
Abstract
Purpose
American medical students exhibit higher rates of depression, anxiety, and psychological distress than age-matched members of the general population, yet the majority of students do not seek help for these conditions. A necessary precursor to help-seeking is disclosure, or the sharing of one’s diagnosis or symptoms with others. This pilot study aims to explore mental health disclosure decision-making among medical students.
Design
Semi-structured qualitative interviews.
Setting
Students were interviewed virtually using Zoom.
Participants
20 students enrolled in nine American undergraduate medical education institutions (MD or DO).
Method
Interviews were audio-recorded and transcribed. Using Constructivist Grounded Theory (CGT) and iterative cycles of analysis with focused and theoretical coding, a preliminary framework was developed to represent mental health disclosure decision-making among medical students.
Results
The proposed framework presents three factors that impact students’ disclosure decisions: Assessing Anticipated Outcomes, Evaluating Priorities, and Determining Appropriate Recipients. The framework also identifies two moderating variables—Disclosure Goals and Severity and Type of Symptoms—that affect students’ perspectives on outcomes and recipients.
Conclusion
This pilot study highlights the complexity of student disclosure decision-making. While limited by the small sample size, the results suggest the importance of considering student perspectives on disclosure recipients, communication surrounding disclosure outcomes, and the flexibility of student schedules when pursuing future projects related to medical student well-being and mental health disclosure.
Purpose
Physicians exhibit increased rates of psychological distress compared to the general population.1,2 Previous studies have indicated that psychological distress—including depression, anxiety, and other mental health conditions—is associated with reduced quality of patient care, increased expressions of irritability and anger, and more medical errors.3-5
Increasing rates of mental health distress have been shown to emerge as early as medical school. Although matriculating medical students report lower rates of burnout and depression than age-similar college graduates, 6 an estimated 27.2% of current medical students exhibit depression or depressive symptoms and 11.1% exhibit suicidal ideation. 7 These rates are nearly double the prevalence for age-matched members of the general population 8 and have likely risen further following the COVID-19 pandemic.9,10 Concerningly, among medical students experiencing symptoms of mental health distress, the majority do not seek treatment.11,12 Prior literature suggests that barriers to help-seeking include stigma, institutional norms, and fear of unwanted consequences.11-13
Before medical students can seek help, they must disclose their symptoms. Self-disclosure is defined as the process through which an individual (the discloser) reveals information about themselves to another person (the recipient).14,15 Self-disclosure plays a role in shaping interpersonal relationships, self-worth, and identity. 14 Mental health disclosure also reduces “us vs. them” thinking and combats negative attitudes towards people with mental illness.16,17 This effect has been demonstrated within medical education, with one study suggesting that an older physician’s disclosure of lived experience with mental health struggles increases medical students’ willingness to seek care and improves attitudes towards mental illness. 18 Therefore, encouraging senior physicians to role-model mental health disclosure has the potential to both encourage student help-seeking and reduce stigmatizing attitudes that presently discourage student help-seeking.
To achieve these effects, it is necessary to understand how students decide to self-disclose. Greene’s Disclosure Decision-Making Model (DD-MM) asserts that disclosure decisions result from a discloser’s assessment of three components: information about their diagnosis, their relation to and the anticipated response of the receiver, and disclosure efficiency, or their perceived ability to share a message and receive a desired response.19,20 This model has been adapted to apply to individuals with severe mental illness, 21 and studies have also explored how decision-making is impacted by particular contexts, such as the workplace, 22 or particular populations, such as athletes. 23
Although research suggests that fear of stigmatization, punitive institutional responses, and a belief that disclosure is irrelevant are potential barriers to mental health disclosure for medical students,24,25 there is limited information on the factors that facilitate disclosure events and no qualitative research on how American medical students make mental health disclosure decisions. Using Constructivist Ground Theory (CGT), this pilot study seeks to explore these knowledge gaps by developing a preliminary framework that represents how American medical students understand and approach mental health disclosure decisions.
