
Abstract
Evidence shows that well-being for mental health in prison is an important component of prison rehabilitation efforts—including notably lowering recidivism rates after release. While support for well-being initiatives in U.K. prisons has grown, few prison programs offer a health-promoting focus or invest in well-being interventions. Therefore, this study seeks to replicate and extend emerging data on an innate health intervention. Volunteers from HMP Nottingham (N=127) participated in normal prison programming. The intervention group (n=66) received an additional 3-day intensive. This study found higher levels of innate health, self-control, well-being, and prosocial behavior and lower levels of aggression within the intervention group and as compared with the control group. Next, we conducted a mediation analysis to test if innate health, self-control, and/or social desirability bias could explain these positive changes. Importantly, innate health did play a mediating role equivalent to and/or partnering with self-control, whereas social desirability bias did not.
Keywords
Interest in how to promote positive outcomes in community mental health (World Health Organization, 2021) and the criminal justice system (Epperson et al., 2021; Ward et al., 2022) has grown over the last 30 years. Evidence shows that human beliefs about one’s internal development capacity can improve well-being even in the face of illness (Smith et al., 2019), stress (Park, 2010), and disasters (Park, 2016) and have a significant impact on the framing and reasoning one makes about life events (i.e., meaning-making; Baumeister, 1991; Park, 2010) and about health (i.e., primal world beliefs; Clifton & Kim, 2020). Changes in appraisal and meaning-making are well-recognized processes for improving well-being outcomes such as emotional regulation and coping activities (Lazarus & Folkman, 1984). So too in criminology. Research shows that shifts in meaning-making, mindset, and identity play a “critical role in desistance from criminality and assist in the process of successful reentry” (Lerman & Sadin, 2022, p. 2). Further research into the types of interventions that facilitate these changes and the mechanism(s) behind these shifts is needed.
Prison programs that use a combination of methods that build skill acquisition, develop self-control, and promote perspective-taking have reliably demonstrated promising outcomes (McGuire, 2020). Complimentary interventions (added to traditional offerings) focused on fostering these strengths within prison environments have already demonstrated a significant impact on measures related to well-being (e.g., forgiveness therapy: Praptomojati & Subandi, 2020; compassion development: Ptacek & Daubman, 2020; mindfulness-based cognitive therapy: Song et al., 2021). Pettus et al. (2021) identified healthy thinking patterns, effective coping strategies, positive social engagement, and positive interpersonal relationships as essential to increasing well-being—especially needed in prison programming—among people who face individual and structural barriers.
In this study, we build and extend previous research into the Insight to Well-being (Beyond Recovery CIC et al., 2019) program. Designed to teach participants to “realize for themselves that they are not broken” (Dingle et al., 2023, p. 4), this program teaches a realization capacity or innate health stance that is rarely delivered directly, articulated clearly, operationalized, and/or empirically evidenced. Thus, this study examines this largely overlooked construct within criminology. How does realization, understanding, or changes in meaning-making about one’s innate health impact important psychosocial variables in a high-risk population? Furthermore, questions about the “practice framework” for positive change toward desistance (Fox, 2022) prompted us to investigate the role innate health can play as a potential mechanism to explain these results—as compared with and contrasted with self-control—suggesting distinct and potentially complementary mechanisms requiring future study.
Innate Health
Compared with the general population, imprisoned populations report higher levels of self-harm/suicide (Zhong et al., 2021), severe mental illness (Fazel et al., 2016), and substance abuse (Baranyi et al., 2019). Evidence demonstrates that (a) support for well-being initiatives in U.K. prisons has grown (Tweed et al., 2021); (b) well-being for mental health in prison is an important component of prison rehabilitation efforts (Woodall & Freeman, 2020); and (c) improved levels of well-being can significantly lower recidivism rates after release (Wallace et al., 2020)—however, few prison programs offer a health-promoting focus (Woodall & Freeman, 2021) or invest in well-being interventions (Turner et al., 2021). Criminology research theory (Bersani & Doherty, 2018), prisoner narratives (Maier & Ricciardelli, 2021), and positive criminology (Ronel & Elisha, 2011) recognize that internal sources can act as a primary catalyst for change. The realization of innate human potential is central to the Insight to Well-being program under investigation.
The Insight to Well-being program is based on the work of Sydney Banks (1998; Quiring, 1975; Suarez et al., 1987). Within the scientific literature, Sedgeman (2005) coined the term “innate health” as a capacity for health realization, where a positive state of mind can be accessed and sustained regardless of circumstances. Larimer (2008) further defined innate health as “an inherent human capacity to access the wisdom and creativity required for optimal learning and development, regardless of conditions or circumstances” (p. 4). In the prison environment, innate health was defined as a source of resilience “always available to people no matter what circumstances, stressors, or traumatic events they encounter over time” (Kelley et al., 2018, p. 2832).
While the range of these developing definitions implies that circumstances do not matter, there is a central theoretical claim pointing to an underlying structure that could enable factors such as mental health or self-control to be awakened or trained even in the face of terrible conditions. This idea is not so different from Muraven and Baumeister’s (2000) notion of self-control as a “moral muscle” that needs practice to function at a high level but was always there. Indeed, the shared theoretical foundation, that humans have an innate potential for realizing one’s capacity, can be found across psychological literature. For example, the concepts of self-realization (Ryff, 1989), inner strength (Rose, 1990), and a natural inherent growth tendency (Ryan & Deci, 2000)—all share this idea of a “basic part of our essence” (Maslow & Hoffman, 1996, p. 83). Link et al. (2019) demonstrated the need for such strength-based programming among the prison population, concluding that “being one’s best self” increases beneficial outcomes across employment, relationships, and reentry into communities. Fox’s (2022) desistance framework review concluded that successful interventions within criminology emphasized individual strengths and enhanced prosocial identities. Similarly, innate health programming strives to improve well-being outcomes, moving beyond the content of intrusive or negative thoughts (Halcón et al., 2007), or deficit-based interventions, to understanding one’s hidden potential for creativity, wisdom, and clarity (innate health).
Empirical evidence across innate health-focused interventions found positive changes in levels of (a) stress, depression, and anxiety as well as enhanced well-being among female Somali refugees in the midwestern region of the United States (Robertson et al., 2019); (b) drug use, well-being, and commitment to sobriety among residents at a Northeastern, U.S. treatment facility (Denkers & Catherine-Gray, 2022); and, (c) in well-being, resilience, and impulse control among adolescents living in London, England (Kelley et al., 2021). While there are several small and promising studies (Catherine-Gray et al., 2022; El-Mokadem et al., 2023; Felix et al., 2022; Rees-Evans & Pevalin, 2017), the first large-scale randomized controlled trial of an innate health intervention demonstrated significant improvements in communication, decision-making, problem-solving, emotional regulation, and resilience in children (Green et al., 2021a, 2021b).
