
Abstract
Purpose
To investigate whether changes in volunteering from adolescence to young adulthood are associated with subsequent health and well-being outcomes in adulthood.
Design
Longitudinal cohort study.
Setting
National Longitudinal Study of Adolescent to Adult Health.
Subjects
U.S. adults from Wave IV (2008/2009; N = 12,234) and Wave V (2016-2018; N = 9,971).
Measures
Any volunteering and nine types of volunteering (independent variables) and 41 health and well-being outcomes (dependent variables) using an outcome-wide approach with multiple linear-, logistic-, and generalized linear regressions.
Results
Volunteering in young adulthood was associated with better health behaviors (e.g., 34% decreased risk of binge drinking, 95% CI [0.54, 0.81]) and improved psychosocial and civic outcomes (e.g., lower depressive symptoms (β = −0.08, 95% CI [−0.14, −0.02]) in adulthood. Volunteering showed little evidence of associations with other health and well-being outcomes (e.g., loneliness, (β = −0.04, 95% CI [−0.09, 0.01])). Assessing volunteering by organization types showed a range of positive and negative outcomes. For example, volunteering in hospitals/nursing homes was associated with a 36% increased risk of high cholesterol (95% CI [1.06, 1.73]) and volunteering with political clubs was associated with a 52% increased risk of an anxiety diagnosis (95% CI [1.13, 2.05]).
Conclusion
Our findings suggest more work is needed to determine the conditions under which volunteering is health promoting and to minimize potential adverse effects associated with some types of volunteering.
Purpose
There is growing evidence of the individual and societal benefits of volunteering. Previous studies have demonstrated health and well-being benefits among middle-aged and older adult volunteers.1,2 However, volunteering in younger populations is less studied. Though a substantial number of US young adults engage in volunteering (nearly 20% annually),3,4 there is little known about how volunteering in young adulthood contributes to health and well-being throughout adulthood. In response to global trends of young people delaying important milestones (e.g., longer education, later ages of marrying and having kids), researchers increasingly recognize the young adulthood years (roughly from age 18 to mid-twenties) as a distinct developmental period in which this age group has “the sense…that they are no longer adolescent but only partly adult, emerging into adulthood but not there yet.” 5 This period is characterized by identity formation, instability, self-focus, transitions, and possibilities (e.g., potentially moving out of ones’ childhood home, developing health habits, and making important decisions independently for the first time in ones’ lifetime). 5 There is good reason to believe that health promoting activities performed during this sensitive period of young adulthood will contribute even more substantially to health and well-being across the lifespan than changes during other developmental periods. If many young adults are volunteering, and this is a sensitive developmental period which may influence health across the lifespan,6,7 it is important to understand whether and how volunteering during young adulthood influences subsequent health and well-being.
Some prior work in adolescents and young adults has assessed associations between volunteering and health and well-being. Volunteering has been associated with improved physical health (e.g., reduced cardiovascular risk: lower interleukin 6, cholesterol, & body-mass index [BMI] in a randomized controlled trial of adolescents), 8 health behaviors (e.g., increased physical activity, 9 decreased smoking, 10 decreased risk of heavy drinking, 11 decreased marijuana use, 12 reduced risk of teen pregnancy, 13 and decreased risky behaviors14,15), improved psychosocial outcomes (e.g., decreased depressive symptoms,14,16-18 increased: life satisfaction, 19 purpose in life,16,20 resilience, 21 and positive affect, 22 and higher perceived quality of volunteering has been associated with improved interpersonal skills 23 ). Further, volunteering in youth was positively associated with educational attainment and earnings in adulthood.14,17 However, volunteering has not been associated with health and well-being outcomes in other studies (e.g., null associations with smoking, 11 depressive symptoms, 22 and loneliness 24 ), and has even been associated with adverse health outcomes (e.g., increased drinking 10 and higher loneliness 25 ).
These past studies helped break important new ground; however, many of these studies have limitations that the current study aims to improve upon. First, there are limited studies on volunteering and health and well-being outcomes in young adulthood. Most work has been done on older adults and existing studies focused on younger populations primarily examine adolescents. 26 Second, there is limited longitudinal work looking at volunteering during young adulthood and health outcomes later in life. While there are several rigorous longitudinal studies,14,17,18 most look at youth volunteering (prior to young adulthood) or look at outcomes cross-sectionally in early life. 27 Cross-sectional studies on adolescent and younger populations may not adequately capture the health benefits of volunteering, given that young people generally enjoy good health, while longitudinal work allows us to look at the potential long-term health benefits of volunteering. Third, many experimental studies used small sample sizes and specific samples (e.g., public high school students in Western Canada), 8 limiting the generalizability of these findings. Fourth, most studies have not examined a broad range of health outcomes within the same sample 10 – our study will investigate a wide array of physical, behavioral, psychosocial, and civic outcomes, at two separate life stages. Fifth, few studies adjust for earlier reports of volunteering to look at changes in volunteering (most only look at volunteering at a single time point). Sixth, few studies assess and compare specific types of volunteering (e.g., volunteering at hospitals/nursing homes vs volunteering with environmental groups).