Design
This study utilized CGT, a methodology that emphasizes the impact of social, cultural, and relational contexts on knowledge creation.26,27 This approach was chosen to develop knowledge about disclosure that is grounded in participant experiences and relationships and sensitive to unique social processes within medical education. Consistent with a constructivist epistemology, each individual was assumed to understand and experience mental health in their own way, impacted by their unique experiences.
To protect participant well-being, participants were not required to disclose information about their own mental health. Instead, participants were asked to share their perspectives on mental health disclosure broadly and to theorize about what might affect disclosure decision-making. While there may be differences between how students think they will act and how they actually behave, this approach broadened the participant population to include all students, rather than only those who have experienced mental health challenges, increasing the probability that these findings capture the perspectives of the “average” medical student. Ethical approval was obtained from the Research Compliance Office at the authors’ primary institution for all components of this study prior to initiation.
Setting
A convenience sample of 20 participants was recruited by publicizing study information via social media and medical student newsletters, utilizing professional contacts, and receiving referrals from enrolled participants. To reduce self-selection bias, recruitment materials were catered to a general medical student population, rather than those with a specific interest in mental health.
Participants were eligible to participate if they were currently completing coursework for, or were on short-term leave from, an American medical education (MD or DO) program. Enrolled participants attended nine institutions across the country, with representation from the northeast, middle Atlantic, south, southwest, and western geographic regions, as well as suburban, urban, and rural campuses. Three institutions were public and three were ranked as a top 20 medical institution for research by U.S. News in 2023. 28
All interviews were recorded using Zoom, a secure teleconferencing software with audio and video recording capabilities. Participants were sent an IRB-approved Waiver of Documentation prior to their interview and were given time to ask questions. After these questions, if any, were addressed, participants provided verbal consent that they had read and understood the study content and agreed to participate in the study. No participants declined to participate at this stage.
Participants
Of the 20 participants, 15 self-identified as women, 11 self-identified as white, and seven self-identified as Asian. 10 participants had entered the clinical portion of their training, and four were completing their first year of medical training.
Method
Semi-structured interviews were conducted by the primary investigator (SS) between July 2021 and January 2022. This study utilized a pre-determined interview guide with open-ended questions to encourage consistency and allow flexibility to pursue topics that arose during the interview. The guide was developed through discussion between SS, two researchers specializing in qualitative research, and one medical doctor with a background in student well-being. Questions were grounded in conceptions of mental health disclosure and mental health stigma from prior research and knowledge of existing institutional mental health resources. Institution-specific mental health resources were provided to participants if requested or deemed necessary by SS. Participants were not compensated for their participation.
Verbatim transcripts were generated for each interview. Each transcript was de-identified and reviewed twice to standardize format and enhance descriptive validity. Once de-identified, a micro dataset of three interviews from participants at three different institutions was hand-coded using a preliminary coding chart containing both a priori and grounded codes. A priori codes were generated by prior research, while grounded codes reflected perspectives and voices of study participants. This step was intended to improve the coding scheme and identify and combat investigator biases. 29
All interview transcripts were then uploaded to MAXQDA 2022 and coded in multiple passes, 30 moving from descriptive and categorical codes to interpretive codes. After two coding passes, matrices and other data displays were developed to investigate themes and address emerging ideas about mental health disclosure. 31 These tools informed a final pass of focused coding guided by specific thematic ideas. All coding was completed by SS and reviewed by two qualitative research experts and one medical doctor. Throughout the iterative coding process, SS wrote analytic memos and met regularly with the co-authors to discuss the analytic process, document emerging themes, acknowledge researcher bias, and receive feedback. Consistent with CGT, the coding chart was modified after each round of coding to refine code definitions, add new codes, and track code frequency. After coding was completed, matrices were used to confirm emerging ideas, assess outliers and rival explanations, and refine and generate conclusions. 31
Results
Students reported three primary factors that impact disclosure decisions: anticipated disclosure outcomes, preferred disclosure recipients, and student priorities. These factors reflect three questions that students consider when deciding whether to disclose mental health challenges: (1) What may happen if I disclose this information? (2) Who do I want to disclose to? (3) Is disclosure more important than my other responsibilities?