The first prison study conducted on the Insight to Well-Being program (before it was manualized), examined the impact of the program delivered over 10 weeks to 92 men living in HMP Onley, United Kingdom (Kelley et al., 2018). Compared with the control group (n = 39), the treatment group (n = 53) post-intervention demonstrated significant improvement in levels of well-being, purpose in life, anxiety, and anger. Following this study, Kelley et al. (2022) examined the same program delivered in a 3-day intensive format (15 hr of training) to men (N = 132) incarcerated for sexual violence at HMP Rye Hill, United King. Compared with the control group (n = 65), the treatment group (n = 67) demonstrated significant decreases in depression, anxiety, anger, and low self-control as well as significant increases in well-being. Dingle et al. (2023) expanded this research into women (N = 90) living in a Pacific Northwest United States incarceration facility receiving the Insight to Well-being program over 10 weeks (20 hr). Recruited from a medium security facility, participants were randomized to either a treatment (n = 49) or a waitlist control (n = 41). This study found further support for reductions in psychological distress (i.e., stress, depression, and bolstering of well-being) and significant baseline to post-treatment and baseline to 6-month reductions in trauma-related symptoms among participants in the intervention condition. This analysis supports previous claims that this intervention supports “mentally healthier” lives (Kelley et al., 2018) and could provide a transdiagnostic treatment approach.
In addition, Dingle et al. (2023) were the first to publish mediation analyses to investigate the effects of innate health interventions. However, they tested whether changes in psychological inflexibility, instead of changes in innate health, were responsible for improvements in outcome measures. Their mediation analyses demonstrated a significant indirect effect of treatment via psychological inflexibility on post-course outcomes (i.e., trauma symptoms, emotional dysregulation, and global mental health), indicating that the reduction in psychological inflexibility might be responsible for the beneficial effects of the program. This does not shed any light on the effects of the mechanism that the program targets to influence—innate health.
While these studies are promising, it is puzzling why no study has tested whether the key construct of innate health (awareness of one’s capacity for wisdom, creativity, and clarity) causes beneficial outcomes. To test whether innate health causes these changes, a mediation analysis must be performed. This statistical test demonstrates whether the effects of the intervention are likely to be caused by innate health. As innate health has not been tested this way before, it is also important to compare this new construct with a known, reliable, and tested measure, one that has already been proven to have a significant impact within the prison setting. Perhaps the single most widely acknowledged concept within the criminological literature as “one of the strongest correlates to crime” is self-control (Burt, 2020, p. 2).
Self-Control
Self-control is widely considered the key mediating factor for outcomes related to one’s ability to override, change, or interrupt undesired emotional and behavioral responses (Tangney et al., 2004). Investigations into self-control have demonstrated a robust association between low self-control and deviance (Vazsonyi et al., 2017) and maladaptive behaviors (i.e., substance misuse, recidivism, and failure to positively adapt) and between high self-control and adaptive behaviors such as prosocial behaviors (Malouf et al., 2014). Widely applied in criminology (Gottfredson & Hirschi, 1990), self-control theory demonstrates cross-cultural applicability (Vazsonyi et al., 2021), and low self-control predicts antisocial outcomes among immigrants (Kundakova et al., 2022) as well as other serious social consequences (Burt, 2020). However, self-control is not itself a permanent trait but a “set of skills, capacities, and behaviors that we need to ‘operate’ in a self-regulation feedback loop” (Gillebaart, 2018, p. 4), which seems to be related to social and environmental contexts. However, interventions that improve self-control are considered an integral aspect of reducing crime and delinquency and promoting overall health outcomes (Piquero & Rocque, 2020). While Kelley et al. (2022) found a significant increase in self-control for men incarcerated for sexual violence offenses, mediation analyses were not conducted. In addition, few studies examining high-risk populations, such as men living in prison, control for social desirability (Malouf et al., 2014). This is especially important because social desirability bias can threaten the validity of self-report assessments.
Study Aim
The primary aim of this study is to replicate research on the effects of an innate health intervention on well-being and mental health among men living in prison and to extend research in three ways. The first extension concerns additional dependent variables: Does the intervention, next to well-being, also affect moral self-esteem, aggression, drug abuse, and anti- and pro-social behavior? The second extension is the test of the mechanism that is assumed to cause the beneficial outcomes of the intervention, a mediation analysis: Are changes in innate health responsible for changes in outcome measures? The third extension is the test of alternative explanations for the expected effects: Are changes in self-control, rather than those in innate health, responsible for changes in outcome measures? In addition, we controlled for social desirability bias. This bias tends to be particularly disturbing for the results regarding individuals living in prison (Cobo et al., 2021).
Method
Participants
A total of 127 participants were recruited from the Incentivized Substance Free Living (ISFL) wing (Her Majesty’s Prison and Probation Service, 2019) of Nottingham Prison (category B: housing local, long-term, and high-risk men in England). All residents admitted to the ISFL wing were voluntarily living on the wing after being fully vetted by a team located at the prison, including a psychologist. The ISFL initiative was designed to provide voluntary drug testing and better living conditions (including various program opportunities and preference accommodation). Program participants were recruited via flyers or word of mouth (invited by agency staff and/or previous participants). The design provided the following parameters for this study: (a) inclusion and exclusion criteria were met through the residency process; (b) residents living on the wing were encouraged to enroll in the program of their choice; and (c) an onsite research supervisor visited the wing regularly to invite residents to enroll in the research (66 from the treatment and 61 from the waitlist conditions). While all participants were enrolled in various prison programs, only the intervention group received the additional 3-day Insight to Well-Being intensive.
Participants in both groups: (a) had an average age of 32 years, with ages ranging from 18 to 56; (b) had an equivalent level of education (10% had reached primary school level or below, 53% secondary school, 29% college or sixth form and 8% university or higher); (c) were incarcerated, on average, eight times before; and (d) spent an average 19 months in prison during the current incarceration varying from under a month to 21 years.
Only one difference between the two conditions was observed; participants in the treatment condition were on the wing for an average of 4 weeks longer than participants in the waitlist condition. This may be a direct result of the researchers arriving after the Insight to Well-Being program had begun, so men living on the wing longer had already enrolled in the program, leaving newer arrivals available for the wait-list control condition. While the total dropout rate was 24%, the treatment condition filled out fewer post-surveys (42: 36% dropout rate) than the waitlist condition (52: 15% dropout rate). This is likely because the waitlist condition had no program to drop out of and was available on the wing at the time of post-survey collection. Reasons for dropping out were transferred to another prison, released, stopped participation, or other activities (e.g., education or work).
Procedure
A quasi-experimental study with a wait-list control group was conducted from April 1, 2019, through October 19, 2019. Reviewed by Her Majesty’s Prison and Probation Service and approved by the Governor of Nottingham Prison, ethical clearance was obtained from the Human Research Review Committee of the California Institute of Integral Studies.
Participants from the ISFL wing (which, at any given time housed 125 men) were verbally informed by the onsite research supervisor about the study, provided a three-page Participation Information Sheet, and assured of voluntary participation with anonymous data processing. Participants received a £3 phone credit for enrolling in the study. After obtaining informed consent, participants were assigned a unique identifier to ensure confidentiality. Surveys, constructed in Qualtrics and administered by the onsite research supervisor, in a private room using an offline electronic tablet, were conducted before or within a week following the intervention.
The treatment program remains consistent with Dingle’s et al. (2023) description of the Insight to Well-Being program where at least two facilitators emphasize experimental exercises, storytelling, and reflection. The only change was program length: a 3-day intensive (15 hr) instead of 10 weeks (20 hr). Unlike traditional prison programs, the focus was not on risk factors, behavioral problems, or mindfulness practices but on the central assumption that innate health exists, that it is universal, accessible, and—when understood—transformative.
Instruments
The questionnaires included 87 randomized items (ground variables and items measuring nine concepts). Seven of these concepts were scored on visual analog scales rather than on traditional categorical scoring scales. Visual analog scales tend to feel more intuitive to participants, can save space on the screen, and are more sensitive to minor changes (Toepoel & Funke, 2018).