We asked the question, if volunteering were increased in young adulthood (ages 18-26 in the present study), what improvements to health and well-being outcomes might we observe in adulthood? To begin addressing this question, we used an outcome-wide analytic approach (described further in the Statistical Analysis section). 28 Outcome-wide analyses are a hypothesis-generating, data-driven approach aimed at discovering promising health and well-being outcomes associated with various exposures, such as increased volunteering, which may then undergo further investigation in future studies. Using this approach, we examined if changes in volunteering were associated with better subsequent health and well-being across 41 outcomes in adulthood, including indicators of physical health, health behaviors, psychosocial factors, and civic behavior. We also assessed associations between (a) nine different types of volunteering and (b) the number of different types of volunteering reported, and subsequent health and well-being.
Methods
Design and Sample
We used data from Waves I, III, IV, and V of the National Longitudinal Study of Adolescent to Adult Health (Add Health), which was funded by the National Institute of Child Health and Human Development (NICHD) and other federal agencies. 29 Participants were recruited using a multistate, stratified, random, and school-based cluster sampling procedure. Interviews were held in the respondents’ homes. Data were collected in Wave I (1994-1995) from American adolescents in grades 7-12 (ages 12-19; N = 20,745), Wave III (2001/2002) when participants were aged 18-26 during young adulthood and when volunteering was first assessed (N = 15,197), Wave IV (2008/2009) when participants were aged 24-32 during early adulthood (N = 15,701), and Wave V (2016-2018) when participants were aged 33-43 during early midlife (N = 12,300). Covariates were assessed in Wave I, the exposure (volunteering) was assessed in Wave III, and outcomes were assessed in Waves IV and V.
We used Add Health weight variables to adjust for the complex sample design for analyses corresponding to each of the outcome waves. This effectively limits the analysis for each respective wave to participants who were surveyed at that wave. The analytic sample was restricted to those who: (1) participated in the survey at the exposure wave (Wave III, N = 15,226), (2) had valid sampling weights at the outcome waves (either Wave IV or Wave V), and (3) answered the volunteering predictor and covariate items, yielding a final analytic sample of N = 12,234 in Wave IV and N = 9971 in Wave V. In our analyses, we prioritized the latest available data from Wave V whenever possible, and included Wave IV data when Wave V data was unavailable. Add Health has been approved by several ethics committees including the University of North Carolina IRB, and informed consent was obtained from all respondents.
Measures
Volunteering
Respondents were asked about recent volunteer work at Wave III using the following item: “During the last 12 months did you perform any unpaid volunteer or community service work?” Responses were coded as 0 = no recent volunteering and 1 = recent volunteering. We also adjusted for Wave III retrospective report of volunteering during adolescence using the following item: “At any time during your adolescence, when you were between 12 to 18 years old, did you regularly participate in volunteer or community service work? Don’t count things like washing cars or selling candy to raise money.” Responses were coded as 0 = no regular volunteering and 1 = regular volunteering during adolescence.
Covariates
We adjusted for a wide range of covariates in Wave I (unless otherwise noted), including: sociodemographic and family factors (age, sex, race/ethnicity, nativity status, geographic region, family structure, number of siblings, household income, household welfare receipt, insurance status, smoker in household, mother age, mother race/ethnicity, parent nativity, parental education, mother employment status, mother religious service attendance, mother health status, mother happiness, parent has a disability, parent has obesity, parent has alcoholism, childhood maltreatment by parents [retrospectively assessed at Wave III]), psychosocial and academic factors (mental health condition diagnosis, depressive symptoms, happiness, self-esteem, life expectancy, relationship quality with a parent, parental control, neighborhood social cohesion, religious service attendance, romantic relationship status, has a learning disability, Peabody Picture Vocabulary Test [PPVT], school connectedness, grade point average [GPA], delinquency), and health status and health behaviors (somatic symptoms, pubertal development, physical health condition diagnosis, overweight/obesity, functional limitations, self-rated health, suicidal ideation, sleep disturbance, physical inactivity, cigarette smoking, binge drinking, marijuana use, illicit drug use, history of sexually transmitted infections [STIs], preventative health care use), as well as retrospective report of volunteering during adolescence assessed at Wave III.
Outcomes
We evaluated 41 outcomes in adulthood (across Waves IV and V) including measures of: physical health (number of physical health conditions, cancer, high cholesterol, hypertension, diabetes, asthma, sleep apnea, migraines, allostatic load, overweight/obesity, functional limitations, cognition, and self-rated health), health behaviors (sleep disturbance, physical inactivity, cigarette smoking, binge drinking, marijuana use, prescription drug misuse, illicit drug use, history of STIs, preventative health care use), mental health (depressive symptoms, depression diagnosis, anxiety diagnosis, post-traumatic stress disorder [PTSD] diagnosis, attention-deficit disorder/attention-deficit hyperactivity disorder [ADD/ADHD] diagnosis, suicidal ideation, perceived stress), psychological well-being (happiness, job satisfaction, sense of control, optimism, perceived discrimination), social factors (social activities, social support, relationship quality with parent, loneliness, romantic relationship quality, satisfaction with parenting), and civic behavior (voting). Supplemental Text 1 and the Add Health website with codebooks (https://addhealth.cpc.unc.edu/documentation/codebooks/) provide further details about these variables.
