simulation program to continue the clinical lactation education of its interns.
Background
In preparation for the start of the Fall 2020 cohort, our university’s lactation department contacted clinical sites for the placement of our incoming interns. It became apparent that facilities were unable to participate in preceptorships due to new protocols implementing COVID-19 restrictions. It was decided to develop and implement a computer-based clinical simulation program focusing on lactation care. Our program concentrated on immersion simulation. This is a real-life depiction of a clinical scenario where the interns’ emotions and senses are involved in their perception of realism (Cant et al., 2019). Simulation-based experiences (SBE) facilitate learning opportunities by reproducing clinical scenarios for the learner to practice as the clinician. SBE provides common and uncommon educational opportunities before in-person settings to enhance clinical preparation. (Diaz et al., 2021; Weston & Zauche, 2021).
Because of their efficacy, SBEs are increasingly used in educational programs to provide clinical skills practice for health care professionals (Diaz et al., 2021; Weston & Zauche, 2021). An advantage of using SBEs as a teaching modality includes the creation of simulation scenarios with specific clinical skills, objectives, and outcomes in mind (Diaz et al., 2021). Virtual simulations create opportunities for inclusivity and educational access in remote and underserved areas. Our program attracts lactation interns from all over the United States, many from areas where few IBCLCs practice. Historically, enrollment was denied if a clinical site was not secured. The barrier of clinical scarcity is mitigated by using SBE. Our program’s Clinical Director partnered with a Certified Healthcare Simulation Educator (CHSE) to review the literature regarding technology-based simulation to prepare for program development. According to Leighton et al. (2021), in-person clinical experiences were not always superior to SBEs in learner outcomes. Based on the evidence reported by researchers in the literature, we felt confident we could develop and implement a quality virtual SBE for our lactation interns.
Our program’s Clinical Director, together with the CHSE Lactation expert, developed clinical simulation scenarios. The CHSE conducted faculty development in simulation education essentials for the Clinical Instructors (CIs) who would be facilitating the SBEs. Guidelines from the International Nursing Association for Clinical Simulation and Learning Standards Committee (INACSLSC; Table 1) were followed to ensure a standardized simulation design. Criteria for simulation design included performing a needs assessment for the SBE, developing necessary and measurable outcomes, maintaining a learner-centered facilitative approach, and designing clinical scenarios with a perception of realism, beginning with a prebriefing, and ending with a debriefing (INACSLSC, 2021). Considering adult learning styles, the program developers referred to Kolb’s experiential learning theory and Brenner’s novice to expert model when constructing the SBEs (Brenner, 1989; Kolb, 1984).