Student interviews also indicated two moderating variables—the severity and type of mental health symptoms and the goals of disclosure—which impact the relationships between these primary questions and a student’s decision to either disclose or conceal mental health challenges.
What May Happen if I Disclose This Information?
Participants felt that disclosure could lead to four main outcomes: harm to career prospects, changes to interpersonal relationships, improved academic performance through improved self-care, and de-stigmatization. When discussing disclosure decisions, students reported considering the pros and cons of each outcome and the likelihood that each would occur in their situation.
Harm to Career Prospects
Many participants felt that disclosing mental health challenges could harm their future career prospects. Although students acknowledged that sharing mental health challenges is not incompatible with a successful medical career, they worried that disclosing would “put [them] in a harder place” (Student [S] 9). Given the competitive landscape and financial burdens of medical education, students worried that, if they disclosed and later failed to reach desired career milestones, they would “always be wondering if that [their disclosure] played a role” (S9).
Changes to Interpersonal Relationships
Students felt that disclosure could strengthen some interpersonal relationships while straining others. In some cases, students noted that self-disclosure fostered a sense of community among peers, providing a cathartic opportunity to share one’s challenges: “Whenever you see [other students], you get super excited and you're like ‘Oh my God, I’ve been so exhausted all this time and all these horrible things are happening.’” (S9)
This student describes the excitement of encountering a classmate and being able to talk about her difficulties with them. In other cases, students cited uncertainty over the appropriate relationship to maintain with their peers: These will be my best friends, many of them, but they are also my colleagues, and there is a line somewhere… Do you want the person who you have to have a professional relationship with knowing the more intimate details of your mental health and personal life? (S10)
These competing identities—of peers as both friends and colleagues—complicate disclosure decision-making by introducing competing messages about the proper amount of personal information to share with one’s classmates.
Concerns about disclosure also extended to students’ relationships with superiors. When interacting with professors or older physicians, students worried that disclosure could lead others to view them as “less competent” (S1) or to wrongly ascribe their behavior to mental illness: “If I had bipolar, they’re like ‘Oh, I think she’s just a little manic today.’ ‘Like no, I’m not, you’re just mean’” (S1).
Improved Academic Performance
Students frequently noted that mental health challenges affect one’s ability to fulfill their academic responsibilities, with one participant likening the impact of mental illness on a medical student to the impact of physical injury on an athlete: “It would be like if you were a marathon runner, and you broke your leg. And now you’re behind, and you’re just frustrated that you can’t run fast” (S11). In these situations, students hoped that disclosure would enable access to resources that help students better fulfill their academic obligations. This sentiment emerged as particularly relevant during clinical years of training, when students worried that neglecting their own well-being by attempting to “pour from an empty cup” (S4) could harm patient care. Students also frequently acknowledged the threat of burnout in their future careers, with some participants viewing disclosure as a proactive strategy that “build[s] up your buffer” by enabling students to address mental health needs early, before training becomes even more difficult (S15).
De-stigmatization
One of the most frequently cited benefits of disclosure was the opportunity to normalize mental health challenges and “create a culture of vulnerability” within medical communities (S8). This attitude, in which de-stigmatization is perceived to result from the sharing of personal narratives from those with a stigmatized identity, confirms findings from previous studies.18,32
Severity and Type of Symptoms
Student expectations about the outcomes of self-disclosure varied based on the specific symptoms or mental health condition that would be disclosed. Mental health challenges that were perceived to be less severe were associated with fears of judgment and invalidation, such as an outsider’s assessment that a person struggling with something so minor is not “fit” for medicine. Students also shared that counseling felt less available in cases when “you’re not super depressed or anxious” because, given limited resources, more attention would be given to those “who really need it” (S8).