Dependent Variables
Well-being was assessed using seven items from the short version of the Warwick-Edinburgh Mental Well-Being Scale, such as “I’ve been thinking clearly.” This scale has been found to have good psychometric qualities (Haver et al., 2015). Participants responded on visual analog scales ranging from “never” to “all the time.” The scale formed a reliable measure in this study (Cronbach’s α total = .87; αbefore = .83; αafter = .93).
Three psychosocial concepts from the Dutch “Connectedness Project” (De Jong & Denkers, 2020; Denkers & De Jong, 2020) were integrated into this study: moral self-esteem, anti-, and pro-social behavior. This project developed tools for assessing psychosocial concepts and behaviors among high-risk youth, utilizing concise wording and graphical support (constructed by a street artist) to enable independent participation for individuals with moderate learning disabilities and cognitive impediments. The participants in the current study completed the two-item moral self-esteem scale (e.g., “Have you been a good/bad person [last three months]?”), the three-item antisocial behavior scale (e.g., “Did you damage things or people [last 3 months]?”), and the three-item prosocial behavior scale (e.g., Did you help others [last 3 months]?’). All items were rated on visual analog scales ranging from, for example, “did not damage” to “damaged a lot.” The correlation between the moral self-esteem items was .49 (both before and after this was .48). Reliability (Cronbach’s α) of the two scales concerning pro- and anti-social behavior were, respectively, .59 (before .46 and after .67) and .62 (before .58 and after .67). The relatively low reliability is attributed to the three items for antisocial behavior reflecting distinct factors (aggression, stealing, and drugs), underlying traditional tools for measuring delinquent behavior (Sanches et al., 2016; Weerman, 2011). Prosocial items represent the opposite of the antisocial behavior scale, encompassing repairing, giving, and healthy behavior.
To test drug use, participants were asked “How often during the last 3 months did you use the following substances?” and asked to respond to a list of eight distinct types of drugs (e.g., cannabis and cocaine; Berman et al., 2004, 2007). Participants answered on visual analog scales with as anchor-points “never,” “once a month,” “2 to 4 times a week,” and “more often.” The eight drug use items form a reasonably reliable scale, with Cronbach’s αtotal = .71 (αbefore = .67; αafter = .67).
The level of aggression was measured using a short version of the Buss and Perry (1992) Aggression Questionnaire scale (Bryant & Smith, 2001; Diamond & Magaletta, 2006). Eight items (e.g., “Given enough provocation, I may hit another person” and “I wonder why sometimes I feel so bitter about things”) were scored on a five-point rating scale, ranging from “very unlike me” to “very like me.” This scale demonstrated reliability in this study (Cronbach’s αtotal = .91; αbefore = .89; αafter = .94).
Mediating Variables
Innate health scale
Innate health was assessed using a seven item scale (e.g., “I concentrate on things that make me feel bad” [reversed], “I take negative thoughts seriously” [reversed], and ‘I know I’m part of something good’; Denkers & Catherine-Gray, 2021). Specifically designed to gauge individuals’ alignment with assumptions about innate health concepts such as thought, consciousness, and mind, the items were scored on visual analog scales ranging from “never” to “always.” The scale exhibited reliability, with Cronbach’s αtotal = .81 (αbefore = .82; αafter = .82).
Brief self-control scale
The brief self-control scale (Tangney et al., 2004) consists of 13 questions assessing participants’ willingness to control thoughts, emotions, and impulses to conform to life’s normal demands (e.g., “I am good at resisting temptation”), is frequently used (de Ridder et al., 2012), and demonstrates strong reliability (Cronbach’s αtotal= .86; αbefore = .85; αafter = .88). Participants rated items on visual analogue scales ranging from “not at all” to “very much.”
Social desirability scale
To control for social desirability bias (Crowne & Marlowe, 1960), participants completed an eight-item scale (e.g., ‘I’m always willing to admit it when I make a mistake’; Gorsira et al., 2018) on visual analog scales, with responses ranging from “never” to “always.” The scale displayed good reliability, with Cronbach’s α total = .82 (αbefore = .77; αafter = .86).
Analytic Strategy
All analyses were conducted using SPSS 29. Pearson correlations were employed to explore relationships between variables. In line with Baron and Kenny (1986), evidence of relationships between mediators and dependent variables is important as it indicates if mediation is possible. Next, mean differences between the treatment and waitlist conditions, both before and after the program, on the dependent and mediating variables were examined using analyses of variance. These analyses check for differences between conditions before the intervention took place. Differences between conditions before an intervention took place can complicate the interpretation of any further results. Subsequently, generalized estimating equations (GEE) analyses were performed to assess the impact of the condition (treatment versus waitlist) by time (before versus after) on the outcome measures and establish mediation effects.
The GEE method was chosen for its suitability in analyzing longitudinal response data (Hanley et al., 2003). It estimates parameters while controlling for within-subject correlated errors present in longitudinal data (Liang & Zeger, 1986; Morrow-Howell et al., 2003). Before entering into the equations, all measurements were standardized into z-scores.
Initially, GEE analyses were conducted on the mediating variables of innate health and self-control to test the assumed influence of the treatment on these variables. Both analyses included condition (control versus treatment), time (first versus second wave), and condition by time as independent variables. A positive and significant condition by time interaction term would indicate relative improvement of the outcome measures in the treatment group over time compared with the waitlist group. Here, in line with Baron and Kenny (1986), we assume that mediation can only occur if the mediator is affected by the treatment (in this case indicated by a condition by time interaction). Social desirability was then added to control for its influence.
Next, GEE analyses were applied to the dependent variables: well-being, moral self-esteem, pro- and anti-social behavior, drug use, and aggression. The same condition, time, and condition by time model was used. In the case of a significant condition by time interaction term, innate health, and self-control were separately added to test for possible mediating effects. A reduction of at least by 3.84 (p < .05) or 6.64 (p < .01) in Wald χ2 for the effect of condition by time after entering a mediator into the equation would indicate a mediation effect. Finally, social desirability was added to check whether the results might have been caused by this bias.
