
Abstract
Purpose
To assess diet quality and nutrition self-efficacy in pregnant women, the relationship between diet quality and nutrition self-efficacy, and differences in diet quality and self-efficacy when information obtained from health and non-health professionals.
Design
Observational cross-sectional study.
Setting
Online survey.
Sample
Australian pregnant women.
Measures
Australian Eating Survey measured diet quality, Ralf Schwarzer and Britta Renner nutrition self-efficacy scale measured nutrition self-efficacy.
Analysis
Spearman’s correlation measured the association between diet quality and nutrition self-efficacy. Linear regression examined the influence of nutrition self-efficacy on diet quality. T-tests examined differences in diet quality and nutrition self-efficacy scores in groups who did/did not obtain nutrition information from health professionals.
Results
Participants (n = 171) (mean (SD) age 32.5 (3.9) years, 81.9% born in Australia) reported a mean diet quality score of 33.9 (8.7) out of 73 and mean nutrition self-efficacy score of 14.7 (3.7) out of 20. A moderate positive linear relationship was observed between diet quality and nutrition self-efficacy (r s = 0.27, P < .001). Nutrition information was obtained by 88%, most commonly via the internet. Diet quality scores were not significantly different when nutrition information was obtained from health professionals (t(24) = −0.823, P = .32), however, nutrition self-efficacy scores were significantly higher (U = 856, z = 2.18, P = .03).
Conclusion
Pregnant women report poor diet quality. Improving nutrition self-efficacy may be effective for improving diet quality. Evidence-based nutrition information should be accessible via the internet and promoted by health authorities.
Keywords
Purpose
During pregnancy, the consumption of a high-quality diet that meets energy and nutrient requirements is needed to support foetal growth and development, reduce the risk of birth defects, achieve healthy weight gain, and reduce pregnancy and birth complications.1-4 Diet quality can be defined as “the nutritional adequacy of an individual’s dietary pattern and how closely this aligns with national dietary guidelines” 5 and can be measured via diet quality indices which provide an overall diet quality score. 6 In previous studies in pregnant women, dietary assessment has mostly focused on intake of individual nutrients or types of foods, rather than on overall diet quality.7,8 This is not without merit, given that consuming single nutrients in appropriate amounts assists in the prevention of certain nutrient deficiencies and abnormalities, for example folic acid consumption to prevent neural tube defects. 9 In reality though, nutrients are not consumed in isolation, but rather as foods and beverages, eaten in combinations to form meals. As nutrients have been shown to act synergistically when consumed together, ie, they demonstrate a cumulative impact on the human body, 9 assessing the diet as a whole and evaluating the diet quality of pregnant women is important to quantify the risk of adverse health outcomes for themselves and their offspring. 5
The ‘Nutrition self-efficacy’ concept was developed from Albert Bandura’s concept of self-efficacy. It describes the belief in achieving nutritional goals set for oneself, and the ability to use this information,10,11 such as following healthy eating patterns and choosing foods that are nutritionally beneficial. There are many intrapersonal, interpersonal and environmental factors that can influence dietary behaviours, of which nutrition self-efficacy is considered one. 12 Higher nutrition self-efficacy during pregnancy may correlate with higher diet quality, but currently there is limited research regarding the relationship between nutrition self-efficacy and maternal diet quality. A 2014 study in the United States with 75 women who had previously been pregnant, with gestational diabetes, reported that higher self-efficacy was significantly associated with higher diet quality. 12 Other studies that have investigated maternal self-efficacy have examined this construct in relation to their child’s diet quality and dietary intake.13-15 More broadly, the relationship between self-efficacy and diet quality has been investigated in young adults, and found to be significant. 16 To the best of our knowledge, there is no study on the assessment of the relationship between nutrition self-efficacy and diet quality in pregnant women. This relationship in contemporary pregnant women is important to elucidate, as improving nutrition self-efficacy may be an effective strategy for improving pregnant women’s overall diet quality.
For health promotion to be effective, high-quality and accurate information is imperative. Nutrition information provided to women from health professionals throughout their pregnancy has the potential to mediate higher nutrition self-efficacy which then may correlate with a higher diet quality during pregnancy. 17 Information presented through digital channels, including social media, smartphone applications and the internet, can be inaccurate and/or of poor quality, and may have negative implications on women’s nutrition knowledge and diet quality.18-20 For example, a study which evaluated the quality and accuracy of nutrition-related information posted by popular Australian Instagram accounts reported that the information is often inaccurate and of sub-optimal quality and suggested that the public should be sceptical of the credibility. 21 Knowledge on the most common sources pregnant women use to obtain nutrition information could inform future health promotion initiatives and positively influence diet quality in this population. Therefore, research is warranted in contemporary pregnant women.