For mental health challenges severe enough to warrant a formal diagnosis and psychiatric care, disclosure was often perceived as less risky because of the promise of patient confidentiality. However, this sense of safety was moderated by the specific diagnostic label applied by a professional. Depression and anxiety were frequently viewed as “acceptable” diagnoses (S1), both because of their high prevalence among medical students and because institutions have explicitly encouraged students to seek treatment for these conditions. In contrast, disclosure of schizophrenia, bipolar disorder, or a substance use disorder—disorders deemed by one student as “serious diagnoses”—was perceived to more frequently cause others to doubt an individual’s competency, primarily due to heightened concerns about the ability of physicians with these diagnoses to safely care for patients (S11).
Who Do I Want to Disclose To?
Disclosure decision-making is also influenced by a student’s ability to determine and locate an appropriate disclosure recipient. Students reported that disclosure goals—or the outcomes that a student hopes to achieve following disclosure—play a large role in determining the most appropriate type of disclosure recipient. Participants identified five major goals of disclosure—policy change, cultural change, advice for next steps, validation, and mental health treatment—and related each of these goals to a specific type of disclosure recipient (Figure 1). For example, students aiming to receive mental health treatment will likely wish to disclose to mental health professionals, while students seeking information on available resources or “permission” to seek help will more likely disclose to individuals with knowledge of institutional supports (S20), such as professors or classmates. Anticipated Relationship Between Disclosure Goals and Desired Disclosure Recipients.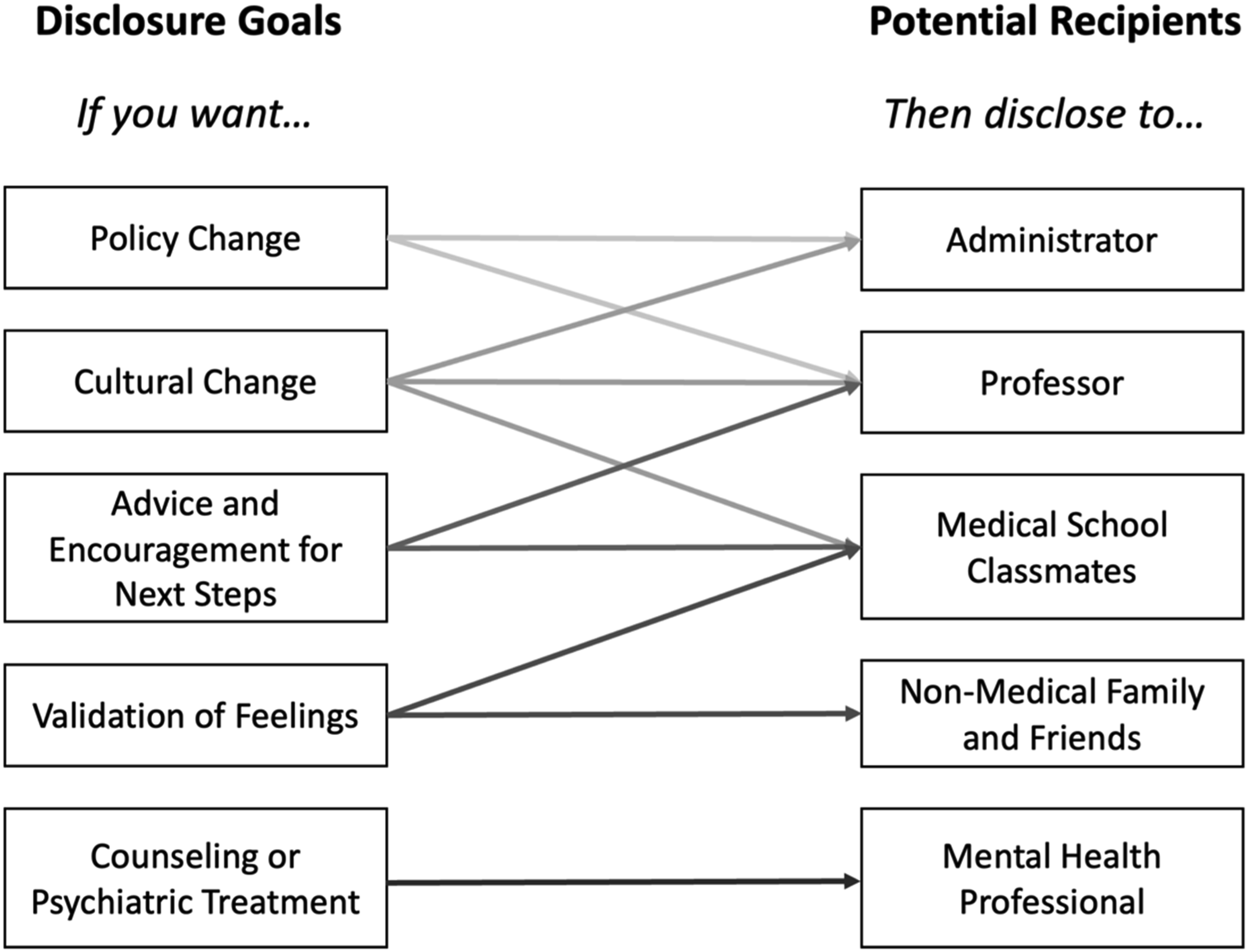
Some students also noted that disclosure may occur because students want to help others by promoting cultural change or voicing complaints with school policies. Students seeking cultural change sought to disclose to people within medical communities, such a classmates and professors, while those seeking reform sought recipients with the institutional power to revise policies. Finally, in some cases, disclosure was viewed as a way “get something off your chest” (S19), rather than a tool to achieve a specific result. In these situations, students elected to disclose to family and friends.
For all recipient groups except non-medical family and friends, students also described qualities of individuals within a given group that encourage and discourage disclosure. Classmates who understand the stressors of medical training and “know that it can be a tough environment” were viewed as attractive recipients (S12), although students preferred to disclose to classmates with whom they already had a close relationship. Students also emphasized the importance of disclosing to friends whom they see often and who have enough time to address the information that is disclosed.