Results
This study sought to describe how innate health can impact important psychosocial variables in a high-risk population. To clarify the relationships between variables a correlation analysis was conducted (Table 1). All correlations in Table 1 were in the expected direction and significant with p < .001, except for the relationships between prosocial behavior and social desirability bias (p < .05) and between prosocial behavior and drug use (p < .01), which were weaker. Results indicate moderate to strong correlations between the dependent variables and innate health, and the dependent variables and self-control, indicating these data can be further explored according to the proposed analytic strategy
Correlation Analysis for Psychosocial Variables
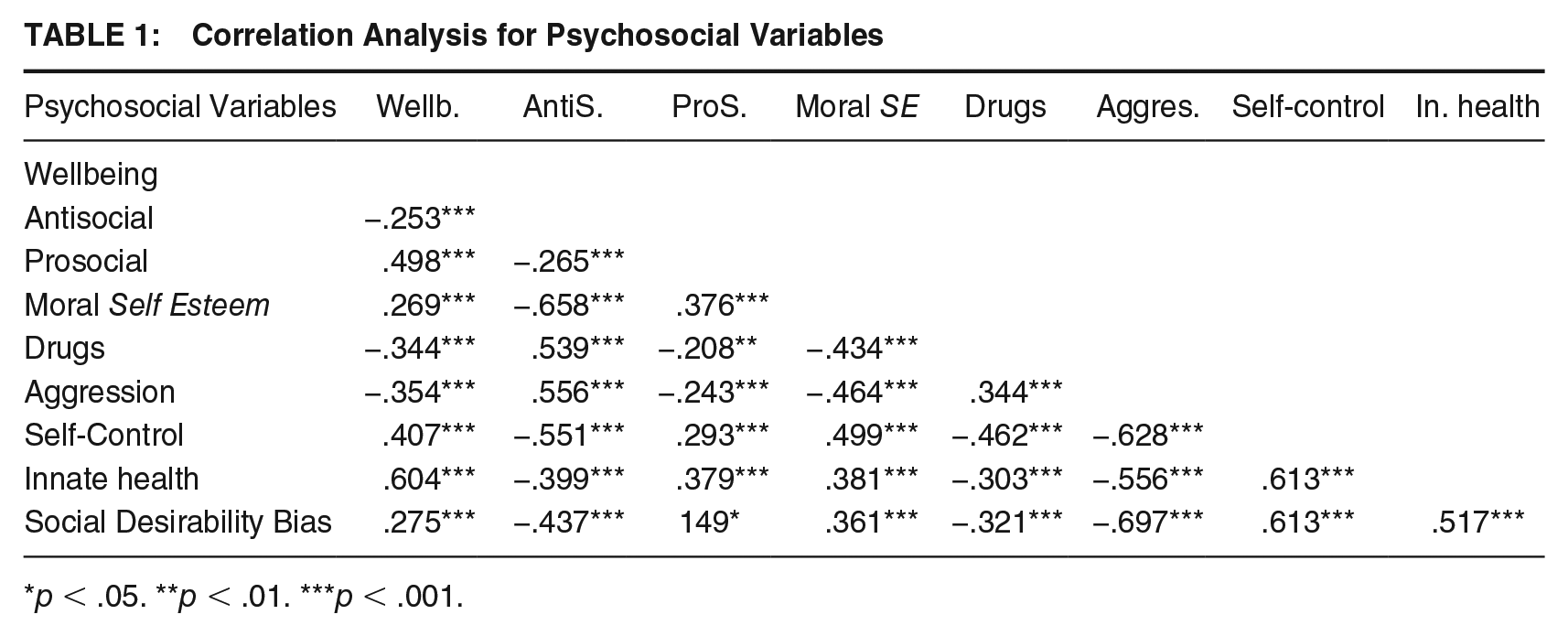
p < .05. **p < .01. ***p < .001.
To ensure no significant differences existed between the groups means and standard deviations were examined before the program (Table 2). No significant differences between conditions were found on innate health, self-control, social behavior, or moral self-esteem were seen before the program.
Means and Standard Deviations in Treatment and Wait-List Conditions Before and After the Program
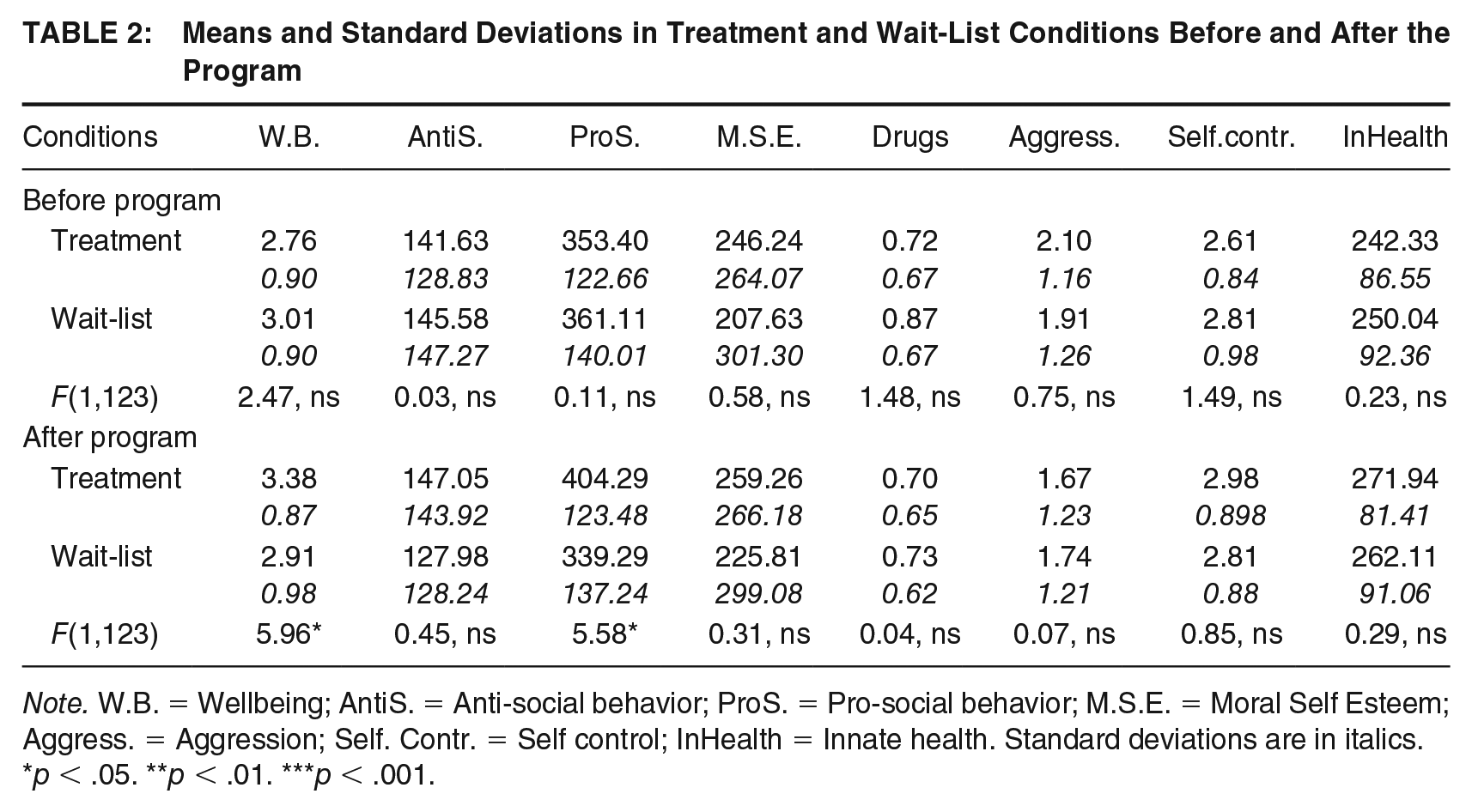
Note. W.B. = Wellbeing; AntiS. = Anti-social behavior; ProS. = Pro-social behavior; M.S.E. = Moral Self Esteem; Aggress. = Aggression; Self. Contr. = Self control; InHealth = Innate health. Standard deviations are in italics.
p < .05. **p < .01. ***p < .001.