Criteria Necessary to Meet Simulation Standards of Best Practice.
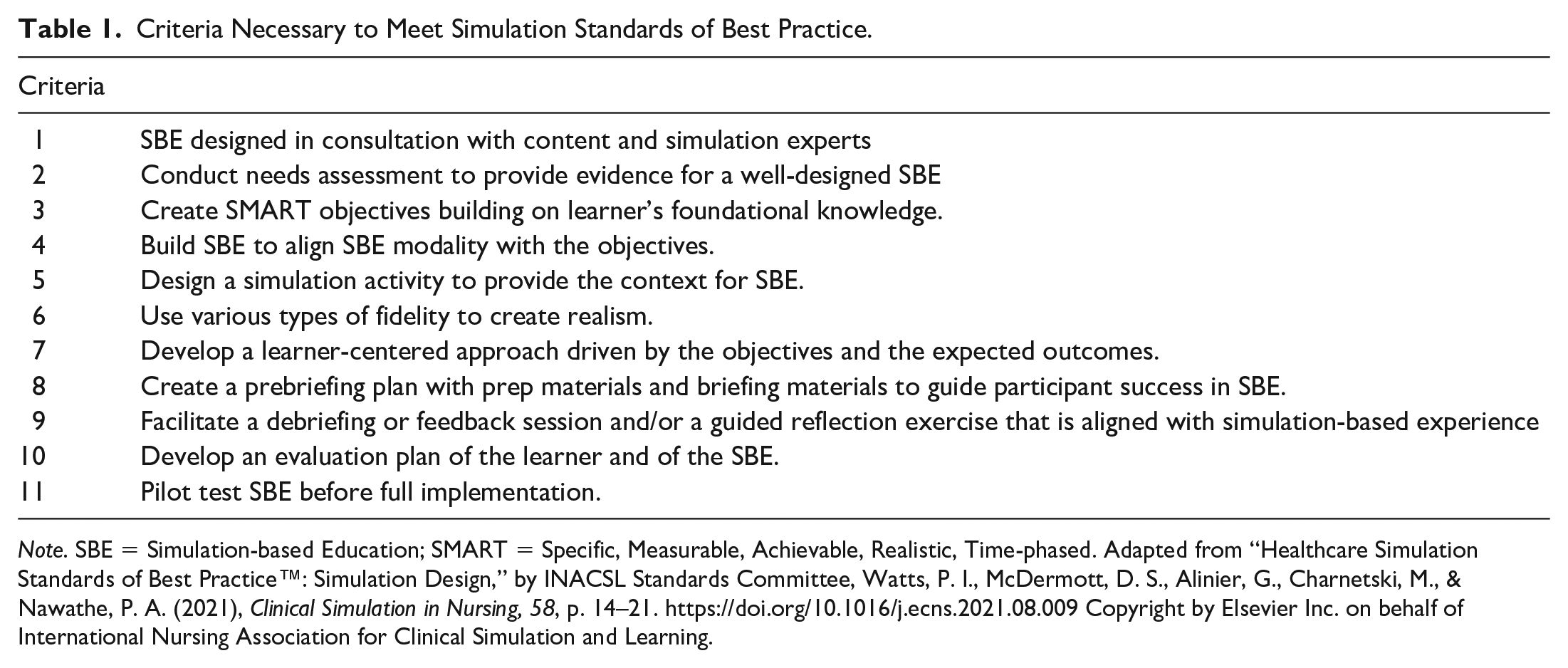
Note. SBE = Simulation-based Education; SMART = Specific, Measurable, Achievable, Realistic, Time-phased. Adapted from “Healthcare Simulation Standards of Best Practice™: Simulation Design,” by INACSL Standards Committee, Watts, P. I., McDermott, D. S., Alinier, G., Charnetski, M., & Nawathe, P. A. (2021), Clinical Simulation in Nursing, 58, p. 14–21. https://doi.org/10.1016/j.ecns.2021.08.009 Copyright by Elsevier Inc. on behalf of International Nursing Association for Clinical Simulation and Learning.
Educational Clinical Innovation
The Lactation Education Accreditation and Approval Review Committee (LEAARC) Clinical Skills Checklist (LEAARC Tracking Competencies, 2016) and the International Board of Lactation Consultant Examiners Blueprint Outline (2016) were used to guide the clinical skills and focused clinical reasoning incorporated into case scenarios. The LEAARC Checklist (2016) provided detailed criteria regarding communication, assessment, and professional development skills. A sample of the LEAARC Checklist can be found in Table 2. Scenarios involved various clinical presentations, including slow weight gain, sore nipples, postpartum psychosis, late-preterm twins, and hyperbilirubinemia. Our interns simulated the “visits” at hospitals, outpatient clinics, and in-home telehealth via ZoomTM meetings. Each clinical scenario was created using the Simulation Design Template created by the National League for Nursing (Alexander et al, 2015; Childs et al., 2007; National League of Nursing Simulation Innovation Resource Center, 2019). The SBE’s utilized Kolb’s (1984) four learning styles: concrete experience (role-play and manual tasks using the simulation kit); reflective observation (weekly self-reflection assignment); abstract conceptualization (using learned concepts from previous weeks); and active experimentation (final proficiency assessment test). As the quarter progressed, so did the complexity of the scenarios. Keeping Brenner’s (1989) novice to expert model in mind, this increase in complexity led to the interns’ progression from novice to advanced beginner by the end of the program.
Sample of the Lactation Education Accreditation and Approval Review Committee (LEAARC) Clinical Skills Checklist Used to Create Our Program’s Simulation Scenarios and the Quality Assurance Peer Review Checklist.