To the best of our knowledge, no research has investigated the relationship between diet quality, nutrition self-efficacy, and sources used to obtain pregnancy nutrition information in pregnant women. The objectives of this study were to, (1) Assess the diet quality, dietary intake and nutrition self-efficacy in a contemporary sample of Australian pregnant women, (2) Assess the relationship between diet quality and nutrition self-efficacy in the sample, and (3) Assess the pregnant women’s sources of pregnancy nutrition information and evaluate differences in diet quality and nutrition self-efficacy scores in women who obtained nutrition information from health professionals and women who did not. We hypothesised that pregnant women who have a higher nutrition self-efficacy score will have a higher diet quality score, and a significant difference will be observed in nutrition self-efficacy scores and diet quality scores in pregnant women who received nutrition information from health professionals, relative to pregnant women who did not.
Methods
Study Design
The current study is a primary data analysis of an observational cross-sectional study. Ethics approval was granted by the Human Research Ethics Committee of the University of Newcastle (H-2023-0225). All participants provided informed consent to participate. Reporting of this study adheres to the Strengthening the Reporting of Observational Studies in Epidemiology - Nutritional Epidemiology (STROBE-nut) guidelines (Supplemental Table 1). 22
Sample and Recruitment
Participants were eligible to participate if they reported being pregnant, ≥18 years of age, and resided in Australia. Participants were recruited September to December 2023 from across Australia, primarily via sponsored Facebook advertisements. The study was also promoted to participants via social media posts and the Hunter Medical Research Institute (HMRI) website. Participants were incentivised to participate by having the opportunity to enter a draw to win a gift card at Baby Bunting.
Measures
Data were collected via a 171-item online survey hosted on the QuestionPro platform (Version 13, QuestionPro Inc, Austin Texas).
Diet Quality
Diet quality was assessed using the Australian Recommended Food Score (ARFS), a food-based diet quality score calculated as a single continuous variable based on responses to a food frequency questionnaire (FFQ). 5 The ARFS measures dietary variety within core food groups recommended in the Australian Guide to Healthy Eating (AGHE), 23 and was derived from a subset of 70 questions from the Australian Eating Survey (AES). The ARFS includes eight sub-scales, of which 20 questions relate to vegetables, 12 to fruit, 12 to breads and cereals, 10 to dairy foods, seven to meat, six to meat alternatives, two to spreads/sauces and one to water. Most food items are awarded one point for a consumption frequency of once per week or more, with exception of red meat and some dairy foods (eg, ice-cream, frozen yoghurt), where a limit is applied for higher intakes as they are associated with higher saturated fat intake and disease risk. For these foods, zero points are awarded for a higher frequency of consumption (e.g., more than four times per week for red meat). Additional points are awarded for greater consumption of vegetables, healthier choices of breads (e.g., brown, multigrain), and milk. Participants who indicate they follow a vegetarian eating pattern are assigned a zero score for the meat subscale, with double points awarded for each of the meat alternatives questions. An additional point is also awarded if soybeans, tofu, other beans and lentils were reported as consumed once per week or more. The total score, ranging from zero to 73, is calculated by summing the points for each food item, with higher scores indicating a higher diet quality. 24 The ARFS questions and scoring are available at Supplemental Table 2. The total score is categorised into the following groups; ‘needs work’ (<33 points), ‘getting there’ (33-38 points), ‘excellent’ (39-46 points), and ‘outstanding’ (47+ points). The ARFS has been validated and shown high level of reliability and consistency in evaluating diet quality and estimating fruit and vegetable intakes among Australian adults.5,24
Dietary Intake