Effects of Treatment
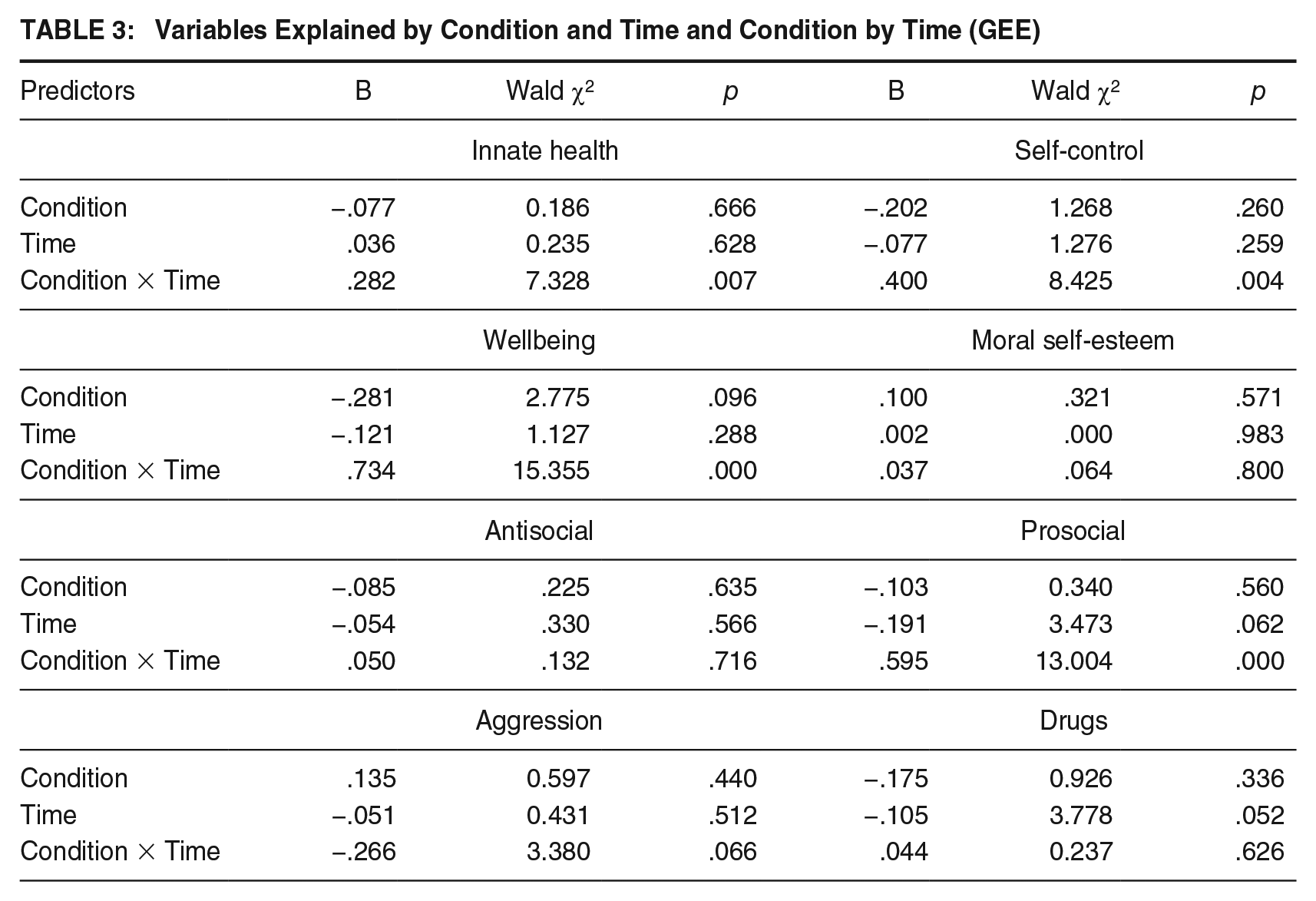
Our initial question is whether a 3-day innate health intervention could influence participants’ levels of innate health, self-control, well-being, moral self-esteem, aggression, drug use, and anti- and pro-social behavior. First, Table 2 demonstrated a post-treatment difference between conditions with higher levels of well-being (η2 = .062) and prosocial behavior (η2 = .058) among the intervention group. Second, a series of (GEE) analyses were conducted to test the effects of condition (treatment versus waitlist), time (pre-versus post-treatment), and their interaction on outcomes (Table 3). We found a positive condition by time interaction effect for both mediating variables, innate health, and self-control. This suggests that compared with the participants on the waitlist, participants in the treatment condition reported improvements in both mediating variables. With regards to the dependent variables Table 3 reveals similar positive effects on well-being and prosocial behavior. In addition, a marginally significant condition by time interaction was found for