Statistical Analysis
The outcome-wide analytic approach 28 uses several analytic decisions not widely implemented outside of biostatistics and causal inference and are thus summarized here. First, it is difficult to discern whether covariates are confounders or mediators if covariates are assessed at the same timepoint as the exposure (Wave III). 28 To reduce this concern and allow for a more comprehensive set of covariates to address confounding, covariates were adjusted for in Wave I in our primary analyses. Second, most outcome variables (or analogous variables to the outcomes if they were not available) were adjusted for at Wave I to reduce the likelihood of reverse causation. Third, to evaluate “changes” in volunteering, we adjusted for a retrospective report of volunteering during adolescence assessed at Wave III. This helps “hold constant” prior volunteering. We assumed that there is no interaction between past and current volunteering (i.e., volunteering at Wave III is constant across past volunteering). Thus, it is possible to evaluate how changes in volunteering are associated with later health and well-being outcomes in the outcome waves (Waves IV and V, see Supplemental Text 2). Adjusting for prior volunteering further reduces risk of reverse causation by “removing” the potential accumulating effects of past volunteering (prevalent exposure).
Separate models were run for each outcome. Depending on the nature of the outcome, 3 different models were used: (1) logistic regression for each binary outcome with a prevalence <10%, (2) generalized linear models (with a log link and Poisson distribution) for each binary outcome with a prevalence ≥10%, and (3) linear regression for each continuous outcome. All continuous outcomes were standardized (mean = 0, standard deviation = 1) so their effect sizes can be interpreted as a standard deviation change in the outcome variable. We marked multiple P-value cutoffs in our tables, including those making Bonferroni correction, because practices for multiple testing vary widely and are continuously evolving.30,31 Further, E-value analyses allow us to evaluate the robustness of our results to unmeasured confounding by assessing the minimum strength unmeasured confounder(s) would have to have on the risk ratio scale (with both volunteering and the outcome) to explain away the association between volunteering and the outcome. 32 We also assessed associations between nine specific types of recent volunteering (youth organizations, service organizations, political clubs, solidarity/ethnic support groups, church groups, community centers, hospitals/nursing homes, educational organizations, and environmental groups) and subsequent health and well-being outcomes.