While professors were not unanimously viewed as desirable disclosure recipients, students emphasized the value of finding “the right person” to whom to disclose (S2). These faculty members were favored because of their knowledge about mental health—whether from personal experience or professional work—and their awareness of institutional resources. Students expressed greater comfort with disclosure when they had a relationship with but were not academically assessed by a professor, such as a mentor or advisor. Disclosure was also encouraged by outward expressions of support by faculty members, such as faculty who ask about student well-being during class or offer support after difficult exams (S17). For some participants, these actions were sufficient to establish the trust necessary for disclosure; others expressed continued hesitancy over letting professors “know more about [a student’s] life than [the student] need[s] to tell them” (S13).
Students expressed a need to “walk with caution” when disclosing to administrators, feeling that they had “something to live up to” because they were “accepted into the school by those people” (S5). This relationship led students to identify administrators as appropriate disclosure recipients only when the source of stress could be resolved—such as one student’s example of meeting with a dean to discuss concerns with a grading policy—or as a last resort when seeking major changes. Students reported being more open to disclosing to administrators when their institution fostered a “pro-student” culture where “mental health disabilities are expected and noted” (S16).
While participants were generally open to disclosing to counselors or psychiatrists, this openness ranged from enthusiastic encouragement—“get to the student counseling center ASAP” (S13)—to begrudging acceptance: “I would feel fine seeing a psychologist. I wouldn't be thrilled about it, but I would be fine with it” (S18). Although no participants explicitly denied the promise of confidentiality when disclosing to a mental health professional, some expressed continued concerns about seeking professional help: I have no doubt that if I had sought out counseling that it probably would have helped because, you know, it’s helpful for people. It’s not something that I’ve ever done because there’s a lot of inertia there. And I think it’s changing, but there’s still a culture in medicine of like ‘you shouldn't do that, you shouldn't talk to someone, you’ll get in trouble.’ (S14)
In these situations, although students noted that counseling would likely be beneficial, they remained concerned about stigma and hesitant to personally utilize mental health resources.
Participants also emphasized the importance of a counselor who is separate from the medical school, both in terms of physical location and professional affiliation, and who understands the structure of medical education. In addition to general discomfort, the main barrier to disclosing to a counselor was financial burden, especially when seeking long-term services.