aggression. No direct effects were found for condition or time on any of these variables. Table 3 further reveals no condition-by-time interaction effect on moral self-esteem, antisocial behavior, or drug use. The lack of effect for these variables might be a consequence of the positive effects of residing in a specialized (drug-free) wing, the short duration of the intervention itself, or the lack of follow-up data.
Variables Explained by Condition and Time and Condition by Time (GEE)
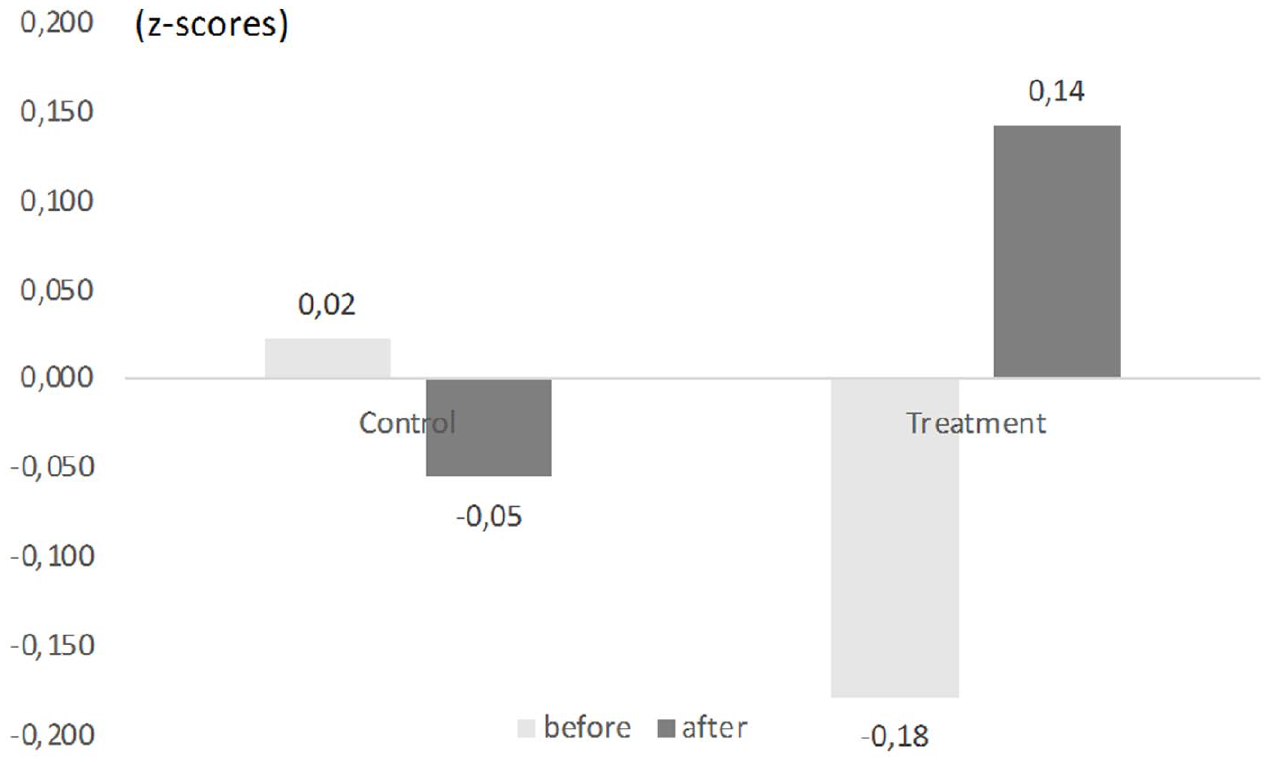
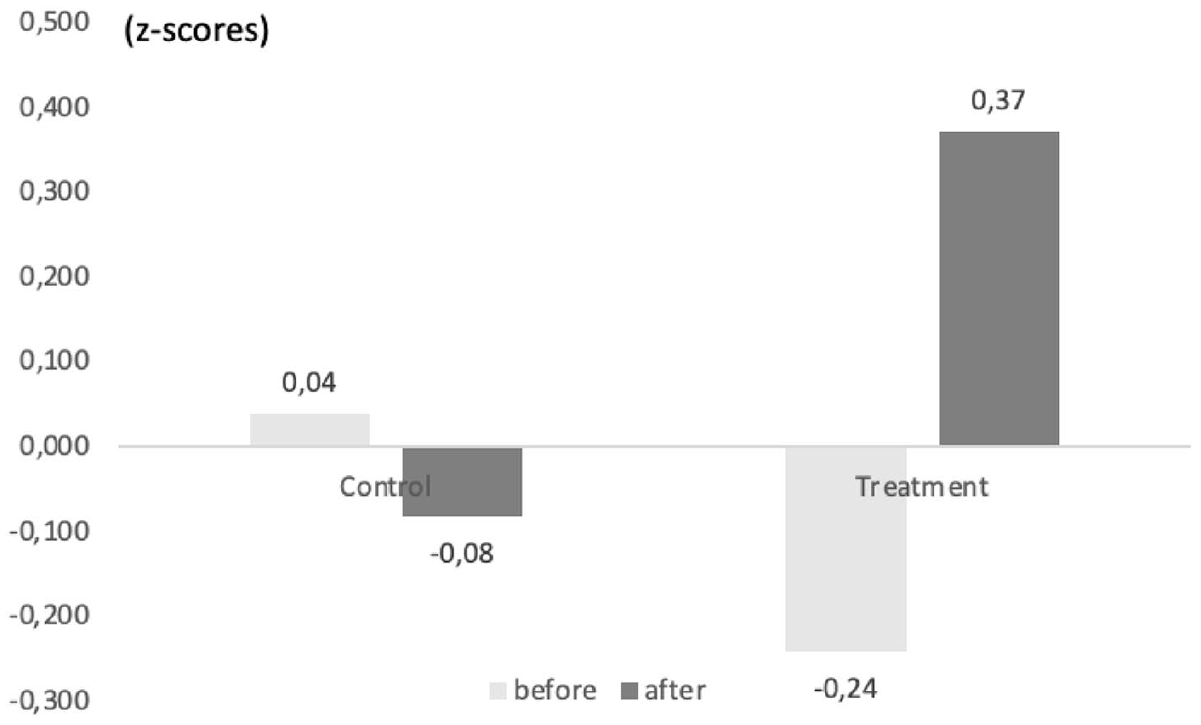
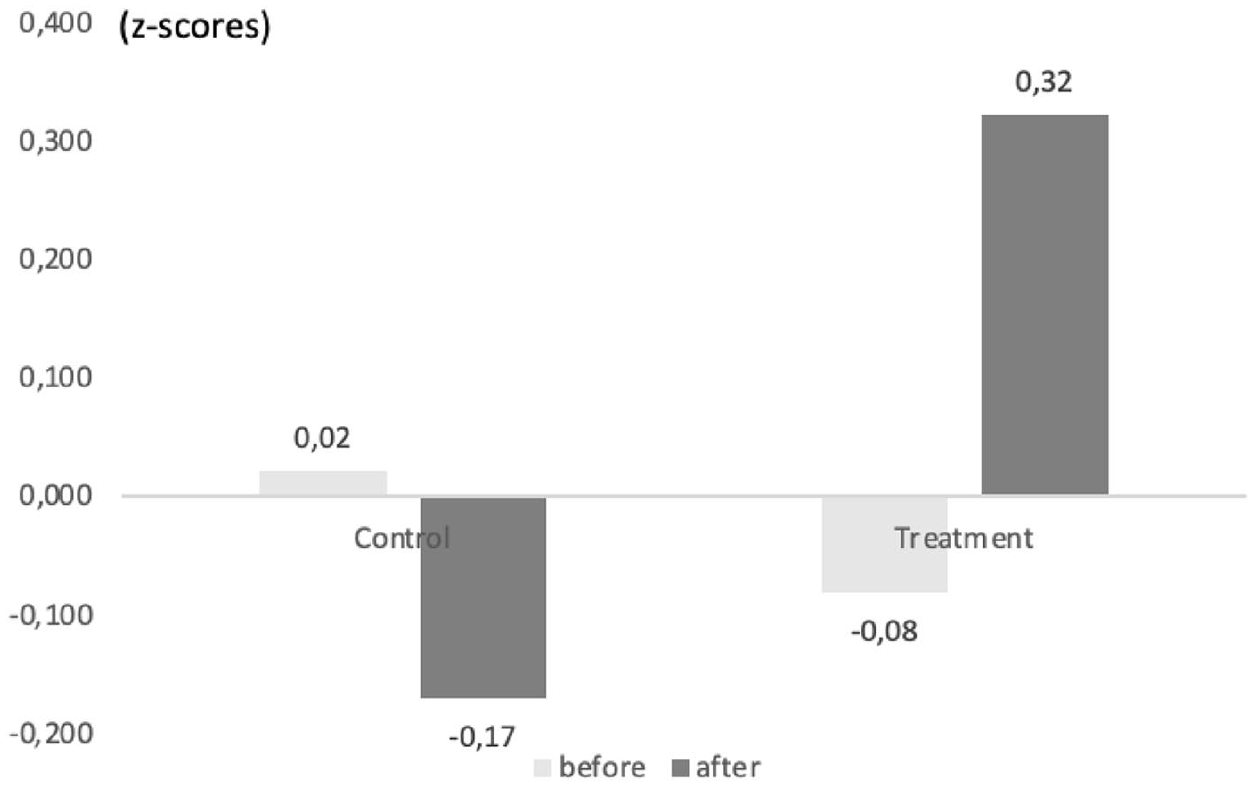
To visualize the condition by time interaction effects, Figures 1 through 5 depict the means (z-scores) of innate health, self-control, well-being, pro-social behavior, and aggression. Positive effects are seen across all outcomes; however, self-control, well-being, prosocial behavior, and aggression also suggest a pattern of slight deterioration in the waitlist condition. This is important as it might imply that the lack of intervention is not a “harmless” state but may lead to a worsening of psycho-social conditions.