Additional Analyses
We conducted several additional analyses. All models were re-analyzed: (1) using covariates drawn from Wave III to assess the impact of the timing of covariate adjustment on results (because confounding adjustment in our main analyses may not have been adequate because of the long lag between our covariates and volunteering in each set of models, 28 we therefore took a more conservative approach of reanalyzing all models while adjusting for covariates at Wave III instead of Wave I in supplemental analyses), (2) using a count of the total number of different types of recent volunteering as the exposure (which may be considered to be a crude proxy for frequency of volunteering), (3) using a reduced list of conventional covariates (only sociodemographic variables; i.e., age, sex, race/ethnicity, nativity status, geographic region, family structure, household income, and parental education; all assessed at Wave 1). This approach (i.e., not adjusting for prior volunteering) might crudely assess the potential cumulative effects that the whole history of volunteering has on outcomes, (4) using only complete cases to assess the impact of multiple imputation on results.
Multiple Imputation
All missing covariates and outcomes were imputed using multiple imputation by chained equations, and 5 datasets were created. This method generally provides a more flexible approach than other methods of handling missing data and addresses problems that arise from attrition. 33 Separate imputations were run for Wave IV and Wave V such that the analyses at each wave constitutes a separate analysis sample. All analyses were conducted using Stata 17.
Results
Characteristics of Participants at Baseline by Volunteering (National Longitudinal Study of Adolescent to Adult Health [Add Health]: N = 15,154).
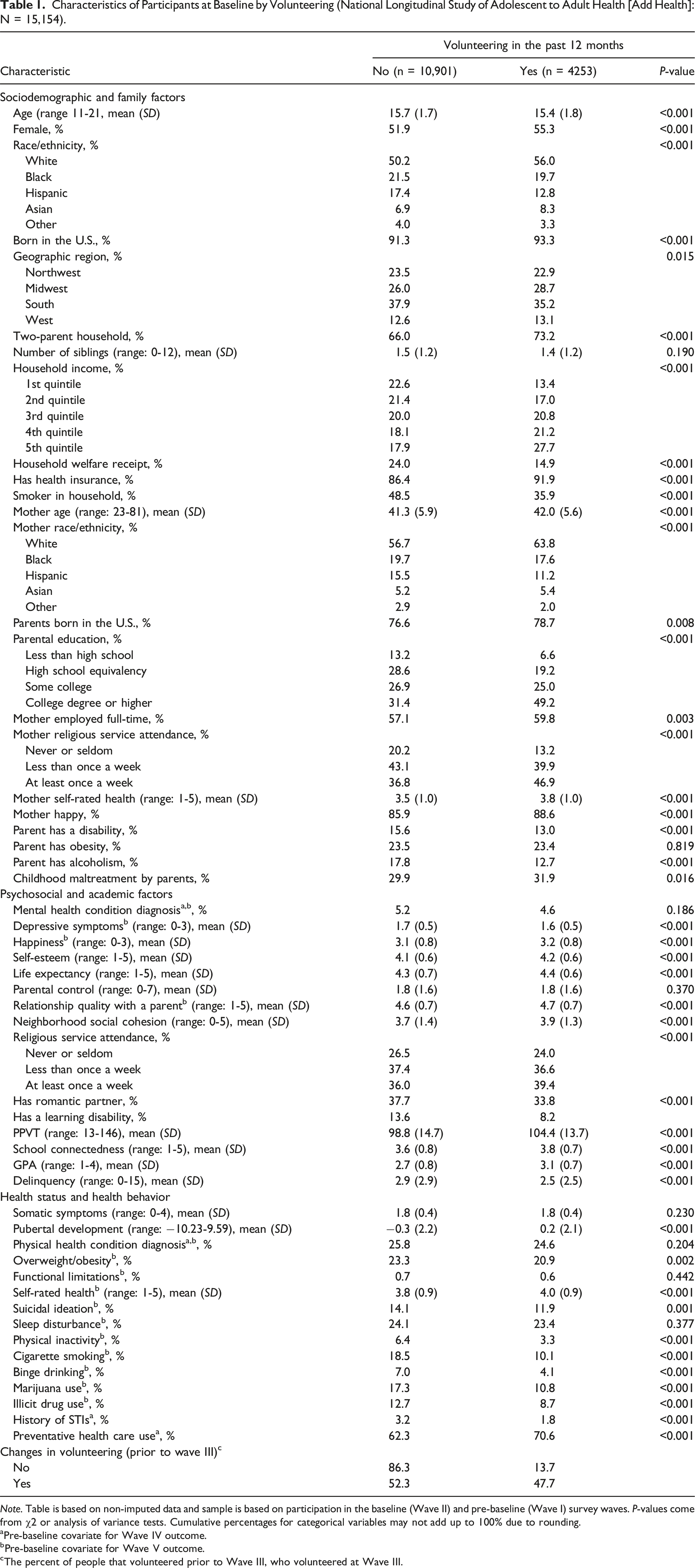
Note. Table is based on non-imputed data and sample is based on participation in the baseline (Wave II) and pre-baseline (Wave I) survey waves. P-values come from χ2 or analysis of variance tests. Cumulative percentages for categorical variables may not add up to 100% due to rounding.
aPre-baseline covariate for Wave IV outcome.
bPre-baseline covariate for Wave V outcome.
cThe percent of people that volunteered prior to Wave III, who volunteered at Wave III.
Volunteering and Subsequent Health and Well-Being in Adulthood (National Longitudinal Study of Adolescent to Adult Health [Add Health]).
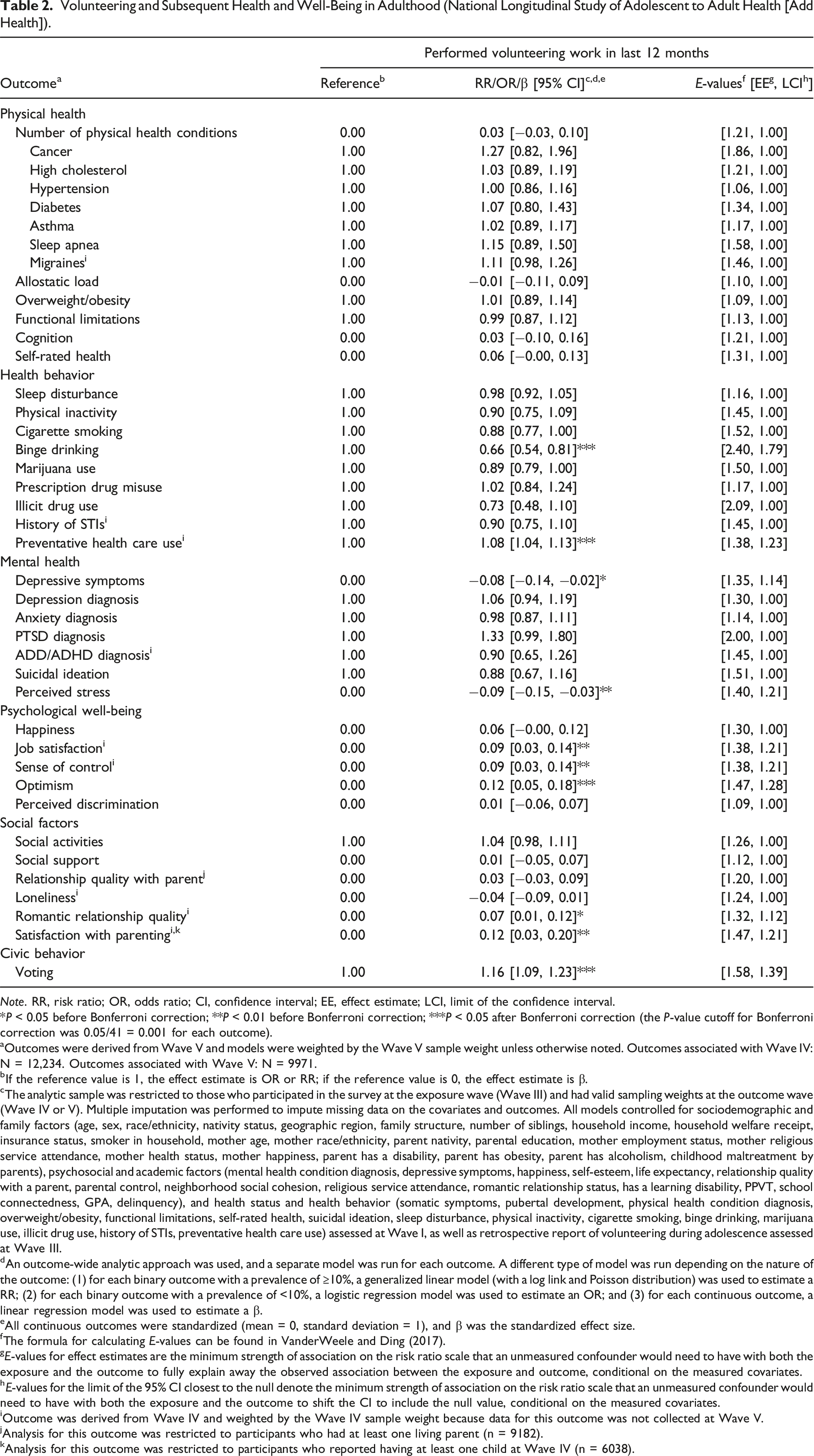
Note. RR, risk ratio; OR, odds ratio; CI, confidence interval; EE, effect estimate; LCI, limit of the confidence interval.