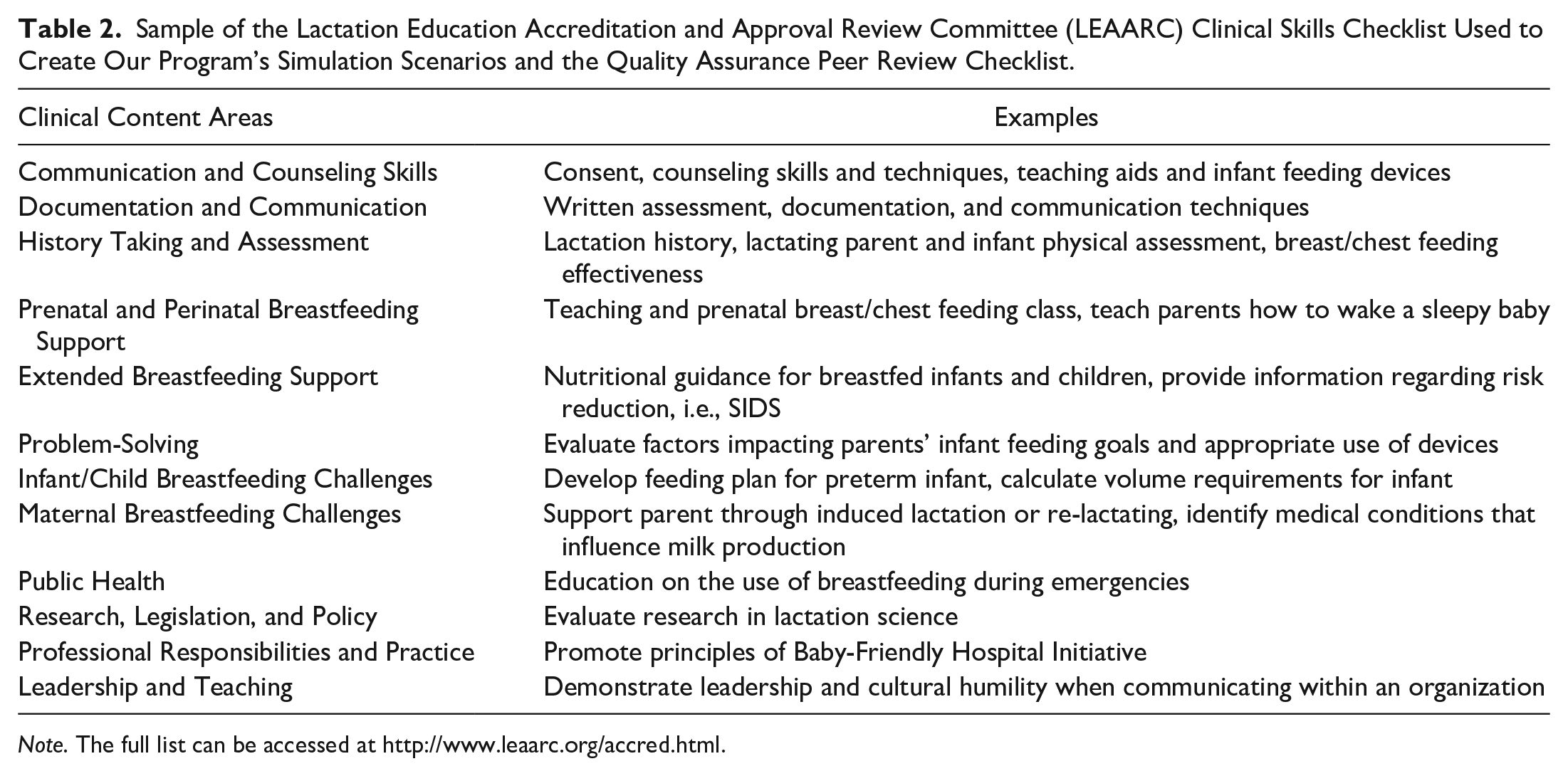
Note. The full list can be accessed at http://www.leaarc.org/accred.html.