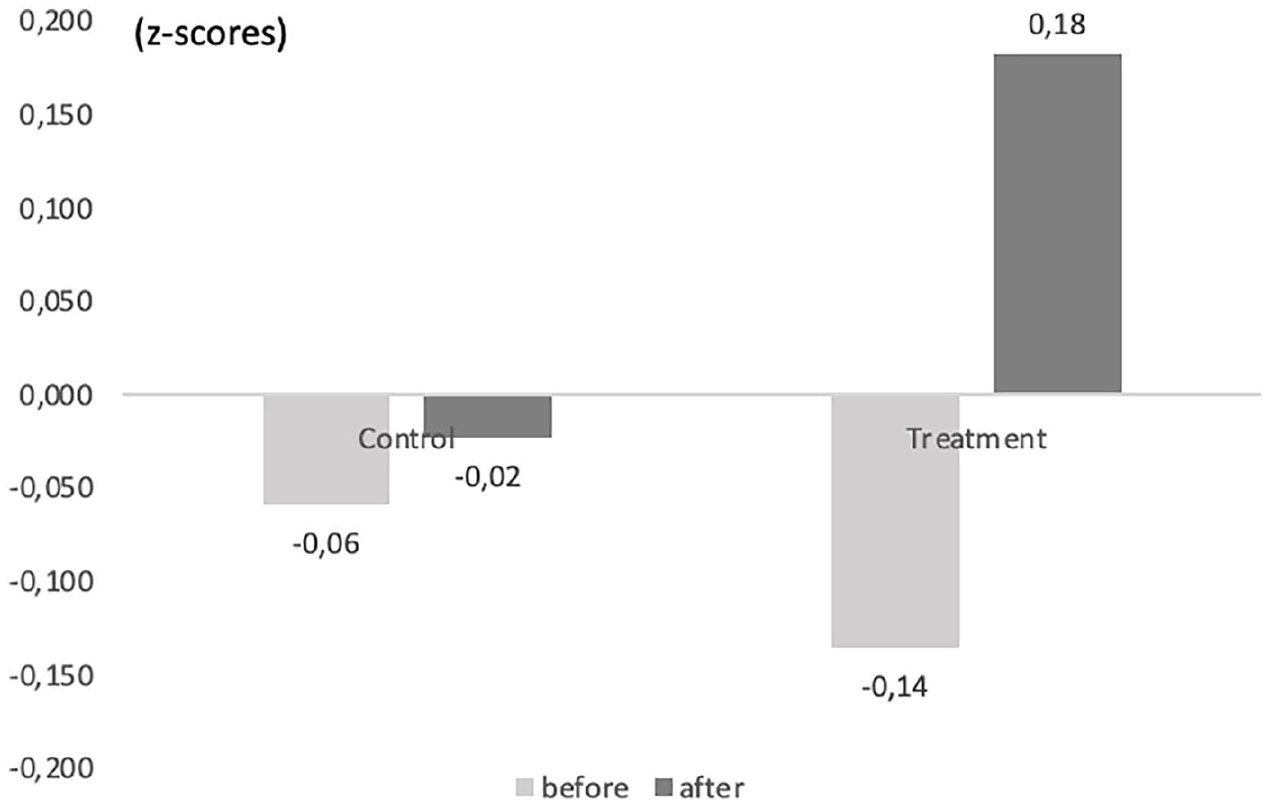
Innate Health Before and After in Treatment and Control Condition (z-Scores)
Self-Control Before and After in Treatment and Control Condition (z-Scores)
Well-Being Before and After in Treatment and Control Condition (z-Scores)
Pro-Social Behavior Before and After in Treatment and Control Condition (z-Scores)
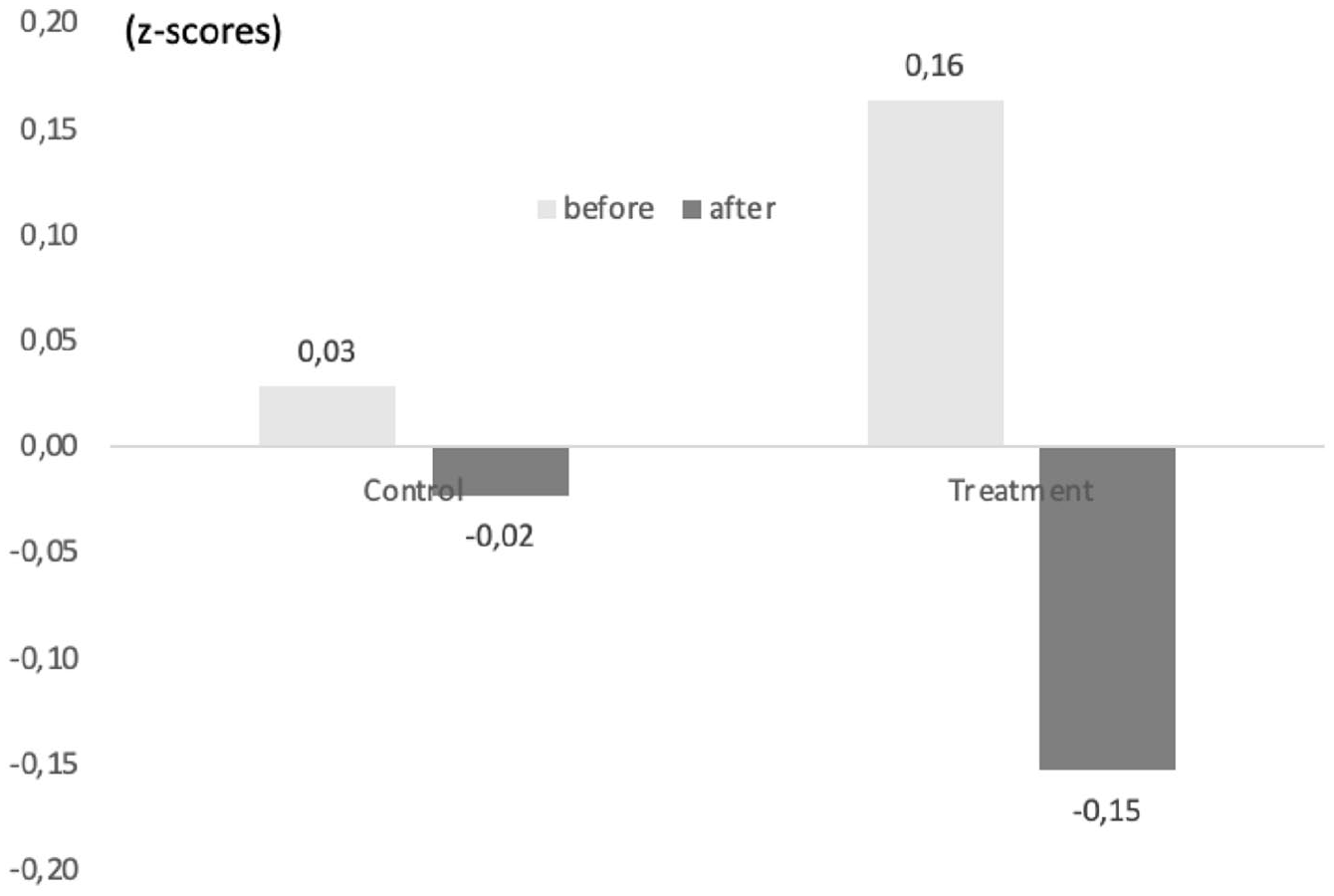
Aggression Before and After in Treatment and Control Condition (z-Scores)
Innate Health and Self-Control as Mediators
To answer the question if changes in innate health or self-control were responsible for changes in outcome measures, we tested for mediation by adding innate health and self-control individually into the equation for each outcome variable. We also checked if social desirability mediated any of the results.