Dietary intake was measured using the AES. The AES is a self-administered, validated semi-quantitative FFQ consisting of 120 questions, including beverages, milk and dairy foods, breads and cereals, sweet and savoury snacks, main meals, vegetables, fruit, and other foods. 25 In addition, the AES contains 15 questions relating to age, height, weight, use of nutritional supplements, and intake-related behaviours. 25 The questions asked are based on the individual’s food intake over the last three to six months. Responses were assessed using a Likert Scale with response options ranging from ‘never’ to up to ‘seven times per day’. Standard portion sizes for each food item in the AES were derived from the most recent National Nutrition Survey data. 26 Nutrient intakes from the AES FFQ were computed using data in the AUSNUT 2011-13 database. 27 Participants’ usual daily servings of vegetables, fruits, grains (cereals), meat and alternatives, and dairy foods (nutrient-dense core foods) were derived from the AES and compared with AGHE food group servings. Macro- and micronutrient intakes captured from the AES for each participant were compared to the respective Nutrient Reference Values (NRVs) to determine adequacy of intake. 28 Total contribution of energy intake from core and non-core foods were derived from the nutrient-dense core foods and discretionary foods that are high in saturated fat, added sugars, added salt and/or alcohol. The AES has been validated in the adult population and demonstrated high level of accuracy in estimating nutrient intake and fruit and vegetable intakes.29,30
Nutrition Self-Efficacy
Nutrition self-efficacy was assessed using the Ralf Schwarzer and Britta Renner Nutrition Self-Efficacy scale which includes five questions on an individual’s perspective of their daily nutrition needs. 31 Each question is scaled from 1 ‘very uncertain’ to 4 ‘very certain’ with a total score out of 20. A higher score on the nutrition self-efficacy scale indicates a higher level of nutrition self-efficacy.
Sources Used for Obtaining Pregnancy Nutrition Information
A series of questions developed for this study were asked to identify if the participant obtained pregnancy nutrition information and if so the sources of nutrition information used, and the frequency in which they were used. To identify the different sources used, a question was asked with the options of ‘General Practitioner (GP)’, ‘Obstetrician’, ‘Midwife’, ‘Dietitian/Nutritionist’, ‘Social media’, ‘Smart phone applications (apps)’, ‘Internet’, ‘Family and friends’ and ‘Other’. Participants were also asked about the frequency that they use/d their most used source of pregnancy nutrition information.
Socio-Demographic Characteristics
Socio-demographic data were collected including age, height, weight, education level, nationality, marital status and income, and health-related data such as parity, gestation length and smoking status.
Analysis
Data were analysed using SPSS statistical software (Version 29, IBM Corp, NY USA). Socio-demographic characteristics, diet quality (ARFS), dietary intake, nutrition self-efficacy and sources of pregnancy nutrition information are reported as a mean (SD) for continuous variables, and as number (%) for categorical variables. To measure the strength of the association between diet quality and nutrition self-efficacy, Spearman’s rank-order correlation was used, due to the non-normal distribution of the nutrition self-efficacy scores. Correlation strength was described as weak <0.2, moderate 0.2-0.6, or strong >0.6, as previously identified within dietary validation studies.30,32 To examine the influence of nutrition self-efficacy on diet quality, linear regression analyses were conducted using an unadjusted model, and a model adjusted for BMI, household income and qualification. Mean comparison tests (independent t test and Mann-Whitney U test) were conducted to investigate differences in mean diet quality scores and nutrition self-efficacy scores for groups who obtained pregnancy nutrition information from at least one health professional compared to those who only obtained nutrition information from other sources (i.e., not any health professional). The level of statistical significance was set at P < .05.
Results
Of the 330 participants that expressed interest in participating in the study, 159 did not satisfy the inclusion criteria or complete the survey and were excluded from the study. To ensure quality of the data, the responses of participants who take less than half the median time to complete are commonly excluded. 33 Of the 171 completed survey responses, no responses were below half the median time taken, therefore, the current study included 171 participants.
Socio-Demographic Characteristics
Socio-Demographic and Health Characteristics of Participants (n = 171).