Designing a Simulation Experience
Using the NLN template, each scenario was developed to include specific background information on the client. The intern was given the client’s previous chart note using the situation-background-assessment-recommendation (SBAR) format. The SBAR format was selected to encourage focused and relevant communication of pertinent clinical information when providing care (Shahid & Thomas, 2018). Each scenario included a list of expected psychomotor skills required of participants before the simulation, literature to be reviewed in preparation for the simulation, and a list of general objectives and specific clinical actions. The template included the location of the visit and a list of props and moulage needed to create more realism for the lactation visit.
Once the clinical simulation template was completed, scenarios were created in three versions: the Educator, the IBCLC, and the Client versions. Each version provided the intern with specific information unique to the role (Table 3). The Educator version was only available to the clinical instructors.
Simulation Scenario Roles Content.
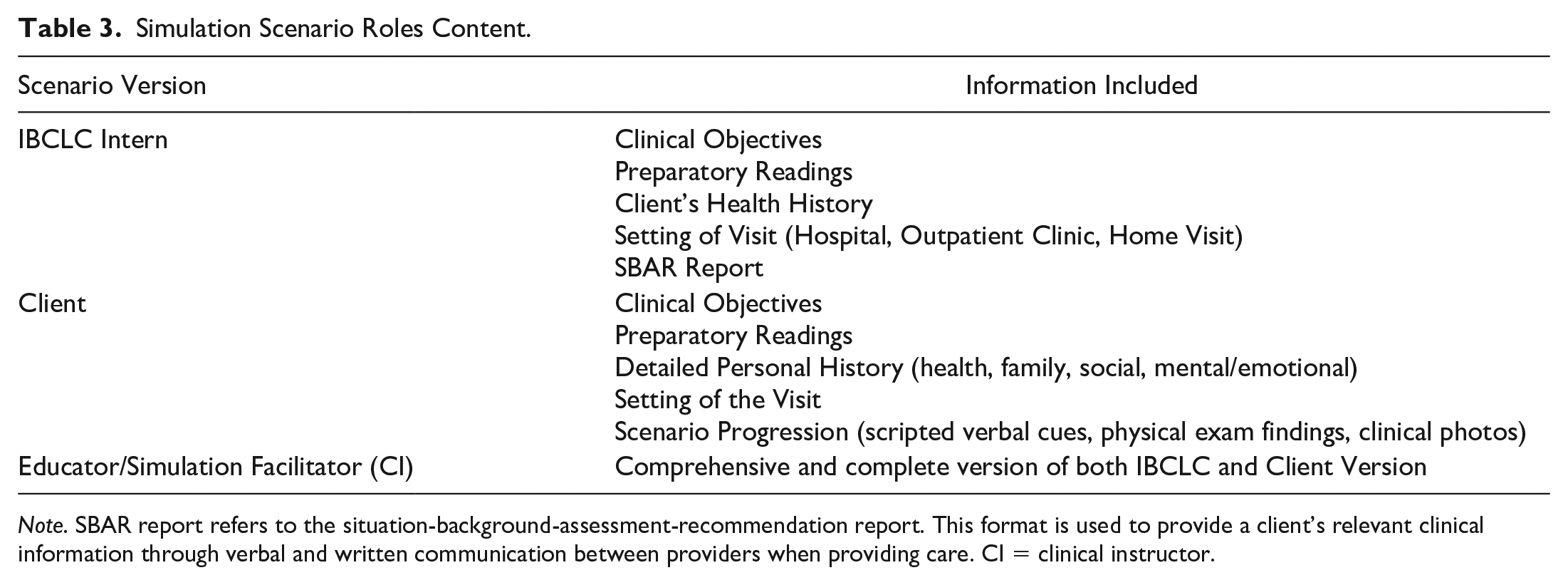
Note. SBAR report refers to the situation-background-assessment-recommendation report. This format is used to provide a client’s relevant clinical information through verbal and written communication between providers when providing care. CI = clinical instructor.