*P < 0.05 before Bonferroni correction; **P < 0.01 before Bonferroni correction; ***P < 0.05 after Bonferroni correction (the P-value cutoff for Bonferroni correction was 0.05/41 = 0.001 for each outcome).
aOutcomes were derived from Wave V and models were weighted by the Wave V sample weight unless otherwise noted. Outcomes associated with Wave IV: N = 12,234. Outcomes associated with Wave V: N = 9971.
bIf the reference value is 1, the effect estimate is OR or RR; if the reference value is 0, the effect estimate is β.
cThe analytic sample was restricted to those who participated in the survey at the exposure wave (Wave III) and had valid sampling weights at the outcome wave (Wave IV or V). Multiple imputation was performed to impute missing data on the covariates and outcomes. All models controlled for sociodemographic and family factors (age, sex, race/ethnicity, nativity status, geographic region, family structure, number of siblings, household income, household welfare receipt, insurance status, smoker in household, mother age, mother race/ethnicity, parent nativity, parental education, mother employment status, mother religious service attendance, mother health status, mother happiness, parent has a disability, parent has obesity, parent has alcoholism, childhood maltreatment by parents), psychosocial and academic factors (mental health condition diagnosis, depressive symptoms, happiness, self-esteem, life expectancy, relationship quality with a parent, parental control, neighborhood social cohesion, religious service attendance, romantic relationship status, has a learning disability, PPVT, school connectedness, GPA, delinquency), and health status and health behavior (somatic symptoms, pubertal development, physical health condition diagnosis, overweight/obesity, functional limitations, self-rated health, suicidal ideation, sleep disturbance, physical inactivity, cigarette smoking, binge drinking, marijuana use, illicit drug use, history of STIs, preventative health care use) assessed at Wave I, as well as retrospective report of volunteering during adolescence assessed at Wave III.
dAn outcome-wide analytic approach was used, and a separate model was run for each outcome. A different type of model was run depending on the nature of the outcome: (1) for each binary outcome with a prevalence of ≥10%, a generalized linear model (with a log link and Poisson distribution) was used to estimate a RR; (2) for each binary outcome with a prevalence of <10%, a logistic regression model was used to estimate an OR; and (3) for each continuous outcome, a linear regression model was used to estimate a β.
eAll continuous outcomes were standardized (mean = 0, standard deviation = 1), and β was the standardized effect size.
fThe formula for calculating E-values can be found in VanderWeele and Ding (2017).
gE-values for effect estimates are the minimum strength of association on the risk ratio scale that an unmeasured confounder would need to have with both the exposure and the outcome to fully explain away the observed association between the exposure and outcome, conditional on the measured covariates.
hE-values for the limit of the 95% CI closest to the null denote the minimum strength of association on the risk ratio scale that an unmeasured confounder would need to have with both the exposure and the outcome to shift the CI to include the null value, conditional on the measured covariates.
iOutcome was derived from Wave IV and weighted by the Wave IV sample weight because data for this outcome was not collected at Wave V.
jAnalysis for this outcome was restricted to participants who had at least one living parent (n = 9182).
kAnalysis for this outcome was restricted to participants who reported having at least one child at Wave IV (n = 6038).
Among health behaviors, volunteering was associated with a decreased risk of harmful health behaviors, including a 34% decreased risk of binge drinking (95% CI [0.54, 0.81]) and an 8% increased likelihood of engaging in preventative health care use (95% CI [1.04, 1.13]).
Amongst mental health outcomes, volunteering was associated with fewer depressive symptoms (β = −0.08, 95% CI [−0.14, −0.02]) and lower perceived stress (β = −0.09, 95% CI [−0.15, −0.03]).
Among psychological well-being factors, volunteering was associated with greater: job satisfaction (β = 0.09, 95% CI [0.03, 0.14]), sense of control (β = 0.09, 95% CI [0.03, 0.14]), and optimism (β = 0.12, 95% CI [0.05, 0.18]).
Among social factors, volunteering was associated with increased romantic relationship quality (β = 0.07, 95% CI [0.01, 0.12]) and satisfaction with parenting (β = 0.12, 95% CI [0.03, 0.20]).
Finally, volunteering was associated with a 16% increased likelihood of voting (95% CI [1.09, 1.23]).
There was little evidence of associations between volunteering and all other health and well-being outcomes.