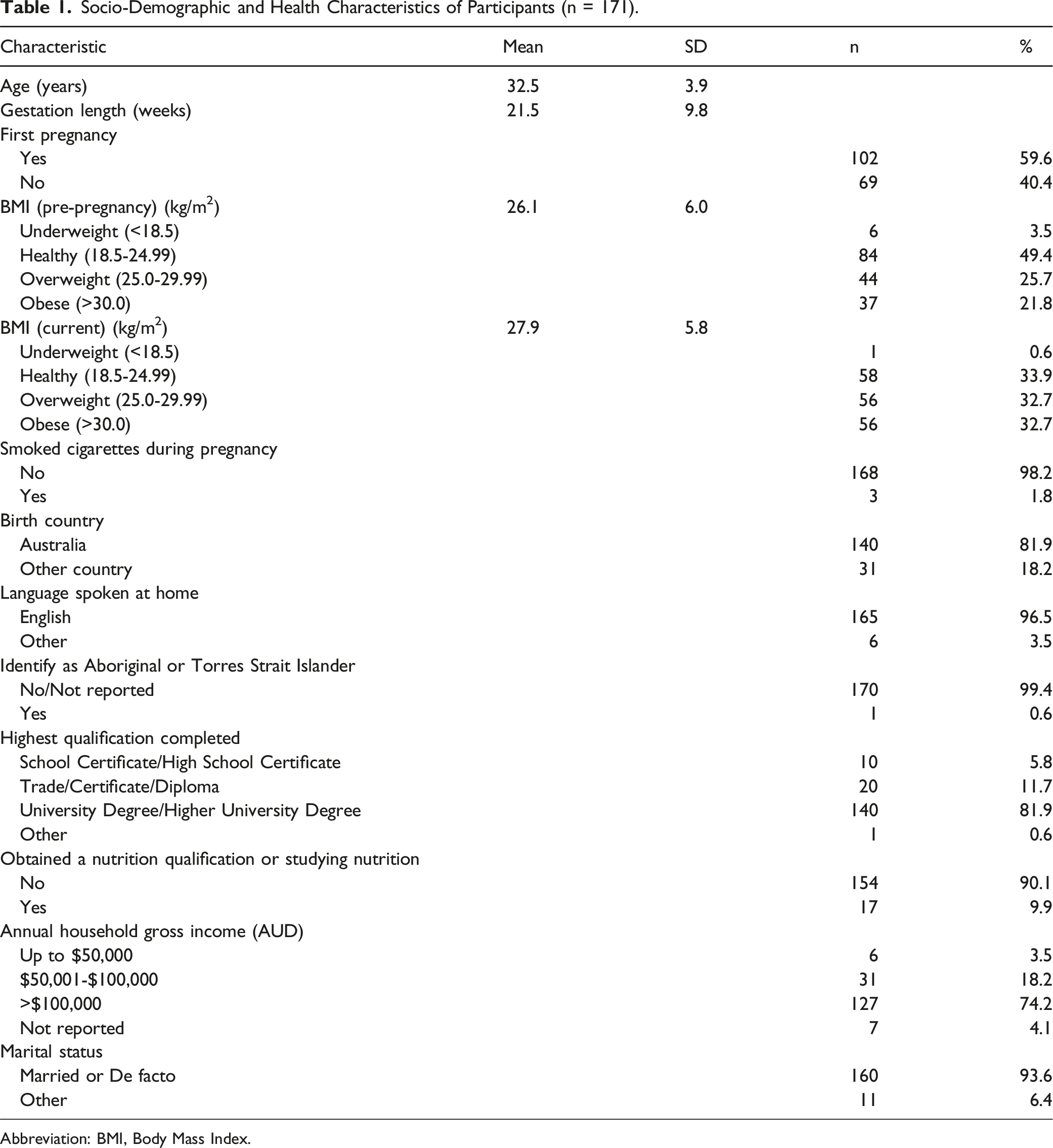
Abbreviation: BMI, Body Mass Index.
Diet Quality and Dietary Intake
Australian Recommended Food Score (ARFS) (n = 171).