Is Disclosure More Important Than My Other Responsibilities?
Students frequently noted how little free time they have during their medical training. One participant shared, for example, that the end of the day comes not when she finishes her work, but when she chooses to stop working. Faced with seemingly endless obligations, students frequently expressed a desire to optimize their time: I’m thinking about like ‘Okay, when I’m working out, how do I make it the most effective? When I’m with friends, how do we have the most fun?’… Whenever I’m doing one thing,… other thoughts pop into my head around like ‘What should I do next?’ (S8)
Given this preoccupation with efficiency, students who decide to disclose mental health challenges must choose to view mental health care as a long-term investment worthy of taking up space in their day: For me, buying into using the resources more has to do with being willing to realize that investing time in going to something like counseling or going to a doctor's appointment or even spending time outdoors or doing things that are not school will be worth the investment compared to just continuing along in the patterns of classes and basically whatever is the easiest route forward. (S17)
As this student suggests, a medical student’s “easiest route forward” often involves prioritizing their academic obligations over their mental health. This “mindset of constantly moving forward” (S15) discourages students from disclosing unless they make a conscious decision to add their mental health to their list of priorities or they reach a point at which they feel that not disclosing is more detrimental to their academic success than taking time to do so.
The latter situation refers to what some participants called the “breaking point,” or the moment “where it feels like things have gotten really bad” and “they need to reach out to someone” (S7). These “really bad” moments could include academic consequences (such as failing exams), exhaustion from managing symptoms alone, or the realization that one is at risk of hurting themself. Reaching this “breaking point” forcibly shifts student priorities to reframe disclosure as an essential next step.
Students reported that their reluctance to prioritize mental health was, at times, enforced by institutional policies that mandate “all these extra pressures” (S7) or create well-being initiatives that “ignore the core of student wellness” by adding supplementary programming without reducing existing obligations (S6). Students also acknowledged that some mental health resources, while beneficial, are impractical to utilize, even when a student wishes to spend time doing so: We have a therapist and, also, I think a psychiatrist… I tried scheduling with them once, but it was on surgery, so I never got my schedule to align, so I've actually never met them. (S2)
Although this student tried to meet with the mental health counselors her school provides, her academic responsibilities prevented her from actually utilizing this resource.
Feedback Loop
Participant interviews suggested that the outcome of previous disclosure decisions can impact how students approach future decision-making: My friend was very distraught and sent an email [to a faculty member] saying how hard she was struggling. And this person took six months to reply and had a phone call that was very brief… Having that experience is definitely going to make it hard for anyone to reach out again to people in higher positions. (S3)
In this example, one participant describes how the unresponsiveness of a friend’s disclosure recipient reduced the likelihood that her friend would decide to disclose again. More positively, another participant shared that hearing upperclassmen speak about their mental health challenges “made [her] want to be more open with having ups and downs” (S17). These insights indicate that disclosure decision-making does not occur in a vacuum, but rather shifts over time as additional disclosure decisions are made and students observe the results of previous disclosure events.