E-Values
E-values suggested that some of the observed associations were moderately robust to unmeasured confounding. For example, in Wave IV, an unmeasured confounder associated with both volunteering and binge drinking by risk ratios of 2.40 each (above and beyond the covariates already adjusted for) could explain away the association, but weaker joint confounder associations could not. Further, to shift the CI to include the null, an unmeasured confounder that was associated with both volunteering and physical inactivity by risk ratios of 1.79 each could suffice, but weaker joint confounder associations could not. However, other associations, for example with physical health conditions, cognition, and self-rated health, were not especially robust to potential unmeasured confounding.
Types of Volunteering
Associations of Different Types of Volunteering and Well-Being in Adulthood (National Longitudinal Study of Adolescent to Adult Health [Add Health]) a .
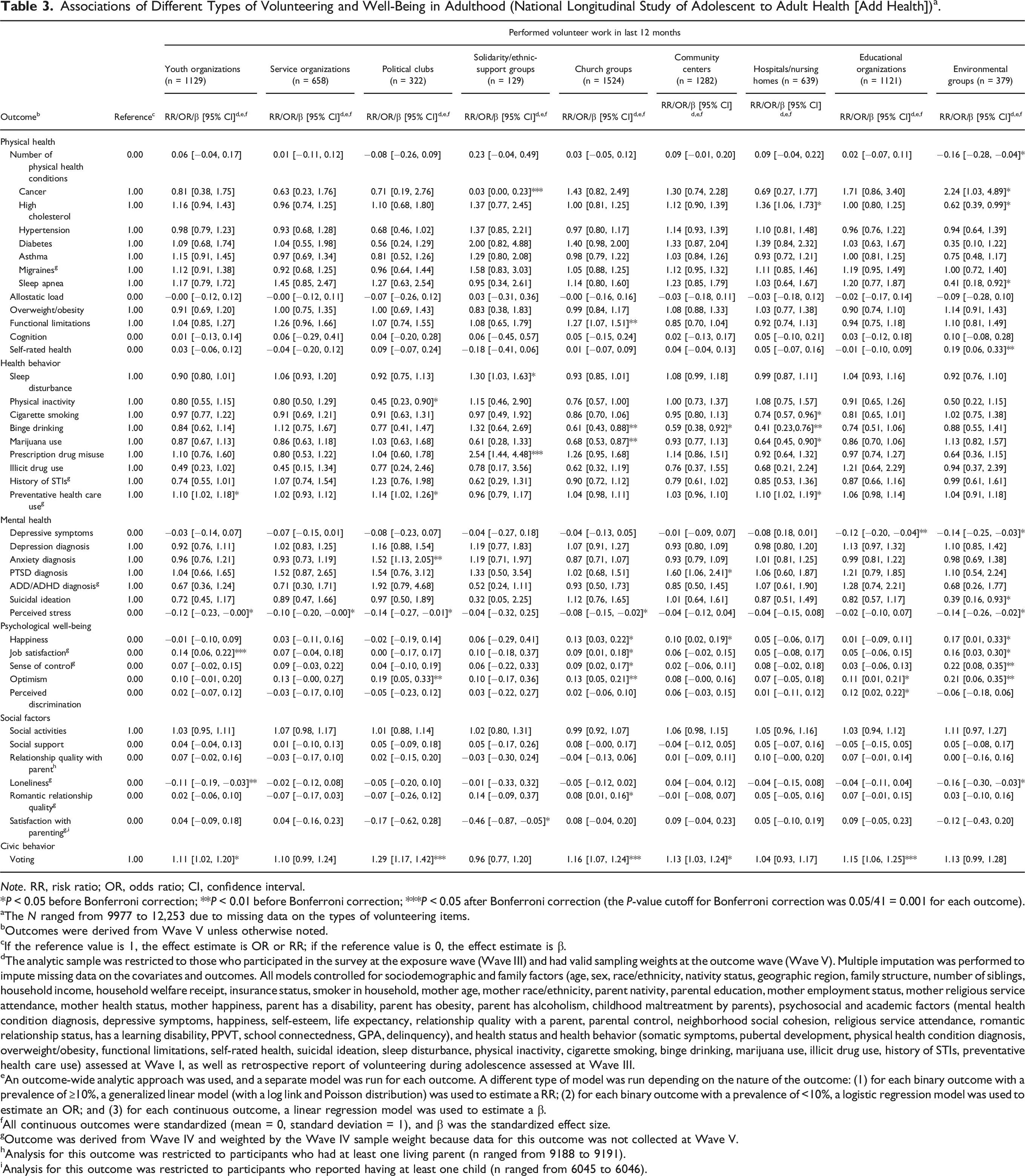
Note. RR, risk ratio; OR, odds ratio; CI, confidence interval.