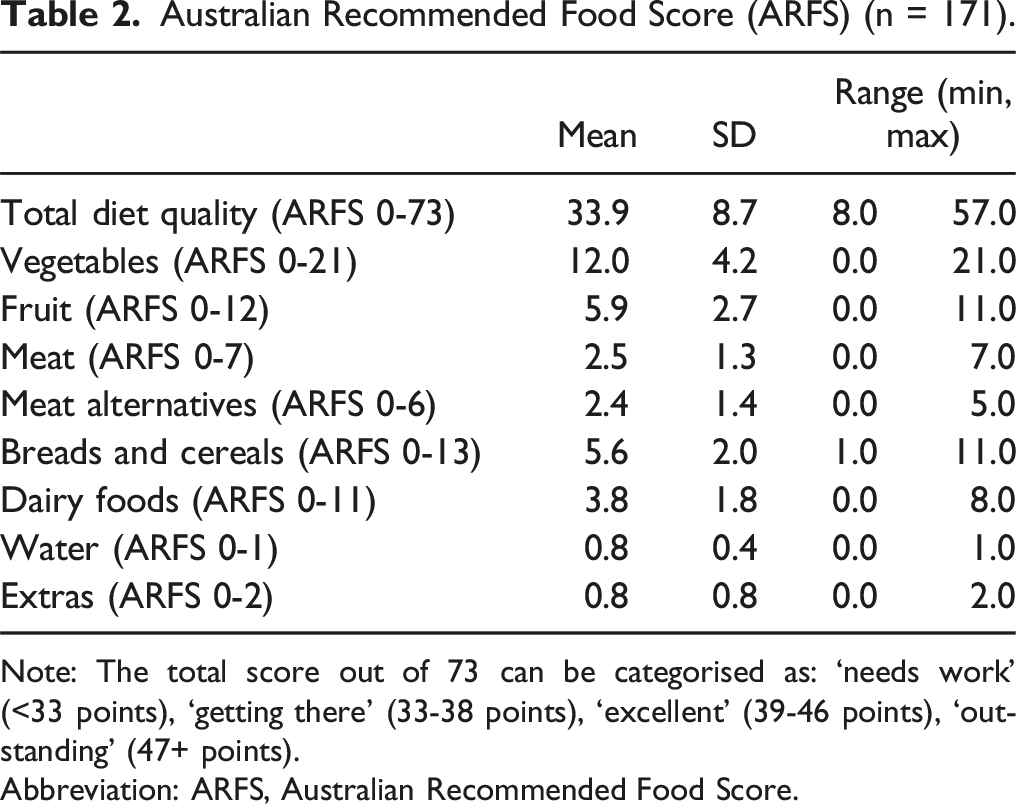
Note: The total score out of 73 can be categorised as: ‘needs work’ (<33 points), ‘getting there’ (33-38 points), ‘excellent’ (39-46 points), ‘outstanding’ (47+ points).
Abbreviation: ARFS, Australian Recommended Food Score.
Mean Dietary Intake of Participants (n = 171).
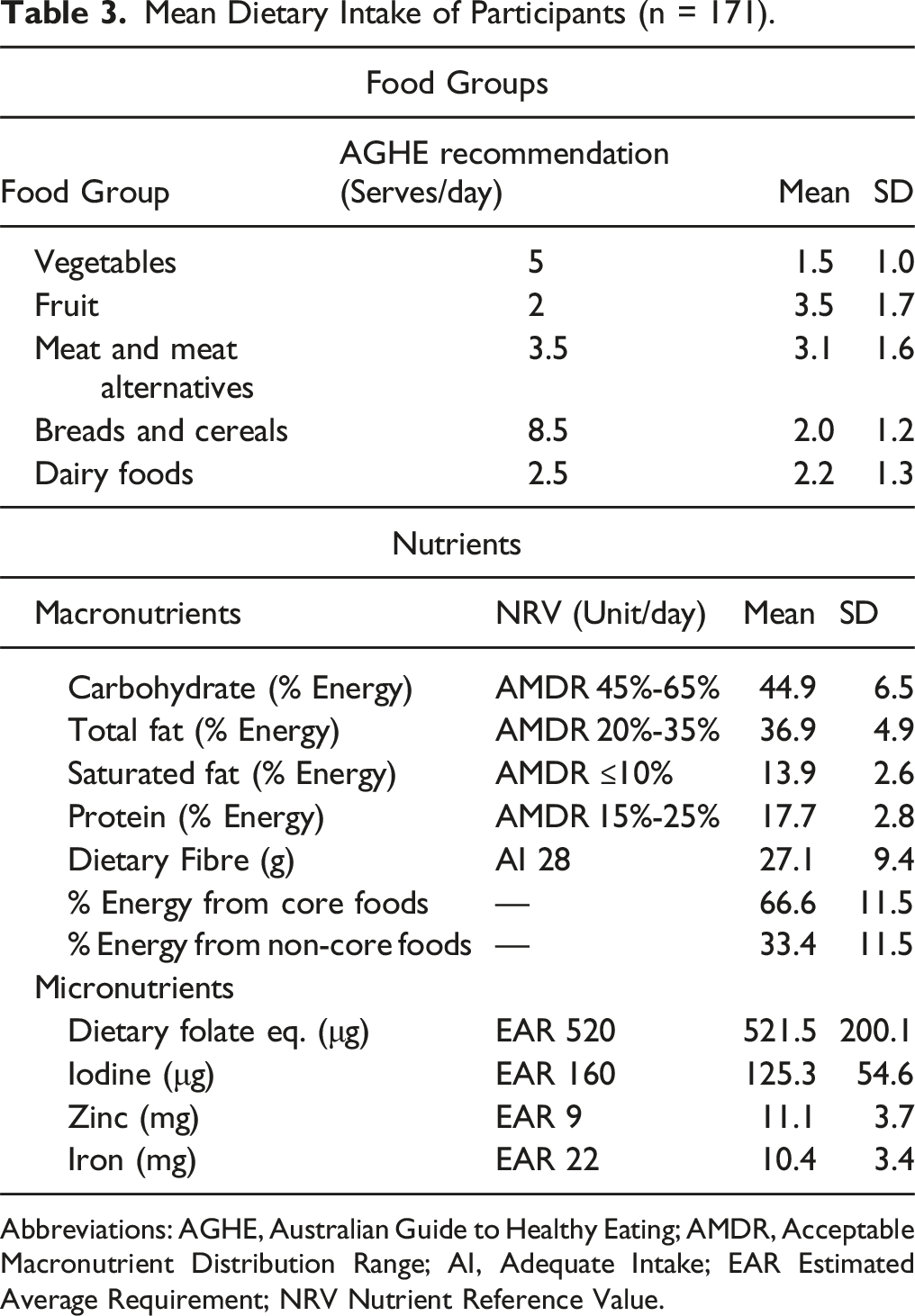
Abbreviations: AGHE, Australian Guide to Healthy Eating; AMDR, Acceptable Macronutrient Distribution Range; AI, Adequate Intake; EAR Estimated Average Requirement; NRV Nutrient Reference Value.
Nutrition Self-Efficacy
The participants’ mean (SD) nutrition self-efficacy score was 14.7 (3.7) points out of 20.0. The nutrition self-efficacy scores ranged from 5.0-20.0 points.
The Relationship Between Diet Quality and Nutrition Self-Efficacy
A correlation analysis showed a moderate positive linear relationship between diet quality and nutrition self-efficacy (rs = 0.27, P < .001). In both the unadjusted and adjusted linear regression analyses, nutrition self-efficacy significantly predicted the diet quality score (Unadjusted model: (F(1, 169) = 11.51, P =< .001, R2 = 0.064,
Sources of Pregnancy Nutrition Information
A total of 137 participants (80.1%) reported obtaining pregnancy nutrition information. With regard to the nutrition information sources used by the participants, the most common source was the internet (n = 112, 65.5%), followed by the participants’ General Practitioner (n = 80, 46.8%) and Midwife (n = 60, 35.1%). Pregnancy nutrition information was obtained from a Dietitian/Nutritionist by 18.1% (n = 31) of participants. When nutrition information sources were categorised as health professionals (general practitioners, obstetricians, midwives, dietitians and nutritionists) and non-health professionals (internet, social media, smartphone applications, friends/family, other source), of the 137 participants, the data showed that 84.7% (n = 116) had obtained nutrition information from at least one health professional, and 15.3% of participants (n = 21) had obtained nutrition information from non-health professionals only.
Differences in Diet Quality scores in Pregnant Women who Obtain Nutrition Information from Health Professionals and Women who do not
An independent samples t-test indicated that the mean diet quality scores were not significantly different in participants who obtained nutrition information from one or more health professional (median = 35, n = 116) compared to the participants who did not obtain nutrition information from any health professionals (median = 37, n = 21), (t (24) = −0.823, P = .32).
Differences in Nutrition Self-Efficacy Scores in Pregnant Women who Obtain Nutrition Information from Health Professionals and Women who do not
A Mann-Whitney U test indicated that the mean nutrition self-efficacy score was significantly higher in the participants who obtained nutrition information from one or more health professional (median = 15, n = 116) compared to the participants who did not obtain nutrition information from any health professionals (median = 13, n = 21), (U = 856, z = 2.18, P = .03, r = −0.19).