A Scenario Progression Outline was provided in the Client version. This document unfolded the clinical situation and provided the client with scripted verbal cues, physical exam findings, and clinical photos. Clinical photos were used to depict the parent’s breasts, infant presentation, oral anatomy, and breastfeeding observation. The goal in developing specific details for each scenario was to create standardization during the role-play for each group of interns.
After all versions were completed, beta testing was conducted with each scenario using recent alumni to role-play each aspect. Beta testing allows the developers to assess each scenario’s educational quality and realism. Changes necessary to increase the fidelity of the SBE are made before intern participation (Sivakumar et al., 2016). The following aspects were noted during beta testing: the time needed to complete the scenario, if the objectives were attainable, and areas where clarification was needed to achieve realism. Next, Clinical Instructors (CI) with adult teaching experience and IBCLC credentials were hired to facilitate the virtual SBEs. Each CI received core essentials about simulation education and individualized mentoring about providing evidence-based simulation education.
Implementing the Simulation Experience
Orientation for interns was given prior to the first day of simulations. A simulation kit was provided to interns to enhance the clinical experience. It included a 30 ml syringe and a 5 French feeding tube to create a supplemental nursing system (SNS), a nipple shield, and a breast model. Interns provided their own baby doll.
Synchronous virtual simulation labs were scheduled for 8 hr weekly via ZoomTM meetings. Each lab consisted of 12–20 interns. Interns were required to wear a lab coat provided by the program to give a sense of professionalism. The interns accessed the IBCLC and Client versions through the Canvas Learning Management System (Instructure, 2022).
Interns were assigned their role and instructed only to look at their version to allow for a more organic and authentic clinical experience. Interns accepted the responsibility of keeping their roles confidential to enhance the experience. Feedback from the self-reflections suggested that the interns respected this request.
Each simulation started with all participants gathered for a prebriefing session facilitated by the CI. This time was used to reassure interns that the virtual lab was a safe, nonjudgmental place to take chances and that mistakes were celebrated. Interns were reminded that anything discussed in the simulation was confidential and not to be shared with interns in other virtual labs. During the prebrief sessions, the CI and interns reviewed the clinical objectives and the client’s clinical background and discussed approaching the scenario. Once prebrief was concluded, groups of two to four interns transitioned to assigned breakout rooms. The CI supervised breakouts rooms. The CIs made frequent and deliberate visits to each breakout room. By doing so, the CIs were able to assess the learning taking place, similar to how an instructor would observe groups of students working on different manikins at the same time.
In the breakout rooms, interns role-played their given clinical scenarios. If there was a participant without an assigned role, they acted as Quality Assurance Peer Reviewer (QA). The QA used a checklist to ensure that the role of IBCLC was performed safely with appropriate counseling and communication skills, based on the LEAARC Clinical Skills Checklist (LEAARC Tracking competencies, 2016). The CI observed each breakout room with their camera and microphone off to avoid distracting or interrupting the scenario progression. The chat feature was available to all interns if additional support was requested.
Once the interns completed their scenarios, everyone returned to the main room to participate in the debriefing session facilitated by the CI. Our program used the Gather, Analyze, and Summarize (GAS) method for debriefing (Abulebda et al, 2021). During the debriefing session, the Socratic method was implemented to gather the interns’ emotional responses (Alexander et al., 2015). During debriefing sessions, CIs guided the interns by asking each to contemplate areas of strength and areas of growth. At the end of the debriefing, the group summarized what they had learned based on the clinical objectives and experience (INACSLSC, 2016).
The prebrief and debrief sessions are essential to the learner’s simulation experience. The learning that occurs during simulation depends on integrating the experience with the learner’s reflection of the SBE. Reflection forces the learner to view their role in the simulation with a critical eye, strengthening their clinical thinking skills and translating this into improved clinical performance. SBEs are not valuable without debriefing (INACSLSC, 2016). In our SBE, the debrief was an opportunity for the interns to express how they felt in each role and consider how they could improve. During the debrief, the discussion led to an opportunity for the intern to create a plan for self-improvement (Abulebda et al, 2021; INACSLSC, 2016). To emphasize the interns’ reflections, they were expected to submit a written self-reflection and chart note weekly. All assignments were submitted within 72 hr of the virtual lab to have more accurate, detailed reflections.