Framework for Mental Health Disclosure
This study frames medical students’ disclosure of mental health challenges in the context of three processes—assessing outcomes, determining recipients, and evaluating priorities—and a feedback loop. These features are visually represented in the framework in Figure 2, which also highlights how disclosure goals moderate student perspectives on disclosure recipients and how the severity/type of symptoms moderates student perspectives on disclosure outcomes. Framework for Medical Student Self-Disclosure Decision-Making.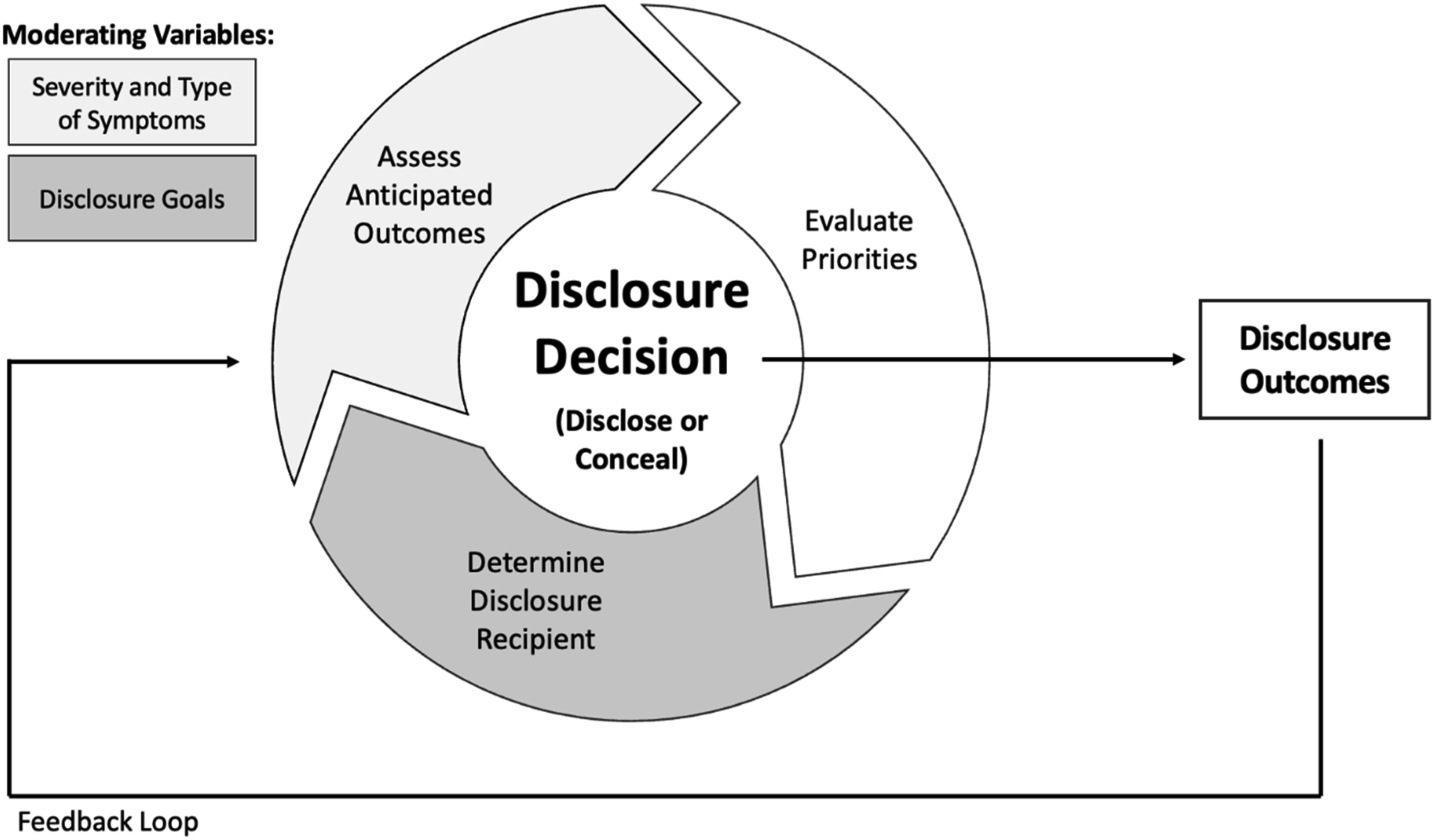
Conclusion
This pilot study and the proposed framework present novel perspectives on medical student disclosure decision-making that can inform researchers and institutions seeking to better understand student mental health. The framework’s inclusion of anticipated outcomes underscores prior research suggesting that fear of social stigma, career repercussions, and an unfavorable response from disclosure recipients represent barriers to mental health disclosure.13,19,24 Through its focus on disclosure recipients and disclosure prioritization, this framework also aligns with the DD-MM’s framing of the relationship between discloser and recipient, and the ease with which disclosure can occur, as key aspects of decision-making.19-21
This preliminary study also reveals insights related to the unique social dynamics of medical education, in which the same cohort of people are often friends, classmates, and colleagues. Participants frequently noted that their closest friends outside of class are also their professional colleagues, a tangled web of relationships within which concerns about the social stigma, changing relationships, or career repercussions that follow disclosure may feel particularly worrisome.