Discussion
The objective of this study was to examine the relationship between diet quality, nutrition self-efficacy and sources of nutrition information in a sample of Australian pregnant women. The results showed that pregnant women had a mean diet quality score of 33.9 points out of 73, categorised as ‘getting there’ but requiring improvement. 34 This finding is consistent with the dietary intake results which showed that overall alignment with dietary recommendations was poor with inadequate intake of four out of five healthy core food groups (vegetables, breads and cereals, meat, and dairy foods) and excessive intake of fat, including saturated fat. The mean nutrition self-efficacy score reported by the participants was 14.7 points out of 20 and a moderate positive relationship between diet quality and nutrition self-efficacy was found, with nutrition self-efficacy significantly predicting the diet quality score. In terms of pregnancy nutrition information, 80% of participants reported obtaining information, with most of these obtaining pregnancy nutrition information from one or more health professionals and 15% obtaining information from non-health professionals only. Participants’ diet quality scores were not significantly different when obtaining nutrition information from at least one health professional, compared to obtaining nutrition information from non-health professionals only, however, their nutrition self-efficacy scores were significantly higher.
The ADG, NRV and AGHE are national dietary recommendations that are in place to ensure that pregnant women optimise and maintain their overall health.23,28,35 Aligning intake with dietary recommendations supports metabolic changes during pregnancy, 36 and can reduce adverse health outcomes in the mother, 37 fetus, and child in later stages.3,4,38 The overall diet quality score in the sample of 33.9 points out of 73, categorised as ‘getting there’, is consistent with other studies in Australian pregnant women39,50 reporting diet quality scores between 32 and 44 points. The diet quality score is also consistent with scores reported in the Australian general population, despite pregnancy being considered a period of increased motivation for healthy eating.34,40 The current study provides further evidence that pregnant women report inadequate intakes of most food groups, with this sample only meeting the recommendation for serves of fruit. This aligns with a cross-sectional web-based survey with 857 Australian pregnant women, 7 in which the sample only met the recommendation for fruit intake. In the current study, daily consumption from food of key pregnancy micronutrients folate and zinc met the EAR, whereas intake of iodine and iron did not. Other studies in Australian pregnant women have also reported inadequate intake of iodine and iron.8,41 The suboptimal diet quality and poor alignment with dietary recommendations in this sample of pregnant women and others highlights an urgent need for further research to identify and address intrapersonal, interpersonal and environmental barriers to meeting dietary recommendations, due to the increased risk of adverse health outcomes that are associated with inadequate intakes. 41
In the current study, the association between diet quality and nutrition self-efficacy was assessed and a moderate positive relationship was observed. Regression analyses found that nutrition self-efficacy significantly predicted the diet quality score. While there is a paucity of literature on this relationship, a cross-sectional study in 75 women in the United States who had been pregnant within the last five years also reported that having a higher nutrition self-efficacy was significantly associated with a higher diet quality. 12 While additional research is needed in larger samples, these findings support our hypothesis that pregnant women who have a higher nutrition self-efficacy score, have a higher diet quality score, suggesting the importance of improving an individual’s nutrition self-efficacy as a potential mediator for improved diet quality.
To the best of our knowledge, no other research has examined differences in diet quality scores in relation to sources of pregnancy nutrition information. In the current study, 80% of women reported that they did obtain pregnancy nutrition information, with the internet being the most common source of information. This correlates with reports that the internet is the primary source of nutrition information for Australians. 42 In a cross-sectional survey conducted in the UK it was reported that before and during pregnancy, women preferred to use the internet rather than see a health professional to obtain nutrition information, however the uptake of obtaining nutrition information from health professionals increased during pregnancy. 43 Moreover, a mixed-methods study which included a survey and content analysis in pregnant women in the years of 2008, 2011, 2014 and 2018, showed a significant increase in the use of the internet for obtaining nutrition information. 44 In the current study, around one-quarter of the pregnant women reported using social media to obtain nutrition information. 45 A 2024 cross-sectional study in 142 women in Australia who were either currently pregnant or who had recently given birth found that two-thirds of the women obtained pregnancy nutrition information from social media platforms. 46 Overall, there has been a significant increase in the use of the internet and social media for obtaining nutrition information in Australia and around the world in recent years.30,47 Experts have noted concerns regarding potential misinformation of nutrition information, due to suboptimal quality and accuracy. 42 A systematic review of seven studies, found that most pregnant women did not discuss the health information found on the internet with any health professional. 47 In the current study, it was found that less than half of the pregnant women sought nutrition information from their general practitioner or midwife, and very few from their obstetrician or dietitian/nutritionist. Health professionals should be aware of the increasing uptake of obtaining nutrition information from the internet and ensure they provide pregnant women with evidence-based nutrition information where possible.42,48
In terms of the differences in diet quality and nutrition self-efficacy scores in pregnant women based on nutrition information sources, the current analysis found that there were no significant differences in the diet quality scores of pregnant women who obtained nutrition information from at least one health professional compared to those who did not obtain nutrition information from any health professionals. However, in this study there was a significant difference in the nutrition self-efficacy scores in the pregnant women who obtained nutrition information from health professionals compared to those who did not, with a higher nutrition self-efficacy score in those who sought information from health professionals. This might suggest that obtaining nutrition information from a health professional validates belief in the women that they can adhere to dietary recommendations. However, the poor diet quality scores in this sample indicate that higher nutrition self-efficacy associated with obtaining information from health professionals did not translate to higher diet quality scores. In light of these findings, it is recommended that further research is conducted to understand the specific barriers pregnant women face in converting higher nutrition self-efficacy to improved diet quality.