*P < 0.05 before Bonferroni correction; **P < 0.01 before Bonferroni correction; ***P < 0.05 after Bonferroni correction (the P-value cutoff for Bonferroni correction was 0.05/41 = 0.001 for each outcome).
aThe N ranged from 9977 to 12,253 due to missing data on the types of volunteering items.
bOutcomes were derived from Wave V unless otherwise noted.
cIf the reference value is 1, the effect estimate is OR or RR; if the reference value is 0, the effect estimate is β.
dThe analytic sample was restricted to those who participated in the survey at the exposure wave (Wave III) and had valid sampling weights at the outcome wave (Wave V). Multiple imputation was performed to impute missing data on the covariates and outcomes. All models controlled for sociodemographic and family factors (age, sex, race/ethnicity, nativity status, geographic region, family structure, number of siblings, household income, household welfare receipt, insurance status, smoker in household, mother age, mother race/ethnicity, parent nativity, parental education, mother employment status, mother religious service attendance, mother health status, mother happiness, parent has a disability, parent has obesity, parent has alcoholism, childhood maltreatment by parents), psychosocial and academic factors (mental health condition diagnosis, depressive symptoms, happiness, self-esteem, life expectancy, relationship quality with a parent, parental control, neighborhood social cohesion, religious service attendance, romantic relationship status, has a learning disability, PPVT, school connectedness, GPA, delinquency), and health status and health behavior (somatic symptoms, pubertal development, physical health condition diagnosis, overweight/obesity, functional limitations, self-rated health, suicidal ideation, sleep disturbance, physical inactivity, cigarette smoking, binge drinking, marijuana use, illicit drug use, history of STIs, preventative health care use) assessed at Wave I, as well as retrospective report of volunteering during adolescence assessed at Wave III.
eAn outcome-wide analytic approach was used, and a separate model was run for each outcome. A different type of model was run depending on the nature of the outcome: (1) for each binary outcome with a prevalence of ≥10%, a generalized linear model (with a log link and Poisson distribution) was used to estimate a RR; (2) for each binary outcome with a prevalence of <10%, a logistic regression model was used to estimate an OR; and (3) for each continuous outcome, a linear regression model was used to estimate a β.
fAll continuous outcomes were standardized (mean = 0, standard deviation = 1), and β was the standardized effect size.
gOutcome was derived from Wave IV and weighted by the Wave IV sample weight because data for this outcome was not collected at Wave V.
hAnalysis for this outcome was restricted to participants who had at least one living parent (n ranged from 9188 to 9191).
iAnalysis for this outcome was restricted to participants who reported having at least one child (n ranged from 6045 to 6046).
Additional Analyses
Concerning the additional analyses, first, adjustment for covariates drawn from Wave III showed mostly similar results to the main analyses with covariate adjustment at Wave I with some exceptions (e.g., associations with PTSD; Supplemental Table S1). Second, using a count of the total number of different types of recent volunteering and health and well-being showed mostly similar results to the main analyses, though some new associations emerged (Supplemental Table S2). For example, in these analyses, greater volunteering across types of organizations showed evidence of associations with lower risk of physical inactivity and marijuana use. Third, using a reduced list of conventional covariates showed mostly similar associations (though more associations overall) and larger effect estimates (Supplemental Table S3). Fourth, analyses with complete cases showed mostly similar results to the main imputed analyses, with some exceptions (e.g., migraines; Supplemental Table S4).
Discussion
In a large, longitudinal, and nationally representative sample of US young adults, volunteering was associated with a range of changes to behavioral and psychosocial health and well-being outcomes (i.e., reduced risk of binge drinking, increased likelihood of engaging in preventive health care use, lower: depressive symptoms and perceived stress; higher: job satisfaction, sense of control, optimism, romantic relationship quality, and satisfaction with parenting), and an increased likelihood of voting in adulthood. However, volunteering in young adulthood showed little evidence of associations with many other health and well-being outcomes in adulthood (e.g., overweight/obesity, loneliness, etc.). Analyses assessing volunteering by organization types (e.g., environmental groups, hospitals/nursing homes) showed a range of positive (e.g., decreased suicidal ideation risk) and negative (e.g., increased risk of PTSD) outcomes depending on the category of volunteering.
Our findings align with prior literature which finds benefits to volunteering, including decreased: binge drinking 11 and depressive symptoms.14,16-18
Contrary to many prior studies, our findings suggest that volunteering may not always be good for health – in some cases, volunteering was associated with worse subsequent health and well-being. For example, certain types of volunteering were shown to be associated with adverse health outcomes (Table 3). To name a few examples, volunteering in community centers was associated with an increased risk of PTSD, volunteering in solidarity/ethnic support groups was associated with an increased risk of prescription drug misuse and sleep disturbances, and volunteering in hospitals/nursing homes was associated with an increased risk of high cholesterol. Volunteers may be unprepared for work in some settings (e.g., hospitals) where there are emergencies, deaths, and sickness, and other factors which may add strain to mental and physical health. If volunteering in some settings is perceived as stressful, it may be associated with adverse coping strategies (e.g., poorer diet). 34 This aligns with prior findings in health care settings where higher Patient Health Questionnaire-9 (PHQ-9) scores were associated with higher Empirical Dietary Inflammatory Index (EDII) scores (a diet that has been associated with increased concentrations of circulating plasma inflammatory markers) among healthcare personnel. 35 While some of these associations (e.g., volunteering for environmental groups and increased risk of cancer) may be explained by the nature of the volunteer work itself (e.g., increased exposure to unsafe chemicals), mechanisms between other associations (e.g., between educational organizations and increased perceived discrimination) require further investigation. Perhaps involvement in educational organizations increases awareness of what discrimination is and the ways in which one can be discriminated against, and therefore raises one’s awareness during times in which they experience discrimination. Others have found similarly negative associations with specific kinds of volunteer work (e.g., volunteering in political organizations and increased alcohol consumption). 11 Clearly, future research will need to assess if these findings are found across studies, when these negative associations occur, and if there are factors (e.g., the amount of time spent volunteering) that contribute to adverse health outcomes. Importantly, several associations did not remain significant after correction for multiple testing.