First, once added, self-control (B = .428; Wald χ2 = 49.313; p < .001) and innate health (B = .585; Wald χ2 = 103.842; p < .001) demonstrated a strong influence on each other. Entering self-control into the equation completely mediated the condition by time interaction influence on innate health (B = .106; Wald χ2 = .944; p > .1; compare Table 3). Similarly, entering innate health into the analysis diminished the influence of condition by time on self-control (B = .256; Wald χ2 = 3.895; p = .048; compare Table 3). This suggests a partial mediation.
Second, up and above the influence of condition and time and their interaction, both innate health and self-control contributed to explaining well-being (respectively: B = .577, Wald χ2 = 105.801, p < .001; B = .345, Wald χ2 = 24.644, p < .001) and diminished the strength of the interaction term between condition and time on well-being (with innate health as mediator: B = .18; Waldχ2 = 11.46; p < .01; and with self-control as mediator: B = .604; Wald χ2 = 9.818; p < .002; compare Table 3). This suggests that both innate health and self-control (partially) mediated the influence of the intervention on well-being. The mediating effects of both are comparable.
Third, innate health and self-control contributed to explaining prosocial behavior (respectively: B = .358, Wald χ2 = 27.077, p < .001; and B = .216, Wald χ2 = 7.383, p < .001). After entering innate health into the equation, the condition-by-time interaction effect on prosocial behavior diminished (B = .491, Wald χ2 = 8.696, p < .001; compare Table 3). Similarly, this interaction effect between condition and time dwindled after entering self-control into the equation (B = .507, Wald χ2 = 8.142, p < .004; compare Table 3). These results suggest that both concepts were partially and equally likely to be responsible for the beneficial effects of the treatment on prosocial behavior.
Fourth, beyond the variables considered in the initial analyses as depicted in Table 3, both innate health (B = −.608, Wald χ2 = 50.575, p < .001) and self-control (B = −.629, Wald χ2 = 76.546, p < .001) contributed to explaining aggression. Also, the interaction effect between condition and time disappeared after entering innate health (B = −.158, Wald χ2 = .760, p > .1) or self-control (B = −.063, Wald χ2 = .117, p > .1), suggesting that both completely mediated the influence of the treatment over time on aggression.
Finally, the inclusion of social desirability bias into each scenario did not alter the pattern of results. An exception was found for the influence of the interaction between condition and time on aggression, which was completely mediated by social desirability (B = −.212, Wald χ2 = 2.174, p > .1). This suggests that innate health, self-esteem, and social desirability all individually explained the relative decline in aggression in the treatment condition.
Discussion
This paper aimed to replicate and extend prior studies investigating the effects of Insight to Well-Being among adults living in prison. First, our results closely replicate earlier findings, indicating that the intervention significantly increases levels of well-being among the intervention group. Second, the intervention’s effects extend beyond well-being; participants in the intervention group reported higher levels of innate health, self-control, prosocial behavior, and slightly reduced aggression as revealed by GEE analysis. Despite the strong correlation of the innate health scale with all the dependent variables, the intervention did not affect moral self-esteem, antisocial behavior, or drug use. Third, changes in innate health mediated the intervention’s effects on self-control, well-being, prosocial behavior, and aggression, suggesting that improved levels of innate health may be responsible for these changes. Fourth, changes in self-control mediated the intervention’s effects on innate health, well-being, prosocial behavior, and aggression, indicating that improved levels of self-control might contribute to observed changes in the dependent variables. Fifth, while social desirability bias might have impacted aggression reporting, it was not responsible for causing other positive changes.
These findings are preliminary; however, by detecting, describing, and testing a new focus of theoretical inquiry (i.e., innate health) within correctional psychology, this study opens the door to identifying a potential change mechanism influencing psychological and social functioning. Research into the mechanisms that cause clinical effects among psycho-social interventions, in general, but especially quasi-experimental pre-, post- studies, are rarely measured in the mental health sciences (Hofmann & Hayes, 2019; van der Velden et al., 2015), and this lack of knowledge can result in ineffective assumptions for practice theory and therapeutic targets in correctional psychology (Ward & Durrant, 2021). This study specifically addresses this gap in criminology, and the mental health literature more broadly, by finding both innate health and self-control as equivalent mediators, explaining improvements after a mental health intervention. This finding suggests distinct and potentially complementary mechanisms.
Future Research
Future research should explore the contrast between models targeting maladaptive cognitions and health-based, such as Innate Health. The latter posits that change arises from realizing one’s innate capacity and potential. Our study underscores the need for future investigations into well-being interventions that incorporate broader meaning making frameworks. Researchers can distinguish interventions based on these assumptions, examining their distinct impacts on therapeutic and educational outcomes. We hypothesize that no matter the setting, interventions grounded in the assumption of innate capacity yield different attention, structure, and potentially greater effectiveness. At the very least, innate health emerges as a potentially effective mechanism for promoting well-being and prosocial behavior in prison settings. This seems to be true even after a brief 3-day intensive program. This suggests that innate health could offer a cost-effective alternative for reducing mental health issues and potential impacts on recidivism. However, further research into innate health as a functioning mechanism is needed.
Limitations
While this study does several novel things well, like other clinical trials conducted with a convenience sample among men living in prison, this study has several limitations. First, the prison environment is highly restrictive and the ISFL wing provided a unique opportunity for residents to choose what kind of programming they enrolled into, so random assignment was not possible. Second, the prison environment is highly unstable with little to no means of tracking research participants after they leave the wing, failing to capture both a second wave of waitlist control participants (as they had moved on) and longitudinal quantitative data (making it difficult to extrapolate findings over a longer period). This issue significantly limited the ability to examine the impact of the program on drug use over time (surveys required a minimum of 3 months to test any changes). Last, due to the need for a rigorous ethics review from two institutions (required for working with high-risk participants), research could not begin as the wing opened up and programs were becoming available. Thus, residents on the wing who had more knowledge (or had lived longer on the wing) had already signed up to take this program. This was evidenced by differences in time living on the wing (4 weeks longer in the intervention group). While this study was sufficiently powered, it only examined men living in one wing of a UK prison.
Conclusion
This is a novel study that identified a common underlying assumption behind human potential and positive psychological interventions specifically—the human capacity for innate health—and asked: Does innate health function as a mediator in the same way self-control does within an incarcerated population? We conducted a mediation analysis, tested social desirability bias, and examined the impact of the intervention on crucial variables such as well-being, self-control, aggression, drug abuse, and anti- and pro-social behavior.
This study showed improvements in levels of innate health, self-control, well-being, and prosocial behavior and lower levels of aggression in the intervention group as compared to the control group. More importantly, innate health was found to serve as a mediator that functions similarly to self-control among men living in prison. This indicates future research should incorporate innate health as a potential mechanism across mental health and well-being variables and populations.
Footnotes
Authors’ note:
The authors declare there are no known conflicts of interest to disclose. This study was funded by the non-profit Innate Health Research. We are deeply grateful to the following people: Douglas MacDonald, for supervising the ethics review process; Jacqueline Hollows, for inviting us to evaluate the Insight to Well-Being intervention; Daniela Palade, for providing onsite research supervision; the governor of HMP Nottingham and prison staff for welcoming us into the prison; as well as Derrick Mason, the facilitators and the men living in prison who shared their time and experiences with us. Anita McGinty, for her editorial guidance.