Lessons Learned
At the beginning of the quarter, interns and instructors were nervous about what to expect in SBE. The program required a leap of faith from all participants. It was a positive endeavor, with lessons learned based on student evaluations and instructor feedback.
The first lesson learned was the need for continued faculty development in clinical simulation. While our faculty were experienced instructors, facilitating simulation was new for them. The CIs met several times during the first quarter to review what was working and what needed improvements. Presented concerns included getting interns comfortable in engaging in role-playing. We recommend that instructors receive more in-depth ongoing training for simulation-based experiences focusing on the pre- and debriefing.
The second lesson was recognition that SBE provided a valuable clinical, educational opportunity. Interns repeatedly described the value of simulation in their self-reflections and communicated feeling prepared for clinical practice. Intern evaluations highlighted the benefit of SBEs’ preparation for specific clinical situations, which they may or may not encounter during in-person internships. The simulation kit succeeded in developing interns’ psychomotor skills and comfort with standard lactation support devices. Throughout the program, simulations were revised based on CI observation and intern evaluations. In addition, a yearly self-study report needs to be submitted to LEAARC, the accrediting body. Based on available data, cohort IBCLE pass rates were consistent with pre-COVID pandemic pass rates.
The third lesson we learned was the potential global impact that simulation education can have on the lactation profession. By educating more IBCLCs, SBEs have the potential to improve public health issues in countries where breastfeeding rates are low. Our program has been contacted by international students interested in pursuing a simulation education due to the lack of IBCLC preceptors in their country.
SBEs can provide equity in lactation education, especially in underserved areas. This is relevant, as securing clinical sites is challenging. Private practice IBCLCs often do not have the volume of clients to provide enough clinical hours. Hospital lactation departments are often reluctant to take interns because they are understaffed or overworked, or their policy precludes them from taking non-nurse interns. We strongly recommend a policy allowing thoughtfully created SBEs to align with Healthcare Simulation Standards of Best Practice (HCSSBP) to complement or replace clinical hours to create equity to lactation education access (INACSLSC, 2021). Other health modalities have accepted that simulation hours can provide learner outcomes that are equal to clinical hours. The National Council of State Boards of Nursing Simulation Study provided evidence that replacing 50% of the clinical hours with simulation hours resulted in similar exam pass rates, clinical competency, and overall readiness for practice (Hayden et al., 2014; Roberts et al., 2019). The authors believe this could be true for lactation education as well. However, total replacement of SBEs for in-person hours might be necessary for those living in areas without IBCLC preceptors. In these cases, an Objective Structured Clinical Examination (OSCE) could be used as a final exam to ensure the intern has achieved the learning objectives (Brown et al., 2010).
Our original limitation—lack of clinical sites due to COVID-19 restrictions—ended up being the inspiration to create this program. Other limitations were a short development period of 6 weeks, a small budget, and low fidelity task trainers. Because this was an unexpected project, there was no budget. The largest cost was curriculum development and faculty salary. Other purchased items included lab coats and simulation kits. The overall startup cost was $258 per intern.
Conclusion
Overall, the SBE was positive for interns and instructors. It allowed continued clinical lactation education when many clinical facilities denied internships. Simulation-based experiences can provide practical training for future IBCLCs. Simulation should be considered a teaching modality for completing at least some of the required clinical hours for the IBLCE exam. Whether in person or virtual, simulations can increase access to lactation education, thus increasing the number of IBCLCs and access to lactation support for communities. Simulation can also create a more standardized clinical education by using the HCSSBP and LEAARC standards as guidelines during the development of SBEs. This standardization of clinical education can expand to global practitioners, elevating the quality of lactation education. The authors recommend simulation to be incorporated into lactation education programs as a viable method of training future IBCLCs globally.
Footnotes
Authors’ Note
Kristina Chamberlain is first author; Carrie Westmoreland Miller is second author. Both are responsible for the development of the concept and the writing and editing of this manuscript.
Author contribution(s)
Disclosures and Conflicts of Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.