A strength of the current study is that it is the first study, to our knowledge, to analyse the relationship between diet quality, nutrition self-efficacy and sources of nutrition information in pregnant women. The study provides new knowledge which can be used as a foundation for future research on the same topic. Additionally, the use of validated dietary assessment tools, the ARFS and AES, to measure diet quality and dietary intake is a strength in the current study.5,24 The study should also be interpreted in the context of some limitations. Firstly, participants were primarily recruited via social media posts and paid advertising, which may limit the generalisability of the findings. Future studies may need to consider additional recruitment strategies beyond online methods to broaden the group of participants, such as advertising in antenatal clinics and hospital waiting rooms and community noticeboards. Also, the sample of participants in this study were more highly educated in comparison to the wider pregnant and non-pregnant Australian population, and which may also limit the generalisability of the results. Self-reported dietary intake also has limitations, such as recall bias and social desirability bias.
32
However, to help mitigate potential social desirability bias all responses were collected anonymously to reduce the likelihood of participants providing socially desirable answers. In addition, the use of well-established and validated questionnaires may also have minimized social desirability bias.
32
These methods are suggested in future research in pregnant women. The use of a social desirability measure such as the Marlowe-Crowne Social Desirability Scale Short-Form
49
could also be warranted, to account for potential confounders in statistical models, however, lengthy data collection surveys can add burden to the participant, decreasing motivation to complete.
32
A further limitation in this study is that the diet quality score (ARFS) used in this study is modelled on foods representative of Australian foods, which may not be generalisable to countries outside of Australia. Australian pregnant women have reported to have poor diet quality and were not consuming adequate nutrients. Finally, the analysis did not account for supplement intake or any sickness during the participants’ pregnancy, which may be useful to consider in future research. Australian pregnant womens’ dietary intake is poorly aligned with dietary recommendations set out in the Australian Dietary Guidelines and Australian Guide to Healthy Eating. This is the first study to investigate the relationship between diet, quality, nutrition self-efficacy and sources of nutrition information in Australian pregnant women. Our findings suggest the need for evidence-based pregnancy nutrition information to be highly accessible via the internet and for health professionals to focus on providing evidence-based nutrition information at all available opportunities. Improving nutrition self-efficacy may be effective for improving diet quality. Further research is needed to elucidate the specific barriers pregnant women face in converting higher nutrition self-efficacy to improved diet quality.So What?
What is Already Known on This Topic?
What Does This Article Add?
What Are the Implications for Health Promotion Practice or Research?
Supplemental Material
Supplemental Material - The Relationship Between Diet Quality, Nutrition Self-Efficacy and Sources of Nutrition Information in Australian Pregnant Women: A Cross-Sectional Analysis
Supplemental Material for The Relationship Between Diet Quality, Nutrition Self-Efficacy and Sources of Nutrition Information in Australian Pregnant Women: A Cross-Sectional Analysis by Akela Phillips, Tamara Bucher, Penta Pristjono, and Sasha Fenton in American Journal of Health Promotion
Footnotes
Author Contributions
Conceptualization: TB, SF, AP. Methodology: TB, SF. Formal analysis: TB, SF, AK. Writing – original draft preparation: AP. Writing – review and editing: AK, SF, TB, PP. All authors read and approved the final manuscript. This study was undertaken as partial requirement for award of the degree of Bachelor of Food Science and Human Nutrition (Honours program) at the University of Newcastle, Australia.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Consent to Participate
All participants provided written informed consent to participate.
Data Availability Statement
The data that support the findings of this study may be available on request from the corresponding author (SF).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.