These findings should be considered in light of their limitations, which inspire important future directions. First, we did not assess differences in associations between volunteering and health and well-being outcomes across sociodemographic groups (e.g., sex/gender, race). Future studies should look at sociodemographic factors as moderators, as well as the mechanisms (mediators) that underly these associations between volunteering and health. Second, many of our outcomes were self-reported (e.g., presence of health conditions). However, several outcomes included objective measures (e.g., allostatic load included biomarkers of stress [e.g., blood pressure, blood samples]) which reduces the risk of self-report bias. Third, while we evaluated different volunteer settings, we did not look at the types of volunteer work participants were doing in these settings. For example, it is likely that volunteering within hospital/nursing homes is more stressful in some roles (e.g., support groups) than others (e.g., in a hospital gift shop). However, assessing type of volunteering in general is an improvement over many prior cohort studies which only evaluate the presence or absence of volunteering. Fourth, the volunteering item in the exposure wave assessed any recent volunteering within the past 12 months, while the measure used to adjust for adolescent volunteering captured regular volunteering (which missed individuals who volunteered occasionally). Fifth, data for this study were collected prior to the COVID-19 pandemic, and thus may not account for meaningful changes brought on by the pandemic and other societal shifts (e.g., associations between volunteering and health and well-being outcomes may look different in a post-COVID climate, societal changes [e.g., ongoing political polarization in the nation] may influence some types of volunteering [e.g., volunteering with political clubs], etc.). Further research is needed to assess these associations in post-pandemic contexts. Finally, the 6-8-year lag between the covariates and volunteering in our main analyses may be too temporally distant for the covariates to sufficiently address potential confounding. This is an important limitation. However, in Supplemental Table S1, we also adjusted for covariates assessed at the same time as the volunteering in Wave III. When using this more conservative approach, that introduces the risk that models might be adjusting for potential mediators (it is difficult to determine whether results reflect adjustment for confounding, mediation, or both), results were mostly similar, and E-value analyses suggest some of the main results were somewhat robust to residual confounding. Future research should use longitudinal data with less time between covariate and exposure waves.
Volunteering during young adulthood was associated with a range of beneficial health and well-being outcomes in adulthood. However, certain types of volunteer work were also associated with some adverse health outcomes. Volunteering organizations, policymakers, and interventionists should carefully consider the ramifications of volunteering in young adulthood and carefully curate volunteer opportunities that promote health and mitigate adverse outcomes associated with volunteering. With further research, volunteering of specific types and amounts in young adulthood may be a way to improve societal well-being and promote health across the lifespan. Volunteering has been associated with improvements to numerous health and well-being outcomes. However, most studies focus on older adults and less is known about how volunteering in young adulthood is associated with improved health and well-being. In this study, we examined whether changes in volunteering (both any volunteering and volunteering in specific settings) from adolescence to young adulthood were associated with 41 health and well-being outcomes in adulthood. While volunteering was generally associated with improved health and well-being outcomes, some volunteer settings were associated with a range of beneficial and harmful health and well-being outcomes. Volunteering is increasingly being considered as a public health intervention. Our findings suggest that there is more work needed to uncover the conditions under which volunteering is health promoting and aim to minimize potential adverse effects associated with some types of volunteering.So what?
What is Already Known on This Topic?
What Does This Article Add?
What are the Implications for Health Promotion Practice or Research?
Supplemental Material
Supplemental Material - Volunteering in Young Adulthood: Complex Associations With Later Health and Well-Being Outcomes
Supplemental Material for Volunteering in Young Adulthood: Complex Associations With Later Health and Well-Being Outcomes by Julia S. Nakamura, MA, Renae Wilkinson, PhD, Marisa A. Nelson, BA, Etsuji Suzuki, MD, PhD, and Tyler J. VanderWeele, PhD in American Journal of Health Promotion.
Footnotes
Acknowledgments
We would like to thank Sofie Jensen, Jiayi Li, Michelle Lin, Cherise Kwok, Rachel Leong, and Isaac Ng for their contributions to this manuscript. This research uses data from Add Health, funded by grant P01 HD31921 (Harris) from the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD), with cooperative funding from 23 other federal agencies and foundations. Add Health is currently directed by Robert A. Hummer and funded by the National Institute on Aging cooperative agreements U01 AG071448 (Hummer) and U01AG071450 (Aiello and Hummer) at the University of North Carolina at Chapel Hill. Add Health was designed by J. Richard Udry, Peter S. Bearman, and Kathleen Mullan Harris at the University of North Carolina at Chapel Hill.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Tyler J. VanderWeele reports receiving personal fees from Flerish Inc. and Flourishing Metrics. Julia S. Nakamura, Renae Wilkinson, Marisa A. Nelson, and Etsuji Suzuki have no competing interests to declare that are relevant to the content of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Vanier Canada Graduate Scholarships (Vanier CGS) Program – Canadian Institutes of Health Research (CIHR) to JSN. The funding sources played no role in the study design; in the collection, analysis and interpretation of data; in the writing of the report; and in the decision to submit the article for publication.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.