This complexity clarifies the importance of thinking carefully about the disclosure recipients available to students. While family members and classmates were sometimes deemed appropriate recipients, students also cited situations in which mental health counselors, professors, or administrators were preferable. These diverse needs suggest the importance of providing an array of counseling resources and communicating clearly about which faculty members and administrators are available for students to disclose to and what actions, if any, will take place following a disclosure event. Student interviews also underscored previous findings indicating that students are more likely to disclose when they see faculty members model disclosure and have access to disclosure recipients who have disclosed their own lived experiences. 18
This work also presents a barrier to disclosure that has not yet been reported in a medical student population: lack of prioritization of mental health needs. This finding suggests that disclosure events will increase when students are provided with disclosure opportunities that more conveniently align with their schedules. Although recent years have seen a growing focus on wellness in medical education, critics have questioned institutions’ tendency to add additional programming without acknowledging or reducing academic obligations.33,34 This study underscores the problem with these approaches and suggests that wellness interventions should reduce student commitments, increase the flexibility of student schedules, and expand disclosure opportunities beyond traditional working hours. While self-disclosure remains a personal decision, efforts to reduce the time and energy burdens of disclosure may help institutions encourage disclosure events. Because research suggests that contact with people who have disclosed a mental illness can promote de-stigmatization within a broader community, 35 these efforts may result in a domino effect, increasing the number of students who disclose and, in turn, reducing the stigma and fear that presently discourage disclosure.
This study has several limitations. The small sample size (n = 20) and the inclusion of only nine institutions limits the generalizability of findings. Compared to total medical student populations, these participants represent a slight overrepresentation of white students, a moderate overrepresentation of Asian students, and a substantial overrepresentation of female students.36-38 Additionally, it is possible that only students with pre-existing interests in mental health chose to participate. As a result, these perspectives may be informed by a commitment to student well-being that a general population of medical students would not possess. This participant population is also limited to students with sufficient free time to volunteer to participate, a luxury that students who are most impacted by mental health challenges, or other difficulties associated with medical education, may not possess. Given existing research on gender and race discrimination in medical spaces,39-42 it is possible that students who hold marginalized identities may be more wary of the possibility that disclosure will lead others to doubt their competency or treat them unfairly than students without these identities. As such, students with minoritized identities may consider the self-disclosure process differently.
Due to these limitations, this work is best interpreted as a pilot study that presents a preliminary framework of student decision-making that can and should be shaped and revised by further research. Specifically, future research should honor the diversity of medical student populations by endeavoring to recruit a larger and more representative study population and by employing an intersectional approach that more intentionally explores how race, gender, socioeconomic status, and/or personal interest in student well-being impact student perspectives on mental health disclosure.
43
American medical students frequently choose not to disclose or seek treatment for mental health challenges. Primary barriers to disclosure include stigma, anticipated consequences, and fear of unfavorable reactions from disclosure recipients. This study deepens existing knowledge of barriers and presents new insights on factors that facilitate mental health disclosure among medical students. By presenting a framework, this article also provides a representation of potential key decision-making elements to investigate in future research. Institutions may be able to encourage mental health disclosure by increasing the flexibility of student schedules, communicating clearly about what happens after students disclose, and developing mental health resources with an array of disclosure recipients and availability beyond traditional work hours.So What?
What is Already Known on This Topic?
What Does This Article Add?
What are the Implications for Health Promotion Practice or Research?
Footnotes
Authors’ Note
Sofia Schlozman conducted this research as an undergraduate at Stanford University. As of March 2025, Sofia is a medical student at the University of California, San Francisco.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by an Undergraduate Research Student Grant from the Vice Provost for Undergraduate Education at Stanford University.